Real-World Outcomes of Incurable Cancer Patients Treated with Unlisted Anticancer Treatments in an Academic Center in Quebec, Canada


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Collected Data
2.3. Outcome Description and Statistical Analysis
3. Results
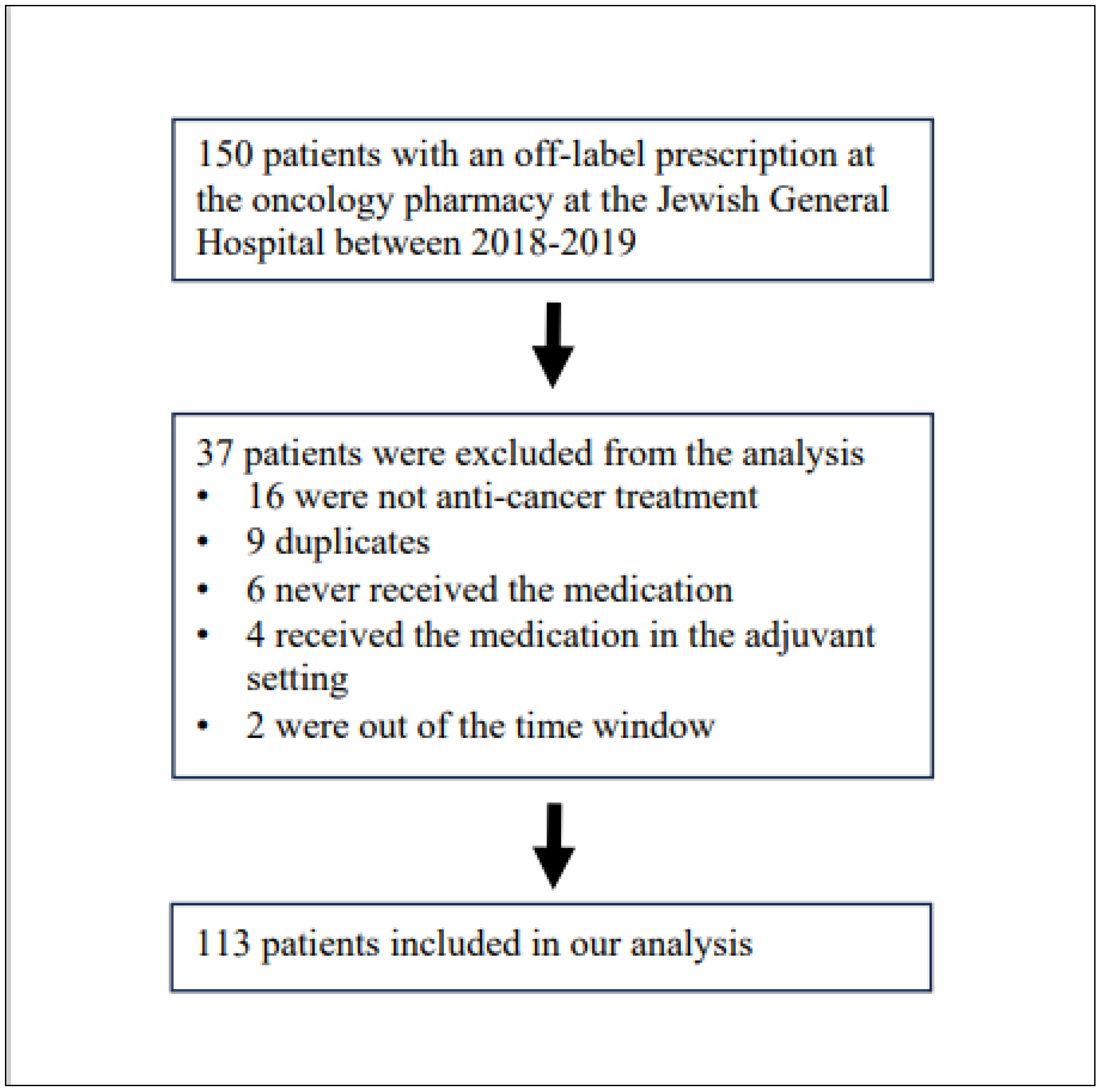
3.1. Description of the Patients Receiving an Unlisted Anticancer Prescription
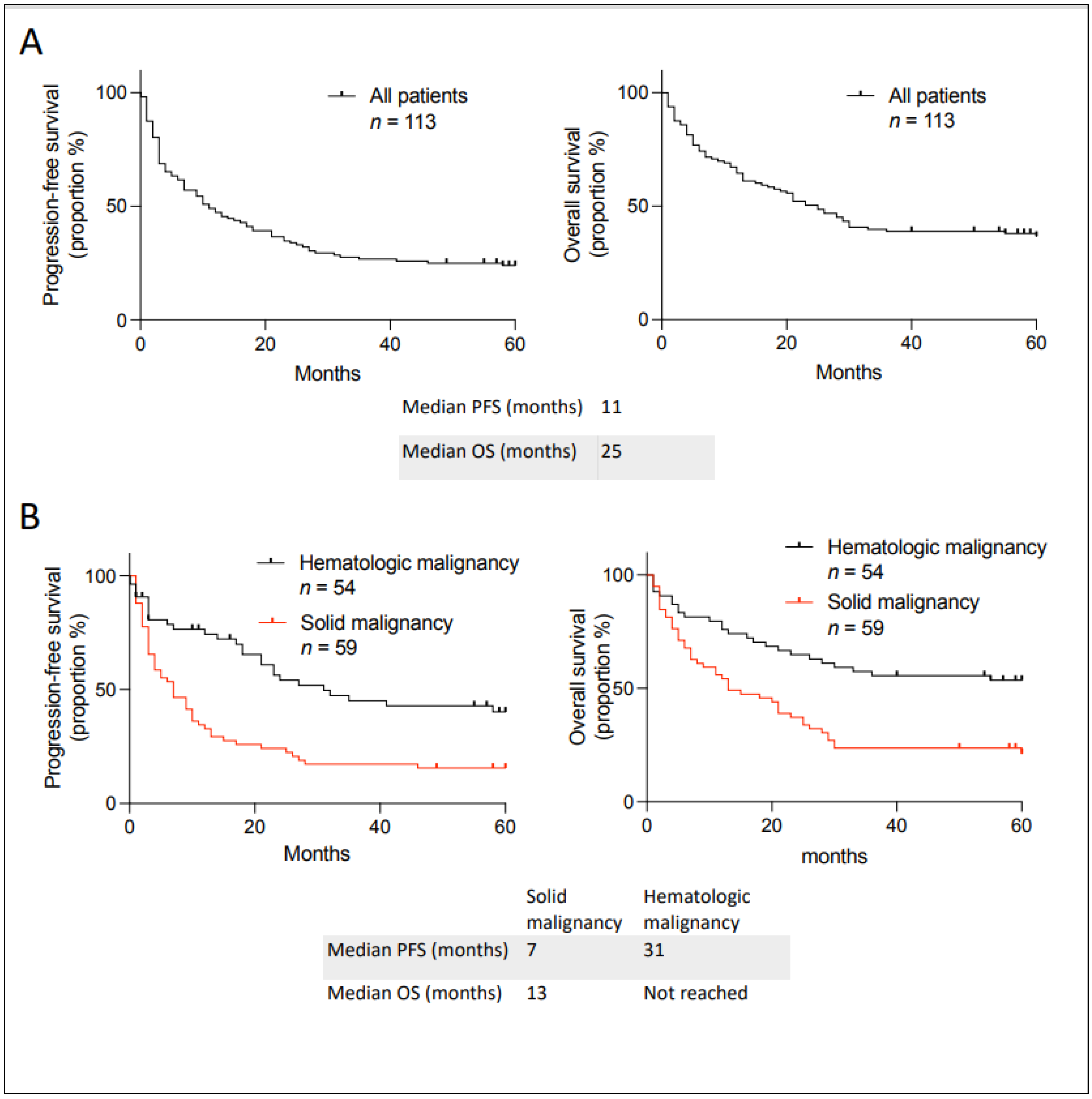
3.2. Clinical Outcomes in Patients Receiving an Unlisted Anticancer Prescription
