177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: A Review of the Evidence and Implications for Canadian Clinical Practice

 , ,
, ,  ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
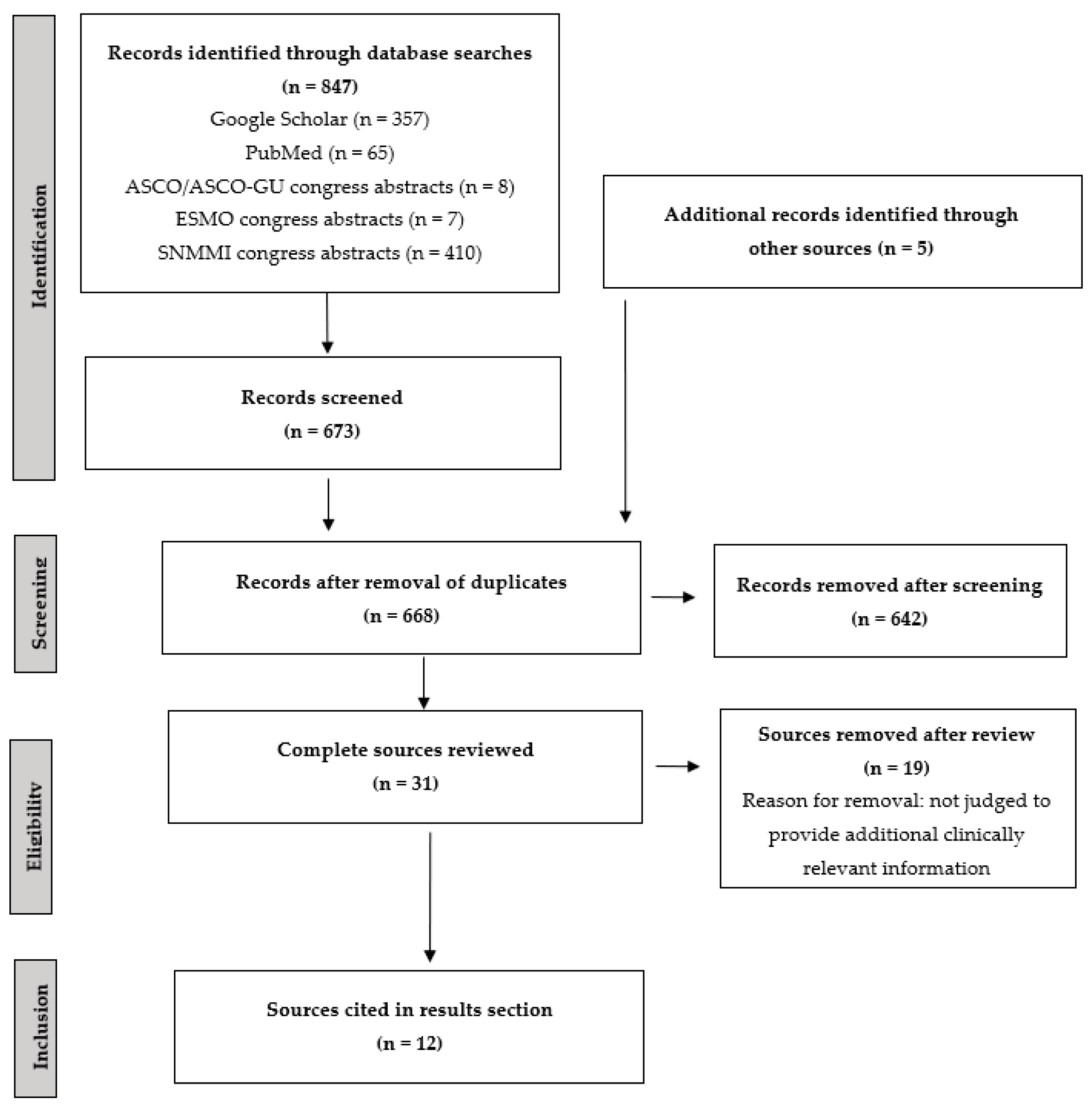
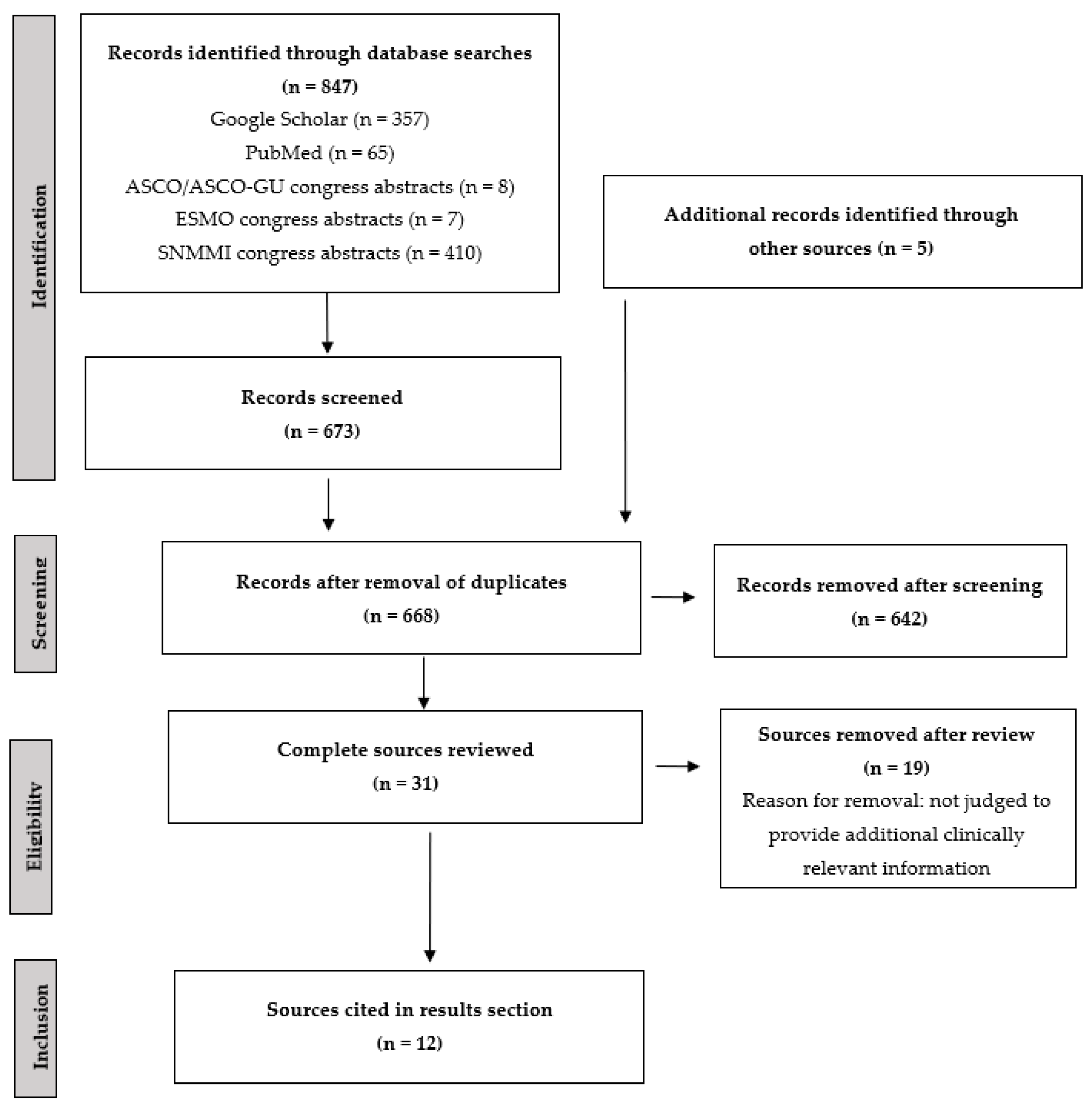
3.1. Results of Literature Review
3.2. Patients Treated with 177Lu-PSMA-617
