An Overview of Long-Acting GnRH Agonists in Premenopausal Breast Cancer Patients: Survivorship Challenges and Management



Abstract
1. Introduction
1.1. Epidemiology
1.2. Current Management of Early-Stage HR-Positive Breast Cancer
1.3. Ongoing Challenges in Premenopausal Breast Cancer Management
1.3.1. Side Effects of OFS
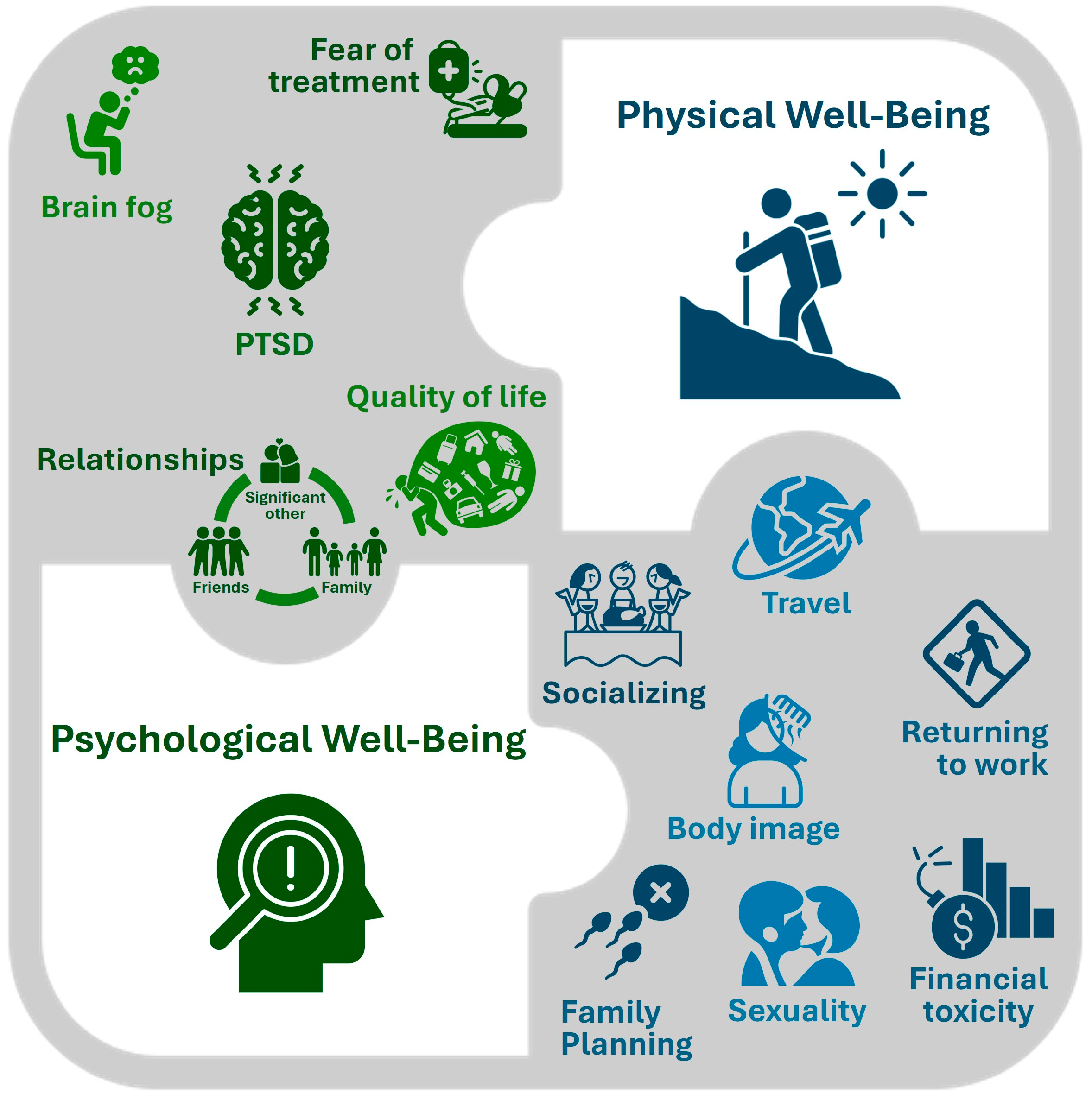
1.3.2. Survivorship Challenges
2. Management of Ovarian Function Suppression with GnRH Agonists Administered Every 3 Months in Breast Cancer
2.1. Goserelin Dosage Options and Guidelines for Use
2.2. Efficacy Studies of Goserelin 10.8 mg LA in Breast Cancer
3. Use Cases for GnRH Agonist LA Formulations in Breast Cancer
4. Benefits of the Goserelin 10.8 mg LA Formulation
4.1. Goserelin as the GnRH Agonist of Choice for OFS
4.2. Off-Label Use of Goserelin 10.8 mg LA during the Pandemic
4.3. Expanded Indications for Goserelin 10.8 mg LA
4.4. More Efficient Healthcare Resource Utilization with Goserelin 10.8 mg LA
5. Recommendations for Monitoring Patients on GnRH Agonist LA Formulations in Breast Cancer
6. Future Directions
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canadian Cancer Society. Canadian Cancer Statistics 2023. Available online: https://cdn.cancer.ca/-/media/files/cancer-information/resources/publications/canadian-cancer-statistics-2023/2023pdfen.pdf (accessed on 6 February 2024).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Nelson, D.R.; Brown, J.; Morikawa, A.; Method, M. Breast cancer-specific mortality in early breast cancer as defined by high-risk clinical and pathologic characteristics. PLoS ONE 2022, 17, e0264637. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.F.; Karami, S.; Peidl, A.S.; Waiters, K.D.; Babajide, M.F.; Bawa-Khalfe, T. Androgen receptor in hormone receptor-positive breast cancer. Int. J. Mol. Sci. 2023, 25, 476. [Google Scholar] [CrossRef] [PubMed]
- Cancer Care Ontario. Clinical Utility of Multigene Profiling Assays in Invasive Early-Stage Breast Cancer. Available online: https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/31766 (accessed on 14 May 2024).
