Evaluation of Tumor Control and Normal Tissue Complication Probabilities in Patients Receiving Comprehensive Nodal Irradiation for Left-Sided Breast Cancer

Abstract

1. Introduction
2. Materials and Methods
2.1. Simulation Procedure
2.2. Contouring Process
2.3. Radiotherapy Planning and Dosimetric Evaluation
2.4. Radiobiological Assessment
2.5. Statistical Analysis
3. Results
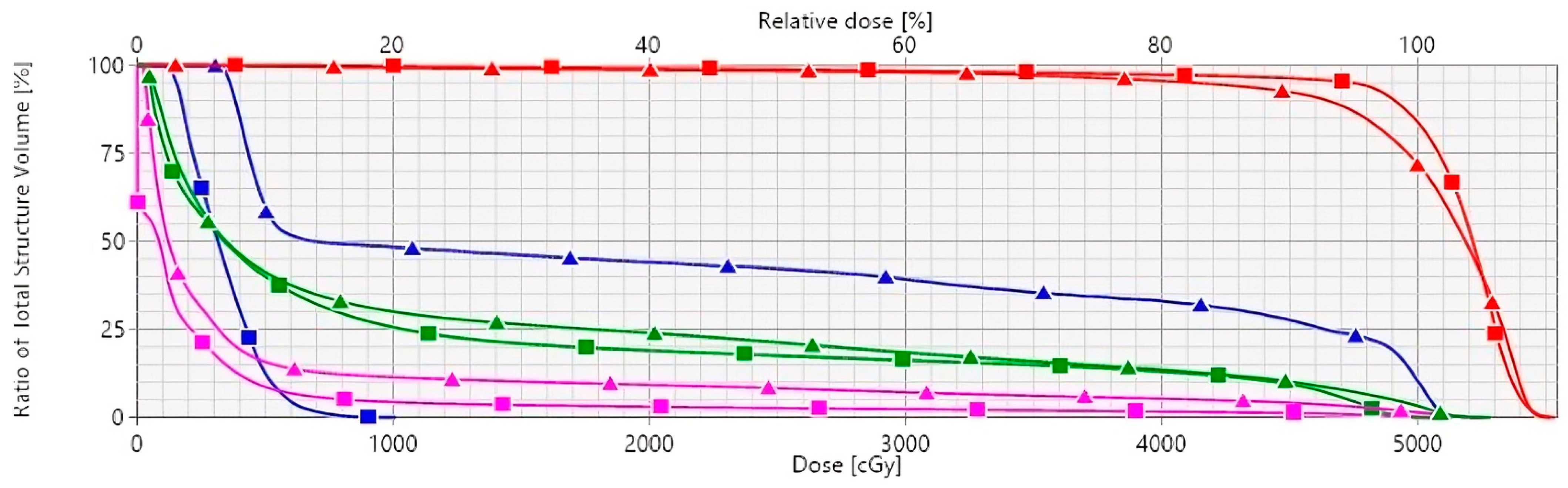
3.1. Plan Comparison and DVH Evaluation
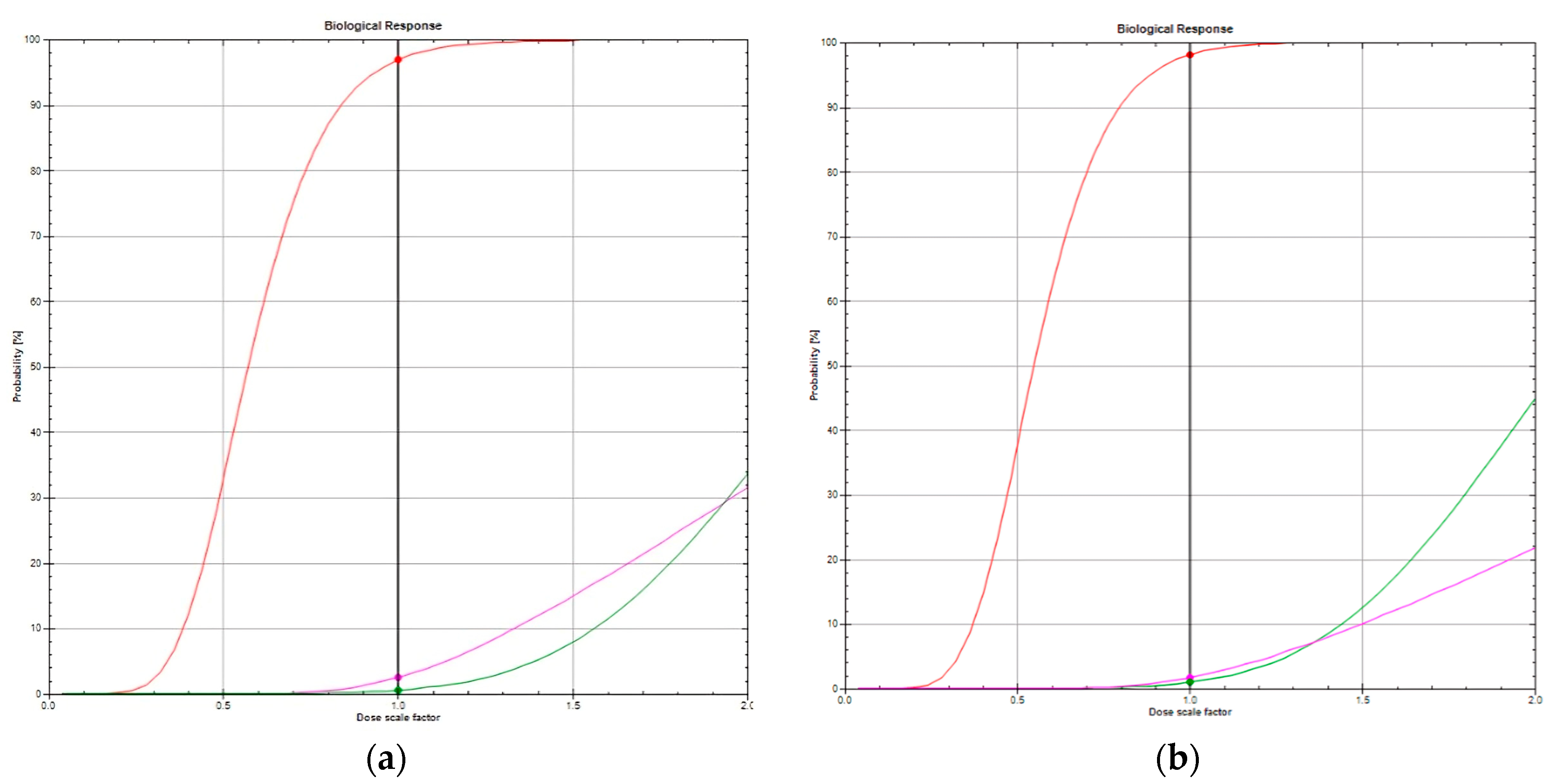
3.2. TCP and NTCP Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wheeler, S.B.; Rocque, G.; Basch, E. Benefits of Breast Cancer Screening and Treatment on Mortality. JAMA 2024, 331, 199–200. [Google Scholar] [CrossRef]
- Kolářová, I.; Melichar, B.; Sirák, I.; Vaňásek, J.; Petera, J.; Horáčková, K.; Pohanková, D.; Ďatelinka, F.; Šinkorová, Z.; Vošmik, M. The Role of Adjuvant Radiotherapy in the Treatment of Breast Cancer. Curr. Oncol. 2024, 31, 1207–1220. [Google Scholar] [CrossRef]
- Stefan, M.F.; Herghelegiu, C.G.; Magda, S.L. Accelerated Atherosclerosis and Cardiovascular Toxicity Induced by Radiotherapy in Breast Cancer. Life 2023, 13, 1631. [Google Scholar] [CrossRef]
- Stowe, H.B.; Andruska, N.D.; Reynoso, F.; Thomas, M.; Bergom, C. Heart Sparing Radiotherapy Techniques in Breast Cancer: A Focus on Deep Inspiration Breath Hold. Breast Cancer Targets Ther. 2022, 14, 175–186. [Google Scholar] [CrossRef]
- Fletcher, G.H. Keynote address: The scientific basis of the present and future practice of clinical radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 1983, 9, 1073–1082. [Google Scholar] [CrossRef]
- Lyman, J.T. Complication probability as assessed from dose-volume histograms. Radiat. Res. 1985, 8, S13–S19. [Google Scholar] [CrossRef]
- Källman, P.; Agren, A.; Brahme, A. Tumour and normal tissue responses to fractionated non-uniform dose delivery. Int. J. Radiat. Biol. 1992, 62, 249–262. [Google Scholar] [CrossRef]
- Edvardsson, A.; Nilsson, M.P.; Amptoulach, S.; Ceberg, S. Comparison of doses and NTCP to risk organs with enhanced inspiration gating and free breathing for left-sided breast cancer radiotherapy using the AAA algorithm. Radiat. Oncol. 2015, 10, 84. [Google Scholar] [CrossRef]