3.3. Survival Outcomes with 177Lu-PSMA-617
3.4. Quality of Life with 177Lu-PSMA-617
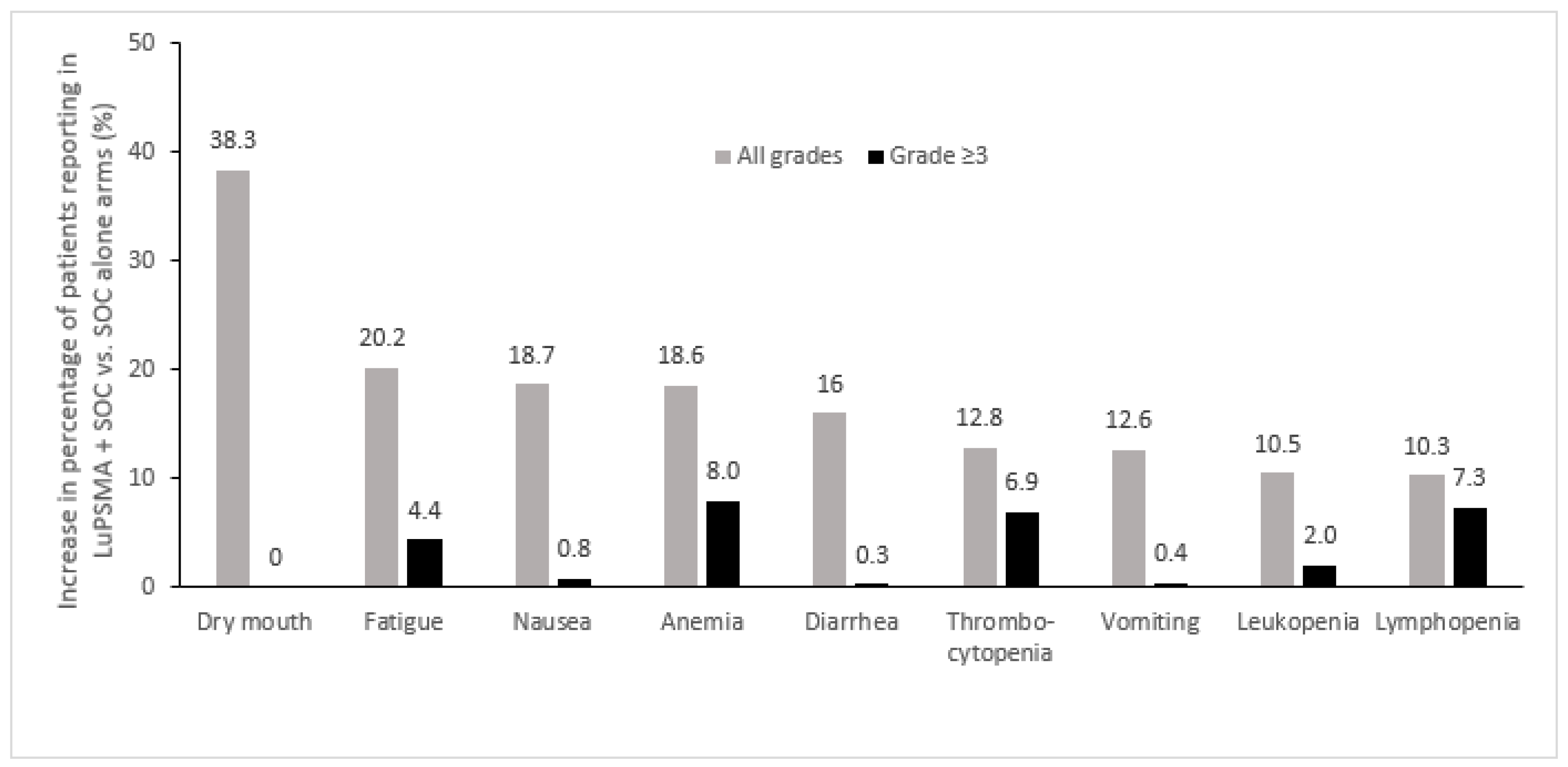
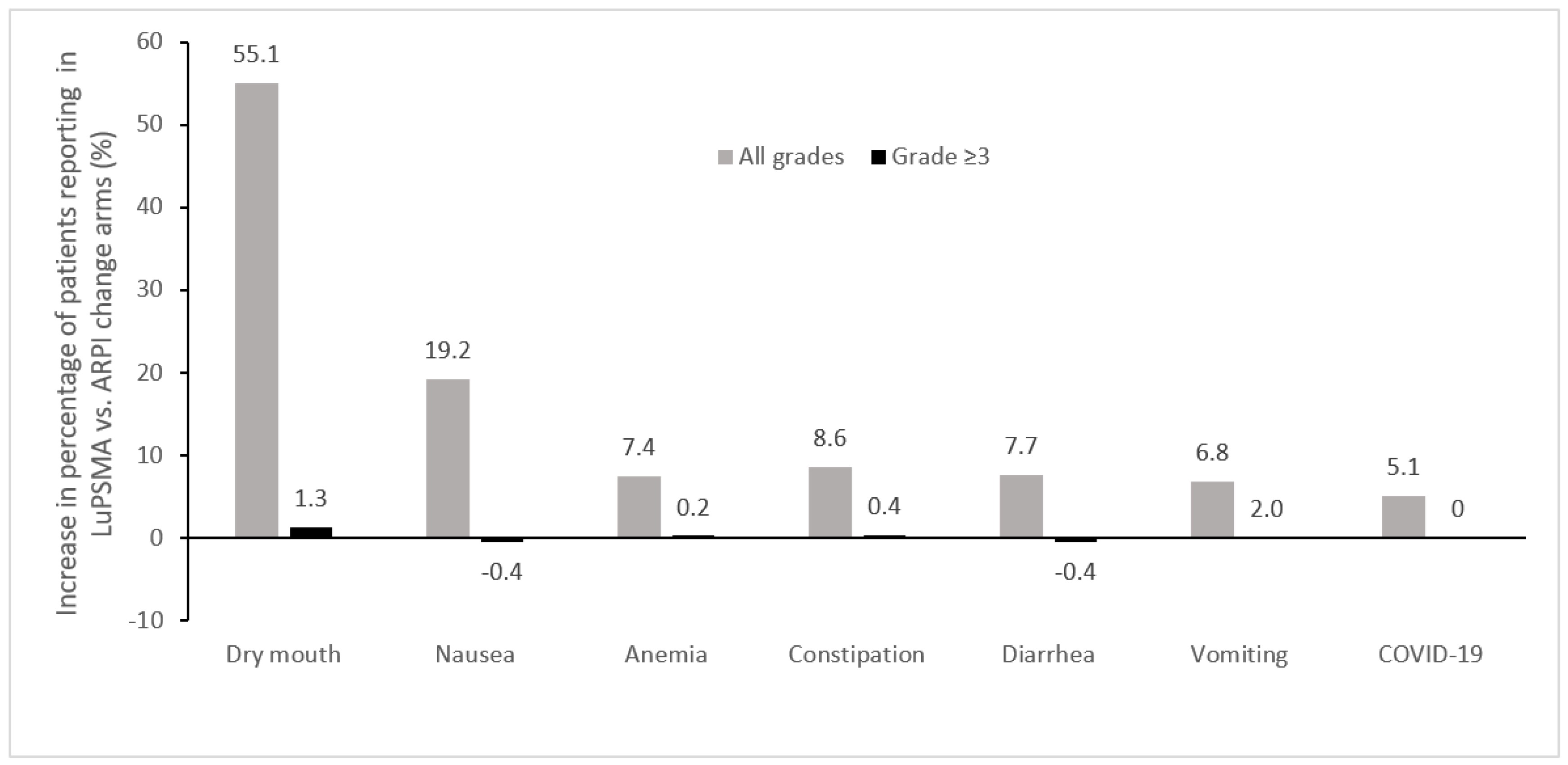
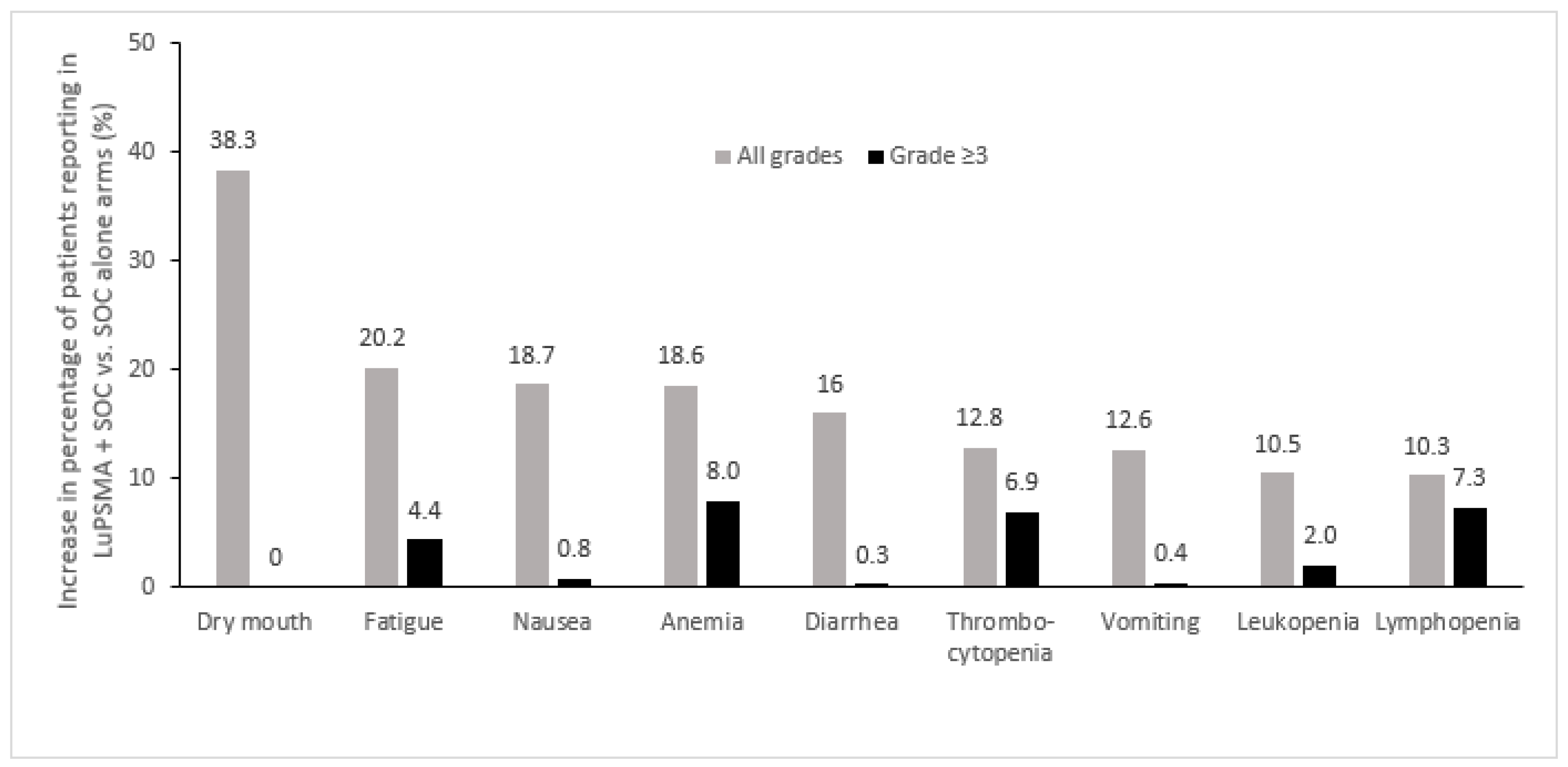
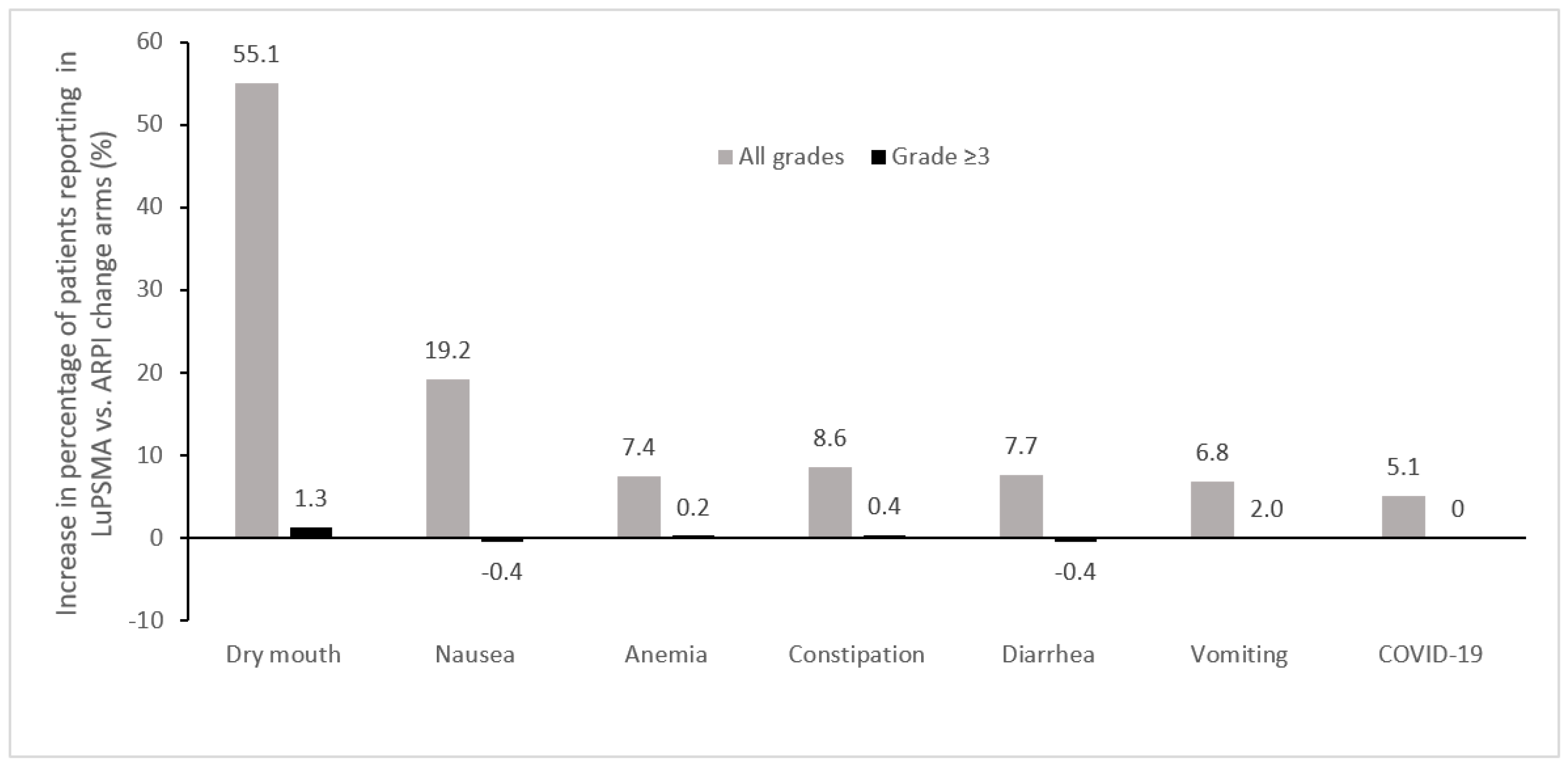
3.5. Adverse Events Associated with 177Lu-PSMA-617
4. Discussion
