Chemotherapy Regimens for Non-Metastatic Conventional Appendicular Osteosarcoma: A Literature Review Based on the Outcomes

 ,
,
Abstract
1. Introduction
2. Materials and Methods
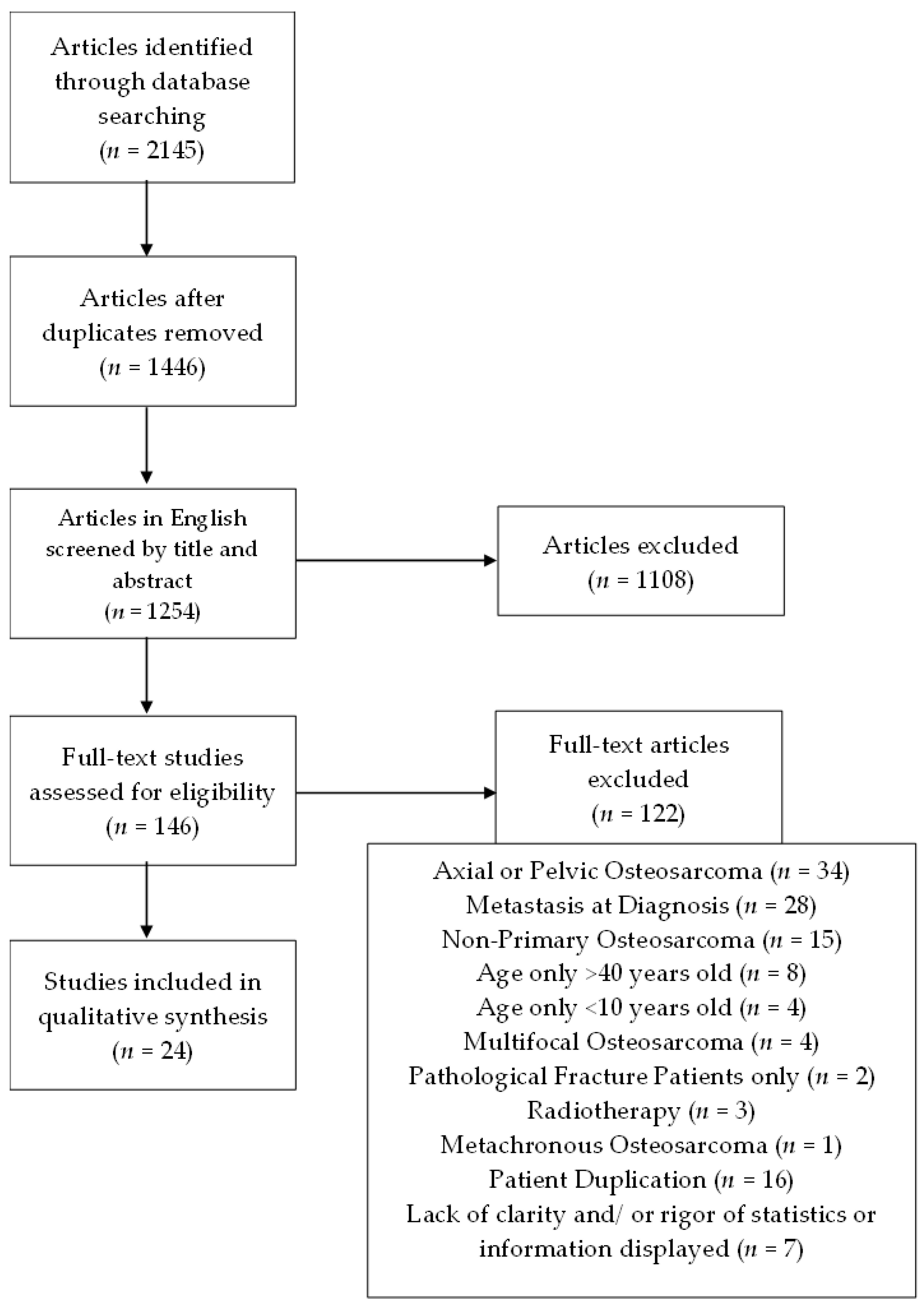
- Population: patients with primary non-metastatic conventional localized appendicular osteosarcoma. Regarding age, in this systematic review we excluded articles referring only to patients >40 years old or <10 years old.