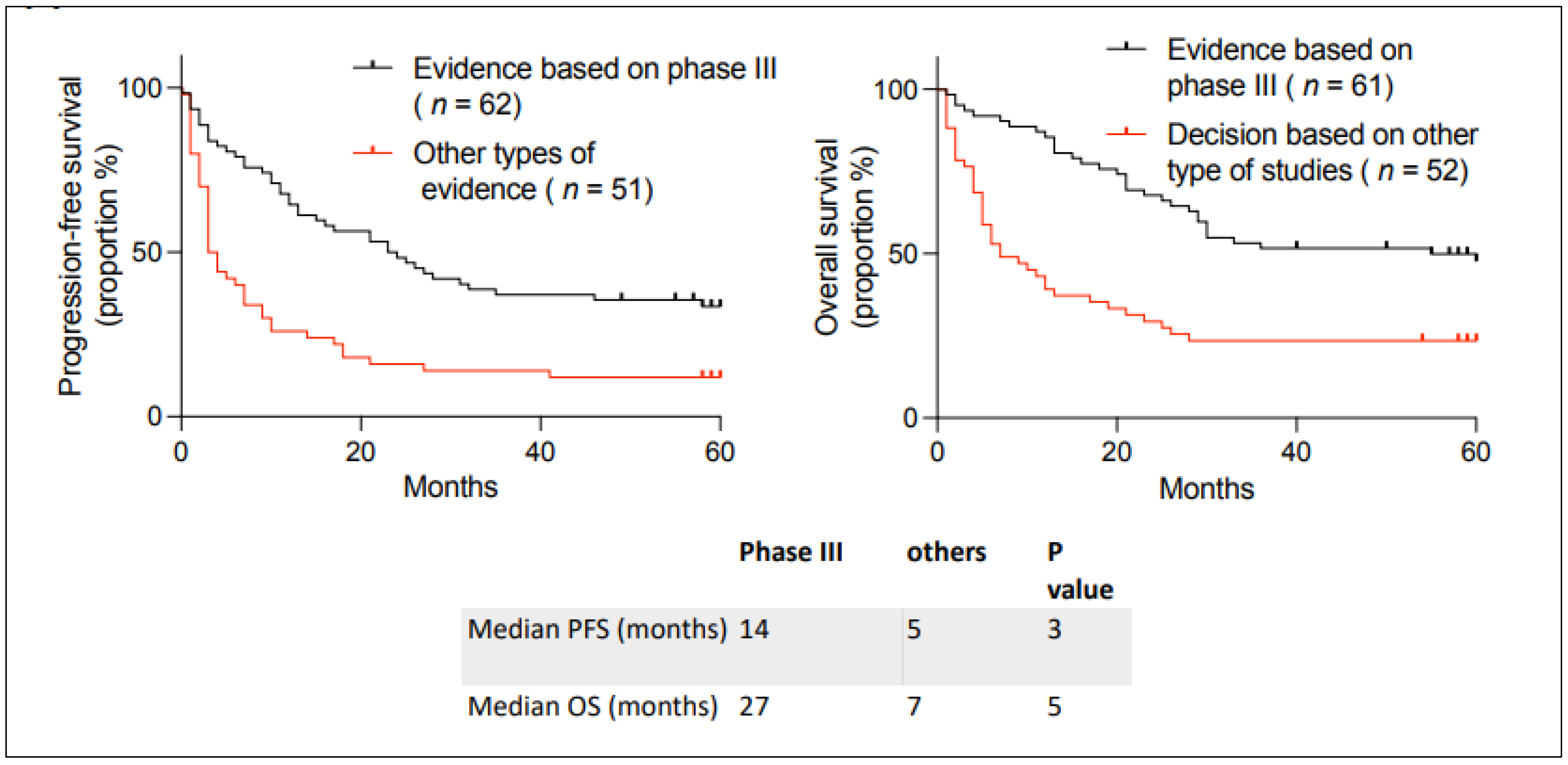
3.3. Analysis of Outcomes According to the Level of Evidence Supporting the Request
3.4. Analysis of Outcomes if the Medication Was Subsequently Reimbursed in Quebec
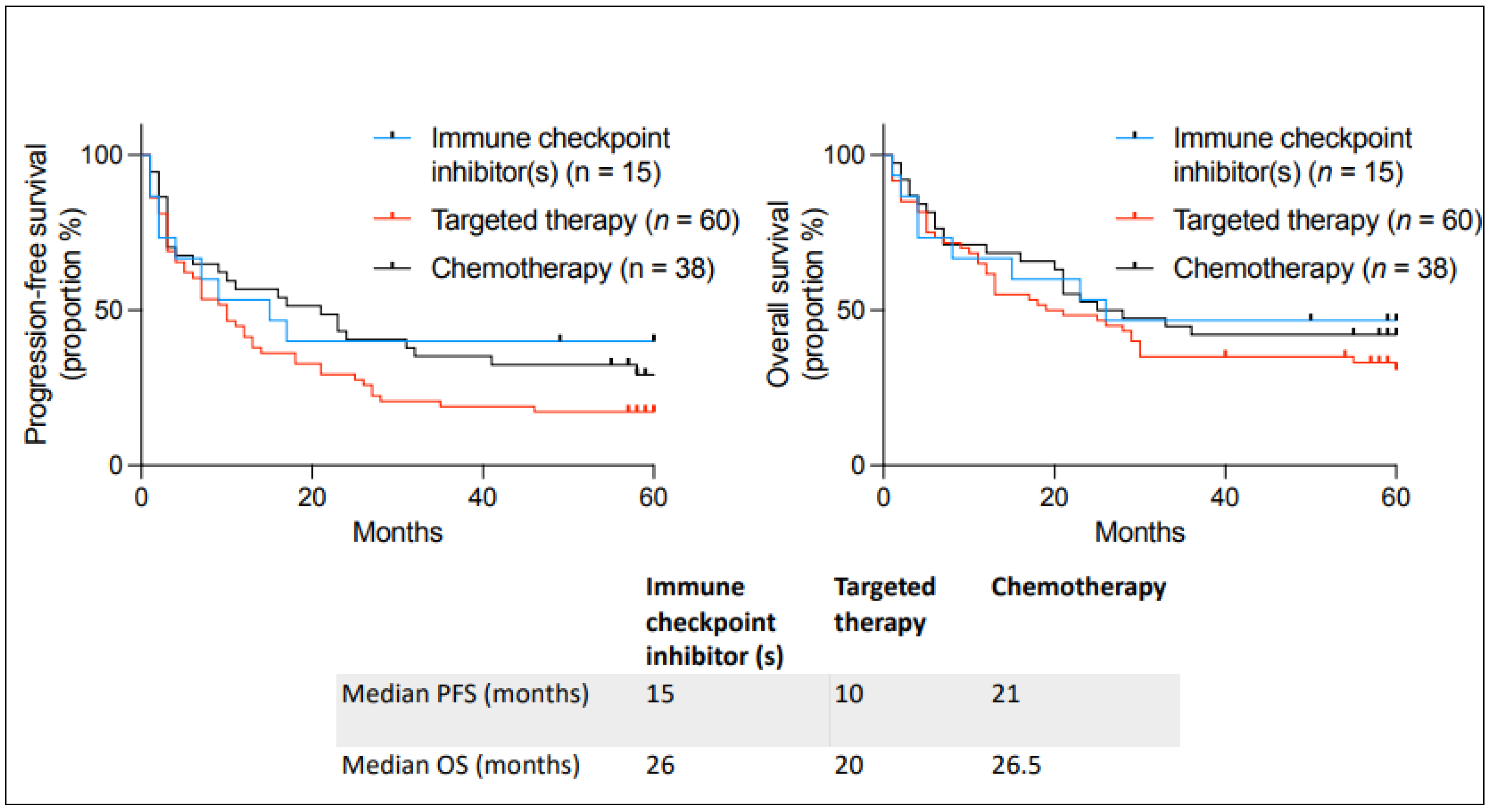
3.5. Analysis of Outcomes According to the Type of Anticancer Medication
3.6. Analysis of Outcomes in Comparison to the Published Literature
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, D.G.; Wobst, H.J. A Decade of FDA-Approved Drugs (2010–2019): Trends and Future Directions. J. Med. Chem. 2021, 64, 2312–2338. [Google Scholar] [CrossRef] [PubMed]
- MacEwan, J.P.; Dennen, S.; Kee, R.; Ali, F.; Shafrin, J.; Batt, K. Changes in mortality associated with cancer drug approvals in the United States from 2000 to 2016. J. Med. Econ. 2020, 23, 1558–1569. [Google Scholar] [CrossRef] [PubMed]
- Michaeli, D.T.; Michaeli, J.C.; Michaeli, T. Advances in cancer therapy: Clinical benefit of new cancer drugs. Aging 2023, 15, 5232–5234. [Google Scholar] [CrossRef] [PubMed]
- Glennie, J.; Villalba, E.; Wheatley-Price, P. Closing the Gaps to Timely Patient Access: Perspectives on Conditional Funding Models. Curr. Oncol. 2022, 29, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. The Government of Canada Announces the Creation of the Canadian Drug Agency. 18 December 2023. Available online: https://www.canada.ca/en/health-canada/news/2023/12/the-government-of-canada-announces-the-creation-of-the-canadian-drug-agency---helping-make-canadas-drug-system-more-sustainable-and-better-prepared.html (accessed on 3 July 2024).
