Genetic Polymorphisms and Tumoral Mutational Profiles over Survival in Advanced Colorectal Cancer Patients: An Exploratory Study

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
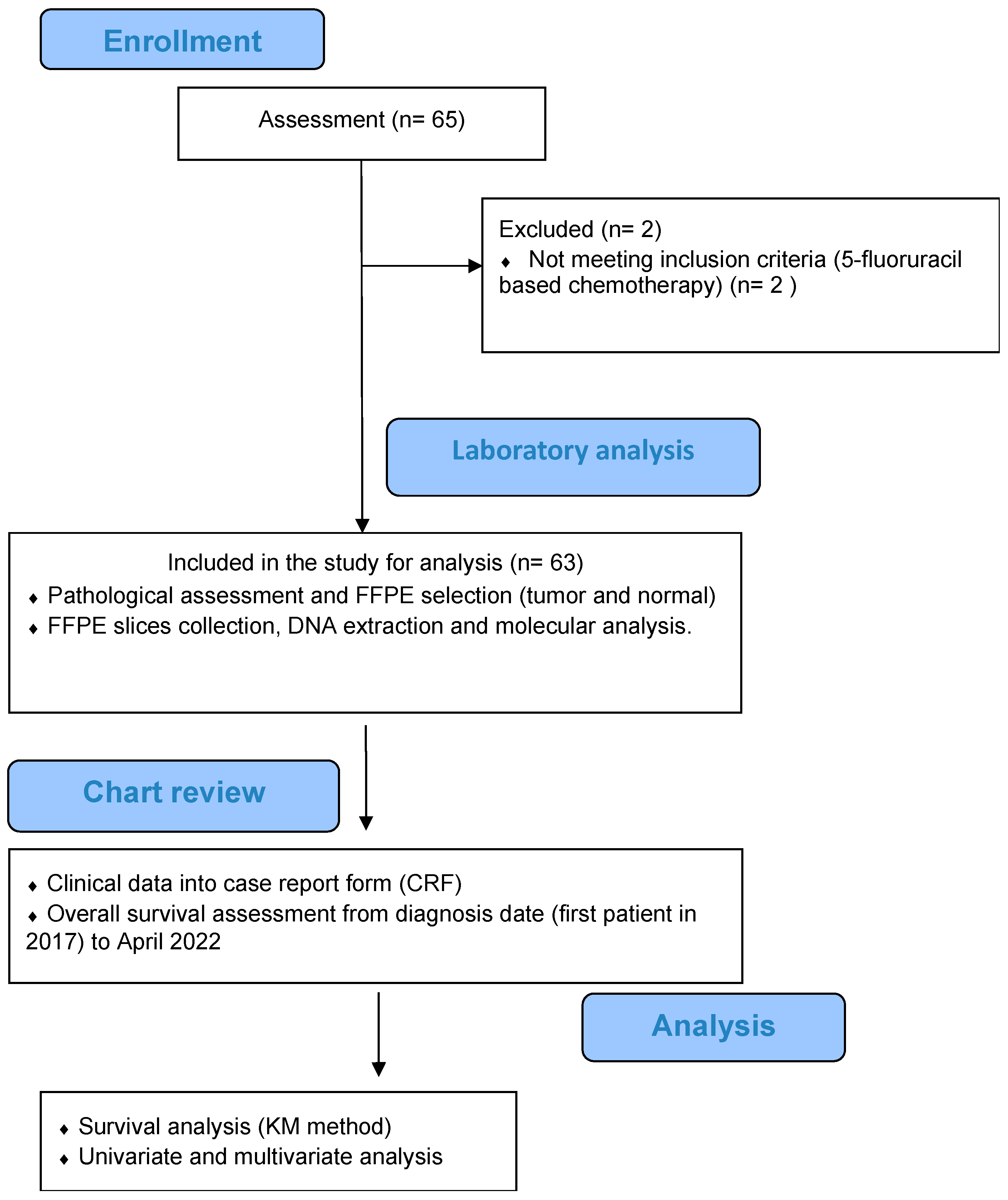
2.1. Patients and Tissue Sampling
2.2. Molecular Testing