- Kalinsky, K.; Barlow, W.E.; Gralow, J.R.; Meric-Bernstam, F.; Albain, K.S.; Hayes, D.F.; Lin, N.U.; Perez, E.A.; Goldstein, L.J.; Chia, S.K.L.; et al. 21-gene assay to inform chemotherapy benefit in node-positive breast cancer. N. Engl. J. Med. 2021, 385, 2336–2347. [Google Scholar] [CrossRef]
- Cardoso, F.; van’t Veer, L.J.; Bogaerts, J.; Slaets, L.; Viale, G.; Delaloge, S.; Pierga, J.Y.; Brain, E.; Causeret, S.; DeLorenzi, M.; et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer. N. Engl. J. Med. 2016, 375, 717–729. [Google Scholar] [CrossRef]
- Piccart, M.; van ‘t Veer, L.J.; Poncet, C.; Lopes Cardozo, J.M.N.; Delaloge, S.; Pierga, J.Y.; Vuylsteke, P.; Brain, E.; Vrijaldenhoven, S.; Neijenhuis, P.A.; et al. 70-gene signature as an aid for treatment decisions in early breast cancer: Updated results of the phase 3 randomised MINDACT trial with an exploratory analysis by age. Lancet Oncol. 2021, 22, 476–488. [Google Scholar] [CrossRef] [PubMed]
- Mamounas, E.P. NRG-BR009: Phase III adjuvant trial evaluating the addition of the adjuvant chemotherapy to Ovarian Function Suppression plus Endocrine Therapy in premenopausal patients with pN0-1, ER-positive/HER2-negative breast cancer and an oncotype recurrence score ≤ 25 (OFSET). In Proceedings of the San Antonio Breast Cancer Symposium, San Antonio, TX, USA, 5–9 December 2023. [Google Scholar]
- Ambikairajah, A.; Walsh, E.; Cherbuin, N. A review of menopause nomenclature. Reprod. Health 2022, 19, 29. [Google Scholar] [CrossRef]
- Referenced with Permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Breast Cancer V 3.2024. © National Comprehensive Cancer Network, Inc. 2024. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 17 June 2024).
- Menen, R.S.; Hunt, K.K. Considerations for the treatment of young patients with breast cancer. Breast J. 2016, 22, 667–672. [Google Scholar] [CrossRef]
- Corrigan, K.L.; Kouzy, R.; Jaoude, J.A.; Patel, R.R.; Layman, R.M.; Giordano, S.H.; Woodward, W.A.; Smith, B.D.; Shaitelman, S.F.; Ludmir, E.B. Inclusion of premenopausal women in breast cancer clinical trials. Breast 2022, 66, 204–207. [Google Scholar] [CrossRef]
- Burstein, H.J.; Lacchetti, C.; Anderson, H.; Buchholz, T.A.; Davidson, N.E.; Gelmon, K.A.; Giordano, S.H.; Hudis, C.A.; Solky, A.J.; Stearns, V.; et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO Clinical Practice Guideline focused update. J. Clin. Oncol. 2019, 37, 423–438. [Google Scholar] [CrossRef]
- Burstein, H.J.; Lacchetti, C.; Anderson, H.; Buchholz, T.A.; Davidson, N.E.; Gelmon, K.E.; Giordano, S.H.; Hudis, C.A.; Solky, A.J.; Stearns, V.; et al. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: American Society of Clinical Oncology Clinical Practice Guideline update on ovarian suppression. J. Clin. Oncol. 2016, 34, 1689–1701. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; on behalf of the ESMO Guidelines Committee. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-updagger. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed]
- Francis, P.A.; Regan, M.M.; Fleming, G.F.; Lang, I.; Ciruelos, E.; Bellet, M.; Bonnefoi, H.R.; Climent, M.A.; Da Prada, G.A.; Burstein, H.J.; et al. Adjuvant ovarian suppression in premenopausal breast cancer. N. Engl. J. Med. 2015, 372, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Pagani, O.; Francis, P.A.; Fleming, G.F.; Walley, B.A.; Viale, G.; Colleoni, M.; Lang, I.; Gomez, H.L.; Tondini, C.; Pinotti, G.; et al. Absolute improvements in freedom from distant recurrence to tailor adjuvant endocrine therapies for premenopausal women: Results from TEXT and SOFT. J. Clin. Oncol. 2020, 38, 1293–1303. [Google Scholar] [CrossRef] [PubMed]
- Telli, M.L.; Gradishar, W.J.; Ward, J.H. NCCN guidelines updates: Breast cancer. J. Natl. Compr. Cancer Netw. 2019, 17, 552–555. [Google Scholar] [CrossRef]