4.1. Treatment Sequencing and Patient Selection Criteria
4.2. Necessary Facilities for Treatment Procedures
4.3. Counselling Patients on the Practicalities of Administration
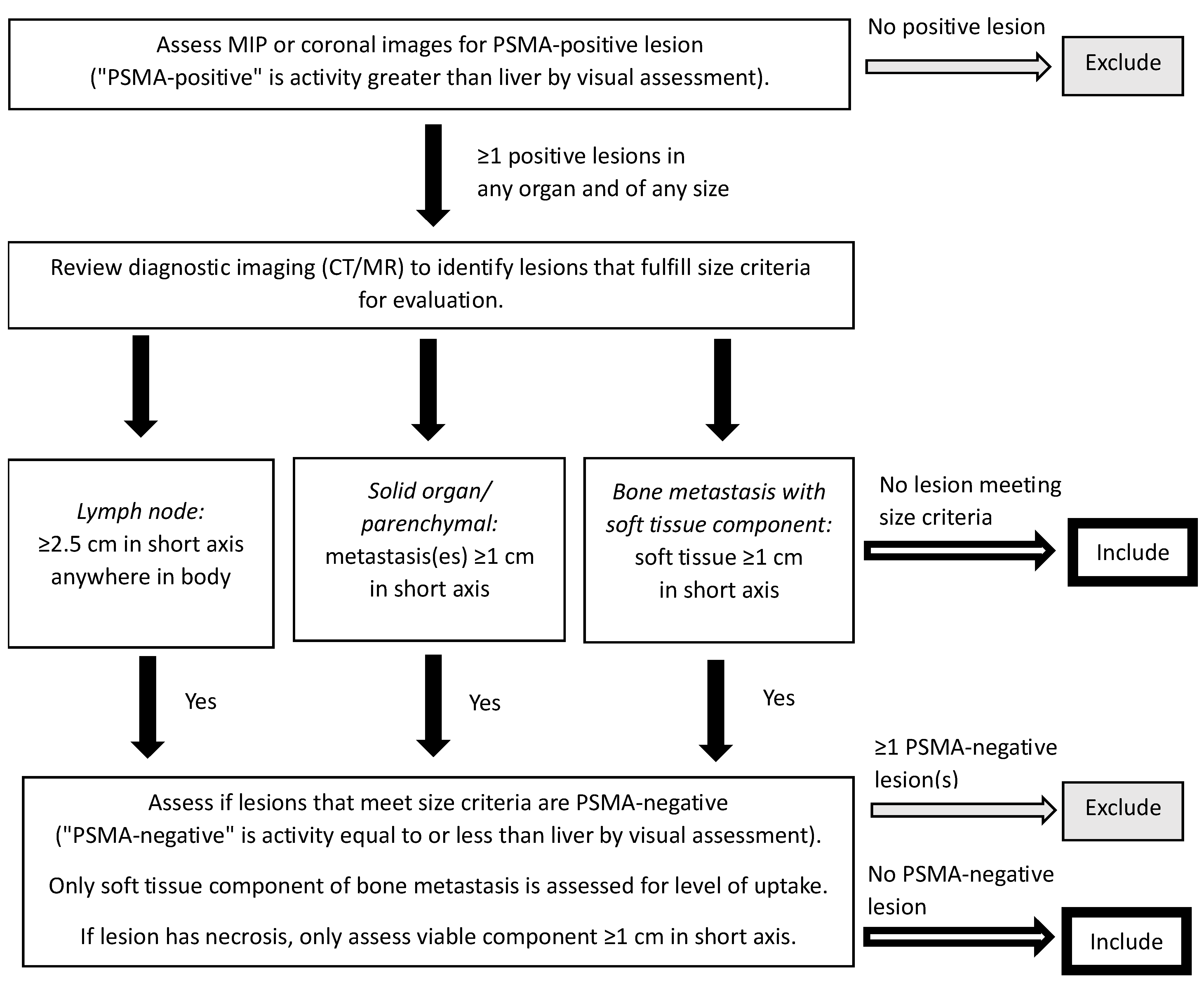
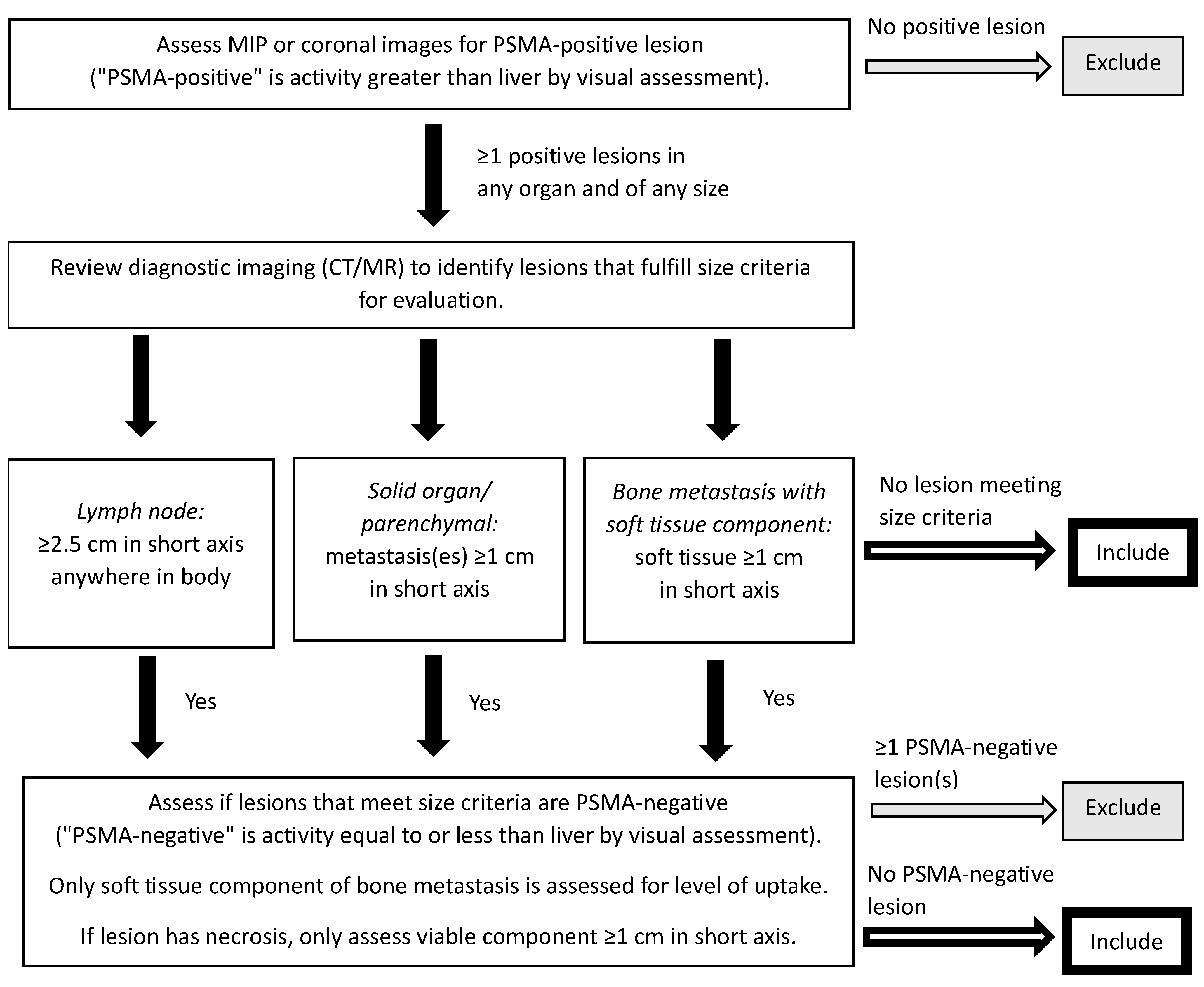
4.4. Assessment of Treatment Response
4.5. Management of Adverse Events
4.6. Ongoing Questions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Literature Search Strategy
- Objective: to identify clinical trials and observational studies on the use of 177Lu-PSMA-617 in patients with prostate cancer that were published in the literature within the last 10 years or presented at a major congress within the last 3 years.