2.3. Drug Sensitivity Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Molecular Profile
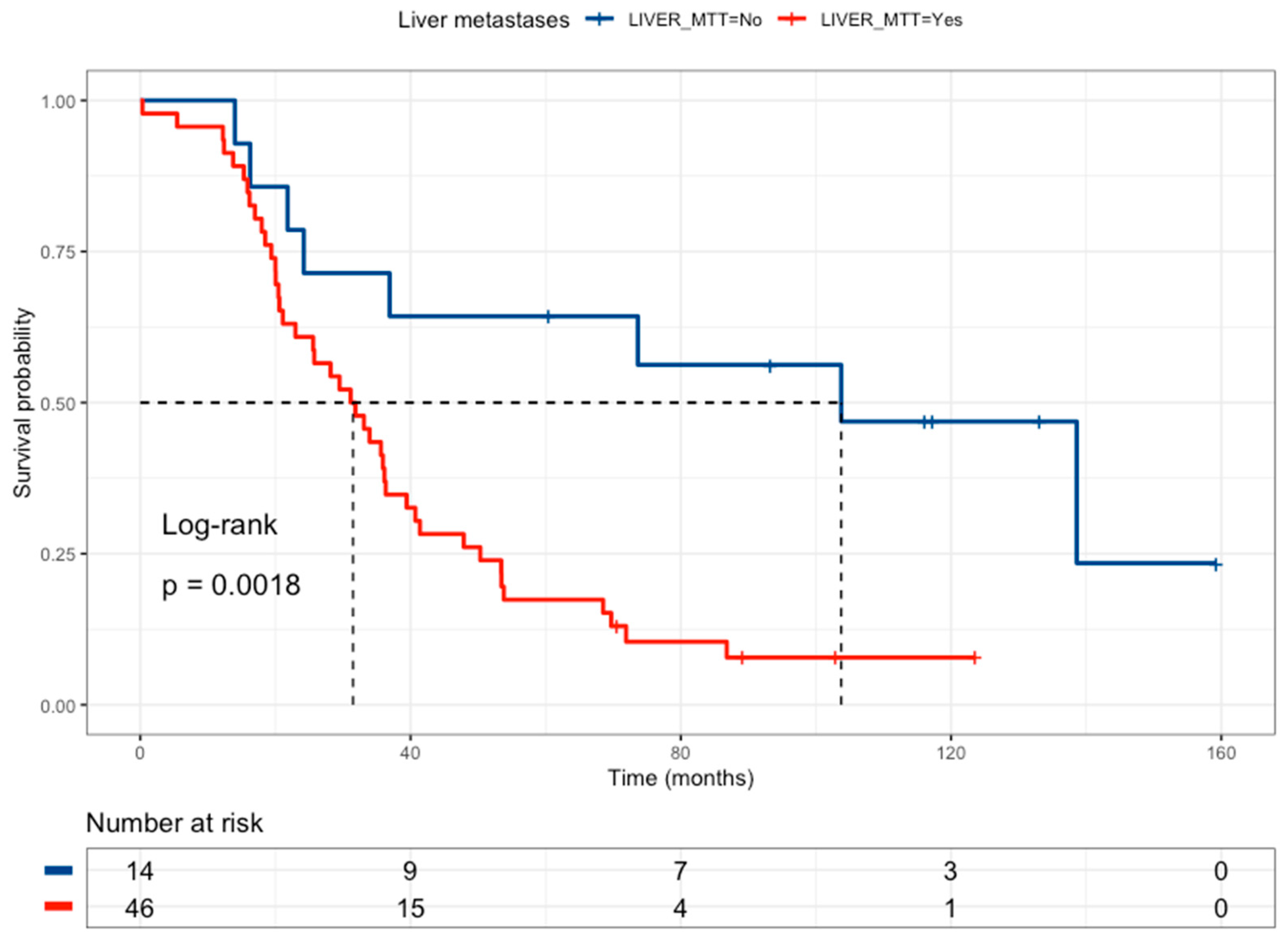
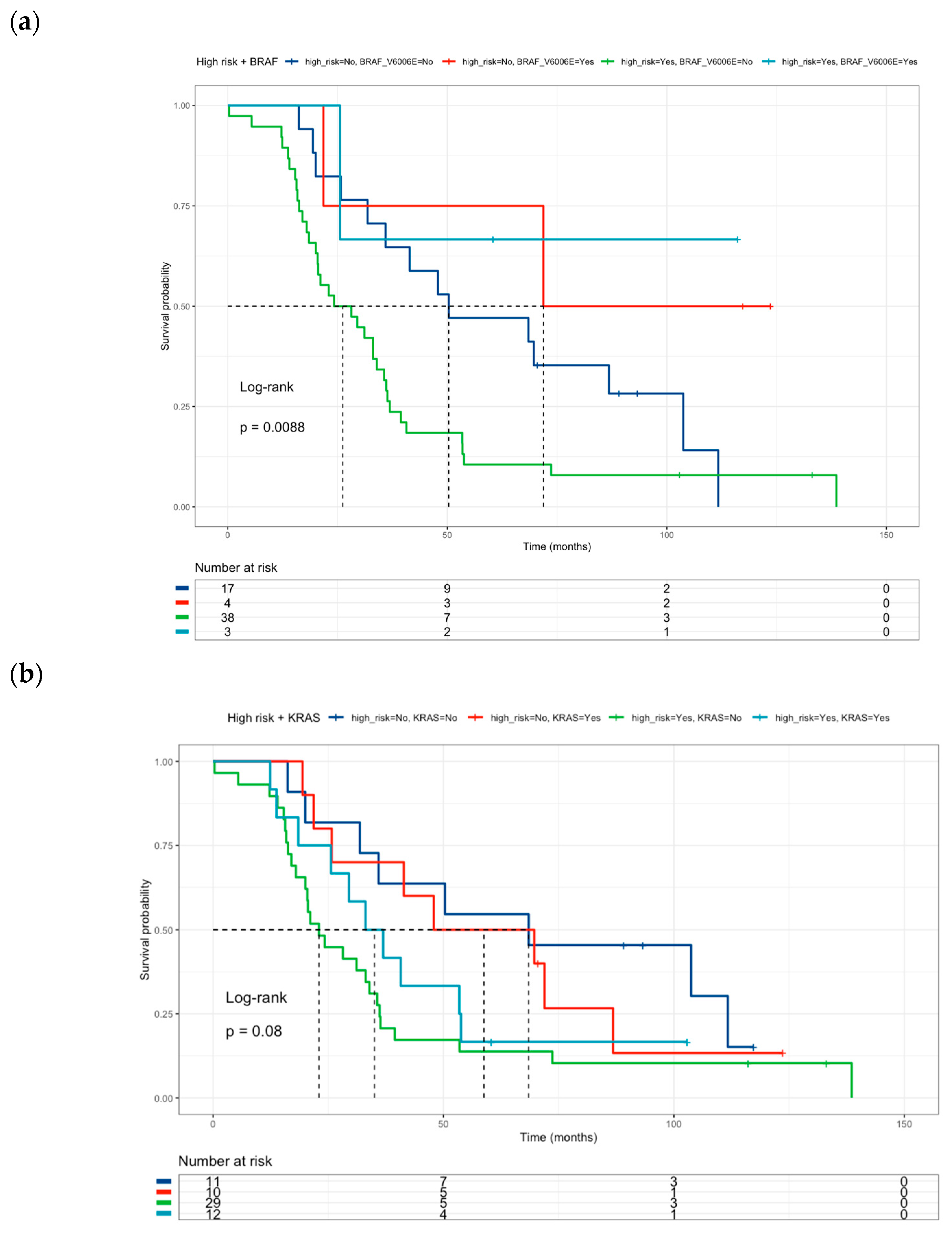
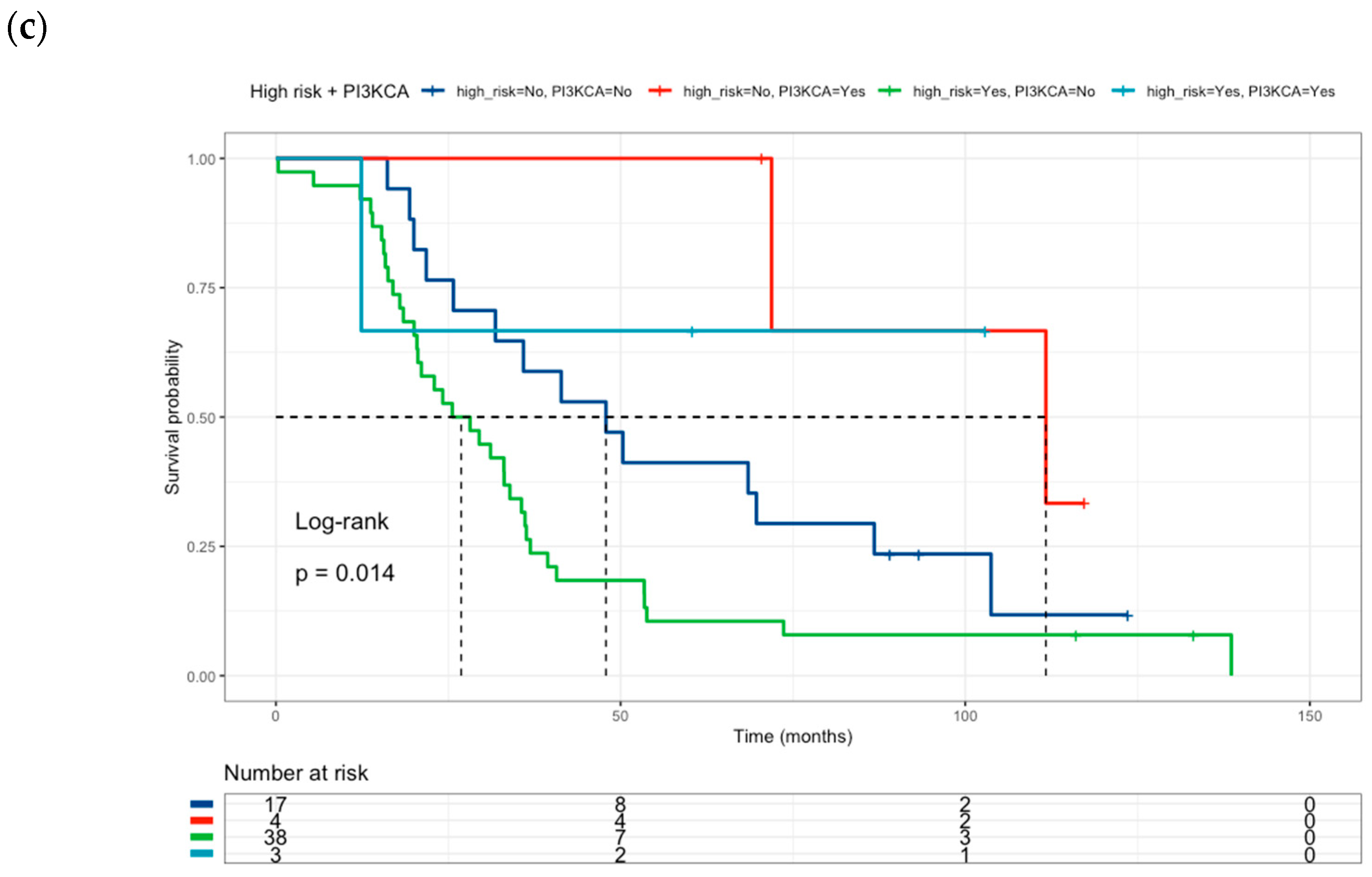
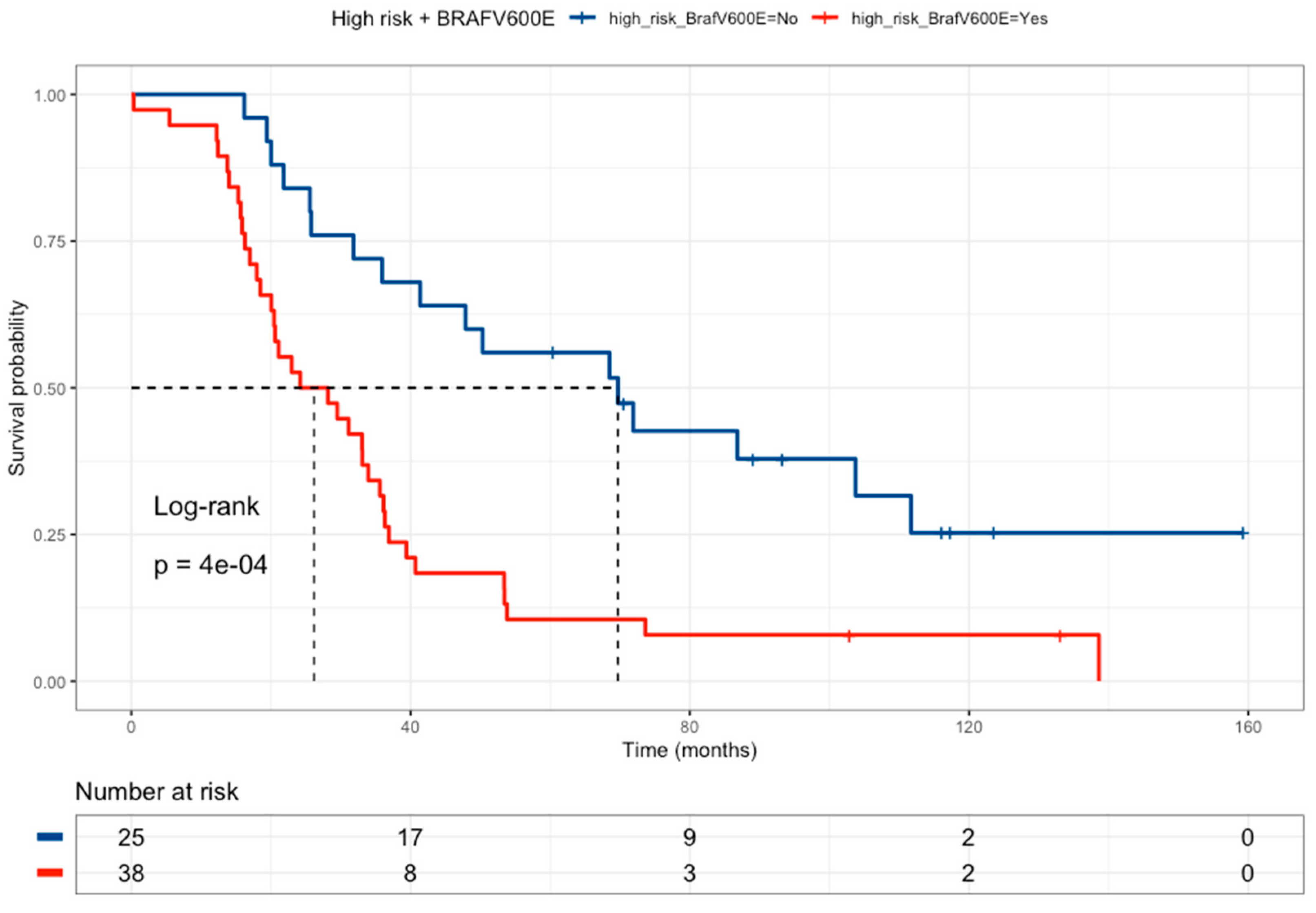