- Lambertini, M.; Viglietti, G.; de Azambuja, E. Impact of ovarian function suppression in premenopausal women with estrogen receptor-positive early breast cancer. Curr. Opin. Oncol. 2019, 31, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Ferreiro, E.; de Uralde, B.L.; Abreu, R.; Garcia-Velasco, J.A.; Munoz, E. Aromatase inhibitors for ovarian stimulation in patients with breast cancer. Curr. Drug Targets 2020, 21, 910–921. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.G.; Bradley, R.; Braybrooke, J.; Clarke, M.; Hills, R.K.; Peto, R.; Bergh, J.C.S.; Swain, S.M.; Davidson, N.E.; Francis, P.A.; et al. Effects of ovarian ablation or suppresson on breast cancer recurrence and survival: Patient-level meta-analysis of 14,993 pre-menopausal women in 25 randomized trials. J. Clin. Oncol. 2023, 41, 503. [Google Scholar] [CrossRef]
- Partridge, A.H.; Niman, S.M.; Ruggeri, M.; Peccatori, F.A.; Azim, H.A., Jr.; Colleoni, M.; Saura, C.; Shimizu, C.; Saetersdal, A.B.; Kroep, J.R.; et al. Interrupting endocrine therapy to attempt pregnancy after breast cancer. N. Engl. J. Med. 2023, 388, 1645–1656. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Menopause: Diagnosis and Management. Available online: https://www.nice.org.uk/guidance/ng23 (accessed on 23 April 2024).
- Honour, J.W. Biochemistry of the menopause. Ann. Clin. Biochem. 2018, 55, 18–33. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. NCT05879926: Evaluating the Addition of Adjuvant Chemotherapy to Ovarian Function Suppression Plus Endocrine Therapy in Premenopausal Patients with pN0-1, ER-Positive/HER2-Negative Breast Cancer and an Oncotype Recurrence Score Less than or Equal to 25 (OFSET). Available online: https://classic.clinicaltrials.gov/ct2/show/NCT05879926 (accessed on 13 May 2024).
- Quan, M.L.; Olivotto, I.A.; Baxter, N.N.; Friedenreich, C.M.; Metcalfe, K.; Warner, E.; MacLennan, K.; Stephen, J.E.; Akbari, M.R.; Howell, D.; et al. A pan-Canadian prospective study of young women with breast cancer: The rationale and protocol design for the RUBY study. Curr. Oncol. 2020, 27, e516–e523. [Google Scholar] [CrossRef] [PubMed]
- Ribi, K.; Luo, W.; Bernhard, J.; Francis, P.A.; Burstein, H.J.; Ciruelos, E.; Bellet, M.; Pavesi, L.; Lluch, A.; Visini, M.; et al. Adjuvant tamoxifen plus ovarian function suppression versus tamoxifen alone in premenopausal women with early breast cancer: Patient-reported outcomes in the suppression of ovarian function trial. J. Clin. Oncol. 2016, 34, 1601–1610. [Google Scholar] [CrossRef]
- Saha, P.; Regan, M.M.; Pagani, O.; Francis, P.A.; Walley, B.A.; Ribi, K.; Bernhard, J.; Luo, W.; Gomez, H.L.; Burstein, H.J.; et al. Treatment efficacy, adherence, and quality of life among women younger than 35 years in the International Breast Cancer Study Group TEXT and SOFT adjuvant endocrine therapy trials. J. Clin. Oncol. 2017, 35, 3113–3122. [Google Scholar] [CrossRef] [PubMed]
- Francis, P.A.; Pagani, O.; Fleming, G.F.; Walley, B.A.; Colleoni, M.; Lang, I.; Gomez, H.L.; Tondini, C.; Ciruelos, E.; Burstein, H.J.; et al. Tailoring adjuvant endocrine therapy for premenopausal breast cancer. N. Engl. J. Med. 2018, 379, 122–137. [Google Scholar] [CrossRef]
- Dinas, K.D. Fertility counseling and preservation for breast cancer patients. Adv. Exp. Med. Biol. 2020, 1252, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Hoving, J.L.; Broekhuizen, M.L.; Frings-Dresen, M.H. Return to work of breast cancer survivors: A systematic review of intervention studies. BMC Cancer 2009, 9, 117. [Google Scholar] [CrossRef] [PubMed]
- Islam, T.; Dahlui, M.; Majid, H.A.; Nahar, A.M.; Mohd Taib, N.A.; Su, T.T.; MyBCC study group. Factors associated with return to work of breast cancer survivors: A systematic review. BMC Public Health 2014, 14 (Suppl. S3), S8. [Google Scholar] [CrossRef] [PubMed]
- PDQ® Adult Treatment Editorial Board. PDQ Financial Toxicity (Financial Distress) and Cancer Treatment. Available online: https://www.cancer.gov/about-cancer/managing-care/track-care-costs/financial-toxicity-pdq (accessed on 13 April 2024).