- Intervention: treatment using neoadjuvant chemotherapy, surgery, and consolidation chemotherapy, which we compared to treatment with surgery and adjuvant chemotherapy only.
- Outcomes: (a) primary outcomes: overall survival, disease-free survival, event-free survival; (b) secondary outcomes: toxicity.
- For this type of study, we included prospective and retrospective observational studies, randomized controlled trials, case-controlled studies, and cohort studies.
3. Results
3.1. Selected Studies
3.2. Primary Outcomes
Overall Survival (OS), Disease-Free Survival (DFS)/Event-Free Survival (EFS)
3.3. Secondary Outcomes
Treatment-Related Toxicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Luetke, A.; Meyers, P.A.; Lewis, L.; Juergens, H. Osteosarcoma treatment: Where do we stand? A state-of-the-art review. Cancer Treat. Rev. 2014, 40, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Bielack, S.; Carrle, D.; Casali, P.G. ESMO guidelines working group. Osteosarcoma: ESMO clinical recommendations for diagnosis, treatment, and follow-up. Ann. Oncol. 2009, 20, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Bielack, S.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brennan, B.; et al. Bone sarcomas: ESMO-PaedCan-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv79–iv95. [Google Scholar] [CrossRef] [PubMed]
- Geller, D.S.; Gorlick, R. Osteosarcoma: A review of diagnosis, management, and treatment strategies. Clin. Adv. Hematol. Oncol. 2010, 8, 705–718. [Google Scholar] [PubMed]
- Ritter, J.; Bielack, S.S. Osteosarcoma. Ann. Oncol. 2010, 21, vii320–vii325. [Google Scholar] [CrossRef] [PubMed]
- Grimer, R.J. Surgical options for children with osteosarcoma. Lancet Oncol. 2005, 6, 85–92. [Google Scholar] [CrossRef]
- Eilber, F.; Giuliano, A.; Eckardt, J.; Patterson, K.; Moseley, S.; Goodnight, J. Adjuvant chemotherapy for osteosarcoma: A randomized prospective trial. J. Clin. Oncol. 1987, 5, 21–26. [Google Scholar] [CrossRef]
- Marcove, R.C.; Mike, V.; Hajek, J.V.; Levin, A.G.; Hutter, R.V. Osteogenic sarcoma under the age of twenty-one. A review of one hundred and forty-five operative cases. J. Bone Jt. Surg. 1970, 52, 411–423. [Google Scholar] [CrossRef]
- Link, M.P.; Goorin, A.M.; Miser, A.W.; Green, A.A.; Pratt, C.B.; Belasco, J.B.; Pritchard, J.; Malpas, J.S.; Baker, A.R.; Kirkpatrick, J.A.; et al. The effect of adjuvant chemotherapy on relapse-free survival in patients with osteosarcoma of the extremity. N. Engl. J. Med. 1986, 314, 1600–1606. [Google Scholar] [CrossRef]
- Goorin, A.M.; Schwartzentruber, D.J.; Devidas, M.; Gebhardt, M.C.; Ayala, A.G.; Harris, M.B.; Helman, L.J.; Grier, H.E.; Link, M.P. Presurgical chemotherapy compared with immediate surgery and adjuvant chemotherapy for nonmetastatic osteosarcoma: Pediatric Oncology Group Study POG-8651. J. Clin. Oncol. 2003, 21, 1574–1580. [Google Scholar] [CrossRef]