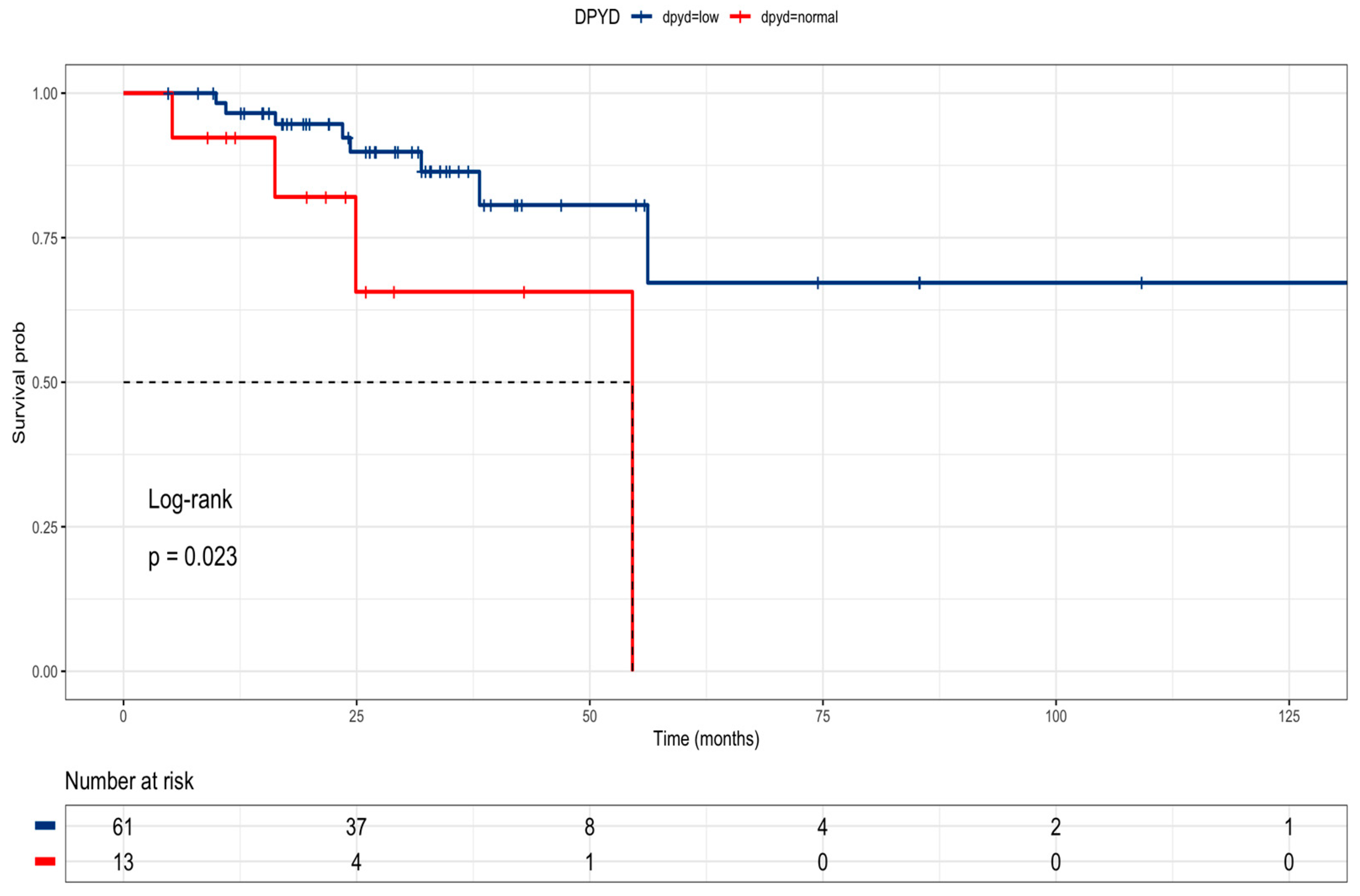
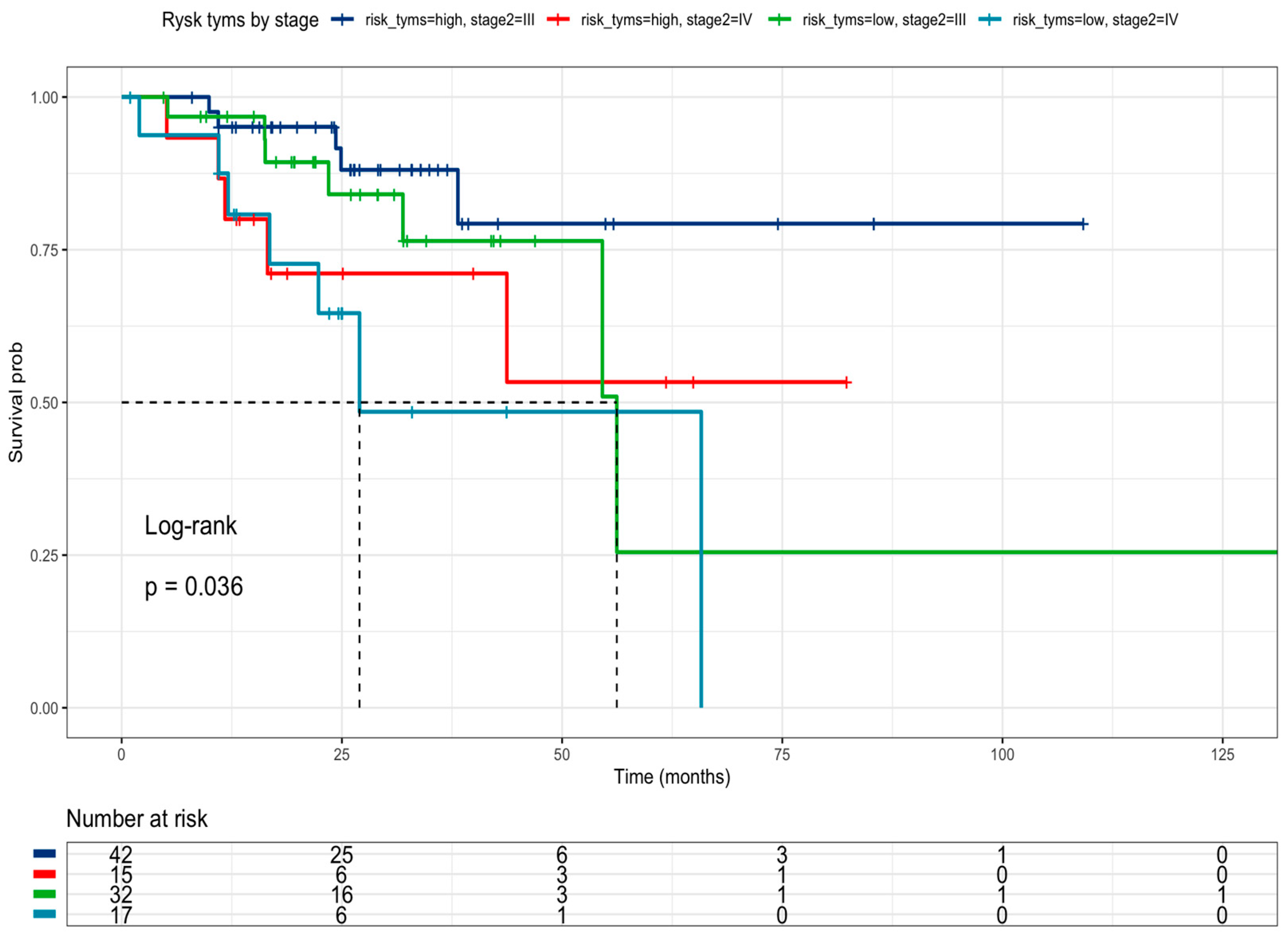
3.3. Correlations of Clinicopathological Characteristics and Mutation Profile with Overall Survival
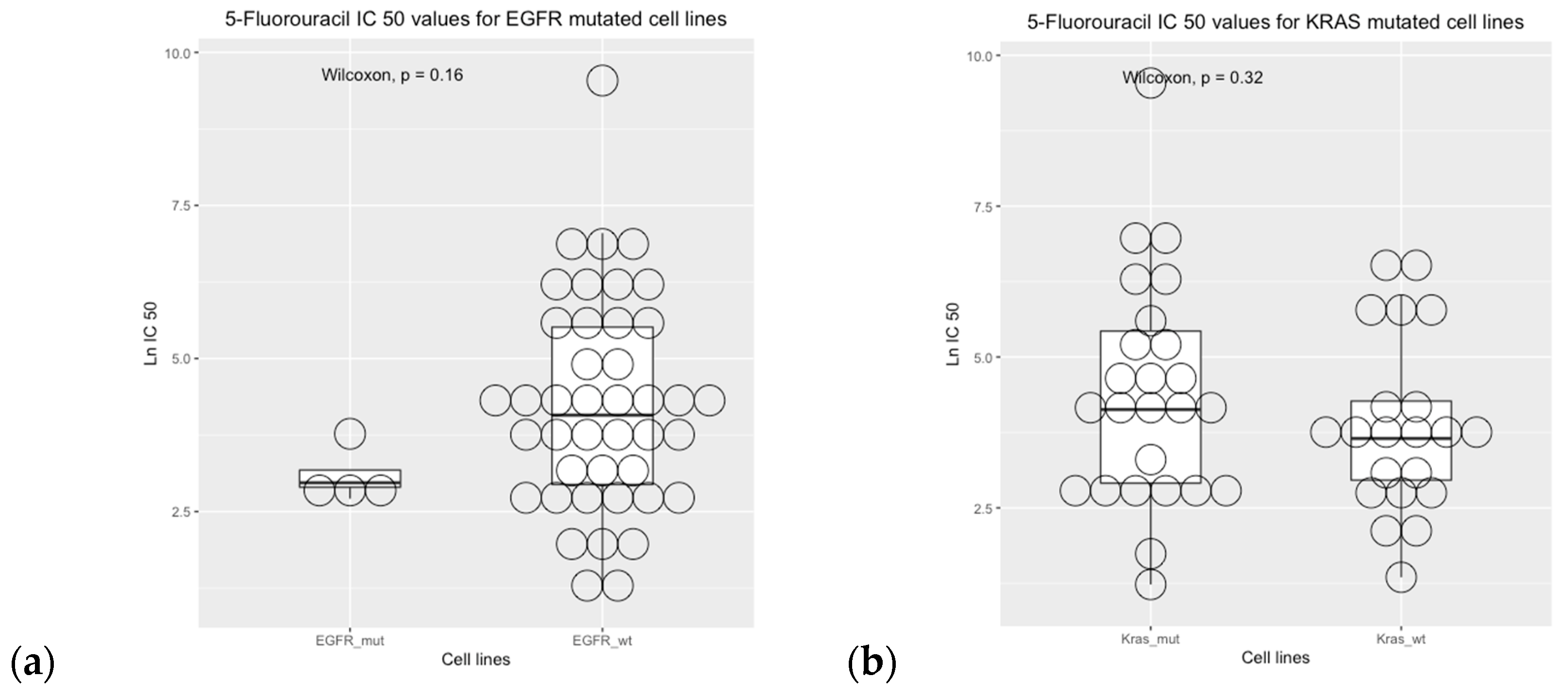
3.4. Drug Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MINSAL. Guía de Práctica Clínica Cáncer Colorectal en Personas de 15 Años y Más. Available online: https://diprece.minsal.cl/garantias-explicitas-en-salud-auge-o-ges/guias-de-practica-clinica/cancer-colorectal-en-personas-de-15-anos-y-mas/resumen-ejecutivo/ (accessed on 30 October 2023).
