Ablative or Surgical Treatment for Small Renal Masses (T1a): A Single-Center Comparison of Perioperative Morbidity and Complications

 , ,
, ,
Abstract

1. Introduction
2. Materials and Methods
2.1. Treatment Modalities
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.H.; Klatte, T.; Usher-Smith, J.; Stewart, G.D. Epidemiology and screening for renal cancer. World J. Urol. 2018, 36, 1341–1353. [Google Scholar] [CrossRef] [PubMed]
- Correa, R.J.M.; Louie, A.V.; Zaorsky, N.G.; Lehrer, E.J.; Ellis, R.; Ponsky, L.; Kaplan, I.; Mahadevan, A.; Chu, W.; Swaminath, A.; et al. The Emerging Role of Stereotactic Ablative Radiotherapy for Primary Renal Cell Carcinoma: A Systematic Review and Meta-Analysis. Eur. Urol. Focus. 2019, 5, 958–969. [Google Scholar] [CrossRef] [PubMed]
- Acosta Ruiz, V.; Batelsson, S.; Onkamo, E.; Wernroth, L.; Nilsson, T.; Lonnemark, M.; Dahlman, P.; Magnusson, A. Split renal function after treatment of small renal masses: Comparison between radiofrequency ablation and laparoscopic partial nephrectomy. Acta Radiol. 2021, 62, 1248–1256. [Google Scholar] [CrossRef] [PubMed]
- Chan, V.W.; Abul, A.; Osman, F.H.; Ng, H.H.; Wang, K.; Yuan, Y.; Cartledge, J.; Wah, T.M. Ablative therapies versus partial nephrectomy for small renal masses—A systematic review and meta-analysis. Int. J. Surg. 2022, 97, 106194. [Google Scholar] [CrossRef] [PubMed]
- Alam, R.; Patel, H.D.; Osumah, T.; Srivastava, A.; Gorin, M.A.; Johnson, M.H.; Trock, B.J.; Chang, P.; Wagner, A.A.; McKiernan, J.M.; et al. Comparative effectiveness of management options for patients with small renal masses: A prospective cohort study. BJU Int. 2019, 123, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Almdalal, T.; Sundqvist, P.; Harmenberg, U.; Hellstrom, M.; Lindskog, M.; Lindblad, P.; Lundstam, S.; Ljungberg, B. Clinical T1a Renal Cell Carcinoma, Not Always a Harmless Disease-A National Register Study. Eur. Urol. Open Sci. 2022, 39, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bedke, J.; Capitanio, U.; Dabestani, S.; Fernandez-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022, 82, 399–410. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Assel, M.; Sjoberg, D.; Elders, A.; Wang, X.; Huo, D.; Botchway, A.; Delfino, K.; Fan, Y.; Zhao, Z.; Koyama, T.; et al. Guidelines for Reporting of Statistics for Clinical Research in Urology. Eur. Urol. 2019, 75, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Abu-Ghanem, Y.; Fernandez-Pello, S.; Bex, A.; Ljungberg, B.; Albiges, L.; Dabestani, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. Limitations of Available Studies Prevent Reliable Comparison Between Tumour Ablation and Partial Nephrectomy for Patients with Localised Renal Masses: A Systematic Review from the European Association of Urology Renal Cell Cancer Guideline Panel. Eur. Urol. Oncol. 2020, 3, 433–452. [Google Scholar] [CrossRef] [PubMed]