- Zhao, X.; Wu, Q.; Gong, X.; Liu, J.; Ma, Y. Osteosarcoma: A review of current and future therapeutic approaches. Biomed. Eng. Online 2021, 20, 24. [Google Scholar] [CrossRef] [PubMed]
- Isakoff, M.S.; Bielack, S.S.; Meltzer, P.; Gorlick, R. Osteosarcoma: Current treatment and a collaborative pathway to success. J. Clin. Oncol. 2015, 33, 3029. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, L.J.; Douglass, H.O.; Mindell, E.R.; Sinks, L.F.; Tebbi, C.K.; Risseeuw, D.; Freeman, A.I. Adjuvant adriamycin 547 and cisplatin in newly diagnosed, nonmetastatic osteosarcoma of the extremity. J. Clin. Oncol. 1986, 4, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Glasser, D.B.; Lane, J.M.; Huvos, A.G.; Marcove, R.C.; Rosen, G. Survival, prognosis, and therapeutic response in osteogenic sarcoma. The Memorial Hospital Experience. Cancer 1992, 69, 698–708. [Google Scholar] [CrossRef]
- Smeland, S.; Müller, C.; Alvegard, T.A.; Wiklund, T.; Wiebe, T.; Björk, O.; Stenwig, A.E.; Willén, H.; Holmström, T.; Follerås, G.; et al. Scandinavian Sarcoma Group Osteosarcoma Study SSG VIII: Prognostic factors for outcome and the role of replacement salvage chemotherapy for poor histological responders. Eur. J. Cancer 2003, 39, 488–494. [Google Scholar] [CrossRef]
- Zalupski, M.M.; Rankin, C.; Ryan, J.R.; Lucas, D.R.; Muler, J.; Lanier, K.S.; Budd, G.T.; Biermann, J.S.; Meyers, F.J.; Antman, K. Adjuvant therapy of osteosarcoma—A phase II trial Southwest Oncology Group Study 9139. Cancer 2004, 100, 818–825. [Google Scholar] [CrossRef]
- Ford, S.; Saithna, A.; Grimer, R.J.; Picci, P. Comparison of the outocome of conventional osteosarcoma at two specialist international orthopaedic oncology centres. Sarcoma 2004, 8, 13–18. [Google Scholar] [CrossRef]
- Wilkins, R.M.; Cullen, J.W.; Camozzi, A.B.; Jamroz, B.A.; Odom, L. Improved survival in primary nonmetastatic pediatric osteosarcoma of the extremity. Clin. Orthop. Relat. Res. 2005, 438, 128–136. [Google Scholar] [CrossRef]
- Bacci, G.; Longhi, A.; Fagioli, F. Adjuvant and neoadjuvant chemotherapy for osteosarcoma of the extremities: 27-year experience at Rizzoli Institute. Italy Eur. J. Cancer 2005, 41, 2836–2845. [Google Scholar] [CrossRef]
- Ferrari, S.; Smeland, S.; Mercuri, M.; Bertoni, F.; Longhi, A. Neoadjuvant chemotherapy with high-dose ifosfamide, high-dose methotrexate, cisplatin, and doxorubicin for patients with localized osteosarcoma of the extremity: A joint study by the Italian and Scandinavian Sarcoma Groups. J. Clin. Oncol. 2005, 23, 8845–8852. [Google Scholar] [CrossRef]
- Petrilli, A.S.; de Camargo, B.; Filho, V.O.; Bruniera, P.; Brunetto, A.L.; Jesus-Garcia, R.; Camargo, O.; Pena, W.; Péricles, P.; Davi, A.; et al. Results of the Brazilian osteosarcoma treatment group studies III and IV: Prognostic factors and impact on survival. J. Clin. Oncol. 2006, 24, 1161–1168. [Google Scholar] [CrossRef] [PubMed]