- Singer, S.; Blettner, M.; Kreienberg, R.; Janni, W.; Wockel, A.; Kuhn, T.; Felberbaum, R.; Flock, F.; Schwentner, L.; for the BRENDA II study group. Breast cancer patients’ fear of treatment: Results from the multicenter longitudinal study BRENDA II. Breast Care 2015, 10, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Carreira, H.; Williams, R.; Muller, M.; Harewood, R.; Stanway, S.; Bhaskaran, K. Associations between breast aancer survivorship and adverse mental health outcomes: A systematic review. J. Natl. Cancer Inst. 2018, 110, 1311–1327. [Google Scholar] [CrossRef]
- Schmidt, M.E.; Scherer, S.; Wiskemann, J.; Steindorf, K. Return to work after breast cancer: The role of treatment-related side effects and potential impact on quality of life. Eur. J. Cancer Care 2019, 28, e13051. [Google Scholar] [CrossRef]
- Yeo, H.Y.; Liew, A.C.; Chan, S.J.; Anwar, M.; Han, C.H.; Marra, C.A. Understanding patient preferences regarding the important determinants of breast cancer treatment: A narrative scoping review. Patient Prefer. Adherence 2023, 17, 2679–2706. [Google Scholar] [CrossRef] [PubMed]
- Nourmoussavi, M.; Pansegrau, G.; Popesku, J.; Hammond, G.L.; Kwon, J.S.; Carey, M.S. Ovarian ablation for premenopausal breast cancer: A review of treatment considerations and the impact of premature menopause. Cancer Treat. Rev. 2017, 55, 26–35. [Google Scholar] [CrossRef] [PubMed]
- TerSera Therapeutics LLC. Zoladex 10.8 mg Product Monograph. Available online: https://documents.tersera.com/zoladex-ca/10.8mg_ProductMonograph.pdf (accessed on 6 May 2024).
- Chen, Y.; Zhang, R.; Yan, Y.; Li, H.; Song, G. Effectiveness of gonadotropin-releasing hormone agonists for ovarian function suppression in premenopausal patients with hormone receptor-positive breast cancer: A retrospective single-center real-world study. Breast Cancer Res. Treat. 2024, 206, 543–550. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Leuprorelin Acetate SR 11.25 mg for Injection Specified Drug-Use Survey “Long-Term Use Survey on Premenopausal Breast Cancer Patients (96 Weeks)”. Available online: https://clinicaltrials.gov/study/NCT02154139 (accessed on 17 June 2024).
- Kendzierski, D.C.; Schneider, B.P.; Kiel, P.J. Efficacy of different leuprolide administration schedules in premenopausal breast cancer: A retrospective review. Clin. Breast Cancer 2018, 18, e939–e942. [Google Scholar] [CrossRef] [PubMed]
- Kurebayashi, J.; Shiba, E.; Toyama, T.; Matsumoto, H.; Okazaki, M.; Nomizu, T.; Ohtake, T.; Fujii, T.; Ohashi, Y. A follow-up study of a randomized controlled study evaluating safety and efficacy of leuprorelin acetate every-3-month depot for 2 versus 3 or more years with tamoxifen for 5 years as adjuvant treatment in premenopausal patients with endocrine-responsive breast cancer. Breast Cancer 2021, 28, 684–697. [Google Scholar] [CrossRef] [PubMed]
- Kurebayashi, J.; Toyama, T.; Sumino, S.; Miyajima, E.; Fujimoto, T. Efficacy and safety of leuprorelin acetate 6-month depot, TAP-144-SR (6M), in combination with tamoxifen in postoperative, premenopausal patients with hormone receptor-positive breast cancer: A phase III, randomized, open-label, parallel-group comparative study. Breast Cancer 2017, 24, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Wu, Z.Y.; Kim, H.J.; Lee, J.W.; Chung, I.Y.; Kim, J.; Lee, S.B.; Son, B.H.; Kim, S.B.; Jung, J.H.; et al. Change in estradiol levels among premenopausal patients with breast cancer treated using leuprolide acetate 11.25 milligrams 3-month depot and tamoxifen. J. Breast Cancer 2020, 23, 553–559. [Google Scholar] [CrossRef]
- Schmid, P.; Untch, M.; Kosse, V.; Bondar, G.; Vassiljev, L.; Tarutinov, V.; Lehmann, U.; Maubach, L.; Meurer, J.; Wallwiener, D.; et al. Leuprorelin acetate every-3-months depot versus cyclophosphamide, methotrexate, and fluorouracil as adjuvant treatment in premenopausal patients with node-positive breast cancer: The TABLE study. J. Clin. Oncol. 2007, 25, 2509–2515. [Google Scholar] [CrossRef]
- Schmid, P.; Untch, M.; Wallwiener, D.; Kosse, V.; Bondar, G.; Vassiljev, L.; Tarutinov, V.; Kienle, E.; Luftner, D.; Possinger, K.; et al. Cyclophosphamide, methotrexate and fluorouracil (CMF) versus hormonal ablation with leuprorelin acetate as adjuvant treatment of node-positive, premenopausal breast cancer patients: Preliminary results of the TABLE-study (Takeda Adjuvant Breast cancer study with Leuprorelin Acetate). Anticancer Res. 2002, 22, 2325–2332. [Google Scholar]
- Shiba, E.; Yamashita, H.; Kurebayashi, J.; Noguchi, S.; Iwase, H.; Ohashi, Y.; Sasai, K.; Fujimoto, T. A randomized controlled study evaluating safety and efficacy of leuprorelin acetate every-3-months depot for 2 versus 3 or more years with tamoxifen for 5 years as adjuvant treatment in premenopausal patients with endocrine-responsive breast cancer. Breast Cancer 2016, 23, 499–509. [Google Scholar] [CrossRef]