- National Comprehensive Cancer Network (NCCN). Colon Cancer, Version 2.2023, NCCN Clinical Practice Guidelines in Oncol-ogy. Natl Compr Cancer Netw: JNCCN. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 30 October 2023).
- Watanabe, T.; Wu, T.-T.; Catalano, P.J.; Ueki, T.; Satriano, R.; Haller, D.G.; Benson, A.B.; Hamilton, S.R. Molecular Predictors of Survival after Adjuvant Chemotherapy for Colon Cancer. NEJM 2001, 344, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC). Global Cancer Observatory. Available online: https://gco.iarc.fr/ (accessed on 30 October 2023).
- Sargent, D.; Sobrero, A.; Grothey, A.; O’Connell, M.J.; Buyse, M.; Andre, T.; Zheng, Y.; Green, E.; Labianca, R.; O’Callaghan, C.; et al. Evidence for Cure by Adjuvant Therapy in Colon Cancer: Observations Based on Individual Patient Data From 20,898 Patients on 18 Randomized Trials. J. Clin. Oncol. 2009, 27, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.I.; Lim, S.-B.; Yoon, Y.S.; Kim, C.W.; Yu, C.S.; Kim, T.W.; Kim, J.H.; Kim, J.C. Comparison of Recurrence Patterns between ≤5 Years and >5 Years after Curative Operations in Colorectal Cancer Patients. J. Surg. Oncol. 2013, 108, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Lenz, H.-J.; Ou, F.-S.; Venook, A.P.; Hochster, H.S.; Niedzwiecki, D.; Goldberg, R.M.; Mayer, R.J.; Bertagnolli, M.M.; Blanke, C.D.; Zemla, T.; et al. Impact of Consensus Molecular Subtype on Survival in Pa-tients With Metastatic Colorectal Cancer: Results from CALGB/SWOG 80405 (Alliance). J. Clin. Oncol. 2019, 37, 1876–1885. [Google Scholar] [CrossRef] [PubMed]
- Meta-Analysis Group In Cancer. Efficacy of Intravenous Continuous Infusion of Fluorouracil Compared with Bolus Administration in Advanced Colorectal Can-cer. Meta-Analysis Group In Cancer. J. Clin. Oncol. 1998, 16, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Mahfouf, H.; Djeddi, H.; Belhadef, S.; Bouzid, K.; Bentabak, K. Capecitabine Combined with Oxaliplatin (XELOX) as First-Line Chemotherapy in Colorectal Cancer with. Liver Metastases. J. Clin. Oncol. 2009, 27, e15146. [Google Scholar] [CrossRef]
- Bleiberg, H.; de Gramont, A. Oxaliplatin plus 5-Fluorouracil: Clinical Experience in Patients with Advanced Colorectal Cancer. Semin. Oncol. 1998, 25, 32–39. [Google Scholar]
- Giacchetti, S.; Perpoint, B.; Zidani, R.; Le Bail, N.; Faggiuolo, R.; Focan, C.; Chollet, P.; Llory, J.F.; Letourneau, Y.; Coudert, B.; et al. Phase III Multicenter Ran-domized Trial of Oxaliplatin Added to Chronomodulated Fluorouracil–Leucovorin as First-Line Treatment of Metastatic Colo-rectal Cancer. J. Clin. Oncol. 2000, 18, 136. [Google Scholar] [CrossRef]
- Douillard, J.; Cunningham, D.; Roth, A.; Navarro, M.; James, R.; Karasek, P.; Jandik, P.; Iveson, T.; Carmichael, J.; Alakl, M.; et al. Irinotecan Combined with Fluorouracil Compared with Fluorouracil Alone as First-Line Treatment for Metastatic Colorectal Cancer: A Multicentre Randomised Trial. Lancet 2000, 355, 1041–1047. [Google Scholar] [CrossRef]
- Saltz, L.B.; Cox, J.V.; Blanke, C.; Rosen, L.S.; Fehrenbacher, L.; Moore, M.J.; Maroun, J.A.; Ackland, S.P.; Locker, P.K.; Pirotta, N.; et al. Irinotecan plus Fluorouracil and Leucovorin for Metastatic Colorectal Cancer. NEJM 2000, 343, 905–914. [Google Scholar] [CrossRef]
- Fakih, M.G.; Kopetz, S.; Kuboki, Y.; Kim, T.W.; Munster, P.N.; Krauss, J.C.; Falchook, G.S.; Han, S.-W.; Heinemann, V.; Muro, K.; et al. Sotorasib for Previously Treated Colorectal Cancers with KRASG12C Mutation (CodeBreaK100): A Prespecified Analysis of a Single-Arm, Phase 2 Trial. Lancet Oncol. 2022, 23, 115–124. [Google Scholar] [CrossRef] [PubMed]
- MINSAL. Guias Clínicas AUGE. Colecistectomía Preventiva en adultos de 35 a 49 años. Available online: http://www.supersalud.gob.cl/difusion/665/w3-article-600.html (accessed on 30 October 2023).
- Caudle, K.E.; Thorn, C.F.; Klein, T.E.; Swen, J.J.; McLeod, H.L.; Diasio, R.B.; Schwab, M. Clinical Pharmacogenetics Implementa-tion Consortium Guidelines for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing. Clin. Pharmacol. Ther. 2013, 94, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Hirota, T.; Date, Y.; Nishibatake, Y.; Takane, H.; Fukuoka, Y.; Taniguchi, Y.; Burioka, N.; Shimizu, E.; Nakamura, H.; Otsubo, K.; et al. Dihydropyrimidine Dehydrogenase (DPD) Expression Is Negatively Regulated by Certain MicroRNAs in Human Lung Tissues. Lung Cancer 2012, 77, 16–23. [Google Scholar] [CrossRef] [PubMed]
- van Kuilenburg, A.B.P.; Häusler, P.; Schalhorn, A.; Tanck, M.W.T.; Proost, J.H.; Terborg, C.; Behnke, D.; Schwabe, W.; Jabschinsky, K.; Maring, J.G. Evaluation of 5-Fluorouracil Pharmacokinetics in Cancer Patients with a c.1905+1G>A Mutation in DPYD by Means of a Bayesian limited sampling strategy. Clin. Pharmacokinet. 2012, 51, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Cevik, M.; Namal, E.; Sener, N.D.; Koksal, U.I.; Cagatay, P.; Deliorman, G.; Ciftci, C.; Karaalp, A.; Susleyici, B. Investigation of DPYD, MTHFR and TYMS polymorphisms on 5-fluorouracil related toxicities in colorectal cancer. Pers. Med. 2022, 19, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Panczyk, M. Pharmacogenetics Research on Chemotherapy Resistance in Colorectal Cancer over the Last 20 Years. World J. Gas-troenterol. 2014, 20, 9775. [Google Scholar] [CrossRef] [PubMed]
- Lunenburg, C.A.T.C.; van der Wouden, C.H.; Nijenhuis, M.; Crommentuijn-van Rhenen, M.H.; de Boer-Veger, N.J.; Buunk, A.M.; Houwink, E.J.F.; Mulder, H.; Rongen, G.A.; van Schaik, R.H.N.; et al. Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction of DPYD and fluoropyrimidines. Eur. J. Hum. Genet. 2020, 28, 508–517. [Google Scholar] [CrossRef]
- Amstutz, U.; Henricks, L.M.; Offer, S.M.; Barbarino, J.; Schellens, J.H.; Swen, J.J.; Klein, T.E.; McLeod, H.L.; Caudle, K.E.; Diasio, R.B.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing: 2017 Update. Clin. Pharmacol. Ther. 2018, 103, 210–216. [Google Scholar] [CrossRef]
- Ontario Health (Quality). DPYD Genotyping in Patients Who Have Planned Cancer Treatment With Fluoropyrimidines: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2021, 21, 1–186. [Google Scholar]
- Fedorinov, D.S.; Lyadov, V.K.; Sychev, D.A. Genotype-based chemotherapy for patients with gastrointestinal tumors: Focus on oxaliplatin, irinotecan, and fluoropyrimidines. Drug Metab. Pers. Ther. 2021, 37, 223–228. [Google Scholar] [CrossRef]