- Ko, H.; Chang, J.S.; Moon, J.Y.; Lee, W.H.; Shah, C.; Shim, J.S.A.; Han, M.C.; Baek, J.G.; Park, R.H.; Kim, Y.B.; et al. Dosimetric Comparison of Radiation Techniques for Comprehensive Regional Nodal Radiation Therapy for Left-Sided Breast Cancer: A Treatment Planning Study. Front. Oncol. 2021, 11, 645328. [Google Scholar] [CrossRef]
- Semenenko, V.A.; Li, X.A. Lyman-Kutcher-Burman NTCP model parameters for radiation pneumonitis and xerostomia based on combined analysis of published clinical data. Phys. Med. Biol. 2008, 53, 737–755. [Google Scholar] [CrossRef]
- Haviland, J.S.; Owen, J.R.; Dewar, J.A.; Agrawal, R.K.; Barrett, J.; Barrett-Lee, P.J.; Dobbs, H.J.; Hopwood, P.; Lawton, P.A.; Magee, B.J.; et al. The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol. 2013, 14, 1086–1094. [Google Scholar] [CrossRef]
- Warkentin, B.; Stavrev, P.; Stavreva, N.; Field, C.; Fallone, B.G. A TCP-NTCP estimation module using DVHs and known radiobiological models and parameter sets. J. Appl. Clin. Med. Phys. 2004, 5, 50–63. [Google Scholar] [CrossRef] [PubMed]
- Okunieff, P.; Morgan, D.; Niemierko, A.; Suit, H.D. Radiation dose-response of human tumors. Int. J. Radiat. Oncol. Biol. Phys. 1995, 32, 1227–1237. [Google Scholar] [CrossRef]
- Gagliardi, G.; Lax, I.; Ottolenghi, A.; Rutqvist, L.E. Long-term cardiac mortality after radiotherapy of breast cancer—Application of the relative seriality model. Br. J. Radiol. 1996, 69, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Hedin, E.; Bäck, A. Influence of different dose calculation algorithms on the estimate of NTCP for lung complications. J. Appl. Clin. Med. Phys. 2013, 14, 127–139. [Google Scholar] [CrossRef] [PubMed]
- Vasiljevic, D.; Arnold, C.; Neuman, D.; Fink, K.; Popovscaia, M.; Kvitsaridze, I.; Nevinny-Stickel, M.; Glatzer, M.; Lukas, P.; Seppi, T. Occurrence of pneumonitis following radiotherapy of breast cancer—A prospective study. Häufigkeit einer Pneumonitis nach Bestrahlung bei Brustkrebs –Eine prospektive Studie. Strahlenther. Onkol. 2018, 194, 520–532. [Google Scholar] [CrossRef]
- Terry, M.B.; Colditz, G.A. Epidemiology and Risk Factors for Breast Cancer: 21st Century Advances, Gaps to Address through Interdisciplinary Science. Cold Spring Harb. Perspect. Med. 2023, 13, a041317. [Google Scholar] [CrossRef]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef] [PubMed]