- Gotfrit, J.; Shin, J.J.W.; Mallick, R.; Stewart, D.J.; Wheatley-Price, P. Potential Life-Years Lost: The Impact of the Cancer Drug Regulatory and Funding Process in Canada. Oncologist 2020, 25, e130–e137. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, A.; Stewart, D.J.; Batist, G.; Spadafora, S.; Sehdev, S.; Goodman, S.G. Access Denied? The Unintended Consequences of Pending Drug Pricing Rules. Curr. Oncol. 2022, 29, 2504–2508. [Google Scholar] [CrossRef] [PubMed]
- Gotfrit, J.; Jackson, A.; Shin, J.J.W.; Stewart, D.J.; Mallick, R.; Wheatley-Price, P. Determinants of the Cancer Drug Funding Process in Canada. Curr. Oncol. 2022, 29, 1997–2007. [Google Scholar] [CrossRef] [PubMed]
- Vanderpuye-Orgle, J.; Erim, D.; Qian, Y.; Boyne, D.J.; Cheung, W.Y.; Bebb, G.; Shah, A.; Pericleous, L.; Maruszczak, M.; Brenner, D.R. Estimating the Impact of Delayed Access to Oncology Drugs on Patient Outcomes in Canada. Oncol. Ther. 2022, 10, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Uyl-de Groot, C.A.; Heine, R.; Krol, M.; Verweij, J. Unequal Access to Newly Registered Cancer Drugs Leads to Potential Loss of Life-Years in Europe. Cancers 2020, 12, 2313. [Google Scholar] [CrossRef] [PubMed]
- International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3). Available online: https://www.who.int/standards/classifications/other-classifications/international-classification-of-diseases-for-oncology (accessed on 14 June 2024).
- Flinn, I.W.; van der Jagt, R.; Kahl, B.; Wood, P.; Hawkins, T.; MacDonald, D.; Simpson, D.; Kolibaba, K.; Issa, S.; Chang, J.; et al. First-Line Treatment of Patients With Indolent Non-Hodgkin Lymphoma or Mantle-Cell Lymphoma With Bendamustine Plus Rituximab Versus R-CHOP or R-CVP: Results of the BRIGHT 5-Year Follow-Up Study. J. Clin. Oncol. 2019, 37, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.; Rutkowski, P.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1480–1492. [Google Scholar] [CrossRef] [PubMed]
- Fiegl, M.; Mlineritsch, B.; Hubalek, M.; Bartsch, R.; Pluschnig, U.; Steger, G.G. Single-agent pegylated liposomal doxorubicin (PLD) in the treatment of metastatic breast cancer: Results of an Austrian observational trial. BMC Cancer 2011, 11, 373. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Escudier, B.; Powles, T.; Tannir, N.M.; Mainwaring, P.N.; Rini, B.I.; Hammers, H.J.; Donskov, F.; Roth, B.J.; Peltola, K.; et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): Final results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2016, 17, 917–927. [Google Scholar] [CrossRef] [PubMed]
- Yoo, C.; Im, H.S.; Kim, K.P.; Oh, D.Y.; Lee, K.H.; Chon, H.J.; Kim, J.H.; Kang, M.; Kim, I.; Lee, G.J.; et al. Real-world efficacy and safety of liposomal irinotecan plus fluorouracil/leucovorin in patients with metastatic pancreatic adenocarcinoma: A study by the Korean Cancer Study Group. Ther. Adv. Med. Oncol. 2019, 11, 1758835919871126. [Google Scholar] [CrossRef] [PubMed]
