Efficacy and Safety of Anti-HER2 Targeted Therapy for Metastatic HR-Positive and HER2-Positive Breast Cancer: A Bayesian Network Meta-Analysis


Abstract
:1. Introduction
2. Methods
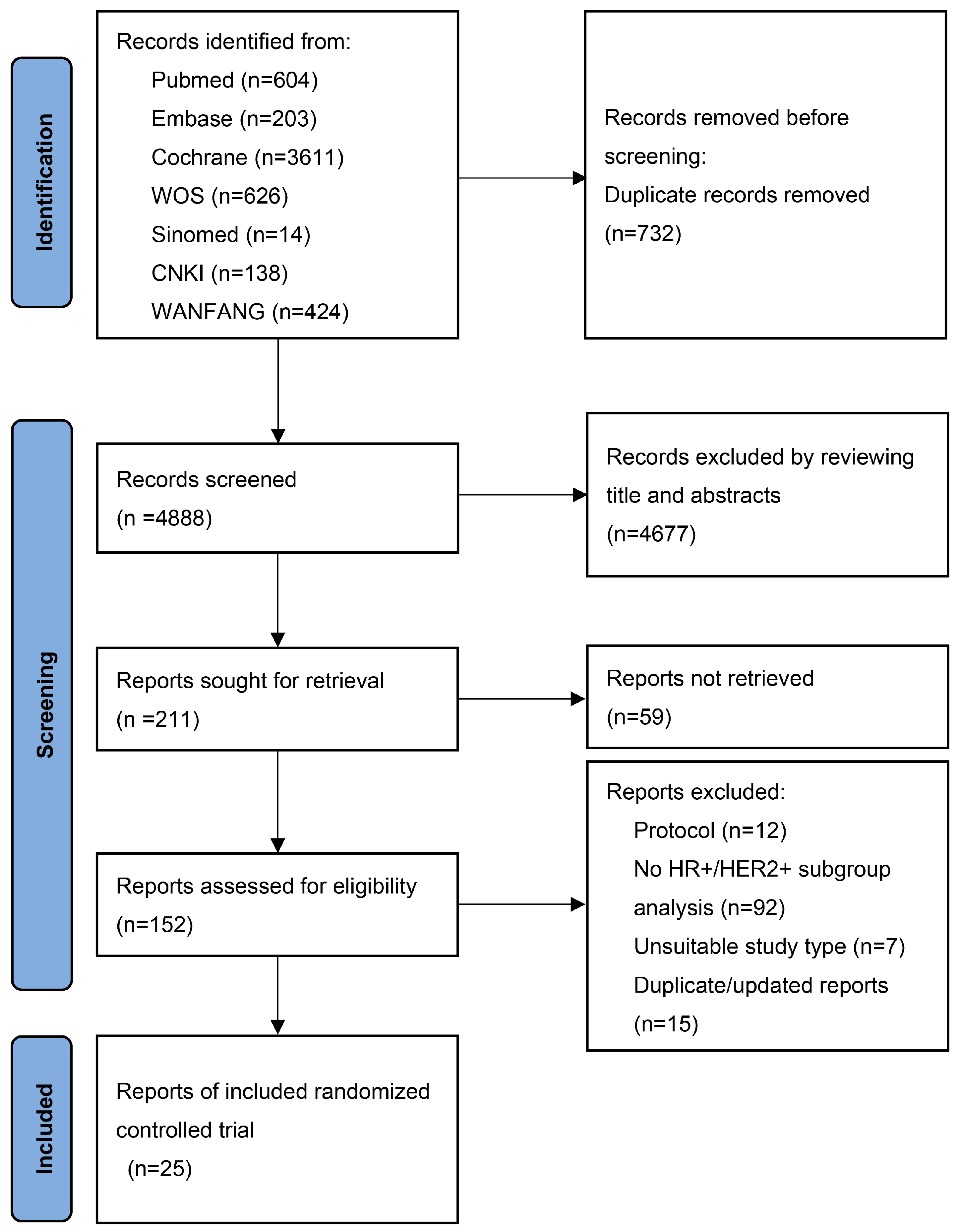
2.1. Search Strategy and Selection Criteria
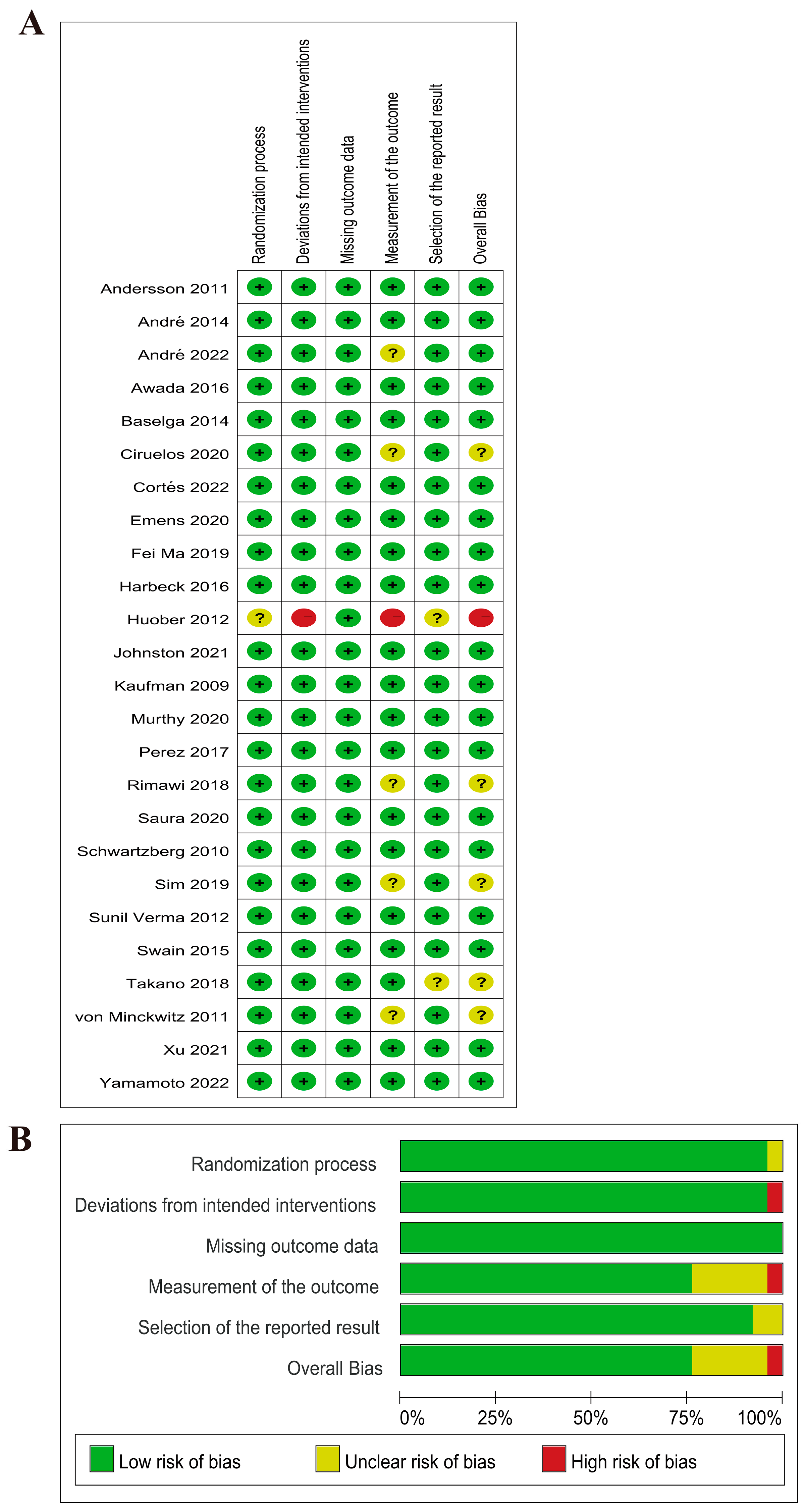
2.2. Data Extraction and Quality Assessment
2.3. Data Synthesis and Statistical Analysis
2.4. Subgroup Analysis
3. Results
3.1. Characteristics of the Included Study
3.2. Network Meta-Analysis
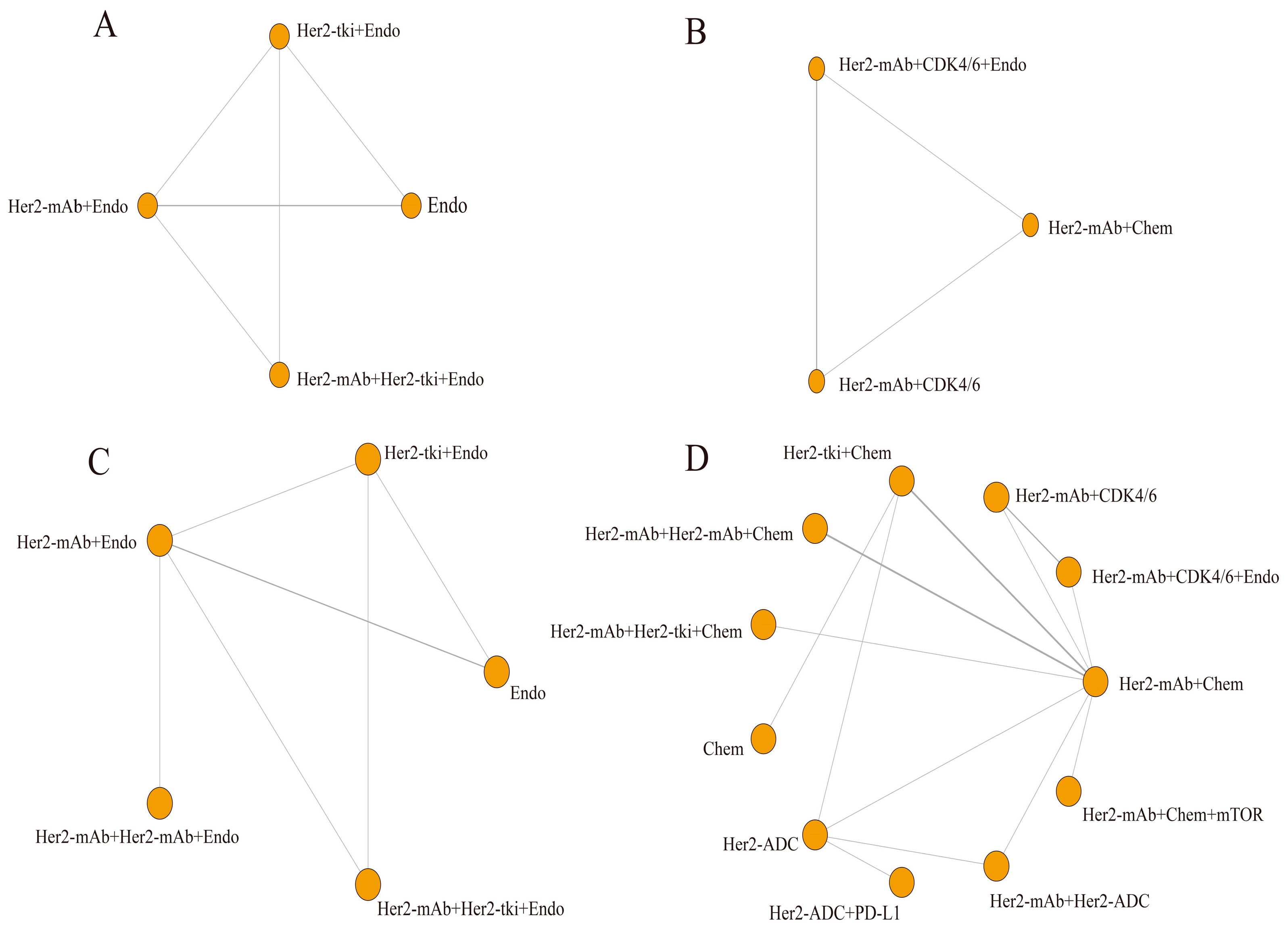
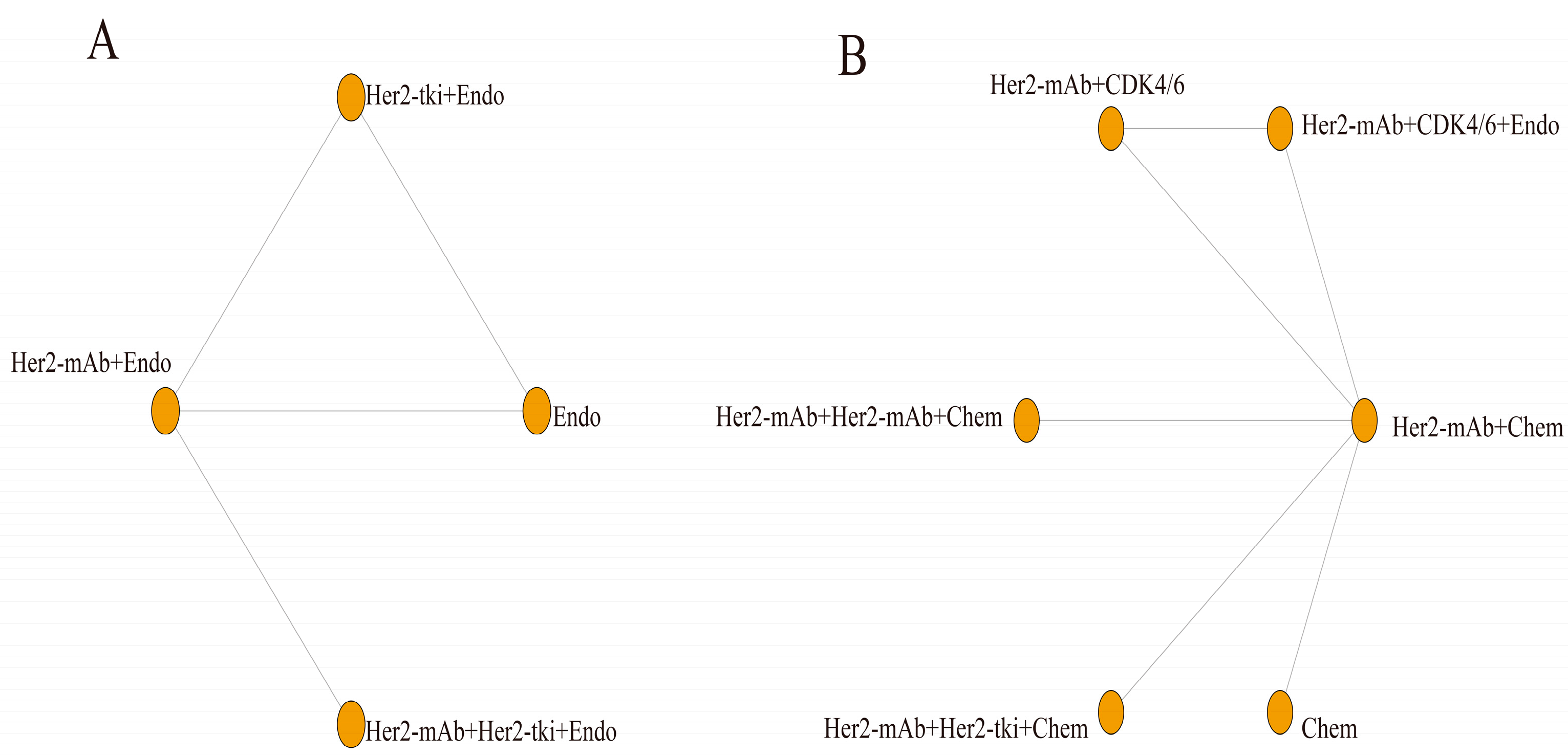
3.2.1. Network Diagrams
3.2.2. Efficacy
3.2.3. Safety
3.2.4. Inconsistency
3.2.5. Subgroup and Sensitivity Analyses
3.2.6. Small-Study Effects
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABC | Advanced Breast Cancer |
| ADC | Antibody-Drug Conjugate |
| AEs | Adverse Events |
| AI | Aromatase Inhibitor |
| Akt | Protein Kinase B |
| CDK4/6 | Cyclin-Dependent Kinase 4/6 |
| CNS | Central Nervous System |
| CrI | Credible Interval |
| DIC | Error Information Criterion |
| EMA | European Medicines Agency |
| Endo | Endocrine Therapy |
| ER+ | Estrogen Receptor Positive |
| ErbB | Human Epidermal Growth Factor Receptor |
| HER2+ | Epidermal Growth Factor Receptor 2 Positive |
| Her2-ADC | Anti-Her2 Antibody-Drug Conjugate |
| Her2-mAb | Anti-Her2 Monoclonal Antibody |
| Her2-tki | Anti-Her2 Tyrosine Kinase Inhibitor |
| HR | Hazard Ratio |
| HRs | Hormone Receptors |
| mAb | Monoclonal Antibody |
| MBC | Metastatic Breast Cancer |
| mTOR | Mammalian Target of Rapamycin |
| NCCN | National Comprehensive Cancer Network |
| NMA | Network Meta-Analysis |
| OR | Odds Ratio |
| ORR | Objective Response Rate |
| OS | Overall Survival |
| p-Akt | Phosphorylated Akt |
| PD-1 | Programmed Death 1 |
| PD-L1 | Programmed Death Ligand 1 |
| PFS | Progression-Free Survival |
| PR+ | Progesterone Receptor Positive |
| SUCRA | Surface Under the Cumulative Ranking Curve |
| T-DM1 | Trastuzumab Emtansine |
| T-DXd | Trastuzumab Deruxtecan |
| TKI | Tyrosine Kinase Inhibitor |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Ca-Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Dieci, M.V.; Guarneri, V. Should triple-positive breast cancer be recognized as a distinct subtype? Expert. Rev. Anticancer Ther. 2020, 20, 1011–1014. [Google Scholar] [CrossRef]
- Gradishar, W.J.; Anderson, B.O.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Blair, S.L.; Burstein, H.J.; Dang, C.; Elias, A.D.; et al. Breast Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 452–478. [Google Scholar] [CrossRef]
- Kaufman, B.; Mackey, J.R.; Clemens, M.R.; Bapsy, P.P.; Vaid, A.; Wardley, A.; Tjulandin, S.; Jahn, M.; Lehle, M.; Feyereislova, A.; et al. Trastuzumab Plus Anastrozole Versus Anastrozole Alone for the Treatment of Postmenopausal Women With Human Epidermal Growth Factor Receptor 2–Positive, Hormone Receptor–Positive Metastatic Breast Cancer: Results From the Randomized Phase III TAnDEM Study. J. Clin. Oncol. 2009, 27, 5529–5537. [Google Scholar] [CrossRef] [PubMed]