- Henson, K.E.; McGale, P.; Darby, S.C.; Parkin, M.; Wang, Y.; Taylor, C.W. Cardiac mortality after radiotherapy, chemotherapy and endocrine therapy for breast cancer: Cohort study of 2 million women from 57 cancer registries in 22 countries. Int. J. Cancer 2020, 147, 1437–1449. [Google Scholar] [CrossRef]
- Käsmann, L.; Dietrich, A.; Staab-Weijnitz, C.A.; Manapov, F.; Behr, J.; Rimner, A.; Jeremic, B.; Senan, S.; De Ruysscher, D.; Lauber, K.; et al. Radiation-induced lung toxicity—Cellular and molecular mechanisms of pathogenesis, management, and literature review. Radiat. Oncol. 2020, 15, 214. [Google Scholar] [CrossRef]
- Gueiderikh, A.; Sarrade, T.; Kirova, Y.; De La Lande, B.; De Vathaire, F.; Auzac, G.; Martin, A.L.; Everhard, S.; Meillan, N.; Bourgier, C.; et al. Radiation-induced lung injury after breast cancer treatment: Incidence in the CANTO-RT cohort and associated clinical and dosimetric risk factors. Front. Oncol. 2023, 13, 1199043. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.; Collins, R.; Darby, S.; Davies, C.; Elphinstone, P.; Evans, V.; Godwin, J.; Gray, R.; Hicks, C.; James, S.; et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 366, 2087–2106. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, A.A.; Sadaka, E.A.; Abouegylah, M.; Amin, S.A.; Elmansy, H.; Asal, M.F.; Köksal, M.A.; Gawish, A. Impact of breath-hold technique on incidence of cardiac events in adjuvant left breast cancer irradiation. J. Cancer Res. Clin. Oncol. 2023, 149, 5853–5859. [Google Scholar] [CrossRef] [PubMed]
- Tommasino, F.; Nahum, A.; Cella, L. Increasing the power of tumour control and normal tissue complication probability modelling in radiotherapy: Recent trends and current issues. Transl. Cancer Res. 2017, 6 (Suppl. 5), S807–S821. [Google Scholar] [CrossRef]
- Utehina, O.; Popovs, S.; Purina, D.; Slosberga, I.; Vevere, I.; Emzins, D.; Berzins, J.; Valuckas, K.P.; Janulionis, E.; Miller, A. Analysis of cardiac and pulmonary complication probabilities after radiation therapy for patients with early-stage breast cancer. Medicina 2009, 45, 276–285. [Google Scholar] [CrossRef]
- Kargar, N.; Zeinali, A.; Molazadeh, M. Impact of Dose Calculation Algorithms and Radiobiological Parameters on Prediction of Cardiopulmonary Complications in Left Breast Radiation Therapy. J. Biomed. Phys. Eng. 2024, 14, 129–140. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Radiobiological Evaluation | Dosimetric Parameters | ||
