Impact of the COVID-19 Lockdown on Physical Activity Levels and Health Parameters in Young Adults with Cancer

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample
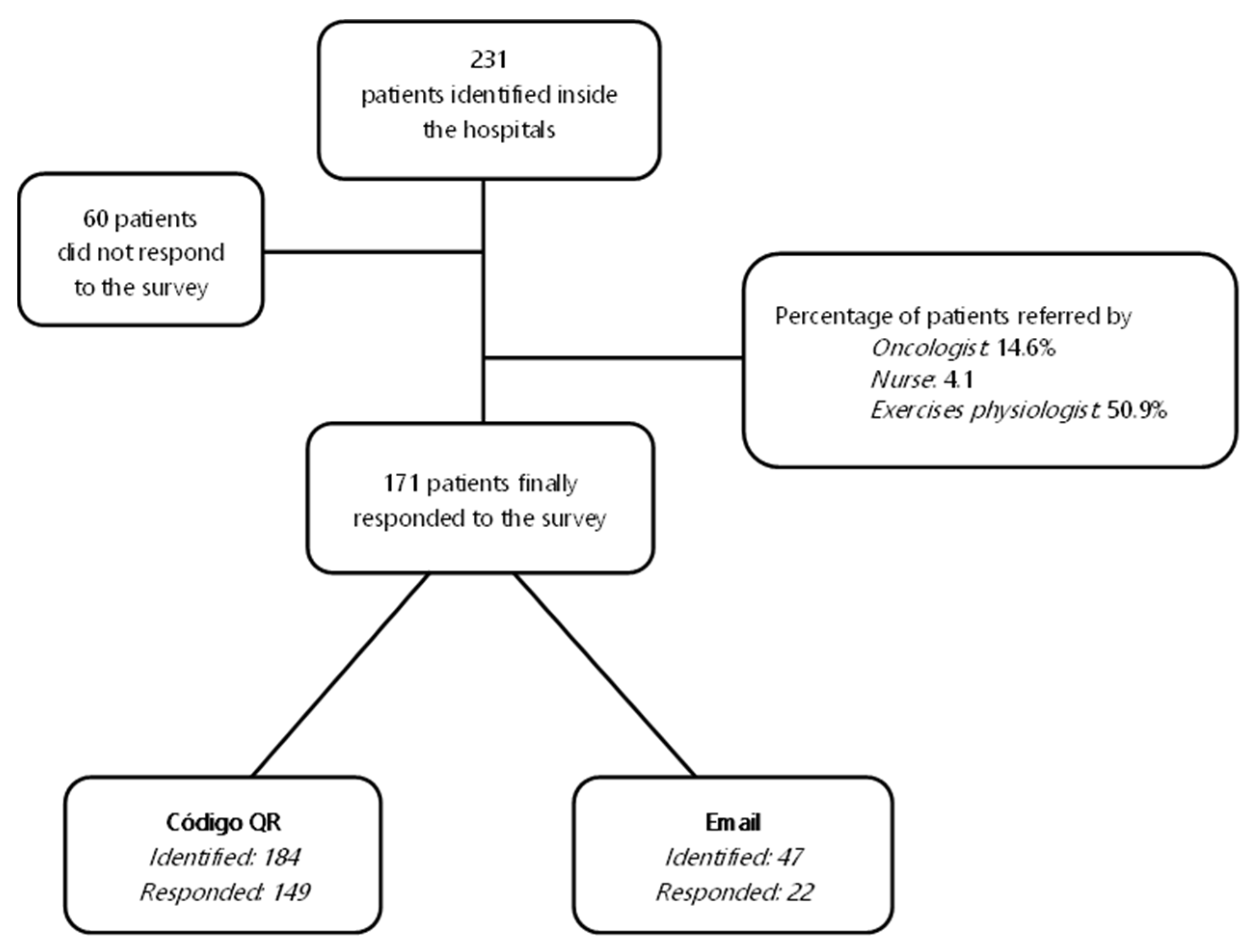
2.3. Recruitment
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Physical Activity Levels
3.3. Secondary Objectives Results
3.3.1. Anthropometrics Measure
3.3.2. HQoL
3.3.3. Fatigue
3.3.4. Sedentary Behaviours
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ECIS. Estimated of Cancer Incidence and Mortality in 2020, for All Cancer Sites. System, European Cancer Information. Available online: https://ecis.jrc.ec.europa.eu/explorer.php?$0-0$1-ES$2-All$4-1,2$3-All$6-20,44$5-2020,2020$7-7$CEstByCancer$X0_8-3$CEstRelativeCanc$X1_8-3$X1_9-AE27$CEstBySexByCancer$X2_8-3$X2_-1-1 (accessed on 30 November 2022).