- Basaran, M.; Bavbek, E.S.; Saglam, S.; Eralp, L.; Sakar, B.; Atalar, A.C.; Bilgic, B.; Ozger, H.; Onat, H. A Phase II study of 581 cisplatin, ifosfamide and epirubicin combination chemotherapy in adults with nonmetastatic and extremity osteosarcomas. Oncology 2007, 72, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Lewis, I.J.; Nooij, M.A.; Whelan, J.; Sydes, M.R.; Grimer, R.; Hogendoorn, P.C.; Memon, M.A.; Weeden, S.; Uscinska, B.M.; Van Glabbeke, M.; et al. Improvement in histologic response but not survival in osteosarcoma patients treated with intensified chemotherapy: A randomized phase III trial of the European Osteosarcoma Intergroup. J. Natl. Cancer Inst. 2007, 99, 112–128. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, Y.; Tanaka, K.; Isu, K.; Kawai, A.; Tatezaki, S.-I.; Ishii, T.; Kushida, K.; Beppu, Y.; Usui, M.; Tateishi, A.; et al. Multiinstitutional phase II study of neoadjuvant chemotherapy for osteosarcoma (NECO study) in Japan: NECO-93J and NECO-95J. J. Ortho. Sci. 2009, 14, 397–404. [Google Scholar] [CrossRef]
- Bielack, S.; Jürgens, H.; Jundt, G.; Kevric, M.; Kühne, T.; Reichardt, P.; Zoubek, A.; Werner, M.; Winkelmann, W.; Kotz, R. Osteosarcoma: The COSS experience. Cancer Treat. Res. 2009, 152, 289–308. [Google Scholar] [CrossRef]
- Hong, S.; Shin, S.J.; Jung, M.; Jeong, J.; Lee, Y.J.; Shin, K.-H.; Roh, J.K.; Rha, S.Y. Comparison of long-term outcome between doublet and triplet neoadjuvant chemotherapy in nonmetastatic osteosarcoma of the extremity. Oncology 2011, 80, 107–117. [Google Scholar] [CrossRef]
- Smeland, S.; Bruland, Ø.S.; Hjorth, L.; Brosjö, O.; Bjerkehagen, B.; Österlundh, G.; Jakobson, Å.; Hall, K.S.; Monge, O.R.; Björk, O.; et al. Results of the Scandinavian sarcoma group XIV protocol for classical osteosarcoma: 63 patients with a minimum follow-up of 4 years. Acta Orthop. 2011, 82, 211–216. [Google Scholar] [CrossRef]
- Li, D.; Cui, Q.; Liu, Y.; Wang, X.; Liu, C.; Liu, S.; Zeng, Y. Chemotherapy response analysis for osteosarcoma with intra-arterial chemotherapy by subcutaneous implantable delivery system. Pathol. Oncol. Res. 2011, 17, 947–953. [Google Scholar] [CrossRef]
- Whelan, J.S.; Jinks, R.C.; McTiernan, A.; Sydes, M.R.; Hook, J.M.; Trani, L.; Uscinska, B.; Bramwell, V.; Lewis, I.J.; Nooij, M.A.; et al. Survival from high-grade localized extremity osteosarcoma: Combined results and prognostic factors from three European Osteosarcoma Intergroup randomised controlled trials. Ann. Oncol. 2012, 23, 1607–1616. [Google Scholar] [CrossRef]
- Kudawara, I.; Aoki, Y.; Ueda, T.; Araki, N.; Naka, N.; Nakanishi, H.; Matsumine, A.; Ieguchi, M.; Mori, S.; Myoui, A.; et al. Neoadjuvant and adjuvant chemotherapy with high-dose ifosfamide, doxorubicin, cisplatin and high-dose methotrexate in non-metastatic osteosarcoma of the extremities: A phase II trial in Japan. J. Chemother. 2013, 25, 41–48. [Google Scholar] [CrossRef]