- Searches conducted:
- ○
- Google Scholar
- ▪
- Search string: allintitle: (177Lu OR “lutetium-177” OR Lu OR lutetium) AND (PSMA OR “PSMA-617” OR “prostate specific membrane antigen” OR “vipivotide tetraxetan”)
- ▪
- Limits: 2013 or more recent; terms in title
- ○
- PubMed
- ▪
- Search string: (“prostate cancer” or “Prostatic Neoplasms” [Mesh]) AND (177Lu OR lutetium-177 OR Lu OR lutetium OR “Lutetium” [Mesh]) AND (PSMA OR PSMA-617 OR “prostate-specific membrane antigen” OR “vipivotide tetraxetan”)
- ▪
- Limits: English language; article types: case reports, clinical study, clinical trial, comparative study, meta-analysis, observational study, randomized controlled trial; 2013 or more recent
- ○
- ASCO database:
- ▪
- Search strings:
- 177Lu
- Lutetium
- ▪
- Limits: ASCO and ASCO-GU conferences; years 2020, 2021, 2022, and 2023; topic: prostate cancer
- ○
- ESMO database:
- ▪
- Search strings:
- 177Lu
- Lutetium
- ▪
- Limits: meeting resources; tumour site: prostate cancer; years 2020, 2021, 2022, and 2023
- ○
- SNMMI congress abstract supplements:
- ▪
- Search string: 177Lu OR lutetium
- ▪
- Years searched: 2020, 2021, 2022, and 2023.
Appendix B. 1777Lu-PSMA Therapy Instructions for Patients
Instructions
- Preferably, drive home alone after your treatment. If this is not possible, keep as much distance as possible between yourself and the driver.
- To minimize radiation exposure to other people, keep a maximum distance and a minimum exposure time between yourself and anyone else. Spend the least amount of time necessary in close contact (stay more than 2 m away) with other people for the next 3 days. For example, sleep alone for the first 3 nights.
- Avoid all contact with children less than 10 years of age for 7 days and with pregnant women for 15 days.
- You can return to daily activities or work as early as 3 days after treatment, while avoiding contact with pregnant women and children less than 10 years of age.
- Drink lots of water after the treatment and for the next 24 h (eight 8-ounce glasses).
- Always follow good hygiene practices. Take at least one shower per day. You must use toilet paper each time you urinate. Wash your hands thoroughly after using the toilet. You should sit while urinating to avoid splashing. Flush the toilet twice after each use for the first 24 h. Caregivers must wear disposable gloves for 3 days after treatment if there is a risk of contact with bodily fluids.
- If you have any nausea or vomiting, take the medication prescribed to you.
- If you are planning to travel outside of the country by any means or to go to an airport in the next 3 months, please inform the Nuclear Medicine Department and you will be provided with a document explaining the therapy you just received.
- Keep this document on you for the next week, and show it to your health care provider(s) should you require any urgent care in the next 7 days. Outside of working hours, health care providers can contact a nuclear medicine physician at TELEPHONE NUMBER.
- Should you have questions regarding your treatment, you can contact someone during working hours at the Department of Nuclear Medicine at TELEPHONE NUMBER.
References
- Canadian Cancer Statistics Advisory Committee; Canadian Cancer Society; Statistics Canada; Public Health Agency of Canada. Canadian Cancer Statistics 2021; Canadian Cancer Society: Toronto, ON, Canada, 2021; Available online: https://cancer.ca/en/research/cancer-statistics/canadian-cancer-statistics (accessed on 20 September 2023).
- Cancer Stat Facts: Prostate Cancer. Available online: https://seer.cancer.gov/statfacts/html/prost.html (accessed on 20 September 2023).