- Schwartzberg, L.S.; Franco, S.X.; Florance, A.; O’Rourke, L.; Maltzman, J.; Johnston, S. Lapatinib plus Letrozole as First-Line Therapy for HER-2+ Hormone Receptor–Positive Metastatic Breast Cancer. Oncologist 2010, 15, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Huober, J.; Fasching, P.A.; Barsoum, M.; Petruzelka, L.; Wallwiener, D.; Thomssen, C.; Reimer, T.; Paepke, S.; Azim, H.A.; Ragosch, V.; et al. Higher efficacy of letrozole in combination with trastuzumab compared to letrozole monotherapy as first-line treatment in patients with HER2-positive, hormone-receptor-positive metastatic breast cancer—Results of the eLEcTRA trial. Breast 2012, 21, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.R.D.; Hegg, R.; Im, S.; Park, I.H.; Burdaeva, O.; Kurteva, G.; Press, M.F.; Tjulandin, S.; Iwata, H.; Simon, S.D.; et al. Phase III, Randomized Study of Dual Human Epidermal Growth Factor Receptor 2 (HER2) Blockade With Lapatinib Plus Trastuzumab in Combination With an Aromatase Inhibitor in Postmenopausal Women With HER2-Positive, Hormone Receptor–Positive Metastatic Breast Cancer: Updated Results of ALTERNATIVE. J. Clin. Oncol. 2021, 39, 79–89. [Google Scholar] [CrossRef]
- Rimawi, M.; Ferrero, J.M.; de la Haba-Rodriguez, J.; Poole, C.; De Placido, S.; Osborne, C.K.; Hegg, R.; Easton, V.; Wohlfarth, C.; Arpino, G.; et al. First-Line Trastuzumab Plus an Aromatase Inhibitor, With or Without Pertuzumab, in Human Epidermal Growth Factor Receptor 2–Positive and Hormone Receptor–Positive Metastatic or Locally Advanced Breast Cancer (PERTAIN):A Randomized, Open-Label Phase II Trial. J. Clin. Oncol. 2018, 28, 2826–2835. [Google Scholar] [CrossRef]
- Kay, C.; Martínez-Pérez, C.; Meehan, J.; Gray, M.; Webber, V.; Dixon, J.M.; Turnbull, A.K. Current trends in the treatment of HR+/HER2+ breast cancer. Future Oncol. 2021, 17, 1665–1681. [Google Scholar] [CrossRef]
- Feng, F.; Zhang, T.; Yin, F.; Liu, C.; Zhuang, J.; Qi, L.; Wang, X.; Li, J.; Wang, L.; Tian, J.; et al. Efficacy and safety of targeted therapy for metastatic HER2-positive breast cancer in the first-line treatment: A Bayesian network meta-analysis. Oncotargets Ther. 2019, 12, 959–974. [Google Scholar] [CrossRef]
- Zhang, X.; Leng, J.; Zhou, Y.; Mao, F.; Lin, Y.; Shen, S.; Sun, Q. Efficacy and Safety of Anti-HER2 Agents in Combination With Chemotherapy for Metastatic HER2-Positive Breast Cancer Patient: A Network Meta-Analysis. Front. Oncol. 2021, 11, 731210. [Google Scholar] [CrossRef] [PubMed]
- Sadeghirad, B.; Foroutan, F.; Zoratti, M.J.; Busse, J.W.; Brignardello-Petersen, R.; Guyatt, G.; Thabane, L. Theory and practice of Bayesian and frequentist frameworks for network meta-analysis. BMJ Evid.-Based Med. 2023, 28, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.R.; Kim, S.J.; Lee, J.; Rucker, G. Network meta-analysis: Application and practice using R software. Epidemiol. Health 2019, 41, e2019013. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ-Brit. Med. J. 2021, 372, n71. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ-Brit. Med. J. 2010, 340, c332. [Google Scholar] [CrossRef]
- Andre, F.; Nadal, J.C.; Denys, H.; Goel, S.; Litchfield, L.M.; Appiah, A.; Chen, Y.; Tolaney, S.M. LBA18 Final overall survival (OS) for abemaciclib plus trastuzumab +/− fulvestrant versus trastuzumab plus chemotherapy in patients with HR+, HER2+ advanced breast cancer (monarcHER): A randomized, open-label, phase II trial. Ann. Oncol. 2022, 33, S1386–S1387. [Google Scholar] [CrossRef]