- Wu, H.; Bian, L.; Xie, J.; Zou, Y.; Wu, L.; Huang, S.; Xie, X.; Wang, X. 111P Goserelin 3 monthly depot is noninferior to goserelin monthly depot in the treatment of breast cancer: A real-world evidence study. ESMO Open 2023, 8, 101335. [Google Scholar] [CrossRef]
- Noguchi, S.; Kim, H.J.; Jesena, A.; Parmar, V.; Sato, N.; Wang, H.C.; Lokejaroenlarb, S.; Isidro, J.; Kim, K.S.; Itoh, Y.; et al. Phase 3, open-label, randomized study comparing 3-monthly with monthly goserelin in pre-menopausal women with estrogen receptor-positive advanced breast cancer. Breast Cancer 2016, 23, 771–779. [Google Scholar] [CrossRef] [PubMed]
- Huerta-Reyes, M.; Maya-Nunez, G.; Perez-Solis, M.A.; Lopez-Munoz, E.; Guillen, N.; Olivo-Marin, J.C.; Aguilar-Rojas, A. Treatment of breast cancer with gonadotropin-releasing hormone analogs. Front. Oncol. 2019, 9, 943. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.S.; Wong, A.; Kim, H.J. Ovarian function suppression with luteinizing hormone-releasing hormone agonists for the treatment of hormone receptor-positive early breast cancer in premenopausal women. Front. Oncol. 2021, 11, 700722. [Google Scholar] [CrossRef] [PubMed]
- TerSera Therapeutics LLC. Zoladex 3.6 mg Product Monograph. Available online: https://documents.tersera.com/zoladex-ca/3.6mg_ProductMonograph.pdf (accessed on 6 March 2024).
- Masuda, N.; Iwata, H.; Rai, Y.; Anan, K.; Takeuchi, T.; Kohno, N.; Takei, H.; Yanagita, Y.; Noguchi, S. Monthly versus 3-monthly goserelin acetate treatment in pre-menopausal patients with estrogen receptor-positive early breast cancer. Breast Cancer Res. Treat. 2011, 126, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Moore, H.C.F.; Leonard, R.C.F.; Loibl, S.; Munster, P.; Bruzzone, M.; Boni, L.; Unger, J.M.; Anderson, R.A.; Mehta, K.; et al. Gonadotropin-releasing hormone agonists during chemotherapy for preservation of ovarian function and fertility in premenopausal patients with early breast cancer: A systematic review and meta-analysis of individual patient-level data. J. Clin. Oncol. 2018, 36, 1981–1990. [Google Scholar] [CrossRef] [PubMed]
- Burns, E.; Koca, E.; Xu, J.; McLean, E.; Lee, R.; Patel, T.; Chang, J.; Niravath, P. Measuring ovarian escape in premenopausal estrogen receptor-positive breast cancer patients on ovarian suppression therapy. Oncologist 2021, 26, e936–e942. [Google Scholar] [CrossRef]
- Bellet, M.; Gray, K.P.; Francis, P.A.; Lang, I.; Ciruelos, E.; Lluch, A.; Climent, M.A.; Catalan, G.; Avella, A.; Bohn, U.; et al. Twelve-month estrogen levels in premenopausal women with hormone receptor-positive breast cancer receiving adjuvant triptorelin plus exemestane or tamoxifen in the Suppression of Ovarian Function Trial (SOFT): The SOFT-EST Substudy. J. Clin. Oncol. 2016, 34, 1584–1593. [Google Scholar] [CrossRef] [PubMed]
- de Ciantis, M.; Faure, C.; Heudel, P.E.; Tredan, O.; Rousset-Jablonski, C. Ovarian suppression failure during GnRH agonist treatment: A report of three breast cancer patients. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 261–264. [Google Scholar] [CrossRef]
- McCann, K.E.; Goldfarb, S.B.; Traina, T.A.; Regan, M.M.; Vidula, N.; Kaklamani, V. Selection of appropriate biomarkers to monitor effectiveness of ovarian function suppression in pre-menopausal patients with ER+ breast cancer. npj Breast Cancer 2024, 10, 8. [Google Scholar] [CrossRef]
- TerSera Therapeutics LLC. Data on File. Clinical Study Report Synopsis: Study Code D8664C00008; AstraZeneca: Macclesfield, UK, 2010. [Google Scholar]
- El Zawawy, S.F.; Khedr, G. 209P Efficacy and feasibility of long acting every three months goserelin for premenopausal breast cancer patients during COVID pandemic. Ann. Oncol. 2022, 33, S631. [Google Scholar] [CrossRef]
- Sa-Nguanraksa, D.; Krisorakun, T.; Pongthong, W.; O-Charoenrat, P. Survival outcome of combined GnRH agonist and tamoxifen is comparable to that of sequential adriamycin and cyclophosphamide chemotherapy plus tamoxifen in premenopausal patients with early breast cancer. Mol. Clin. Oncol. 2019, 11, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Blotta, D.A.; Gomes, J.R.; Moreira, S.B.R.; Colosimo, D.F.; Cavalcanti, C.C.G.; Forgiarini, E.A.; Gagliato, D.D.M.; Buzaid, A.C. Efficacy of ovarian function suppression of 3-monthly versus monthly GnRH agonist as endocrine therapy for premenopausal breast cancer patients. J. Clin. Oncol. 2023, 41, 527. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, X.; Wu, J.; Liu, H.; Zhao, J.; Huang, J.; Liu, J.; Gong, Y.; Wang, H.; Yang, H.; et al. 123P—Goserelin 10.8 mg and 3.6 mg depots in breast cancer (BC): A large real-world noninferiority study. In Proceedings of the ESMO Breast Cancer Annual Congress, Berlin, Germany, 15–17 May 2024. [Google Scholar]
- TerSera Therapeutics LLC. Data on File. 2.7.3 Summary of Clinical Efficacy: Goserelin Acetate; AstraZeneca: Macclesfield, UK, 2021. [Google Scholar]
- AbbVie Corporation. Lupron Depot Product Monograph. Available online: https://www.abbvie.ca/content/dam/abbvie-dotcom/ca/en/documents/products/LUPRON_DEPOT_PM_EN.pdf (accessed on 20 March 2024).