- Armstrong, A.J.; Lin, P.; Tombal, B.; Saad, F.; Higano, C.S.; Joshua, A.M.; Parli, T.; Rosbrook, B.; van Os, S.; Beer, T.M. Five-year survival prediction and safety outcomes with enzalutamide in men with chemotherapy-naïve metastatic castration-resistant prostate cancer from the PREVAIL trial. Eur. Urol. 2020, 78, 347–357. [Google Scholar] [CrossRef]
- Saad, F.; Efstathiou, E.; Attard, G.; Flaig, T.W.; Franke, F.; Goodman, O.B.; Oudard, S.; Steuber, T.; Suzuki, H.; Wu, D.; et al. Apalutamide plus abiraterone acetate and prednisone versus placebo plus abiraterone and prednisone in metastatic, castration-resistant prostate cancer (ACIS): A randomised, placebo-controlled, double-blind, multinational, phase 3 study. Lancet Oncol. 2021, 22, 1541–1559. [Google Scholar] [CrossRef]
- Morris, M.J.; Heller, G.; Hillman, D.W.; Bobek, O.; Ryan, C.; Antonarakis, E.S.; Bryce, A.H.; Hahn, O.; Beltran, H.; Armstrong, A.J.; et al. Randomized phase III study of enzalutamide compared with enzalutamide plus abiraterone for metastatic castration-resistant prostate cancer (Alliance A031201 trial). J. Clin. Oncol. 2023, 41, 3352–3362. [Google Scholar] [CrossRef]
- Clarke, N.W.; Armstrong, A.J.; Thiery-Vuillemin, A.; Oya, M.; Shore, N.D.; Procopio, G.; Guedes, J.D.C.; Arslan, C.; Mehra, N.; Parnis, F.; et al. Final overall survival (OS) in PROpel: Abiraterone (abi) and olaparib (ola) versus abiraterone and placebo (pbo) as first-line (1L) therapy for metastatic castration-resistant prostate cancer (mCRPC). In Proceedings of the 2023 ASCO Genitourinary Cancers Symposium, San Francisco, CA, USA, 16–18 February 2023. [Google Scholar]
- George, D.J.; Sartor, O.; Miller, K.; Saad, F.; Tombal, B.; Kalinovský, J.; Jiao, X.; Tangirala, K.; Sternberg, C.N.; Higano, C.S. Treatment patterns and outcomes in patients with metastatic castration-resistant prostate cancer in a real-world clinical practice setting in the United States. Clin. Genitourin. Cancer 2020, 18, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Paschalis, A.; Sheehan, B.; Riisnaes, R.; Rodrigues, D.N.; Gurel, B.; Bertan, C.; Ferreira, A.; Lambros, M.B.; Seed, G.; Yuan, W.; et al. Prostate-specific membrane antigen heterogeneity and DNA repair defects in prostate cancer. Eur. Urol. 2019, 76, 469–478. [Google Scholar] [CrossRef]
- Donin, N.M.; Reiter, R.E. Why targeting PSMA is a game changer in the management of prostate cancer. J. Nucl. Med. 2018, 59, 177–182. [Google Scholar] [CrossRef]
- Giraudet, A.L.; Kryza, D.; Hofman, M.; Moreau, A.; Fizazi, K.; Flechon, A.; Hicks, R.J.; Tran, B. PSMA targeting in metastatic castration-resistant prostate cancer: Where are we and where are we going? Ther. Adv. Med. Oncol. 2021, 13, 17588359211053898. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov Search Results. Available online: https://www.clinicaltrials.gov/search?cond=PROSTATE%20CANCER&term=radioligand&aggFilters=status:act%20rec%20not (accessed on 7 November 2023).
- Advanced Accelerator Applications USA, Inc. PLUVICTOTM (Lutetium [177Lu] Vipivotide Tetraxetan Injection) Product Monograph Including Patient Medication Information; Advanced Accelerator Applications USA, Inc.: Millburn, NJ, USA, 2022; Available online: https://pdf.hres.ca/dpd_pm/00067158.PDF (accessed on 20 September 2023).
- Hosono, M.; Ikebuchi, H.; Nakamura, Y.; Nakamura, N.; Yamada, T.; Yanagida, S.; Kitaoka, A.; Kojima, K.; Sugano, H.; Kinuya, S.; et al. Manual on the proper use of lutetium-177-labeled somatostatin analogue (Lu-177-DOTA-TATE) injectable in radionuclide therapy (2nd ed.). Ann. Nucl. Med. 2018, 32, 217–235. [Google Scholar] [CrossRef] [PubMed]
- Benešová, M.; Schäfer, M.; Bauder-Wüst, U.; Afshar-Oromieh, A.; Kratochwil, C.; Mier, W.; Haberkorn, U.; Kopka, K.; Eder, M. Preclinical evaluation of a tailor-made DOTA-conjugated PSMA inhibitor with optimized linker moiety for imaging and endoradiotherapy of prostate cancer. J. Nucl. Med. 2015, 56, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Haberkorn, U.; Giesel, F.; Morgenstern, A.; Kratochwil, C. The future of radioligand therapy: α, β, or both? J. Nucl. Med. 2017, 58, 1017–1018. [Google Scholar] [CrossRef] [PubMed]
- Ahmadzadehfar, H.; Rahbar, K.; Kürpig, S.; Bögemann, M.; Claesener, M.; Eppard, E.; Gärtner, F.; Rogenhofer, S.; Schäfers, M.; Essler, M. Early side effects and first results of radioligand therapy with 177Lu-DKFZ-617 PSMA of castrate-resistant metastatic prostate cancer: A two-centre study. EJNMMI Res. 2015, 5, 114. [Google Scholar] [CrossRef]
- Ahmadzadehfar, H.; Eppard, E.; Kürpig, S.; Fimmers, R.; Yordanova, A.; Schlenkhoff, C.D.; Gärtner, F.; Rogenhofer, S.; Essler, M. Therapeutic response and side effects of repeated radioligand therapy with 177Lu-PSMA-DKFZ-617 of castrate-resistant metastatic prostate cancer. Oncotarget 2016, 7, 12477–12488. [Google Scholar] [CrossRef]
- Kratochwil, C.; Giesel, F.L.; Stefanova, M.; Benešová, M.; Bronzel, M.; Afshar-Oromieh, A.; Mier, W.; Eder, M.; Kopka, K.; Haberkorn, U. PSMA-targeted radionuclide therapy of metastatic castration-resistant prostate cancer with Lu-177 labeled PSMA-617. J. Nucl. Med. 2016, 57, 1170–1176. [Google Scholar] [CrossRef]
- Rahbar, K.; Schmidt, M.; Heinzel, A.; Eppard, E.; Bode, A.; Yordanova, A.; Claesener, M.; Ahmadzadehfar, H. Response and tolerability of a single dose of 177Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer: A multicenter retrospective analysis. J. Nucl. Med. 2016, 57, 1334–1338. [Google Scholar] [CrossRef]
- Rahbar, K.; Bode, A.; Weckesser, M.; Avramovic, N.; Claesener, M.; Stegger, L.; Bögemann, M. Radioligand therapy with 177Lu-PSMA-617 as a novel therapeutic option in patients with metastatic castration resistant prostate cancer. Clin. Nucl. Med. 2016, 41, 522–528. [Google Scholar] [CrossRef]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schäfers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German multicenter study investigating 177Lu-PSMA-617 radioligand therapy in advanced prostate cancer patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef]
- Tagawa, S.T.; Vallabhajosula, S.; Christos, P.J.; Jhanwar, Y.S.; Batra, J.S.; Lam, L.; Osborne, J.; Beltran, H.; Molina, A.M.; Goldsmith, S.J.; et al. Phase 1/2 study of fractionated dose lutetium-177-labeled anti-prostate-specific membrane antigen monoclonal antibody J591 (177 Lu-J591) for metastatic castration-resistant prostate cancer. Cancer 2019, 125, 2561–2569. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Sartor, O.; De Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Advanced Accelerator Applications USA, Inc. PLUVICTOTM (Lutetium Lu 177 Vipivotide Tetraxetan) Injection, for Intravenous Use Full Prescribing Information; Advanced Accelerator Applications USA, Inc.: Millburn, NJ, USA, 2022. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/215833s000lbl.pdf (accessed on 20 September 2023).
- Novartis Europharm Limited. PLUVICTOTM (Lutetium [177Lu] Vipivotide Tetraxetan) Summary of Product Characteristics; Novartis Europharm Limited: Dublin, Ireland, 2023; Available online: https://www.ema.europa.eu/en/documents/product-information/pluvicto-epar-product-information_en.pdf (accessed on 20 September 2023).