- Takano, T.; Tsurutani, J.; Takahashi, M.; Yamanaka, T.; Sakai, K.; Ito, Y.; Fukuoka, J.; Kimura, H.; Kawabata, H.; Tamura, K.; et al. A randomized phase II trial of trastuzumab plus capecitabine versus lapatinib plus capecitabine in patients with HER2-positive metastatic breast cancer previously treated with trastuzumab and taxanes: WJOG6110B/ELTOP. Breast 2018, 40, 67–75. [Google Scholar] [CrossRef]
- Awada, A.; Colomer, R.; Inoue, K.; Bondarenko, I.; Badwe, R.A.; Demetriou, G.; Lee, S.C.; Mehta, A.O.; Kim, S.B.; Bachelot, T.; et al. Neratinib Plus Paclitaxel vs Trastuzumab Plus Paclitaxel in Previously Untreated Metastatic ERBB2-Positive Breast Cancer: The NEfERT-T Randomized Clinical Trial. JAMA Oncol. 2016, 2, 1557–1564. [Google Scholar] [CrossRef]
- Harbeck, N.; Huang, C.S.; Hurvitz, S.; Yeh, D.C.; Shao, Z.; Im, S.A.; Jung, K.H.; Shen, K.; Ro, J.; Jassem, J.; et al. Afatinib plus vinorelbine versus trastuzumab plus vinorelbine in patients with HER2-overexpressing metastatic breast cancer who had progressed on one previous trastuzumab treatment (LUX-Breast 1): An open-label, randomised, phase 3 trial. Lancet Oncol. 2016, 17, 357–366. [Google Scholar] [CrossRef]
- Swain, S.M.; Baselga, J.; Kim, S.B.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.M.; Schneeweiss, A.; Heeson, S.; et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N. Engl. J. Med. 2015, 372, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Lidbrink, E.; Bjerre, K.; Wist, E.; Enevoldsen, K.; Jensen, A.B.; Karlsson, P.; Tange, U.B.; Sørensen, P.G.; Møller, S.; et al. Phase III Randomized Study Comparing Docetaxel Plus Trastuzumab With Vinorelbine Plus Trastuzumab As First-Line Therapy of Metastatic or Locally Advanced Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer: The HERNATA Study. J. Clin. Oncol. 2011, 29, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Baselga, J.; Manikhas, A.; Cortés, J.; Llombart, A.; Roman, L.; Semiglazov, V.F.; Byakhov, M.; Lokanatha, D.; Forenza, S.; Goldfarb, R.H.; et al. Phase III trial of nonpegylated liposomal doxorubicin in combination with trastuzumab and paclitaxel in HER2-positive metastatic breast cancer. Ann. Oncol. 2014, 25, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Fei Ma, M.; Quchang Ouyang, M.; Wei Li, M.; Zefei Jiang, M.; Zhongsheng Tong, M.; Yunjiang Liu, M.; Huiping Li, M.P.; Shiying Yu, M.; Jifeng Feng, M.; Shusen Wang, M.; et al. Pyrotinib or Lapatinib Combined With Capecitabine in HER2–Positive Metastatic Breast Cancer With Prior Taxanes, Anthracyclines, and/or Trastuzumab: A Randomized, Phase II Study. J. Clin. Oncol. 2019, 29, 2610–2619. [Google Scholar] [CrossRef]
- Murthy, R.K.; Loi, S.; Okines, A.; Paplomata, E.; Hamilton, E.; Hurvitz, S.A.; Lin, N.U.; Borges, V.; Abramson, V.; Anders, C.; et al. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N. Engl. J. Med. 2020, 382, 597–609. [Google Scholar] [CrossRef]