- Arroyo Álvarez, C.; Rodríguez Pérez, L.; Rodríguez Mateos, M.E.; Martínez Bautista, M.J.; Benítez Rodríguez, E.; Baena-Cañada, J.M. Off-label antineoplastic drugs. An effectiveness and safety study. Farm Hosp. 2017, 41, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, J.G.; Foulkes, W.D.; Pollak, M.N. Cancer Immunoprevention: A Case Report Raising the Possibility of “Immuno-interception”. Cancer Prev. Res. 2020, 13, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Pang, S.A.; Elkrief, A.; Capella, M.P.; Miller, W.H. Two Cases of Durable and Deep Responses to Immune Checkpoint Inhibition-Refractory Metastatic Melanoma after Addition of Camu Camu Prebiotic. Curr. Oncol. 2023, 30, 7852–7859. [Google Scholar] [CrossRef] [PubMed]
- Santiago, R.; Korsos, V.; Assouline, S.; Johnson, N. Successful PD-1 Blockade in a Patient with Refractory EBV-Positive HIV-Related Diffuse Large B-Cell Lymphoma. Clin. Lymphoma Myeloma Leuk. 2019, 19, S258. [Google Scholar] [CrossRef]
- Panet, F.; Young, M.; Wong, S.; Dragomir, A.; Rose, A.A.N.; Panasci, L. Abstract P2-01-06: Real-world outcome and cost analysis of the addition of pertuzumab to neoadjuvant therapy in localized HER2 positive breast cancer: A single center experience. Cancer Res. 2023, 83, P2-01. [Google Scholar] [CrossRef]
- Health Canada. Health Canada’s Special Access Programs: Request a Drug. 23 December 2002. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/special-access/drugs.html (accessed on 15 June 2024).
- Bill 15: The Quebec Government Wants to Limit the Specific Medical Necessity Measure. 17 July 2023. Available online: https://www.fasken.com/en/knowledge/2023/07/bill-15-the-quebec-government-wants-to-limit-the-specific-medical-necessity-measure (accessed on 15 June 2024).
- Stewart, D.J.; Bradford, J.P.; Sehdev, S.; Ramsay, T.; Navani, V.; Rawson, N.S.B.; Jiang, D.M.; Gotfrit, J.; Wheatley-Price, P.; Liu, G.; et al. New Anticancer Drugs: Reliably Assessing “Value” While Addressing High Prices. Curr. Oncol. 2024, 31, 2453–2480. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | N (%) |
|---|---|
| Sex | |
| Male | 57 (50%) |
| Female | 56 (50%) |
| Age (years) | |
| 18–50 | 18 (16%) |
| 51–71 | 62 (55%) |
| ≥71 | 35 (31%) |
| Type of cancer | |
| Solid malignancy | 59 (52%) |
| Breast | 10 (9%) |
| Pancreatic | 8 (7%) |
| Colorectal | 7 (6%) |
| Ovarian | 6 (5%) |
| Skin, melanoma | 6 (5%) |
| Renal cell | 6 (5%) |
| Lung cancer, non-small cell lung cancer | 4 (4%) |
| Skin, squamous carcinoma | 3 (3%) |
| Head and neck, squamous carcinoma | 2 (2%) |
| Bladder | 2 (2%) |
| Angiosarcoma, prostate, leiomyosarcoma, cervix, endometrium | 1 (1%) each |
| Hematological malignancy | 54 (48%) |
| Indolent B-cell lymphoma | 25 (22%) |
| Multiple myeloma | 10 (9%) |
| Acute myeloid leukemia | 5 (4%) |
| Hodgkin lymphoma | 3 (3%) |
| Chronic myelocytic leukemia | 2 (2%) |
| Large B-cell lymphoma | 2 (2%) |
| Myelodysplastic syndrome | 2 (2%) |
| Blastic plasmacytoid dendritic cell neoplasm, lymphoplasmacytic lymphoma, peripheral T cell lymphoma, other monoclonal plasma cell disorder, Castleman disease | 1 (1%) each |
| Variable | N (%) |