- Xu, M.; Xu, S.F.; Yu, X.C. Clinical analysis of osteosarcoma patients treated with high dose methotrexate-free neoadjuvant chemotherapy. Curr. Oncol. 2014, 21, e678–e684. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.; Meazza, C.; Palmerini, E. Nonmetastatic osteosarcoma of the Extremity. Neoadjuvant chemotherapy with methotrexate, cisplatin, doxorubicin and ifosfamide. An Italian Sarcoma Group study (ISG/OS-Oss). Tumori J. 2014, 100, 612–619. [Google Scholar] [CrossRef]
- Bajpai, J.; Chandrasekharan, A.; Talreja, V. Outcomes in non-metastatic extremity osteosarcoma treatment naïve patients, treated with a novel non-high-dose methotrexate-based, dose-dense combination chemotherapy regimen “OGS-12”. Eur. J. Cancer 2017, 85, 49–58. [Google Scholar] [CrossRef]
- Huang, J.; Bi, W.; Han, G.; Jia, J.; Xu, M.; Wang, W. The multidisciplinary treatment of osteosarcoma of the proximal tibia: A retrospective study. BMC Musculoskelet. Disord. 2018, 19, 315. [Google Scholar] [CrossRef] [PubMed]
- Morsy, A.M.; Ahmed, B.M.; Rezk, K.M.; Ramadan, I.K.-A.; Aboelgheit, A.M.; Eltyb, H.A.; Elbadee, O.M.A.; El-Naggar, M.S. Age and tumor location predict survival in nonmetastatic osteosarcoma in Upper Egypt. J. Pediatr. Hematol. Oncol. 2020, 42, e66–e78. [Google Scholar] [CrossRef]
- Whelan, J.S.; Bielack, S.S.; Marina, N.; Smeland, S.; Jovic, G.; Hook, J.M.; Krailo, M.; Anninga, J.; Butterfass-Bahloul, T.; Böhling, T.; et al. EURAMOS-1, an international randomized study for osteosarcoma: Results from pre-randomization treatment. Ann. Oncol. 2015, 26, 407. [Google Scholar] [CrossRef]
- Fuchs, B.; Pritchard, D.J. Etiology of osteosarcoma. Clin. Orthop. Relat. Res. 2002, 397, 40–52. [Google Scholar] [CrossRef]
- Gianferante, D.M.; Mirabello, L.; Savage, S.A. Germline and somatic genetics of osteosarcoma—Connecting aetiology, biology and therapy. Nat. Rev. Endocrinol. 2017, 13, 480–491. [Google Scholar] [CrossRef]
- Antonescu, C.R.; Blay, J.Y.; Bovee, J.V.M.G.; Bridge, J.A.; Cunha, I.W.; Dei Tos, A.P.; Flanagan, A.M.; Fletcher, C.D.M.; Folpe, A.M.; Hornick, J.L.; et al. World Health Organization Classification of Tumours of Soft Tissue and Bone, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2020. [Google Scholar]
- Mirabello, L.; Troisi, R.J.; Savage, S.A. Osteosarcoma incidence and survival rates from 1973 to 2004: Data from the Surveillance, Epidemiology, and End Results Program. Cancer 2009, 115, 1531–1543. [Google Scholar] [CrossRef]
- Grimer, R.J.; Briggs, T.W. Earlier diagnosis of bone and soft-tissue tumors. J. Bone Jt. Surg. Br. 2010, 92, 1489–1492. [Google Scholar] [CrossRef]
- Rosen, G.; Caparros, B.; Huvos, A.G.; Kosloff, C.; Nirenberg, A.; Cacavio, A.; Marcove, R.C.; Lane, J.M.; Mehta, B.; Urban, C. Preoperative chemotherapy for osteogenic sarcoma: Selection of postoperative adjuvant chemotherapy based on the response of the primary tumor to preoperative chemotherapy. Cancer 1982, 49, 1221–1230. [Google Scholar] [CrossRef] [PubMed]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international, randomized controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef] [PubMed]