- Sim, S.H.; Park, I.H.; Jung, K.H.; Kim, S.; Ahn, J.; Lee, K.; Im, S.; Im, Y.; Park, Y.H.; Sohn, J.; et al. Randomised Phase 2 study of lapatinib and vinorelbine vs vinorelbine in patients with HER2 + metastatic breast cancer after lapatinib and trastuzumab treatment (KCSG BR11-16). Brit. J. Cancer 2019, 121, 985–990. [Google Scholar] [CrossRef]
- von Minckwitz, G.; Schwedler, K.; Schmidt, M.; Barinoff, J.; Mundhenke, C.; Cufer, T.; Maartense, E.; de Jongh, F.E.; Baumann, K.H.; Bischoff, J.; et al. Trastuzumab beyond progression: Overall survival analysis of the GBG 26/BIG 3-05 phase III study in HER2-positive breast cancer. Eur. J. Cancer 2011, 47, 2273–2281. [Google Scholar] [CrossRef]
- Sunil Verma, M.D.D.M. Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. N. Engl. J. Med. 2012, 19, 1783–1791. [Google Scholar] [CrossRef]
- Emens, L.A.; Esteva, F.J.; Beresford, M.; Saura, C.; De Laurentiis, M.; Kim, S.B.; Im, S.A.; Wang, Y.; Salgado, R.; Mani, A.; et al. Trastuzumab emtansine plus atezolizumab versus trastuzumab emtansine plus placebo in previously treated, HER2-positive advanced breast cancer (KATE2): A phase 2, multicentre, randomised, double-blind trial. Lancet Oncol. 2020, 21, 1283–1295. [Google Scholar] [CrossRef]
- Perez, E.A.; Barrios, C.; Eiermann, W.; Toi, M.; Im, Y.; Conte, P.; Martin, M.; Pienkowski, T.; Pivot, X.; Burris, H.A.; et al. Trastuzumab Emtansine With or Without Pertuzumab Versus Trastuzumab Plus Taxane for Human Epidermal Growth Factor Receptor 2–Positive, Advanced Breast Cancer: Primary Results From the Phase III MARIANNE Study. J. Clin. Oncol. 2017, 35, 141–148. [Google Scholar] [CrossRef]
- Xu, B.; Yan, M.; Ma, F.; Hu, X.; Feng, J.; Ouyang, Q.; Tong, Z.; Li, H.; Zhang, Q.; Sun, T.; et al. Updated overall survival (OS) results from the phase 3 PHOEBE trial of pyrotinib versus la patinib in combination with capecitabine in patients with HER2-positive metastatic breast cancer. In Proceedings of the San Antonio Breast Cancer Symposium (SABCS), San Antonio, TX, USA, 6–10 December 2022; Volume 82. [Google Scholar]
- Ciruelos, E.; Villagrasa, P.; Pascual, T.; Oliveira, M.; Pernas, S.; Paré, L.; Escrivá-de-Romaní, S.; Manso, L.; Adamo, B.; Martínez, E.; et al. Palbociclib and Trastuzumab in HER2-Positive Advanced Breast Cancer: Results from the Phase II SOLTI-1303 PATRICIA Trial. Clin. Cancer Res. 2020, 26, 5820–5829. [Google Scholar] [CrossRef]
- Cortés, J.; Kim, S.B.; Chung, W.P.; Im, S.A.; Park, Y.H.; Hegg, R.; Kim, M.H.; Tseng, L.M.; Petry, V.; Chung, C.F.; et al. Trastuzumab Deruxtecan versus Trastuzumab Emtansine for Breast Cancer. N. Engl. J. Med. 2022, 386, 1143–1154. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Iwata, H.; Taira, N.; Masuda, N.; Takahashi, M.; Yoshinami, T.; Ueno, T.; Toyama, T.; Yamanaka, T.; Takano, T.; et al. Pertuzumab retreatment for HER2-positive advanced breast cancer: A randomized, open-label phase III study (PRECIOUS). Cancer Sci. 2022, 113, 3169–3179. [Google Scholar] [CrossRef] [PubMed]
- Saura, C.; Oliveira, M.; Feng, Y.H.; Dai, M.S.; Chen, S.W.; Hurvitz, S.A.; Kim, S.B.; Moy, B.; Delaloge, S.; Gradishar, W.; et al. Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in HER2-Positive Metastatic Breast Cancer Previously Treated With >/= 2 HER2-Directed Regimens: Phase III NALA Trial. J. Clin. Oncol. 2020, 38, 3138–3149. [Google Scholar] [CrossRef] [PubMed]