- Allergan Pharma Co. Product Monograph Including Patient Medication Information: Trelstar. Available online: https://pdf.hres.ca/dpd_pm/00059731.PDF (accessed on 2 May 2024).
- Sukumar, J.S.; Quiroga, D.; Kassem, M.; Grimm, M.; Shinde, N.V.; Appiah, L.; Palettas, M.; Stephens, J.; Gatti-Mays, M.E.; Pariser, A.; et al. Patient preferences and adherence to adjuvant GnRH analogs among premenopausal women with hormone receptor positive breast cancer. Breast Cancer Res. Treat. 2021, 190, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Drug Shortages Canada. Drug Shortage Report for Decapeptyl. Available online: https://www.drugshortagescanada.ca/drug/24982 (accessed on 29 April 2024).
- Early Breast Cancer Trialists’ Collaborative Group. Aromatase inhibitors versus tamoxifen in premenopausal women with oestrogen receptor-positive early-stage breast cancer treated with ovarian suppression: A patient-level meta-analysis of 7030 women from four randomised trials. Lancet Oncol 2022, 23, 382–392. [Google Scholar] [CrossRef] [PubMed]
- TerSera Therapeutics LLC. Data on File. LeVasseur, N. Health Canada Supplemental New Drug Submission (SNDS) for Zoladex® LA (Goserelin) 10.8 mg Depot; TerSera Therapeutics LLC: Deerfield, IL, USA, 2022. [Google Scholar]
- Ontario Health Cancer Care Ontario. Pandemic Planning Clinical Guidelines for Patients with Cancer. Available online: https://www.accc-cancer.org/docs/documents/cancer-program-fundamentals/oh-cco-pandemic-planning-clinical-guideline_final_2020-03-10.pdf? (accessed on 30 April 2024).
- World Health Organization. Maintaining Essential Health Services: Operational Guidance for the COVID-19 Context. Available online: https://iris.who.int/bitstream/handle/10665/332240/WHO-2019-nCoV-essential_health_services-2020.2-eng.pdf (accessed on 30 April 2024).
- Kauffman, R.P.; Young, C.; Castracane, V.D. Perils of prolonged ovarian suppression and hypoestrogenism in the treatment of breast cancer: Is the risk of treatment worse than the risk of recurrence? Mol. Cell Endocrinol. 2021, 525, 111181. [Google Scholar] [CrossRef] [PubMed]
- Shuster, L.T.; Rhodes, D.J.; Gostout, B.S.; Grossardt, B.R.; Rocca, W.A. Premature menopause or early menopause: Long-term health consequences. Maturitas 2010, 65, 161–166. [Google Scholar] [CrossRef]
- Storesund, A.; Haugen, A.S.; Hjortas, M.; Nortvedt, M.W.; Flaatten, H.; Eide, G.E.; Boermeester, M.A.; Sevdalis, N.; Softeland, E. Accuracy of surgical complication rate estimation using ICD-10 codes. Br. J. Surg. 2019, 106, 236–244. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. NCT04906395: Ovarian Suppression Evaluating Subcutaneous Leuprolide Acetate in Breast Cancer (OVELIA). Available online: https://clinicaltrials.gov/study/NCT04906395 (accessed on 13 May 2024).