- Atwell, T.D.; Carter, R.E.; Schmit, G.D.; Carr, C.M.; Boorjian, S.A.; Curry, T.B.; Thompson, R.H.; Kurup, A.N.; Weisbrod, A.J.; Chow, G.K.; et al. Complications following 573 percutaneous renal radiofrequency and cryoablation procedures. J. Vasc. Interv. Radiol. 2012, 23, 48–54. [Google Scholar] [CrossRef] [PubMed]
- El Dib, R.; Touma, N.J.; Kapoor, A. Cryoablation vs radiofrequency ablation for the treatment of renal cell carcinoma: A meta-analysis of case series studies. BJU Int. 2012, 110, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Faddegon, S.; Cadeddu, J.A. Does renal mass ablation provide adequate long-term oncologic control? Urol. Clin. North. Am. 2012, 39, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Musi, G.; Luzzago, S.; Mauri, G.; Mistretta, F.A.; Varano, G.M.; Vaccaro, C.; Guzzo, S.; Maiettini, D.; Di Trapani, E.; Della Vigna, P.; et al. Predicting Peri-Operative Outcomes in Patients Treated with Percutaneous Thermal Ablation for Small Renal Masses: The SuNS Nephrometry Score. Diagnostics 2023, 13, 2955. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.A.; Welch, B.T.; Schmit, G.D.; Schmitz, J.J.; Weisbrod, A.J.; Callstrom, M.R.; Welch, T.L.; Thompson, R.H.; Kurup, A.N.; Boorjian, S.A.; et al. Safety and Efficacy of Percutaneous Image-guided Cryoablation of Completely Endophytic Renal Masses. Urology 2019, 133, 151–156. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Open Technique (%) | Conventional Laparoscopy (%) | Robot-Assisted Laparoscopy (%) | |
|---|---|---|---|
| Partial nephrectomy (n = 207) | 57 (n = 118) | 26 (n = 53) | 17 (n = 36) |
| Total nephrectomy (n = 49) | 47 (n = 23) | 33 (n = 16) | 20 (n = 10) |
| Ablative Treatment (n = 188) | Surgical Treatment (n = 256) | X2 | |
|---|---|---|---|
| Active smoker (%) | 14 | 12 | 0.6 |
| Age (years) (range; mean) | 65–78; 73 | 54–73; 64 | <0.001 |
| Tumor size (mm) | 21 | 26 | <0.001 |
| BMI (mean) | 28 | 27 | 0.5 |
| ASA score (mean) | 2.6 | 2.0 | <0.001 |
| ECOG score (mean) | 1.3 | 0.6 | <0.001 |
| RENAL nephrometry score (%) | |||
| Low complexity (RS 4–6) | 60.1 (n = 113) | 50.0 (n = 128) | 0.15 |
| Moderate complexity (RS 7–9) | 38.3 (n = 72) | 44.1 (n = 113) | 0.4 |
| High complexity (RS 10–12) | 1.6 (n = 3) | 5.9 (n = 15) | 0.8 |
| Open Technique (n = 141) | Conventional Laparoscopy (n = 70) | Percutaneous Access (n = 187) | Robot-Assisted Laparoscopy (n = 46) | X2 | |
|---|---|---|---|---|---|
| LOS (days) (range; mean) | 3–15; 6.0 | 1–10; 3.8 | 1–9; 1.2 | 1–15; 2.8 | p < 0.001 |