- Sartor, O.; Gauna, D.C.; Herrmann, K.; de Bono, J.S.; Shore, N.D.; Chi, K.N.N.; Crosby, M.; Rodriguez, J.P.; Flechon, A.; Wei, X.X.; et al. Phase 3 trial of [177Lu]Lu-PSMA-617 in taxane-naive patients with metastatic castration-resistant prostate cancer (PSMAfore). In Proceedings of the ESMO Congress 2023, Madrid, Spain, 20–24 October 2023. [Google Scholar]
- Saad, F.; Aprikian, A.; Finelli, A.; Fleshner, N.E.; Gleave, M.; Kapoor, A.; Niazi, T.; North, S.A.; Pouliot, F.; Rendon, R.A.; et al. 2022 Canadian Urological Association (CUA)-Canadian Uro Oncology Group (CUOG) guideline: Management of castration-resistant prostate cancer (CRPC). Can. Urol. Assoc. J. 2022, 16, E506–E515. [Google Scholar] [CrossRef] [PubMed]
- Canadian Agency for Drugs and Technologies in Health. CADTH reimbursement recommendation: Lutetium (177Lu) vipivotide tetraxetan (Pluvicto). Can. J. Health Technol. 2023, 3, 1–26. [Google Scholar]
- Sadaghiani, M.S.; Sheikhbahaei, S.; Werner, R.A.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A.; Solnes, L.B.; Rowe, S.P. 177Lu-PSMA radioligand therapy effectiveness in metastatic castration-resistant prostate cancer: An updated systematic review and meta-analysis. Prostate 2022, 82, 826–835. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Bauman, G.; von Eyben, R.; Rahbar, K.; Soydal, C.; Haug, A.R.; Virgolini, I.; Kulkarni, H.; Baum, R.; Paganelli, G. Optimizing PSMA radioligand therapy for patients with metastatic castration-resistant prostate cancer. A systematic review and meta-analysis. Int. J. Mol. Sci. 2020, 21, 9054. [Google Scholar] [CrossRef] [PubMed]
- Satapathy, S.; Sahoo, R.K.; Bal, C. [177Lu]Lu-PSMA-radioligand therapy efficacy outcomes in taxane-naïve versus taxane-treated patients with metastatic castration-resistant prostate cancer: A systematic review and metaanalysis. J. Nucl. Med. 2023, 64, 1266–1271. [Google Scholar] [CrossRef]
- Fizazi, K.; Herrmann, K.; Krause, B.J.; Rahbar, K.; Chi, K.N.; Morris, M.J.; Sartor, O.; Tagawa, S.T.; Kendi, A.T.; Vogelzang, N.; et al. Health-related quality of life and pain outcomes with [177Lu]Lu-PSMA-617 plus standard of care versus standard of care in patients with metastatic castration-resistant prostate cancer (VISION): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2023, 24, 597–610. [Google Scholar] [CrossRef]
- Satapathy, S.; Mittal, B.R.; Sood, A. Visceral metastases as predictors of response and survival outcomes in patients of castration-resistant prostate cancer treated with 177Lu-labeled prostate-specific membrane antigen radioligand therapy: A systematic review and meta-analysis. Clin. Nucl. Med. 2020, 45, 935–942. [Google Scholar] [CrossRef]
- Vaishampayan, N.; Morris, M.J.; Krause, B.J.; Vogelzang, N.J.; Kendi, A.T.; Nordquist, L.T.; Calais, J.; Nagarajah, J.; Beer, T.M.; El-Haddad, G.; et al. [177Lu]Lu-PSMA-617 in PSMA-positive metastatic castration-resistant prostate cancer: Prior and concomitant treatment subgroup analyses of the VISION trial. In Proceedings of the 2022 ASCO Annual Meeting, Chicago, IL, USA, 3–7 June 2022. [Google Scholar]
- Buteau, J.P.; Martin, A.J.; Emmett, L.; Iravani, A.; Sandhu, S.; Joshua, A.M.; Francis, R.J.; Zhang, A.Y.; Scott, A.M.; Lee, S.T.; et al. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): A biomarker analysis from a randomised, open-label, phase 2 trial. Lancet Oncol. 2022, 23, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Kuo, P.; Hesterman, J.; Rahbar, K.; Kendi, A.T.; Wei, X.X.; Fang, B.; Adra, N.; Armstrong, A.J.; Garje, R.; Michalski, J.M.; et al. [68Ga]Ga-PSMA-11 PET baseline imaging as a prognostic tool for clinical outcomes to [177Lu]Lu-PSMA-617 in patients with mCRPC: A VISION substudy. In Proceedings of the 2022 ASCO Annual Meeting, Chicago, IL, USA, 3–7 June 2022. [Google Scholar]
- Gafita, A.; Calais, J.; Grogan, T.R.; Hadaschik, B.; Wang, H.; Weber, M.; Sandhu, S.; Kratochwil, C.; Esfandiari, R.; Tauber, R.; et al. Nomograms to predict outcomes after 177Lu-PSMA therapy in men with metastatic castration-resistant prostate cancer: An international, multicentre, retrospective study. Lancet Oncol. 2021, 22, 1115–1125. [Google Scholar] [CrossRef]
- Tagawa, S.T.; Armstrong, A.J.; Krause, B.J.; Herrmann, K.; Rahbar, K.; De Bono, J.S.; Adra, N.; Desilvio, M.; Messmann, R.; Holder, G.; et al. Tolerability of [177Lu]Lu-PSMA-617 by treatment exposure in patients with metastatic castration-resistant prostate cancer (mCRPC): A VISION study subgroup analysis. In Proceedings of the 2022 ASCO Annual Meeting, Chicago, IL, USA, 3–7 June 2022. [Google Scholar]
- Shayegan, B.; Wallis, C.J.; Malone, S.; Cagiannos, I.; Hamilton, R.J.; Ferrario, C.; Gotto, G.T.; Basappa, N.S.; Morgan, S.C.; Fernandes, R.; et al. Real-world use of systemic therapies in men with metastatic castration resistant prostate cancer (mCRPC) in Canada. Urol. Oncol. 2022, 40, 192.e1–192.e9. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Essler, M.; Eiber, M.; la Fougère, C.; Prasad, V.; Fendler, W.P.; Rassek, P.; Hasa, E.; Dittmann, H.; Bundschuh, R.A.; et al. 177Lu-prostate-specific membrane antigen therapy in patients with metastatic castration-resistant prostate cancer and prior 223Ra (RALU study). J. Nucl. Med. 2023, 64, 1925–1931. [Google Scholar] [CrossRef]
- Sartor, O.; la Fougère, C.; Essler, M.; Ezziddin, S.; Kramer, G.; Ellinger, J.; Nordquist, L.; Sylvester, J.; Paganelli, G.; Peer, A.; et al. 177Lu-prostate-specific membrane antigen ligand after 223Ra treatment in men with bone-metastatic castration-resistant prostate cancer: Real-world clinical experience. J. Nucl. Med. 2022, 63, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Fendler, W.P.; Eiber, M.; Hofman, M.S.; Emmett, L.; Calais, J.; Osborne, J.R.; Iravani, A.; Koo, P.; Lindenberg, L.; et al. Joint EANM/SNMMI procedure guideline for the use of 177Lu-labeled PSMA-targeted radioligand-therapy (177Lu-PSMA-RLT). Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 2830–2845. [Google Scholar] [CrossRef] [PubMed]