- Lešnjaković, L.; Ganoci, L.; Bilić, I.; Šimičević, L.; Mucalo, I.; Pleština, S.; Božina, N. DPYD genotyping and predicting fluoropyrimidine toxicity: Where do we stand? Pharmacogenomics 2023, 24, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Wu, H.; Yu, Q.; Kim, D.H.; Lipton, J.H.; Angelini, S.; Soverini, S.; Vivona, D.; Takahashi, N.; Cao, J. ABCB1 Polymor-phisms Predict Imatinib Response in Chronic Myeloid Leukemia Patients: A Systematic Review and Meta-Analysis. Pharmacogenomics J. 2015, 15, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Badic, B.; Durand, S.; El Khoury, F.; De La Grange, P.; Gentien, D.; Simon, B.; Le Jossic-Corcos, C.; Corcos, L. Prognostic Impact of Cancer Stem Cell Markers ABCB1, NEO1 and HIST1H2AE in Colorectal Cancer. Am. J. Transl. Res. 2020, 12, 5797–5807. [Google Scholar] [PubMed]
- Leschziner, G.D.; Andrew, T.; Pirmohamed, M.; Johnson, M.R. ABCB1 Genotype and PGP Expression, Function and Therapeutic Drug Response: A Critical Review and Recommendations for Future Research. Pharmacogenomics J. 2007, 7, 154–179. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, L.; Sandhu, J.K.; Harper, M.-E.; Cuperlovic-Culf, M. Role of Glutathione in Cancer: From Mechanisms to Therapies. Biomolecules 2020, 10, 1429. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Yin, Y.; Xu, S.-J.; Chen, W.-S. 5-Fluorouracil: Mechanisms of Resistance and Reversal Strategies. Molecules 2008, 13, 1551–1569. [Google Scholar] [CrossRef] [PubMed]
- Afzal, S.; Jensen, S.A.; Vainer, B.; Vogel, U.; Matsen, J.P.; Sørensen, J.B.; Andersen, P.K.; Poulsen, H.E. MTHFR Polymorphisms and 5-FU-Based Adjuvant Chemotherapy in Colorectal Cancer. Ann. Oncol. 2009, 20, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Esquivel, A.; Chinchilla-Monge, R.; Abbas, J.; Valle, M. C677T and A1298C MTHFR Gene Polymorphisms and Response to Fluoropyrimidine-Based Chemotherapy in Mestizo Patients with Metastatic Colorectal Cancer. Pharmacogenet. Genom. 2021, 31, 191–199. [Google Scholar] [CrossRef]
- Liu, J.; Li, H.; Sun, L.; Feng, X.; Wang, Z.; Yuan, Y.; Xing, C. The Differential Expression of Core Genes in Nucleotide Excision Repair Pathway Indicates Colorectal Carcinogenesis and Prognosis. Biomed. Res. Int. 2018, 2018, 9651320. [Google Scholar] [CrossRef]
- Li, H.-Y.; Ge, X.; Huang, G.-M.; Li, K.-Y.; Zhao, J.-Q.; Yu, X.-M.; Bi, W.-S.; Wang, Y.-L. GSTP1, ERCC1 and ERCC2 Polymorphisms, Expression and Clinical Outcome of Oxaliplatin-Based Adjuvant Chemotherapy in Colorectal Cancer in Chinese Population. Asian Pac. J. Cancer Prev. 2012, 13, 3465–3469. [Google Scholar] [CrossRef]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF Gene in Human Cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Wang, J.; Han, X.; Yang, H.; Wang, S.; Lin, D.; Shi, Y. Effectors of Epidermal Growth Factor Receptor Pathway: The Genetic Profiling of KRAS, BRAF, PIK3CA, NRAS Mutations in Colorectal Cancer Characteristics and Personalized Medicine. PLoS ONE 2013, 8, e81628. [Google Scholar] [CrossRef] [PubMed]
- Venderbosch, S.; Nagtegaal, I.D.; Maughan, T.S.; Smith, C.G.; Cheadle, J.P.; Fisher, D.; Kaplan, R.; Quirke, P.; Seymour, M.T.; Richman, S.D.; et al. Mismatch Repair Status and BRAF Mutation Status in Metastatic Colorectal Cancer Patients: A Pooled Analysis of the CAIRO, CAIRO2, COIN, and FO-CUS Studies. Clin. Cancer Res. 2014, 20, 5322–5330. [Google Scholar] [CrossRef] [PubMed]
- Samuels, Y.; Diaz, L.A.; Schmidt-Kittler, O.; Cummins, J.M.; DeLong, L.; Cheong, I.; Rago, C.; Huso, D.L.; Lengauer, C.; Kinzler, K.W.; et al. Mutant PIK3CA Promotes Cell Growth and Invasion of Human Cancer Cells. Cancer Cell 2005, 7, 561–573. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, P.; Janku, F.; Naing, A.; Hong, D.S.; Tsimberidou, A.M.; Falchook, G.S.; Wheler, J.J.; Piha-Paul, S.A.; Fu, S.; Stepanek, V.M.; et al. Target-Based Therapeutic Matching in Early-Phase Clinical Trials in Patients with Advanced Colorectal Cancer and PIK3CA Mutations. Mol. Cancer Ther. 2013, 12, 2857–2863. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Laguna, I.; Hong, D.S.; Janku, F.; Nguyen, L.M.; Falchook, G.S.; Fu, S.; Wheler, J.J.; Luthra, R.; Naing, A.; Wang, X.; et al. KRASness and PIK3CAness in Patients with Advanced Colorectal Cancer: Outcome after Treatment with Early-Phase Trials with Targeted Pathway Inhibitors. PLoS ONE 2012, 7, e38033. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Sun, T.; Kang, P.; Qian, K.; Deng, B.; Zhou, J.; Wang, R.; Jiang, B.; Li, K.; Liu, F.; et al. Combined Analysis of Rearrangement of ALK, ROS1, Somatic Mutation of EGFR, KRAS, BRAF, PIK3CA, and MRNA Expression of ERCC1, TYMS, RRM1, TUBB3, EGFR in Patients with Non-Small Cell Lung Cancer and Their Clinical Significance. Cancer Chemother. Pharmacol. 2016, 77, 583–593. [Google Scholar] [CrossRef]
- Tominaga, T.; Tsuchiya, T.; Mochinaga, K.; Arai, J.; Yamasaki, N.; Matsumoto, K.; Miyazaki, T.; Nagasaki, T.; Nanashima, A.; Tsukamoto, K.; et al. Epidermal Growth Factor Signals Regulate Dihydropyrimidine Dehydrogenase Expression in EGFR-Mutated Non-Small-Cell Lung Cancer. BMC Cancer 2016, 16, 354. [Google Scholar] [CrossRef]
- Nita, M.E.; Tominaga, O.; Nagawa, H.; Tsuruo, T.; Muto, T. Dihydropyrimidine Dehydrogenase but Not Thymidylate Synthase Expression Is Associated with Resistance to 5-Fluorouracil in Colorectal Cancer. Hepatogastroenterology 1998, 45, 2117–2122. [Google Scholar]
- Jensen, S.A.; Vainer, B.; Sørensen, J.B. The Prognostic Significance of Thymidylate Synthase and Dihydropyrimidine Dehydro-genase in Colorectal Cancer of 303 Patients Adjuvantly Treated with 5-Fluorouracil. Int. J. Cancer 2007, 120, 694–701. [Google Scholar] [CrossRef]
- Kornmann, M.; Schwabe, W.; Sander, S.; Kron, M.; Sträter, J.; Polat, S.; Kettner, E.; Weiser, H.F.; Baumann, W.; Schramm, H.; et al. Thymidylate Synthase and Dihydropyrimidine Dehydrogenase MRNA Expression Levels: Predictors for Survival in Colorectal Cancer Patients Receiving Adjuvant 5-Fluorouracil. Clin. Cancer Res. 2003, 9, 4116–4124. [Google Scholar] [PubMed]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.-Y.; Wu, C.-H.; Huang, C.-M.; Chung, F.-Y.; Huang, C.-W.; Tsai, H.-L.; Chen, C.-F.; Lin, S.-R.; Wang, J.-Y. DPYD, TYMS, TYMP, TK1, and TK2 Genetic Expressions as Response Markers in Locally Advanced Rectal Cancer Patients Treated with Fluoropyrimidine-Based Chemoradiotherapy. Biomed. Res. Int. 2013, 931028. [Google Scholar] [CrossRef] [PubMed]
- Genomics of Drug Sensitivity in Cancer. Available online: https://www.cancerrxgene.org/ (accessed on 30 October 2023).