- Brookes, M.J.; Chan, C.D.; Baljer, B.; Wimalagunaratna, S.; Crowley, T.P.; Ragbir, M.; Irwin, A.; Gamie, Z.; Beckingsale, T.; Ghosh, K.M.; et al. Surgical Advances in Osteosarcoma. Cancers 2021, 13, 388. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Therapeutic Modality | Therapeutic Relevance * | Comments |
|---|---|---|
| Chemotherapy | ++++ | Relevant toxic and side effects (cardiotoxicity, liver and kidney toxicity, bone marrow suppression, neurotoxicity.) Cancer resistance to chemotherapeutics. |
| Surgery | ++++ | Only allows for local control of the disease. |
| Radiotherapy | ++ | Some impact in unresectable osteosarcomas, in those osteosarcomas where tumor remains on the resection margin and for patients with poor response to chemotherapy. |
| Immunotherapy | ++ | Osteosarcoma cells have low immunogenicity and, hence, therapeutic response is limited. |
| Embolization | +++ | Relevant only for pain control; cannot control local or systemic disease. |
| Author | Year | Type of Study | No. of Patients | Age Median Years (Range) | Average Follow-Up (Months) | Most Common Tumor Location | Treatment | OS | DFS/EFS | TR Toxicity (Major Events) |
|---|---|---|---|---|---|---|---|---|---|---|
| Ettinger et al. [13] | 1986 | Prospective | 22 | 17 (6–46) | 70 | DF (n = 12) PT (n = 6) | ACT (n = 22) | 72 m: 77% | 72 m: 64% | Deaths (n = 0) |
| Glasser et al. [14] | 1991 | Retrospective | 279 | Male: 17 (5–63) Female: 15 (3–58) | 92 | DF (n = 131) PH (n = 52) PT (n = 52) PF (n = 14) | NAC (n = 240) | 5 y: 78% * 10 y: 74% * | 5 y: 70% 10 y: 69% | NR |
| ACT (n = 39) | 5 y: 77% * 10 y: 77% * | |||||||||
| Smeland et al. [15] | 2003 | Retrospective | 113 | <15 (n = 34) >15 (n = 79) | 83 | Femur (n = 60) Tibia (n = 31) Humerus (n = 15) | NAC (n = 113) | 5 y: 74% | 5 y: 61% | Deaths (n = 3) ETC (n = 13) |
| Goorin et al. [10] | 2003 | Prospective | 100 | <12 (n = 19) >12 (n = 26) | - | Femur (n = 26) Tibia (n = 11) | NAC (n = 45) | 5 y: 76% | 5 y: 61% | Deaths (n = 3) [CHF (n = 2) BO (n = 1)] SHL (n = 1) |
| <12 (n = 23) >12 (n = 32) | Femur (n = 35) Tibia (n = 13) | ACT (n = 55) | 5 y: 79% | 5 y: 69% | ||||||
| Zalupski et al. [16] | 2004 | Prospective | 63 | 22 (12–70) | 79 | Femur (n = 32) Tibia (n = 16) | NAC (n = 63) | 5 y: 58% | NR | Death (n = 1) [SML (n = 1)] ETC (n = 11) |
| Ford et al. [17] | 2004 | Retrospective | 428 | 15.8 | - | Femur (n = 271) Tibia (n = 157) | NAC (n = 428) | - | - | NR |
| Center 1 (n = 265) | 15.2 | Femur (n = 171) Tibia (n = 94) | 5 y: 73% | 5 y: 56% | ||||||
| Center 2 (n = 163) | 16.1 | Femur (n = 100) Tibia (n = 63) | 5 y: 60% | 5 y: 43% | ||||||