- André, F.; O’Regan, R.; Ozguroglu, M.; Toi, M.; Xu, B.; Jerusalem, G.; Masuda, N.; Wilks, S.; Arena, F.; Isaacs, C.; et al. Everolimus for women with trastuzumab-resistant, HER2-positive, advanced breast cancer (BOLERO-3): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet Oncol. 2014, 15, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Scheuer, W.; Friess, T.; Burtscher, H.; Bossenmaier, B.; Endl, J.; Hasmann, M. Strongly enhanced antitumor activity of trastuzumab and pertuzumab combination treatment on HER2-positive human xenograft tumor models. Cancer Res. 2009, 69, 9330–9336. [Google Scholar] [CrossRef]
- Nahta, R.; Hung, M.C.; Esteva, F.J. The HER-2-targeting antibodies trastuzumab and pertuzumab synergistically inhibit the survival of breast cancer cells. Cancer Res. 2004, 64, 2343–2346. [Google Scholar] [CrossRef]
- Swain, S.M.; Miles, D.; Kim, S.B.; Im, Y.H.; Im, S.A.; Semiglazov, V.; Ciruelos, E.; Schneeweiss, A.; Loi, S.; Monturus, E.; et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): End-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2020, 21, 519–530. [Google Scholar] [CrossRef]
- Miles, D.; Ciruelos, E.; Schneeweiss, A.; Puglisi, F.; Peretz-Yablonski, T.; Campone, M.; Bondarenko, I.; Nowecki, Z.; Errihani, H.; Paluch-Shimon, S.; et al. Final results from the PERUSE study of first-line pertuzumab plus trastuzumab plus a taxane for HER2-positive locally recurrent or metastatic breast cancer, with a multivariable approach to guide prognostication. Ann. Oncol. 2021, 32, 1245–1255. [Google Scholar] [CrossRef]
- Xia, W.; Gerard, C.M.; Liu, L.; Baudson, N.M.; Ory, T.L.; Spector, N.L. Combining lapatinib (GW572016), a small molecule inhibitor of ErbB1 and ErbB2 tyrosine kinases, with therapeutic anti-ErbB2 antibodies enhances apoptosis of ErbB2-overexpressing breast cancer cells. Oncogene 2005, 24, 6213–6221. [Google Scholar] [CrossRef]
- Giampaglia, M.; Chiuri, V.E.; Tinelli, A.; De Laurentiis, M.; Silvestris, N.; Lorusso, V. Lapatinib in breast cancer: Clinical experiences and future perspectives. Cancer Treat. Rev. 2010, 36 (Suppl. S3), S72–S79. [Google Scholar] [CrossRef] [PubMed]
- Arteaga, C.L.; Sliwkowski, M.X.; Osborne, C.K.; Perez, E.A.; Puglisi, F.; Gianni, L. Treatment of HER2-positive breast cancer: Current status and future perspectives. Nat. Rev. Clin. Oncol. 2011, 9, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Freedman, R.A.; Gelman, R.S.; Anders, C.K.; Melisko, M.E.; Parsons, H.A.; Cropp, A.M.; Silvestri, K.; Cotter, C.M.; Componeschi, K.P.; Marte, J.M.; et al. TBCRC 022: A Phase II Trial of Neratinib and Capecitabine for Patients With Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer and Brain Metastases. J. Clin. Oncol. 2019, 37, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, E.; Drago, J.Z.; Modi, S. Implementing antibody-drug conjugates (ADCs) in HER2-positive breast cancer: State of the art and future directions. Breast Cancer Res. 2021, 23, 84. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Trial Name | Study Design | Median Follow-Up (m) | Total pts | Treatment-Line | Median Age | Intervention | Control | Main Outcome |