|---|---|---|---|
| Tumor Control Probability [13,14,15] | D50 * | γ ** | s *** |
| Adjuvant pT1-pT2 | 39.89 Gy | 1.3%/% | - |
| Adjuvant pT3 | 42.46 Gy | 0.53%/% | - |
| Adjuvant pN1 | 24.55 Gy | 1.07%/% | - |
| Adjuvant pN2 | 43.40 Gy | 0.68%/% | - |
| Adjuvant pN3 | 50.03 Gy | 2.63%/% | - |
| Normal Tissue Control Probability for Cardiac Death Risk [13,14] | |||
| Entire Heart Volume | 52.3 Gy | 1.28%/% | 1 |
| Normal Tissue Control Probability for Radiation Pneumonitis [15,16] | |||
| Whole Left Lung | 29.23 Gy | 0.966%/% | 0.012 |
| Patient and Treatment Characteristics | Distribution and % |
|---|---|
| Median Age (years), range | 50 (35–80) |
| Hormonal Status Premenopausal Postmenopausal | 8 (36.4) 14 (63.6) |
| AJCC Stage IIA IIB IIIA IIIB IIIC | 6 (27.3) 8 (36.4) 4 (18.2) 2 (9.1) 2 (9.1) |
| Nodal Status Nx N0 N1 N2 N3 | 1 (4.6) 4 (18.6) 13 (58.6) 1 (4.6) 3 (13.6) |
| Tumor Location within the Left Breast Upper Inner Quadrant Lower Inner Quadrant Upper Outer Quadrant Lower Outer Quadrant | 8 (36.4) 9 (40.9) 3 (13.6) 2 (9.1) |
| Molecular Classification Luminal A Luminal B Pure Her2 Triple Negative | 5 (22.7) 9 (40.9) 3 (13.6) 5 (22.7) |
| Histology Ductal Invasive Lobular Invasive | 20 (90.9) 2 (9.1) |
| Grade 1 2 3 N/R | 2 (9.1) 9 (40.9) 9 (40.9) 2 (9.1) |
| Type of Surgery Breast-Conserving + Sentinel Node Procedure Mastectomy + Axillary Dissection | 9 (40.9) 13 (59.1) |
| Radiation Treatment Fields Breast + Supraclavicular + Internal Mammary Chest Wall + Supraclavicular + Internal Mammary | 9 (40.9) 13 (59.1) |
| Timing of Chemotherapy Neoadjuvant Adjuvant | 12 (54.5) 10 (45.5) |
| Systemic Treatment Doxorubicin + Cyclophosphamide followed by Paclitaxel Docetaxel + Cyclophosphamide Capecitabine | 19 (86.4) 2 (9.1) 1 (4.6) |
| Adjuvant Endocrine Therapy Yes No | 14 (63.6) 8 (36.4) |
| Parameters | FB (Median and SD) | DIBH (Median and SD) | p-Value |
|---|---|---|---|
| Target Volume V95 (%) V105 (%) V107 (%) D2 (Gy) D98 (Gy) Dmean (Gy) CI HI | 89.0 ± 5.9 35.1 ± 13.7 14.2 ± 11.2 54.5 ± 0.5 41.1 ± 4.2 50.7 ± 0.8 0.7 ± 0.1 0.2 ± 0.1 | 90.3 ± 4.1 38.0 ± 14.5 18.8 ± 12.9 54.5 ± 0.8 41.6 ± 4.5 51.0 ± 0.7 0.8 ± 0.1 0.2 ± 0.1 | 0.390 0.115 0.217 0.961 0.417 0.026 0.198 0.794 |