- R Core Team, R. A Language and Environment for Statistical Computing (2021); R Foundation for Statistical Computing: Vienna, Austria. Available online: https://www.R-project.org/ (accessed on 30 October 2023).
- Hitre, E.; Budai, B.; Adleff, V.; Czeglédi, F.; Horváth, Z.; Gyergyay, F.; Lövey, J.; Kovács, T.; Orosz, Z.; Láng, I.; et al. Influence of Thymidylate Synthase Gene Polymorphisms on the Survival of Colorectal Cancer Patients Receiving Ad-juvant 5-Fluorouracil. Pharmacogenet. Genom. 2005, 15, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Varghese, V.; Magnani, L.; Harada-Shoji, N.; Mauri, F.; Szydlo, R.M.; Yao, S.; Lam, E.W.-F.; Kenny, L.M. FOXM1 Modulates 5-FU Resistance in Colorectal Cancer through Regulating TYMS Expression. Sci. Rep. 2019, 9, 1505. [Google Scholar] [CrossRef] [PubMed]
- Ntavatzikos, A.; Spathis, A.; Patapis, P.; Machairas, N.; Peros, G.; Konstantoudakis, S.; Leventakou, D.; Panayiotides, I.G.; Karakitsos, P.; Koumarianou, A. Integrating TYMS, KRAS and BRAF Testing in Patients with Metastatic Colorectal Cancer. World J. Gastroenterol. 2017, 23, 5913. [Google Scholar] [CrossRef]
- Ntavatzikos, A.; Spathis, A.; Patapis, P.; Machairas, N.; Vourli, G.; Peros, G.; Papadopoulos, I.; Panayiotides, I.; Koumarianou, A. TYMS/KRAS/BRAF Molecular Profiling Predicts Survival Following Adjuvant Chemotherapy in Colorectal Cancer. World J. Gastrointest. Oncol. 2019, 11, 551–566. [Google Scholar] [CrossRef]
- André, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Bonetti, A.; Clingan, P.; Bridgewater, J.; Rivera, F.; et al. Improved Overall Survival With Oxaliplatin, Fluorouracil, and Leucovorin As Adjuvant Treatment in Stage II or III Colon Cancer in the MOSAIC Trial. J. Clin. Oncol. 2009, 27, 3109–3116. [Google Scholar] [CrossRef]
- Shi, T.; Gao, M.; He, M.; Yue, F.; Zhao, Y.; Sun, M.; He, K.; Chen, L. 5-FU Preferably Induces Apoptosis in BRAF V600E Colorectal Cancer Cells via Downregulation of Bcl-XL. Mol. Cell. Biochem. 2019, 461, 151–158. [Google Scholar] [CrossRef]
- Wang, C.; Sandhu, J.; Tsao, A.; Fakih, M. Presence of Concurrent TP53 Mutations Is Necessary to Predict Poor Outcomes within the SMAD4 Mutated Subgroup of Metastatic Colorectal Cancer. Cancers 2022, 14, 3644. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency |
|---|---|
| Gender | |
| Female | 32 (50.8%) |
| Male | 31 (49.2%) |
| Age | |
| Mean (SD) | 63.3 (12.4) |
| Median [Min, Max] | 66.4 [30.4, 81.8] |
| Histology | |
| Adenocarcinoma | 57 (90.5%) |
| Adenocarcinoma Mucinous | 6 (9.5%) |
| Localization | |
| Left | 46 (73.0%) |
| Right | 15 (17.5%) |
| N.D. * | 2 (3.2%) |
| Liver metastases | |
| Yes | 46 (73.0%) |
| No | 14 (22.2%) |
| N.D. * | 3 (4.8%) |
| Colectomy | |
| Yes | 56 (88.9%) |
| No | 7 (11.1%) |
| Metastasectomy | |
| Yes | 27 (42.9%) |
| No | 21 (33.3%) |
| N.D. * | 15 (23.8%) |
| Radiotherapy | |
| Yes | 11 (17.5%) |
| No | 52 (82.5%) |
| Monoclonal antibodies therapy | |
| Yes | 14 (22.2%) |
| No | 49 (77.8%) |
| First line of treatment | |
| CapeOx | 26 (41.3%) |
| Folfox | 32 (50.8%) |
| Folfiri | 5 (7.9) |
| Second line of treatment (FOLFOX or FOLFIRI) | |
| Yes | 37 (56.8%) |
| No | 26 (41.3%) |
| Variable | Frequency |
|---|---|
| TYMS 3′UTR 6bp ins-del (rs151264360) | |
| DEL/DEL | 31 (49.2%) |
| INS/DEL | 32 (50.8%) |
| GSTP1 c.313A>G (rs1695) | |
| A/A | 20 (31.7%) |
| G/A | 28 (44.4%) |
| G/G | 15 (23.8%) |
| DPYD c.1905+1 G>A (DPYD*2) (rs3918290) | |
| G/G | 63 (100%) |
| G/A | 0 (0%) |
| A/A | 0 (0%) |
| c.2846A>T (rs67376798) | |
| A/A | 1 (1.6%) |
| T/A | 1 (1.6%) |
| T/T | 61 (96.8%) |
| c.1679T>G (DPYD*13) (rs55886062) | |
| T/T | 63 (100%) |
| T/G | 0 (0%) |
| G/G | 0 (0%) |
| c.85T>C (DPYD*9) (rs1801265) | |
| T/T | 37 (58.7%) |
| C/T | 19 (30.2%) |
| C/C | 6 (9.5%) |
| N.D. | 1 (1.6%) |
| ABCB1 c.3435C>T (rs1045642) | |
| T/T | 9 (14.3%) |
| C/T | 31 (49.2%) |
| C/C | 21 (33.3%) |
| N.D. | 2 (3.2%) |
| c.1236 T>C (rs1128503) | |
| T/T | 6 (9.5%) |
| C/T | 41 (65.1%) |
| C/C | 15 (23.8%) |
| N.D | 1 (1.6%) |
| ABCC2 c.-24C>T (rs717620) | |
| C/C | 46 (73.0%) |
| C/T | 11 (17.5%) |
| T/T | 2 (3.2%) |
| N.D. | 4 (6.3%) |
| MTHFR c.1409A>C (rs1801131) | |
| A/A | 33 (52.4%) |
| A/C | 21 (33.3%) |
| C/C | 8 (12.7%) |
| N.D. | 1 (1.6%) |
| Tumor Mutation | Frequency |
|---|---|
| BRAF | |
| Mutated (V600E) | 7 (11.1%) |
| Wild-type | 58 (88.9%) |
| KRAS mutations * | |
| Mutated | 22 (34.9%) |
| Wild-type | 41 (65.1%) |
| NRAS mutations ** | |
| Mutated | 7 (11.1%) |
| Wild-type | 56 (88.9%) |
| PI3KCA mutations *** | |
| Mutated | 7 (11.1%) |
| Wild-type | 56 (88.9%) |
| AKT1 E17K | |
| Mutated | 2 (3.2%) |
| Wild-type | 61 (96.8%) |