|---|---|---|---|---|---|---|---|---|---|
| André 2022 [17] | monarcHER | O, R, P2 | 52.9 | 237 | ≥3 | 55.3 | Group 1: Abemaciclib+Trastuzumab+Fulvestrant Group 2: Abemaciclib+Trastuzumab | Trastuzumab+Standard of Care Single Agent Chemotherapy | ORR, PFS, OS, Safety |
| Schwartzberg 2010 [5] | EGF30008 | DB, R, P3 | 22.8 | 219 | 1 | 60 | Letrozole+Lapatinib | Letrozole+Placebo | ORR, PFS, OS, Safety |
| Takano 2018 [18] | WJOG6110B/ELTOP | O, R, P2 | 44.6 | 54 | ≥1 | 58 | Trastuzumab+Capecitabine | Lapatinib+Capecitabine | PFS |
| Awada 2016 [19] | NEfERT-T | O, R, P2 | 23 | 251 | ≥1 | 55 | Neratinib+Paclitaxel | Trastuzumab+Paclitaxel | PFS |
| Harbeck 2016 [20] | LUX-Breast 1 | O, R, P3 | 9.3 | 147 | 1–2 | 52.2 | Afatinib+Vinorelbine | Trastuzumab+Vinorelbine | PFS |
| Rimawi 2018 [8] | PERTAIN | O, R, P2 | 31 | 258 | 1 | 61.6 | Group 1: Pertuzumab+Trastuzumab+Docetaxel/Paclitaxel→AI Group 2: Pertuzumab+Trastuzumab+AI Group 3: Trastuzumab+Docetaxel/Paclitaxel→ AI | Trastuzumab+AI | PFS, Safety |
| Swain 2015 [21] | CLEOPATRA | DB, R, P3 | 50 | 388 | 1 | 53.5 | Pertuzumab+Trastuzumab+Docetaxel | Placebo+Trastuzumab+Docetaxel | PFS, OS, Safety |
| Andersson 2011 [22] | HERNATA | O, R, P3 | 34 | 161 | 1 | 56 | Docetaxel+Trastuzumab | Vinorelbine+Trastuzumab | PFS |
| Baselga 2014 [23] | STM01-102 | O, R, P3 | 31 | 156 | 1 | 53 | Nonpegylated liposomal doxorubicin+Trastuzumab+Paclitaxel | Trastuzumab+Paclitaxel | PFS, OS |
| Johnston 2021 [7] | ALTERNATIVE | M, O, R, P3 | NA | 355 | 1–5 | 57 | Group 1: Trastuzumab+Lapatinib+AI Group 2: Lapatinib+AI | Trastuzumab+AI | ORR, PFS, OS, Safety |
| Fei Ma 2019 [24] | NA | M, R, P2 | 14.9 | 80 | 1–3 | 48 | Pyrotinib+Capecitabine | Lapatinib+Capecitabine | PFS |
| Murthy 2020 [25] | HER2CLIMB | M, DB, R, P2 | 14 | 289 | ≥2 | 55 | Tucatinib+Trastuzumab+Capecitabine | Placebo+Trastuzumab+Capecitabine | PFS, OS |
| Sim 2019 [26] | KCSG BR11-16 | M, O, R, P2 | NA | 59 | ≥2 | 53 | Lapatinib+Vinorelbine | Vinorelbine | PFS |
| von Minckwitz 2011 [27] | GBG 26/BIG 3-05 | M, O, R, P3 | 20.7 | 85 | ≥2 | NA | Trastuzumab+Capecitabine | Capecitabine | OS |
| Sunil Verma 2012 [28] | EMILIA | M, O, R, P3 | 13 | 991 | ≥1 | 53 | T-DM1 | Lapatinib+Capecitabine | PFS |
| Emens 2020 [29] | KATE2 | M, DB, R, P2 | 8.5 | 117 | ≥1 | 54 | T-DM1+Atezolizumab | T-DM1+Placebo | PFS |
| Perez 2017 [30] | MARIANNE | M, O, R, P3 | 35 | 600 | 1 | 53 | Group 1: T-DM1+Pertuzumab Group 2: T-DM1 | Trastuzumab+Taxane | PFS |
| Kaufman 2009 [4] | TAnDEM | M, O, R, P3 | NA | 207 | 1 | 55 | Trastuzumab+Anastrozole | Anastrozole | PFS, OS |
| Xu 2021 [31] | PHOEBE | M, O, R, P3 | 33.2 | 120 | ≥1 | 49.5 | Pyrotinib+Capecitabine | Lapatinib+Capecitabine | PFS, OS |
| Ciruelos 2020 [32] | SOLTI-1303 PATRICIA | M, O, R, P2 | 42.3 | 56 | 3–5 | 58 | Trastuzumab+Palbociclib+Letrozole | Trastuzumab+Palbociclib | ORR, PFS, OS, Safety |
| Cortés 2022 [33] | DESTINY-Breast03 | M, O, R, P3 | 16.2 | 265 | ≥1 | 54.2 | Trastuzumab Deruxtecan | Trastuzumab Emtansine | PFS |
| Yamamoto 2022 [34] | PRECIOUS | M, O, R, P3 | 14.2 | 122 | 3–6 | 58.5 | Pertuzumab+Trastuzumab+physician’s choice chemotherapy (PTC) | Trastuzumab+PTC | PFS |