{kind=link}
{kind=link}
| Study | Study Design | Treatment Arms | Patient Population | Endpoints |
|---|---|---|---|---|
| Masuda et al., 2011 [55] Phase II (D8664C00004/NCT 00303524) | Open-label, randomized, parallel group, multicenter | Goserelin 10.8 mg LA Q3 months or Goserelin 3.6 mg Q month + Tamoxifen 20 mg PO QD | Premenopausal women * with ER+ early breast cancer who had undergone radical surgery n = 170 (1:1 randomization) | Primary (non-inferiority): AUC(4–24 week) of E2 serum concentration |
| Key secondary: E2 serum concentrations; percentage of patients with mean E2 serum concentration ≤30 pg/mL; menstruation; safety | ||||
| Noguchi et al., 2016 [51] Phase III (D8666C00001/NCT 01073865) | Open-label, randomized, parallel group, multicenter | Goserelin 10.8 mg LA Q3 months or Goserelin 3.6 mg Q month + Tamoxifen 20 mg PO QD | Premenopausal women † with ER+ advanced breast cancer n = 222 (1:1 randomization) | Primary (non-inferiority): PFS at Week 24 |
| Key secondary: ORR at Week 24; E2 serum concentrations; safety | ||||
| Collaborative Data on file [61] Phase III (D8664C00008) | Open-label, randomized, parallel group, multicenter | Goserelin 10.8 mg LA Q3 months or Goserelin 3.6 mg Q month + Tamoxifen 20 mg PO QD | Premenopausal women ‡ with ER+ advanced breast cancer n = 98 (1:1 randomization) | Primary (non-inferiority): PFS at Week 24 |
| Key secondary: ORR at Week 24; E2 serum concentrations | ||||
| Sa-Nguanraksa et al., 2019 [63] | Retrospective, single center | Goserelin 10.8 mg LA Q3 months + Tamoxifen 20 mg PO QD or AC-TAM | Premenopausal women § with HR+ breast cancer n = 170 | DFS |
| Wu et al., 2023 [50] | Retrospective, observational, real-world electronic record review | Goserelin 10.8 mg LA Q3 months or Goserelin 3.6 mg Q month | Pre- and perimenopausal patients with HR+ breast cancer n = 240 | Primary (non-inferiority): E2 serum concentrations |
| Key secondary: OS, DFS for early breast cancer, PFS for advanced breast cancer | ||||
| El Zawawy et al., 2022 [62] | Retrospective review | Goserelin 10.8 mg LA Q12 weeks or Goserelin 3.6 mg Q month + Tamoxifen 20 mg PO QD or an AI ** | Premenopausal women with HR+ breast cancer n = 87 | E2 serum concentrations; DFS for non-metastatic breast cancer; PFS for metastatic breast cancer; safety |
| Blotta et al., 2023 [64] | Retrospective | Goserelin 10.8 mg LA Q3 months or Goserelin 3.6 mg Q month + AI | Premenopausal women with ER+ breast cancer n = 88 | Patients with E2 level >2.72 pg/mL (ineffective OFS) |
| Wang et al., 2024 [65] (NCT 05184257) | Retrospective/prospective, real-world, multicenter, medical record data review | Goserelin 10.8 mg LA Q3 months or Goserelin 3.6 mg Q month ± SERM/AI | Premenopausal women with HR+ breast cancer n = 590 | Primary (non-inferiority): E2 suppression to postmenopausal level at Week 12 ± 4 |
| Study | E2 Levels | PFS | ORR | DFS | Other Endpoints | Safety (10.8 mg vs. 3.6 mg) |
|---|---|---|---|---|---|---|
| Masuda et al., 2011 [55] | Primary endpoint (non-inferiority) 10.8 mg: AUC(4–24 week) 18.32 pg/mL•week 3.6 mg: AUC(4–24 week) 18.95 pg/mL•week Ratio = 0.974 (95% CI: 0.80, 1.19) * | NR | NR | 10.8 mg: 4 events in 675 days 3.6 mg: 1 event in 676 days |
|
|
| ≥98.8% in both groups maintained E2 < 30 pg/mL (postmenopausal range) | ||||||
| Noguchi et al., 2016 [51] | Week 12 10.8 mg: 26.3 pg/mL 3.6 mg: 25.4 pg/mL | Primary endpoint at Week 24 (non-inferiority) † 10.8 mg: 61.5% 3.6 mg: 60.2% Treatment difference 1.3 (95% CI: –11.4, 13.9) | Week 24 10.8 mg: 23.9% 3.6 mg: 26.9% Treatment difference 3.0% (95% CI: –15.5%, 9.7%) | NR | NR |
|
| Week 24 10.8 mg: 20.3 pg/mL 3.6 mg: 24.8 pg/mL | ||||||
| Collaborative Data on file [61] | 10.8 mg: 7.2 pmol/L 3.6 mg: 10.4 pmol/L | Primary endpoint at Week 24 (non-inferiority) ‡ 10.8 mg: 69.4% 3.6 mg: 73.5% Treatment difference –4.1 (95% CI: –21.4, 13.6) | Week 24 10.8 mg: 28.9% 3.6 mg: 25.6% | NR | NR |
|
| Sa-Nguanraksa et al., 2019 [63] | NR | NR | NR | 5-year DFS GnRH-TAM: 0.97 AC-TAM: 0.98 | NR | NR |
| 10-year DFS GnRH-TAM: 0.97 AC-TAM: 0.94 p = 0.86 § hazard ratio = 1.90 (95% CI: 0.19, 18.80) | ||||||
| Wu et al., 2023 [50] | Primary endpoint (non-inferiority) E2 suppression rate: 10.8 mg: 99.0% 3.6 mg: 92.7% Risk difference = 0.065 (95% CI: 0.021, 0.135) ** p = 0.0187 | 3.2-year PFS 10.8 mg: 77.1% 3.6 mg: 80.0% | NR | 5-year DFS 10.8 mg: 99.0% 3.6 mg: 96.7% |
| NR |
| El Zawawy et al., 2022 [62] | Week 12 10.8 mg: 15.4 pg/mL 3.6 mg: NR | Metastatic 10.8 mg: 66.7% 3.6 mg: 63.6% p = 0.88 NS | NR | Non-metastatic 10.8 mg: 86.2% 3.6 mg: 87.1% p = 0.71 NS |