- Kuo, P.H.; Benson, T.; Messmann, R.; Groaning, M. Why we did what we did: PSMA PET/CT selection criteria for the VISION trial. J. Nucl. Med. 2022, 63, 816–818. [Google Scholar] [CrossRef] [PubMed]
- Seifert, R.; Telli, T.; Hadaschik, B.; Fendler, W.P.; Kuo, P.H.; Herrmann, K. Is 18F-FDG PET needed to assess 177Lu-PSMA therapy eligibility? A VISION-like, single-center analysis. J. Nucl. Med. 2023, 64, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Buatti, J.M.; Pryma, D.A.; Kiess, A.P.; Mailman, J.; Ennis, R.D.; Menda, Y.; White, G.A.; Pandit-Taskar, N. A framework for patient-centered pathways of care for radiopharmaceutical therapy: An ASTRO consensus document. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 913–922. [Google Scholar] [CrossRef]
- Straub, M.; Kupferschläger, J.; Higuita, L.M.S.; Weissinger, M.; Dittmann, H.; la Fougère, C.; Fiz, F. Dual-time-point posttherapy 177Lu-PSMA-617 SPECT/CT describes the uptake kinetics of mCRPC lesions and prognosticates patients’ outcome. J. Nucl. Med. 2023, 64, 1431–1438. [Google Scholar] [CrossRef]
- Pathmanandavel, S.; Crumbaker, M.; Ho, B.; Yam, A.O.; Wilson, P.; Niman, R.; Ayers, M.; Sharma, S.; Hickey, A.; Eu, P.; et al. Evaluation of 177Lu-PSMA-617 SPECT/CT quantitation as a response biomarker within a prospective 177Lu-PSMA-617 and NOX66 combination trial (LuPIN). J. Nucl. Med. 2023, 64, 221–226. [Google Scholar] [CrossRef]
- Jackson, P.A.; Hofman, M.S.; Hicks, R.J.; Scalzo, M.; Violet, J. Radiation dosimetry in 177Lu-PSMA-617 therapy using a single posttreatment SPECT/CT scan: A novel methodology to generate time- and tissue-specific dose factors. J. Nucl. Med. 2020, 61, 1030–1036. [Google Scholar] [CrossRef]
- Lantheus and POINT Biopharma Announce Positive Topline Results from Pivotal SPLASH Trial in Metastatic Castration-Resistant Prostate Cancer. Available online: https://www.globenewswire.com/en/news-release/2023/12/18/2797729/0/en/Lantheus-and-POINT-Biopharma-Announce-Positive-Topline-Results-from-Pivotal-SPLASH-Trial-in-Metastatic-Castration-Resistant-Prostate-Cancer.html (accessed on 21 December 2023).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TheraP [23] | VISION [24] | PSMAfore [27] | ||||
|---|---|---|---|---|---|---|
| Study type | Phase 2 | Phase 3 | Phase 3 | |||
| PSMA PET eligibility criteria | 68Ga-PSMA-11, SUVmax ≥ 20 at ≥1 disease site and >10 at all other metastatic disease sites | 68Ga-PSMA-11 uptake greater than liver parenchyma at ≥1 disease site and no PSMA-negative metastatic lesions | 68Ga-PSMA-11 uptake greater than liver parenchyma at ≥1 disease site and no PSMA-negative metastatic lesions | |||
| FDG PET eligibility criteria | No sites with discordant FDG-positive/PSMA-negative lesions | N/A | N/A | |||
| Study arms | LuPSMA | Cabazitaxel | LuPSMA | SOC | LuPSMA | ARPI change |
| Patients, n | 99 | 101 | 551 | 280 | 234 | 234 |
| Median age, years | 72.1 | 71.8 | 70.0 | 71.5 | 71 | 72 |
| ECOG PS 0 or 1, % | 96 | 96 | 92.6 | 92.1 | 99.1 | 97.9 |
| Median PSA level, μg/L | 93.5 | 110 | 77.5 | 74.6 | 18.4 | 14.9 |
| Median ALP level, IU/L | 111 | 130 | 105.0 | 94.5 | 100.0 | 103.5 |
| Disease sites, % | ||||||
| Bone | 90.9 | 89.1 | 91.5 | 91.4 | 87.6 | 86.8 |
| Liver | 7.11 1 | 12.91 1 | 11.4 | 13.6 | 5.6 | 3.0 |
| Lymph node | 52.5 | 46.5 | 49.7 | 50.4 | 32.5 | 31.6 |
| Previous treatments, % | ||||||
| ARPI | 92 | 90 | 100 | 100 | 100 | 100 |
| Cabazitaxel | 0 | 0 | 37.9 | 38.2 | 0 | 0 |
| Docetaxel | 100 | 100 | 96.9 | 97.5 | 0 | 0 |
| TheraP [23] | VISION [24,33] | PSMAfore [27] | ||||
|---|---|---|---|---|---|---|
| Study arms | LuPSMA | Cabazitaxel | LuPSMA | SOC | LuPSMA | ARPI Change |
| Patients, n | 99 | 101 | 551 | 280 | 234 | 234 |
| Median imaging-based PFS, months | NR | NR | 8.7 | 3.4 | 12.0 | 5.6 |
| HR (95% CI) p value | 0.63 (10.46–0.86) 0.0028 | 0.40 (0.29–0.57) <0.001 | 0.41 (0.33–0.54) <0.0001 | |||
| Median OS, months | NR | NR | 15.3 | 11.3 | 19.2 | 19.7 |
| HR (95% CI) p value | NR | 0.62 (0.52–0.75) <0.001 | 1.16 (0.83–1.64) NR | |||
|
Median time to HRQOL worsening, months 1 | NR | NR | 14.3 | 2.9 | 7.5 | 4.3 |
| HR (95% CI) p value | NR | 0.45 (0.33–0.60) <0.001 | 0.59 (0.47–0.72) NR | |||
|
Median time to pain worsening, months 2 | NR | NR | 1.0 | 0.5 | 5.0 | 3.7 |
| HR (95% CI) p value | NR | 0.65 (0.54–0.78) <0.001 | 0.69 (0.56–0.85) NR | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chi, K.N.; Yip, S.M.; Bauman, G.; Probst, S.; Emmenegger, U.; Kollmannsberger, C.K.; Martineau, P.; Niazi, T.; Pouliot, F.; Rendon, R.; et al. 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: A Review of the Evidence and Implications for Canadian Clinical Practice. Curr. Oncol. 2024, 31, 1400-1415. https://doi.org/10.3390/curroncol31030106
Chi KN, Yip SM, Bauman G, Probst S, Emmenegger U, Kollmannsberger CK, Martineau P, Niazi T, Pouliot F, Rendon R, et al. 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: A Review of the Evidence and Implications for Canadian Clinical Practice. Current Oncology. 2024; 31(3):1400-1415. https://doi.org/10.3390/curroncol31030106
Chicago/Turabian StyleChi, Kim N., Steven M. Yip, Glenn Bauman, Stephan Probst, Urban Emmenegger, Christian K. Kollmannsberger, Patrick Martineau, Tamim Niazi, Frédéric Pouliot, Ricardo Rendon, and et al. 2024. "177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: A Review of the Evidence and Implications for Canadian Clinical Practice" Current Oncology 31, no. 3: 1400-1415. https://doi.org/10.3390/curroncol31030106
APA StyleChi, K. N., Yip, S. M., Bauman, G., Probst, S., Emmenegger, U., Kollmannsberger, C. K., Martineau, P., Niazi, T., Pouliot, F., Rendon, R., Hotte, S. J., Laidley, D. T., & Saad, F. (2024). 177Lu-PSMA-617 in Metastatic Castration-Resistant Prostate Cancer: A Review of the Evidence and Implications for Canadian Clinical Practice. Current Oncology, 31(3), 1400-1415. https://doi.org/10.3390/curroncol31030106