| Saura 2020 [6,35] | NALA | M, O, R, P3 | 29.9 | 367 | ≥3 | 54.4 | Neratinib+Capecitabine | Lapatinib+Capecitabine | PFS, OS |
| Huober 2012 [6] | eLEcTRA | M, O, R, P3 | NA | 57 | 1 | 62 | Letrozole+Trastuzumab | Letrozole | ORR, PFS, OS, Safety |
| André 2014 [36] | BOLERO-3 | M, DB, R, P3 | 20.2 | 317 | ≥1 | 54.2 | Everolimus+Trastuzumab+Vinorelbine | Placebo+Trastuzumab+Vinorelbine | PFS |
| Endo | 0.65 (0.39, 1.06) | 0.69 (0.45, 1.05) | 0.38 (0.16, 0.88) | 0.45 (0.23, 0.89) |
| 1.55 (0.94, 2.55) | Her2-tki+Endo | 1.06 (0.64, 1.76) | 0.58 (0.25, 1.41) | 0.69 (0.38, 1.28) |
| 1.46 (0.95, 2.24) | 0.94 (0.57, 1.55) | Her2-mAb+Endo | 0.55 (0.27, 1.13) | 0.65 (0.35, 1.21) |
| 2.66 (1.14, 6.14) | 1.71 (0.71, 4.06) | 1.82 (0.88, 3.71) | Her2-mAb+Her2-mAb+Endo | 1.19 (0.46, 3.05) |
| 2.23 (1.13, 4.39) | 1.44 (0.78, 2.63) | 1.53 (0.83, 2.82) | 0.84 (0.33, 2.16) | Her2-mAb+Her2-tki+Endo |
| Her2-mAb+Chem | 0.8 (0.49, 1.31) | 0.95 (0.59, 1.58) | 1.17 (0.91, 1.51) | 0.76 (0.6, 0.96) | 0.48 (0.29, 0.81) | 0.95 (0.35, 2.54) | 0.88 (0.66, 1.19) | 0.95 (0.47, 1.94) | 0.74 (0.51, 1.08) | 0.93 (0.64, 1.35) |
| 1.25 (0.76, 2.04) | Her2-mAb+CDK4/6+Endo | 1.19 (0.78, 1.84) | 1.46 (0.85, 2.57) | 0.94 (0.55, 1.64) | 0.6 (0.29, 1.23) | 1.18 (0.4, 3.52) | 1.1 (0.63, 1.97) | 1.18 (0.5, 2.88) | 0.92 (0.5, 1.73) | 1.16 (0.63, 2.15) |
| 1.05 (0.63, 1.69) | 0.84 (0.54, 1.28) | Her2-mAb+CDK4/6 | 1.22 (0.71, 2.12) | 0.79 (0.46, 1.36) | 0.5 (0.25, 1.02) | 0.99 (0.33, 2.98) | 0.92 (0.52, 1.62) | 0.99 (0.42, 2.39) | 0.77 (0.42, 1.41) | 0.98 (0.53, 1.78) |
| 0.85 (0.66, 1.09) | 0.69 (0.39, 1.18) | 0.82 (0.47, 1.41) | Her2-tki+Chem | 0.65 (0.46, 0.91) | 0.41 (0.23, 0.73) | 0.81 (0.31, 2.07) | 0.75 (0.57, 1) | 0.81 (0.4, 1.65) | 0.63 (0.42, 0.95) | 0.8 (0.51, 1.24) |
| 1.32 (1.04, 1.66) | 1.06 (0.61, 1.81) | 1.26 (0.74, 2.19) | 1.54 (1.1, 2.18) | Her2-mAb+Her2-mAb+Chem | 0.63 (0.36, 1.12) | 1.25 (0.45, 3.47) | 1.16 (0.8, 1.7) | 1.26 (0.59, 2.64) | 0.97 (0.63, 1.51) | 1.23 (0.79, 1.91) |
| 2.08 (1.24, 3.47) | 1.68 (0.81, 3.41) | 1.99 (0.98, 4.08) | 2.44 (1.36, 4.3) | 1.58 (0.89, 2.77) | Her2-mAb+Her2-tki+Chem | 1.96 (0.64, 6.03) | 1.84 (1.01, 3.31) | 1.99 (0.81, 4.75) | 1.54 (0.81, 2.89) | 1.95 (1.03, 3.62) |
| 1.06 (0.39, 2.84) | 0.85 (0.28, 2.52) | 1.01 (0.34, 3.02) | 1.24 (0.48, 3.22) | 0.8 (0.29, 2.21) | 0.51 (0.17, 1.55) | Chem | 0.93 (0.35, 2.53) | 1 (0.31, 3.27) | 0.78 (0.28, 2.19) | 0.99 (0.34, 2.84) |
| 1.13 (0.84, 1.52) | 0.91 (0.51, 1.59) | 1.08 (0.62, 1.91) | 1.33 (1, 1.76) | 0.86 (0.59, 1.25) | 0.54 (0.3, 0.99) | 1.07 (0.4, 2.85) | Her2-ADC | 1.08 (0.56, 2.07) | 0.84 (0.57, 1.22) | 1.06 (0.65, 1.69) |
| 1.05 (0.52, 2.13) | 0.84 (0.35, 1.98) | 1.01 (0.42, 2.38) | 1.23 (0.61, 2.5) | 0.8 (0.38, 1.68) | 0.5 (0.21, 1.23) | 1 (0.31, 3.22) | 0.93 (0.48, 1.77) | Her2-ADC+PD-L1 | 0.78 (0.37, 1.64) | 0.98 (0.44, 2.17) |
| 1.36 (0.93, 1.97) | 1.09 (0.58, 2) | 1.3 (0.71, 2.4) | 1.59 (1.06, 2.39) | 1.03 (0.66, 1.6) | 0.65 (0.35, 1.24) | 1.28 (0.46, 3.6) | 1.19 (0.82, 1.75) | 1.29 (0.61, 2.74) | Her2-mAb+Her2-ADC | 1.26 (0.74, 2.13) |
| 1.07 (0.74, 1.56) | 0.86 (0.47, 1.58) | 1.02 (0.56, 1.9) | 1.25 (0.81, 1.98) | 0.81 (0.52, 1.27) | 0.51 (0.28, 0.97) | 1.01 (0.35, 2.96) | 0.95 (0.59, 1.54) | 1.02 (0.46, 2.29) | 0.79 (0.47, 1.35) | Her2-mAb+Chem+mTOR |