|---|---|
| Type of treatment | |
| Targeted therapy | 60 (53%) |
| Chemotherapy | 38 (34%) |
| Immune checkpoint inhibitor | 15 (13%) |
| Evidence supporting the request | |
| Phase III randomized clinical trial | 62 (55%) |
| Others | 51 (45%) |
| Subsequently reimbursed by the public health system in Quebec | |
| Yes | 50 (44%) |
| No | 63 (56%) |
| Line of therapy | |
| First line | 31 (27%) |
| Second line | 24 (21%) |
| Third line | 26 (23%) |
| Fourth line | 17 (15%) |
| Fifth line | 6 (5%) |
| Sixth to tenth line | 9 (8%) |
| Types of Evidence | All Types of Evidence N = 113 (100%) | Phase III Clinical Trial N = 62 (54.8%) | Other Types of Evidence N = 51 (45%) |
|---|---|---|---|
| Subsequently reimbursed | 50 (44%) | 40 (65%) | 10 (20%) |
| Number of Patients in Our Real-World Cohort | Type of Cancer | Previous Line of Treatment | Drug Name | Type of Comparator Trial, Reference | Outcomes in the Comparator Trial | Outcomes in Our Unlisted Cohort |
|---|---|---|---|---|---|---|
| 14 | Indolent B-cell lymphoma | 0 | Bendamustine-rituximab | Phase III, [12] | PFS at 5 years: 65% | PFS at 5 years: 9/14 (64%) |
| 6 | Melanoma | 0 | Ipilimumab-nivolumab | Phase III, [13] | Median PFS: 11.5 months Median OS: not reached | Median PFS: 12 months Median OS: not reached (3/6 still alive at five years) |
| 5 | Breast cancer | 4 to 9 | Liposomal doxorubicin | Retrospective analysis, [14] | Median PFS: 5.8 months Median OS: 14.2 months | Median PFS: 3 months Median OS: 6 months |
| 5 | Renal cell cancer | 2 to 3 | Cabozantinib | Phase III, [15] | Median PFS: 7.4 months Median OS: 21.4 months | Median PFS: 7 months Median OS: 28 months |
| 5 | Pancreatic cancer | 2 to 3 | Liposomal irinotecan with 5-FU * | Retrospective data, [16] | Median PFS: 3.5 months Median OS: 9.4 months | Median PFS: 3 months Median OS: 6 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, A.; Panet, F.; Korsos, V.; Miller, W.H., Jr.; Batist, G. Real-World Outcomes of Incurable Cancer Patients Treated with Unlisted Anticancer Treatments in an Academic Center in Quebec, Canada. Curr. Oncol. 2024, 31, 5908-5918. https://doi.org/10.3390/curroncol31100440
Miller A, Panet F, Korsos V, Miller WH Jr., Batist G. Real-World Outcomes of Incurable Cancer Patients Treated with Unlisted Anticancer Treatments in an Academic Center in Quebec, Canada. Current Oncology. 2024; 31(10):5908-5918. https://doi.org/10.3390/curroncol31100440
Chicago/Turabian StyleMiller, Adam, Francois Panet, Victoria Korsos, Wilson H. Miller, Jr., and Gerald Batist. 2024. "Real-World Outcomes of Incurable Cancer Patients Treated with Unlisted Anticancer Treatments in an Academic Center in Quebec, Canada" Current Oncology 31, no. 10: 5908-5918. https://doi.org/10.3390/curroncol31100440
APA StyleMiller, A., Panet, F., Korsos, V., Miller, W. H., Jr., & Batist, G. (2024). Real-World Outcomes of Incurable Cancer Patients Treated with Unlisted Anticancer Treatments in an Academic Center in Quebec, Canada. Current Oncology, 31(10), 5908-5918. https://doi.org/10.3390/curroncol31100440