|
|
| Week 24 10.8 mg: 10.8 pg/mL 3.6 mg: NR | ||||||
| Week 36 10.8 mg: 9.6 pg/mL 3.6 mg: NR | ||||||
| Blotta et al., 2023 [64] | E2 level > 2.72 pg/mL (ineffective OFS): 10.8 mg: 14.8% 3.6 mg: 40.7% p = 0.007 | NR | NR | NR | NR | NR |
| Wang et al., 2024 [65] | Primary endpoint (non-inferiority) E2 suppression to postmenopausal level at Week 12 ± 4 10.8 mg: 99.1% 3.6 mg: 95.3% Difference = 3.8 (95% CI: 0.6, 8.1) †† | NR | NR | NR | NR | NR |
| A | Improving patient quality of life with transition from goserelin 3.6 mg monthly to 10.8 mg LA every 3 months |
| A 39-year old premenopausal woman with a post-partum tumor stage pT2 (28 mm), lymph node stage N1a (2/5 nodes involved), no evidence of distant metastases (M0) grade 2 ER (>90%)/PR (80%)-positive, HER2-negative, Ki-67 18%, extensive LVI and PNI positive, invasive ductal carcinoma of the breast. She was treated with adjuvant ddACT chemotherapy, OFS with goserelin 3.6 mg SC monthly, AI therapy with letrozole, zoledronic acid and adjuvant radiotherapy. Subsequently began adjuvant CDK4/6 inhibitor therapy with ribociclib. After 3 months on ribociclib, she returned to work on a progressive schedule. She found it challenging to go back to being a full time working mom and coming in for monthly appointments. After 1 year of goserelin 3.6 mg SC with established ovarian function suppression biochemically based on FSH and E2, she was transitioned to 10.8 mg SC every 12 weeks. She feels much happier with this schedule and reports an improvement in quality of life as a result, with less stress and fewer visits to the cancer center. Consideration can be made for the home injection program for further alleviation of burden on the patient. | |
| B | Initiating OFS with goserelin 10.8 mg LA every 3 months |
| A 47-year-old premenopausal woman who presented with a self-detected left-sided clinical tumor stage T3, lymph node negative (N0), grade 1, ER (>90%)/PR (>90%)-positive, HER2-negative, Ki-67 low 5%, invasive lobular carcinoma of the breast. It measured 5.1 cm in maximal dimension on clinical examination, although the breast magnetic resonance imaging suggested an extent of over 7.1 cm. There were additional microcalcifications in the right breast. She elected to have bilateral mastectomies with immediate reconstruction. The final pathology revealed pT3N2a, grade 2 (mitotic rate 1), 39 mm, 19 mm and 12 mm foci of invasive lobular carcinoma which were adjacent and represented an aggregate of 7 cm of disease with 4/12 nodes involved (10 mm deposit, no ENE). Final surgical margins were positive in the anterior and superior, with LVI present. Staging computed tomography of the chest, abdomen, pelvis revealed no abnormalities. The patient completed adjuvant chemotherapy with the ddACT protocol. Locoregional radiotherapy was completed in March 2023. She started OFS with goserelin 10.8 mg SC, and 4 weeks later added AI therapy with letrozole and then adjuvant CDK4/6 inhibitor therapy with abemaciclib. She had regular monthly menstrual cycles and no symptoms to suggest perimenopausal state prior to presentation. While it is likely that she had chemotherapy-induced ovarian failure, it was decided to offer OFS but at the 10.8 mg dose upfront with iterative approach to add on nonsteroidal AI. Tamoxifen should be avoided with abemaciclib given the higher risk of venous thromboemlism and thus this was the best choice for the patient who also lives in a remote area with a long commute into town. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
LeVasseur, N.; Manna, M.; Jerzak, K.J. An Overview of Long-Acting GnRH Agonists in Premenopausal Breast Cancer Patients: Survivorship Challenges and Management. Curr. Oncol. 2024, 31, 4209-4224. https://doi.org/10.3390/curroncol31080314
LeVasseur N, Manna M, Jerzak KJ. An Overview of Long-Acting GnRH Agonists in Premenopausal Breast Cancer Patients: Survivorship Challenges and Management. Current Oncology. 2024; 31(8):4209-4224. https://doi.org/10.3390/curroncol31080314
Chicago/Turabian StyleLeVasseur, Nathalie, Mita Manna, and Katarzyna J. Jerzak. 2024. "An Overview of Long-Acting GnRH Agonists in Premenopausal Breast Cancer Patients: Survivorship Challenges and Management" Current Oncology 31, no. 8: 4209-4224. https://doi.org/10.3390/curroncol31080314
APA StyleLeVasseur, N., Manna, M., & Jerzak, K. J. (2024). An Overview of Long-Acting GnRH Agonists in Premenopausal Breast Cancer Patients: Survivorship Challenges and Management. Current Oncology, 31(8), 4209-4224. https://doi.org/10.3390/curroncol31080314