| Left Lung Dose V5 (%) V10 (%) V20 (%) V30 (%) Dmean (Gy) Dmax (Gy) Total Volume | 43.9 ± 9.1 30.3 ± 7.5 23.6 ± 6.5 19.8 ± 5.9 12.5± 8.7 52.5 ± 1.3 1133.7 ± 240.1 | 43.1 ±7.6 28.5 ± 6.0 21.1 ± 4.9 17.8 ± 4.1 12.0 ± 2.3 52.4 ± 1.2 1919.2 ± 364.4 | 0.638 0.095 0.036 0.016 0.067 0.130 <0.001 |
| Heart V5 (%) V10 (%) V15 (%) V20 (%) V25 (%) V30 (%) V40 (%) V50 (%) Dmean (Gy) Dmax (Gy) | 14.3 ± 6.1 9.4 ± 5.3 8.3 ± 4.9 6.8 ± 4.8 5.8 ± 4.6 5.3 ± 4.4 3.9 ± 3.9 0.4 ± 1.4 4.3 ± 2.3 51.8 ± 1.6 | 6.6 ± 4.7 3.8 ± 3.4 2.8 ± 2.9 2.2 ± 2.6 2.2 ± 2.4 1.9 ± 2.0 1.2 ± 1.4 0 ± 0.3 2.4 ± 1.2 50.3 ± 10.4 | <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 0.003 <0.001 <0.001 <0.001 |
| LAD V5 (%) V10 (%) V25 (%) Dmean (Gy) Dmax (Gy) | 80.6 ± 26.8 60.6 ± 34.6 43.1 ± 33.3 23.2 ± 13.3 49.5 ± 13.1 | 56.5 ± 26.1 8.6 ± 25.8 0 ± 22.9 6.2 ± 8.4 24.5 ± 15.8 | 0.014 <0.001 <0.001 <0.001 <0.001 |
| Parameters | FB | DIBH | p-Value |
|---|---|---|---|
| Tumor Control Probability | 91.5 [7.8–98.3] | 93.5 [20.9–98.3] | 0.006 |
| Cardiac Death Risk | 1.0 [0.1–5.7] | 0.45 [0–2.4] | <0.001 |
| Risk of Radiation Pneumonitis | 1.2 [0–4.6] | 1.1 [0–3.9] | 0.237 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flores-Balcázar, C.H.; Urías-Arce, D.M. Evaluation of Tumor Control and Normal Tissue Complication Probabilities in Patients Receiving Comprehensive Nodal Irradiation for Left-Sided Breast Cancer. Curr. Oncol. 2024, 31, 3189-3198. https://doi.org/10.3390/curroncol31060241
Flores-Balcázar CH, Urías-Arce DM. Evaluation of Tumor Control and Normal Tissue Complication Probabilities in Patients Receiving Comprehensive Nodal Irradiation for Left-Sided Breast Cancer. Current Oncology. 2024; 31(6):3189-3198. https://doi.org/10.3390/curroncol31060241
Chicago/Turabian StyleFlores-Balcázar, Christian H., and Dulce M. Urías-Arce. 2024. "Evaluation of Tumor Control and Normal Tissue Complication Probabilities in Patients Receiving Comprehensive Nodal Irradiation for Left-Sided Breast Cancer" Current Oncology 31, no. 6: 3189-3198. https://doi.org/10.3390/curroncol31060241
APA StyleFlores-Balcázar, C. H., & Urías-Arce, D. M. (2024). Evaluation of Tumor Control and Normal Tissue Complication Probabilities in Patients Receiving Comprehensive Nodal Irradiation for Left-Sided Breast Cancer. Current Oncology, 31(6), 3189-3198. https://doi.org/10.3390/curroncol31060241