- GBD 2019 Adolescent Young Adult Cancer Collaborators. The Global Burden of Adolescent and Young Adult Cancer in 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Oncol. 2022, 23, 27–52. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.; Anderson, C.; Lippman, S.M. Physical Activity, Sedentary Behaviour, Diet, and Cancer: An Update and Emerging New Evidence. Lancet Oncol. 2017, 18, e457–e471. [Google Scholar] [CrossRef]
- Silva, D.A.S.; Tremblay, M.S.; Marinho de Souza, M.D.F.; Guerra, M.R.; Mooney, M.; Naghavi, M.; Malta, D.C. Mortality and Years of Life Lost Due to Breast Cancer Attributable to Physical Inactivity in the Brazilian Female Population (1990–2015). Sci. Rep. 2018, 8, 11141. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.A.S.; Tremblay, M.S.; Marinho de Souza, M.d.F.; Mooney, M.; Naghavi, M.; Malta, D.C. Mortality and Years of Life Lost by Colorectal Cancer Attributable to Physical Inactivity in Brazil (1990–2015): Findings from the Global Burden of Disease Study. PLoS ONE 2018, 13, e0190943. [Google Scholar] [CrossRef] [PubMed]
- Tricoli, J.V.; Blair, D.G.; Anders, C.K.; Bleyer, W.A.; Boardman, L.A.; Khan, J.; Kummar, S.; Hayes-Lattin, B.; Hunger, S.P.; Merchant, M.; et al. Biologic and Clinical Characteristics of Adolescent and Young Adult Cancers: Acute Lymphoblastic Leukemia, Colorectal Cancer, Breast Cancer, Melanoma, and Sarcoma. Cancer 2016, 122, 1017–1028. [Google Scholar] [CrossRef] [PubMed]
- Murphy, B.L.; Day, C.N.; Hoskin, T.L.; Habermann, E.B.; Boughey, J.C. Adolescents and Young Adults with Breast Cancer Have More Aggressive Disease and Treatment Than Patients in Their Forties. Ann. Surg. Oncol. 2019, 26, 3920–3930. [Google Scholar] [CrossRef]
- Chao, C.; Xu, L.; Bhatia, S.; Cooper, R.; Brar, S.; Wong, F.L.; Armenian, S.H. Cardiovascular Disease Risk Profiles in Survivors of Adolescent and Young Adult (AYA) Cancer: The Kaiser Permanente AYA Cancer Survivors Study. J. Clin. Oncol. 2016, 34, 1626–1633. [Google Scholar] [CrossRef]
- Nowe, E.; Stöbel-Richter, Y.; Sender, A.; Leuteritz, K.; Friedrich, M.; Geue, K. Cancer-Related Fatigue in Adolescents and Young Adults: A Systematic Review of the Literature. Crit. Rev. Oncol. Hematol. 2017, 118, 63–69. [Google Scholar] [CrossRef]
- Nowe, E.; Friedrich, M.; Leuteritz, K.; Sender, A.; Stöbel-Richter, Y.; Schulte, T.; Hinz, A.; Geue, K. Cancer-Related Fatigue and Associated Factors in Young Adult Cancer Patients. J. Adolesc. Young Adult Oncol. 2019, 8, 297–303. [Google Scholar] [CrossRef]
- Marec-Bérard, P.; Delrieu, L.; Febvey-Combes, O.; Mongondry, R.; Pérol, O.; Moumjid-Ferdjaoui, N.; Boyle, H.; Fervers, B.; Carretier, J. Implementation of a Prevention Program Based on Adapted Physical Activity and Recommendations for Adolescents and Young Adults with Cancer: PREVAPAJA Study. J. Adolesc. Young Adult Oncol. 2022, 11, 189–201. [Google Scholar] [CrossRef]
- Moraitis, A.M.; Seven, M.; Sirard, J.; Walker, R. Expert Consensus on Physical Activity Use for Young Adult Cancer Survivors’ Biopsychosocial Health: A Modified Delphi Study. J. Adolesc. Young Adult Oncol. 2022, 11, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Adame, H.; Wettersten, K.; Schwinghamer, A.; Friesen-Janochoski, A. Cancer-Related Fatigue as a Mediator between Self-Efficacy and Quality of Life for Adolescents and Young Adults Impacted by Cancer. J. Psychosoc. Oncol. 2022, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.M.; Zabor, E.C.; Schwitzer, E.; Koelwyn, G.J.; Adams, S.C.; Nilsen, T.S.; Moskowitz, C.S.; Matsoukas, K.; Iyengar, N.M.; Dang, C.T.; et al. Efficacy of Exercise Therapy on Cardiorespiratory Fitness in Patients with Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2018, 36, 2297–2305. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.M.; Nilsen, T.S.; Gupta, D.; Jones, L.W. Exercise Therapy and Cardiovascular Toxicity in Cancer. Circulation 2018, 137, 1176–1191. [Google Scholar] [CrossRef]