| Variables | Patients (n) | HR | 95% CI Lower-Upper | p-Value ** |
|---|---|---|---|---|
| Liver metastases | ||||
| Yes | 46 | 3.51 | 1.52–8.07 | 0.003 |
| No | 14 | Ref. | ||
| Colectomy | ||||
| Yes | 56 | 0.480 | 0.214–1.08 | 0.079 |
| No | 7 | Ref. | ||
| GSTP1 rs1695 | ||||
| Yes (G/G) | 15 | 0.484 | 0.234–1.00 | 0.05 |
| No (G/A+A/A) | 48 | Ref. | ||
| DPYD rs1801265 | ||||
| Yes (C/C + C/T) | 25 | 1.819 | 1.03–3.19 | 0.0377 |
| No (T/T) | 37 | Ref. | ||
| ABCB1 rs1045642 | ||||
| Yes C/C | 21 | 1.782 | 1.00–3.16 | 0.0483 |
| No (C/T+T/T) | 40 | Ref. | ||
| MTHFR rs180113 | ||||
| Yes C/C | 6 | 2.295 | 1.05–4.97 | 0.0352 |
| No (A/C+A/A) | 54 | Ref. | ||
| TYMS rs151264360 | ||||
| Yes Ins/Del | 32 | 2.169 | 1.21–3.86 | 0.0087 |
| No Del/Del | 31 | Ref. | ||
| Mutated PI3KCA | ||||
| Yes | 7 | 0.271 | 0.084–0.876 | 0.0292 |
| No | 56 | Ref. | ||
| BRAF | ||||
| Wild-type | 56 | 0.28 | 0.087–0.909 | 0.034 |
| Mutated (V600E) | 7 | Ref. | ||
| High-Risk Profile *** | ||||
| Yes | 41 | 2.06 | 1.13–3.74 | 0.018 |
| No | 21 | Ref. | ||
| High-Risk Profile *** + BRAF wild-type patients | ||||
| Yes | 38 | 2.80 | 1.55–5.06 | <0.005 |
| No | 25 | Ref. |
| Variables | Patients (n) | HR | 95% CI Lower-Upper | p-Value * |
|---|---|---|---|---|
| Liver metastases | ||||
| Yes | 45 | 3.69 | 1.49–9.09 | 0.004 |
| No | 13 | Ref. | ||
| DPYDrs1801265 | ||||
| Yes (C/C + C/T) | 23 | 1.88 | 0.99–3.54 | 0.052 |
| No (T/T) | 35 | |||
| ABCB1 rs1045642 | ||||
| Yes C/C | 20 | 2.62 | 1.37–4.99 | 0.003 |
| No C/T + T/T | 38 | Ref. | ||
| MTHFR rs180113 | ||||
| Yes C/C | 8 | 2.63 | 1.13–6.15 | 0.004 |
| No A/C + A/A | 50 | Ref. |
| a. High-Risk Profile * and BRAF V600E Mutation. | ||||
|---|---|---|---|---|
| Variables | Patients (n) | HR | 95% CI Lower-Upper | p-Value ** |
| High-risk presence | ||||
| Yes | 38 | 2.18 | 1.15–4.11 | 0.017 |
| No | 20 | Ref. | ||
| Liver metastases | ||||
| Yes | 45 | 3.34 | 1.39–8.05 | 0.006 |
| No | 13 | Ref | ||
| BRAF V600E | ||||
| Mutated | 7 | 0.41 | 0.12–1.39 | 0.153 |
| Wild-type | 51 | Ref. | ||
| b. High-risk profile * and KRAS mutation. | ||||
| Variables | Patients (n) | HR | 95% CI Lower-Upper | p-value ** |
| High-risk presence | ||||
| Yes | 38 | 2.28 | 1.20–4.33 | 0.012 |
| No | 20 | Ref. | ||
| Liver metastases | ||||
| Yes | 45 | 4.71 | 1.91–11.6 | <0.005 |
| No | 13 | Ref | ||
| KRAS | ||||
| Mutated | 21 | 0.59 | 0.31–1.11 | 0.105 |
| Wild-type | 37 | Ref. | ||
| c. High-risk profile * and PI3KCA mutation. | ||||
| Variables | Patients (n) | HR | 95% CI Lower-Upper | p-value ** |
| High-risk presence | ||||
| Yes | 38 | 2.43 | 1.26–4.66 | 0.007 |
| No | 20 | Ref. | ||
| Liver metastases | ||||
| Yes | 45 | 4.08 | 1.68–9.86 | 0.002 |
| No | 13 | Ref | ||
| PI3KCA | ||||
| Mutated | 6 | 0.22 | 0.05–0.95 | 0.042 |
| Wild-type | 52 | Ref. | ||
| Variables | Patients (n) | HR | 95% CI Lower-Upper | p-Value * |
|---|---|---|---|---|
| High-risk ** + BRAF wild-type patients | ||||
| Yes | 35 | 2.71 | 1.46–5.01 | 0.001 |
| No | 23 | Ref. | ||
| Liver metastases | ||||
| Yes | 45 | 3.55 | 1.52–8.29 | 0.003 |
| No | 13 | Ref |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cayún, J.P.; Cerpa, L.C.; Colombo, A.; Cáceres, D.D.; Leal, J.L.; Reyes, F.; Gutiérrez-Cáceres, C.; Calfunao, S.; Varela, N.M.; Quiñones, L.A. Genetic Polymorphisms and Tumoral Mutational Profiles over Survival in Advanced Colorectal Cancer Patients: An Exploratory Study. Curr. Oncol. 2024, 31, 274-295. https://doi.org/10.3390/curroncol31010018
Cayún JP, Cerpa LC, Colombo A, Cáceres DD, Leal JL, Reyes F, Gutiérrez-Cáceres C, Calfunao S, Varela NM, Quiñones LA. Genetic Polymorphisms and Tumoral Mutational Profiles over Survival in Advanced Colorectal Cancer Patients: An Exploratory Study. Current Oncology. 2024; 31(1):274-295. https://doi.org/10.3390/curroncol31010018
Chicago/Turabian StyleCayún, Juan Pablo, Leslie Carol Cerpa, Alicia Colombo, Dante Daniel Cáceres, José Luis Leal, Felipe Reyes, Carolina Gutiérrez-Cáceres, Susan Calfunao, Nelson Miguel Varela, and Luis Abel Quiñones. 2024. "Genetic Polymorphisms and Tumoral Mutational Profiles over Survival in Advanced Colorectal Cancer Patients: An Exploratory Study" Current Oncology 31, no. 1: 274-295. https://doi.org/10.3390/curroncol31010018
APA StyleCayún, J. P., Cerpa, L. C., Colombo, A., Cáceres, D. D., Leal, J. L., Reyes, F., Gutiérrez-Cáceres, C., Calfunao, S., Varela, N. M., & Quiñones, L. A. (2024). Genetic Polymorphisms and Tumoral Mutational Profiles over Survival in Advanced Colorectal Cancer Patients: An Exploratory Study. Current Oncology, 31(1), 274-295. https://doi.org/10.3390/curroncol31010018