| Wilkins et al. [18] | 2005 | Prospective | 62 | 14 (5–21) | 91 | Femur (n = 40) Tibia (n = 14) | NAC (n = 62) | 5 y: 96.6% 10 y: 93.2% | 5 y: 86.4% 10 y: 86.4% | Deaths (n = 0) G3-Ct (n = 1) G3-OT (n = 1) |
| Bacci et al. [19] | 2005 | Retrospective | 1148 | 16.7 (3–40) | 177.6 | Femur (n = 612) Tibia (n = 327) Humerus (n = 128) | NAC (n = 900) | 5 y: 66% (1148) 10 y: 57% (1148) | 5 y: 61% | Death from Toxicity (n = 12) |
| ACT (n = 248) | 5 y: 43% | Death from Toxicity (n = 6) | ||||||||
| Ferrari et al. [20] | 2005 | Prospective | 182 | 16 (4–40) | 55 | Femur (n = 93) Tibia (n = 48) Humerus (n = 30) | NAC (n = 182) | 5 y: 77% | 5 y: 64% | Death from Toxicity (n = 3) |
| Petrilli et al. [21] | 2006 | Prospective | Included in This Review: 168 out of 209 | ≤14 (n = 90) >14 (n = 88) | 61 | Femur (n = 96) Tibia (n = 58) | NAC (n = 168) | 5 y: 60.5% 10 y: 55.2% | 5 y: 45.5% 10 y: 45.5% | Deaths from Toxicity (n = 15 out of 209) |
| Basaran et al. [22] | 2007 | Prospective | 38 | 22 (15–41) | 64 | Tibia (n = 16) Femur (n = 14) Humerus (n = 6) | NAC (n = 38) | 5 y: 48.2% | 5 y: 41.9% | Severe HT (n = 12) Severe Nausea (n = 2) Severe Vomiting (n= 2) Severe FN (n = 9) |
| Lewis et al. [23] | 2007 | Prospective | 497 | 15 (12–18) | 62 | Femur (n = 296) Tibia (n = 116) | NAC (n = 497) | - | - | G3/G4 Toxicity (n = 468) |
| Reg. C (n = 245) | 5 y: 55% | 5 y: 39% | Excessive Toxicity (n = 12) | |||||||
| Reg. DI (n = 252) | 5 y: 58% | 5 y: 41% | Excessive Toxicity (n = 17) | |||||||
| Iwamoto et al. [24] | 2009 | Prospective | 113 | 15 (6–27) | 75.6 | Femur (n = 62) Tibia (n = 33) | NAC (n = 113) | 5 y: 77.9% | 5 y: 65.5% | Deaths from Toxicity (n = 6) |
| Bielack et al. [25] | 2009 | Retrospective | Included in This Review: 2017 out of 2464 | 15.4 | 67.92 | (Out of 2464) Femur (n = 1229) Tibia (n = 636) | NAC (n = 2017) | 5 y: 74.8% 10 y: 69.5% | NR | (Out of 2464) Deaths from Toxicity during Primary Treatment (n = 29) Secondary Malignancy (n = 12) Cardiomyopathy (n = 7) |
| Hong et al. [26] | 2011 | Retrospective | 124 | <15 (n = 36) 15–40 (n = 82) >40 (n = 6) | 68.4 | DF (n = 68) PT (n = 24) PH (n = 16) | AP NAC (n = 77) IAP NAC (n = 47) | 5 y: 85% 5 y: 63.9% | 5 y: 78.7% 5 y: 63.6% | Deaths from Toxicity: (n = 5) [during Adjuvant Chemotherapy] |
| 46.8 | ||||||||||
| Smeland et al. [27] | 2011 | Prospective | 63 | 15 (8–39) | 77 | Femur (n = 34) Tibia (n = 15) | NAC (n = 63) | 5 y: 76% | 5 y: 65% | Deaths from Toxicity (n = 3) NE (n = 1) G4 Ct (n = 1) |
| Li et al. [28] | 2011 | Retrospective | 111 | 18 (14–39) | 28 | DF (n = 49) PT (n = 32) | NAC (n = 111) | 3 y: 68.3% | 3 y: 65.9% | Deaths from Toxicity (n = 0) |
| ST NAC (n = 87) | 3 y: 80.0% | 3 y: 79.5% | ||||||||
| NST NAC (n = 24) | 3 y: 38.9% | 3 y: 30.1% | ||||||||
| Whelan et al. [29] | 2012 | Retrospective | 1067 | 15 (3–40) | 112.8 | Femur (n = 611) Tibia (n = 264) | NAC (n = 1067) | 5 y: 56% 10 y: 52% | 5 y: 43% 10 y: 42% | NR |