| (A) OS#1 | ||||||
| Endo | 0.69 (0.4, 1.17) | 0.67 (0.4, 1.16) | 0.4 (0.16, 1.04) | |||
| 1.45 (0.86, 2.5) | Her2-tki+Endo | 0.97 (0.56, 1.75) | 0.59 (0.23, 1.55) | |||
| 1.49 (0.86, 2.51) | 1.03 (0.57, 1.78) | Her2-mAb+Endo | 0.6 (0.28, 1.3) | |||
| 2.47 (0.96, 6.21) | 1.7 (0.64, 4.34) | 1.66 (0.77, 3.56) | Her2-mAb+Her2-tki+Endo | |||
| (B) OS#2 | ||||||
| Her2-mAb+Chem | 0.75 (0.41, 1.38) | 0.73 (0.4, 1.34) | 0.71 (0.43, 1.18) | 0.85 (0.49, 1.47) | 1.11 (0.65, 1.92) | |
| 1.33 (0.72, 2.46) | Her2-mAb+CDK4/6+Endo | 0.98 (0.54, 1.78) | 0.95 (0.43, 2.09) | 1.14 (0.5, 2.58) | 1.48 (0.66, 3.38) | |
| 1.36 (0.74, 2.47) | 1.02 (0.56, 1.86) | Her2-mAb+CDK4/6 | 0.97 (0.44, 2.11) | 1.16 (0.52, 2.6) | 1.51 (0.67, 3.39) | |
| 1.4 (0.85, 2.32) | 1.05 (0.48, 2.32) | 1.03 (0.47, 2.25) | Her2-mAb+Her2-mAb+Chem | 1.2 (0.57, 2.51) | 1.56 (0.75, 3.28) | |
| 1.17 (0.68, 2.02) | 0.88 (0.39, 2) | 0.86 (0.38, 1.93) | 0.83 (0.4, 1.76) | Her2-mAb+Her2-tki+Chem | 1.3 (0.6, 2.81) | |
| 0.9 (0.52, 1.55) | 0.68 (0.3, 1.52) | 0.66 (0.29, 1.48) | 0.64 (0.31, 1.33) | 0.77 (0.36, 1.65) | Chem | |
| (A) ORR#1 | ||||
| Endo | 3.26 (1.13, 10.17) | 2.81 (1.08, 8.18) | 7.37 (1.81, 33.72) | |
| 0.31 (0.1, 0.89) | Her2-tki+Endo | 0.86 (0.3, 2.65) | 2.24 (0.64, 8.24) | |
| 0.36 (0.12, 0.92) | 1.17 (0.38, 3.34) | Her2-mAb+Endo | 2.63 (0.71, 9.42) | |
| 0.14 (0.03, 0.55) | 0.45 (0.12, 1.55) | 0.38 (0.11, 1.4) | Her2-mAb+Her2-tki+Endo | |
| (B) ORR#2 | ||||
| Her2-mAb+Chem | 0.7 (0.25, 1.88) | 0.97 (0.36, 2.59) | ||
| 1.44 (0.53, 3.98) | Her2-mAb+CDK4/6+Endo | 1.38 (0.58, 3.41) | ||
| 1.03 (0.39, 2.82) | 0.72 (0.29, 1.72) | Her2-mAb+CDK4/6 | ||
| Indicators | DIC of Inconsistency Model | DIC of Consistency Model |
|---|---|---|
| PFS#1 | 10.865 | 10.213 |
| PFS#2 | 26.618 | 24.799 |
| OS#1 | 7.960 | 7.132 |
| OS#2 | 9.988 | 9.954 |
| ORR#1 | 18.318 | 16.166 |
| ORR#2 | 10.141 | 8.564 |
| Grade 3/4 AEs | 28.848 | 27.587 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, X.-M.; Qian, Y.-K.; Chen, H.-L.; Hu, C.-H.; Chen, B.-W. Efficacy and Safety of Anti-HER2 Targeted Therapy for Metastatic HR-Positive and HER2-Positive Breast Cancer: A Bayesian Network Meta-Analysis. Curr. Oncol. 2023, 30, 8444-8463. https://doi.org/10.3390/curroncol30090615
Wu X-M, Qian Y-K, Chen H-L, Hu C-H, Chen B-W. Efficacy and Safety of Anti-HER2 Targeted Therapy for Metastatic HR-Positive and HER2-Positive Breast Cancer: A Bayesian Network Meta-Analysis. Current Oncology. 2023; 30(9):8444-8463. https://doi.org/10.3390/curroncol30090615
Chicago/Turabian StyleWu, Xian-Meng, Yong-Kang Qian, Hua-Ling Chen, Chen-Hua Hu, and Bing-Wei Chen. 2023. "Efficacy and Safety of Anti-HER2 Targeted Therapy for Metastatic HR-Positive and HER2-Positive Breast Cancer: A Bayesian Network Meta-Analysis" Current Oncology 30, no. 9: 8444-8463. https://doi.org/10.3390/curroncol30090615
APA StyleWu, X.-M., Qian, Y.-K., Chen, H.-L., Hu, C.-H., & Chen, B.-W. (2023). Efficacy and Safety of Anti-HER2 Targeted Therapy for Metastatic HR-Positive and HER2-Positive Breast Cancer: A Bayesian Network Meta-Analysis. Current Oncology, 30(9), 8444-8463. https://doi.org/10.3390/curroncol30090615