| Unplanned readmission (%) | 12.8 (n = 18) | 4.3 (n = 3) | 7.5 (n = 14) | 0 (n = 0) | p = 0.019 |
| Surgical complications (Clavien–Dindo ≥ 3) (%) | 7.1 (n = 10) | 4.3 (n = 3) | 2.1 (n = 4) | 6.5 (n = 3) | p = 0.022 |
| Urinary leakage (%) | 4.3 (n = 6) | 2.2 (n = 1) | |||
| Bleeding (%) | 2.8 (n = 4) | 1.4 (n = 1) | 0.5 (n = 1) | 4.4 (n = 2) | |
| Urinary retention * (%) | 0.5 (n = 1) | ||||
| Other (%) | 1.4 (n = 1) | 1.0 (n = 2) | |||
| Abscess (%) | 1.4 (n = 1) |
| Ablative Treatment (n = 118) | Partial Nephrectomy (n = 207) | Total Nephrectomy (n = 49) | |
|---|---|---|---|
| Anemia | 1 | 1 | |
| Chest pain | 1 | ||
| Herniated disk | 1 | ||
| Dyspnea | 1 | 2 | |
| Esophagitis | 1 | ||
| Minor trauma | 1 | ||
| Intestinal obstruction | 1 | ||
| Infection | 4 | 6 | 1 |
| Pain | 1 | ||
| Syncope | 1 | ||
| Bleeding | 1 | ||
| Hematuria | 1 | ||
| Melena | 1 | ||
| Abdominal pain | 2 | ||
| Jaundice | 1 | ||
| Kidney stone | 1 | ||
| Fatigue | 1 | ||
| Urinary leakage | 1 | ||
| Vertigo | 1 | ||
| Cholecystitis | 1 | ||
| Other | 1 | ||
| Total | 14 | 18 | 3 |
| OR | 95% CI | p | |
|---|---|---|---|
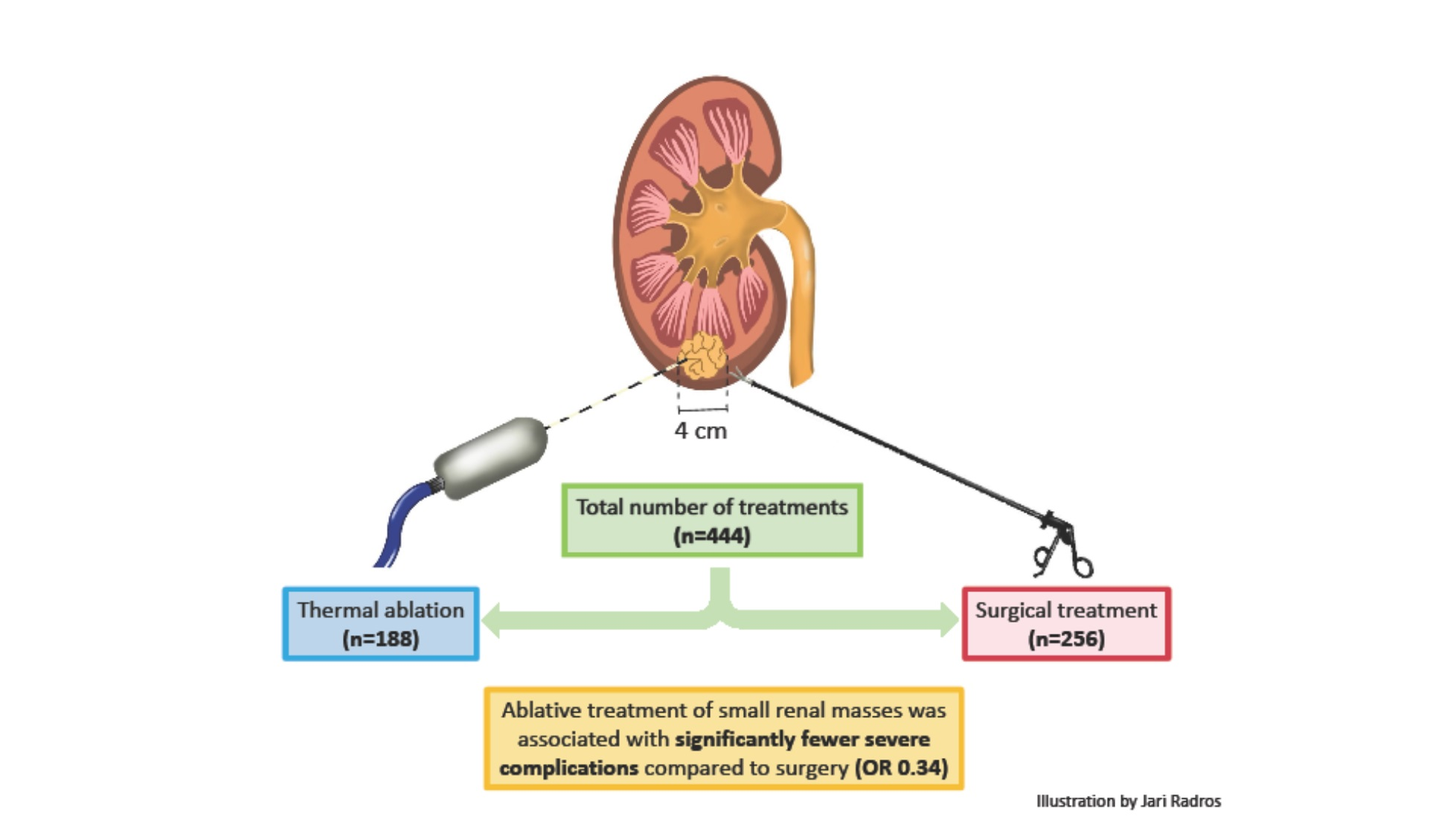
| Unadjusted | 0.39 | 0.19–0.79 | 0.013 |
| Adjusted * | 0.34 | 0.17–0.68 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radros, J.; Kjellman, A.; Henningsohn, L.; Forslin, Y.; Delle, M.; Hrebenyuk, M.; Thor, A.; Thiel, T.; Hermann, M.; Lundgren, P.-O. Ablative or Surgical Treatment for Small Renal Masses (T1a): A Single-Center Comparison of Perioperative Morbidity and Complications. Curr. Oncol. 2024, 31, 933-940. https://doi.org/10.3390/curroncol31020069
Radros J, Kjellman A, Henningsohn L, Forslin Y, Delle M, Hrebenyuk M, Thor A, Thiel T, Hermann M, Lundgren P-O. Ablative or Surgical Treatment for Small Renal Masses (T1a): A Single-Center Comparison of Perioperative Morbidity and Complications. Current Oncology. 2024; 31(2):933-940. https://doi.org/10.3390/curroncol31020069
Chicago/Turabian StyleRadros, Jari, Anders Kjellman, Lars Henningsohn, Yngve Forslin, Martin Delle, Marianna Hrebenyuk, Anna Thor, Tomas Thiel, Maria Hermann, and Per-Olof Lundgren. 2024. "Ablative or Surgical Treatment for Small Renal Masses (T1a): A Single-Center Comparison of Perioperative Morbidity and Complications" Current Oncology 31, no. 2: 933-940. https://doi.org/10.3390/curroncol31020069
APA StyleRadros, J., Kjellman, A., Henningsohn, L., Forslin, Y., Delle, M., Hrebenyuk, M., Thor, A., Thiel, T., Hermann, M., & Lundgren, P.-O. (2024). Ablative or Surgical Treatment for Small Renal Masses (T1a): A Single-Center Comparison of Perioperative Morbidity and Complications. Current Oncology, 31(2), 933-940. https://doi.org/10.3390/curroncol31020069