| Kudawara et al. [30] | 2013 | Retrospective | 40 | 0–15 (n = 17) 16–20 (n = 16) 21–30 (n = 2) >30 (n = 5) | 117 | Femur (n = 20) Tibia (n = 13) | NAC (n = 40) | 5 y: 98% 10 y: 95% | 5 y: 83% 10 y: 80% | Deaths from Toxicity (n = 0) G4 Lp (52% of cycles) G4NphT (n = 1) |
| Xu et al. [31] | 2014 | Retrospective | 39 | 16 (6–39) | 66 | DF (n = 21) PT (n = 13) | NAC (n = 39) | 5 y: 61.5% | 5 y: 54.8% | Deaths from Toxicity (n = 0) |
| Ferrari et al. [32] | 2014 | Retrospective | 171 | 16 (3–40) | 39 | Femur (n = 92) Tibia (n = 56) | NAC (n = 171) | 5 y: 81% | 5 y: 50% | G4Lp (n = 171) G4Thr (n = 58) |
| Bajpai et al. [33] | 2017 | Retrospective | Included in This Review: 209 out of 237 | (209) 17 (6–56) | (209) 35.6 | (237) Femur (n = 109) Tibia (n = 83) | NAC (n = 209) | 3 y: 82% 5 y: 80% | 3 y: 63% 5 y: 60% | Deaths from Toxicity (n = 2) |
| Huang et al. [34] | 2018 | Retrospective | 69 | 20 (12–57) | 75.9 | Proximal Tibia Only | NAC (n = 69) | 3 y: 91.3% 5 y: 87% | - | NR |
| Morsy et al. [35] | 2019 | Retrospective | 30 | 5–9 (n = 5) 10–14 (n = 13) 15–18 (n = 12) | 63 | DF (n = 15) PT (n = 6) | NAC (n = 30) | 3 y: 79% 5 y: 65.3% | 3 y: 69.5% 5 y: 65.2% | NR |
| Total Number of Patients Involved | 5-Year Overall-Survival Range | 5-Year Disease-Free Survival/ Event-Free Survival Range | Treatment-Related Toxicity | ||||
|---|---|---|---|---|---|---|---|
| NAC | ACT | NAC | ACT | NAC | ACT | NAC | ACT |
| 6789 | 364 | 55–80% | 77–79% | 39–65.5% | 43–69% | Early Termination/Modification of Chemotherapy: 125 patients (≈1.84%) Reported Deaths Directly Attributed to Chemotherapy: 25 (≈0.37%) | Reported Deaths Directly Attributed to Chemotherapy: 7 (≈1.92%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares do Brito, J.; Santos, R.; Sarmento, M.; Fernandes, P.; Portela, J. Chemotherapy Regimens for Non-Metastatic Conventional Appendicular Osteosarcoma: A Literature Review Based on the Outcomes. Curr. Oncol. 2023, 30, 6148-6165. https://doi.org/10.3390/curroncol30070457
Soares do Brito J, Santos R, Sarmento M, Fernandes P, Portela J. Chemotherapy Regimens for Non-Metastatic Conventional Appendicular Osteosarcoma: A Literature Review Based on the Outcomes. Current Oncology. 2023; 30(7):6148-6165. https://doi.org/10.3390/curroncol30070457
Chicago/Turabian StyleSoares do Brito, Joaquim, Rodrigo Santos, Marco Sarmento, Pedro Fernandes, and José Portela. 2023. "Chemotherapy Regimens for Non-Metastatic Conventional Appendicular Osteosarcoma: A Literature Review Based on the Outcomes" Current Oncology 30, no. 7: 6148-6165. https://doi.org/10.3390/curroncol30070457
APA StyleSoares do Brito, J., Santos, R., Sarmento, M., Fernandes, P., & Portela, J. (2023). Chemotherapy Regimens for Non-Metastatic Conventional Appendicular Osteosarcoma: A Literature Review Based on the Outcomes. Current Oncology, 30(7), 6148-6165. https://doi.org/10.3390/curroncol30070457