- Armenian, S.H. Anthracycline-Induced Cardiotoxicity in Young Cancer Patients: The Role of Carnitine. Ann. Nutr. Metab. 2016, 68 (Suppl. 3), 10–14. [Google Scholar] [CrossRef]
- Ding, D.; Van Buskirk, J.; Nguyen, B.; Stamatakis, E.; Elbarbary, M.; Veronese, N.; Clare, P.J.; Lee, I.-M.; Ekelund, U.; Fontana, L. Physical Activity, Diet Quality and All-Cause Cardiovascular Disease and Cancer Mortality: A Prospective Study of 346,627 UK Biobank Participants. Br. J. Sports Med. 2022, 56, 20. [Google Scholar] [CrossRef]
- Murnane, A.; Gough, K.; Thompson, K.; Holland, L.; Conyers, R. Adolescents and Young Adult Cancer Survivors: Exercise Habits, Quality of Life and Physical Activity Preferences. Support. Care Cancer 2015, 23, 501–510. [Google Scholar] [CrossRef]
- Adams, S.C.; Petrella, A.; Sabiston, C.M.; Vani, M.F.; Gupta, A.; Trinh, L.; Matthew, A.G.; Hamilton, R.J.; Mina, D.S. Preferences for Exercise and Physical Activity Support in Adolescent and Young Adult Cancer Survivors: A Cross-Sectional Survey. Support. Care Cancer 2021, 29, 4113–4127. [Google Scholar] [CrossRef]
- Martínez-de-Quel, Ó.; Suárez-Iglesias, D.; López-Flores, M.; Pérez, C.A. Physical Activity, Dietary Habits and Sleep Quality before and during COVID-19 Lockdown: A Longitudinal Study. Appetite 2021, 158, 105019. [Google Scholar] [CrossRef]
- Ross, R.; Blair, S.N.; Arena, R.; Church, T.S.; Després, J.-P.; Franklin, B.A.; Haskell, W.L.; Kaminsky, L.A.; Levine, B.D.; Lavie, C.J.; et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement from the American Heart Association. Circulation 2016, 134, e653–e699. [Google Scholar] [CrossRef]
- Yan, A.; Howden, K.; Mahar, A.L.; Scott, I.; Glidden, C.; Deleemans, J.; Chalifour, K.; Eaton, G.; Gupta, A.; Bolton, J.M.; et al. Experiences of Adolescent and Young Adult Cancer Survivors during the COVID-19 Pandemic. J. Cancer Surviv. 2022, 17, 370–383. [Google Scholar] [CrossRef] [PubMed]
- Tabaczynski, A.; Bastas, D.; Whitehorn, A.; Trinh, L. Changes in Physical Activity and Associations with Quality of Life among a Global Sample of Cancer Survivors during the COVID-19 Pandemic. J. Cancer Surviv. 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Castellanos-Montealegre, M.; García-Coll, V.; Hernández, S.; Collado, R.; Gil-Herrero, L.; Casla-Barrio, S. Exercise Intervention Features to Improve Physical Activity Levels in Young Adults with a Cancer Diagnosis: A Systematic Review. Clin. Oncol. 2022, 7, 1957. [Google Scholar]
- Wu, Q.; Vogtmann, E.; Zhang, W.; Xie, L.; Yang, W.S.; Tan, Y.T.; Gao, J.; Xiang, Y.B. Cancer incidence among adolescents and young adults urban Shanghai, 1973–2005. PLoS ONE 2012, 7, e42607. [Google Scholar] [CrossRef] [PubMed]
- Rajani, S.; Young, A.J.; McGoldrick, D.A.; Pearce, D.L.; Sharaf, S.M. The International Charter of Rights for Young with Cancer. J. Adolesc. Young Adults Oncol. 2011, 1, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Wolin, K.Y.; Heil, D.P.; Askew, S.; Matthews, C.E.; Bennett, G.G. Validation of the International Physical Activity Questionnaire-Short among Blacks. J. Phys. Act. Health 2008, 5, 746–760. [Google Scholar] [CrossRef] [PubMed]
- Balestroni, G.; Bertolotti, G. EuroQol-5D (EQ-5D): An instrument for measuring quality of life. Monaldi Arch. Chest Dis. 2012, 78, 155–159. [Google Scholar] [CrossRef] [PubMed]
- King, M.T.; Cella, D.; Osoba, D.; Stockler, M.; Eton, D.; Thompson, J.; Eisenstein, A. Meta-Analysis Provides Evidence-Based Interpretation Guidelines for the Clinical Significance of Mean Differences for the FACT-G, a Cancer-Specific Quality of Life Questionnaire. Patient Relat. Outcome Meas. 2010, 1, 119–126. [Google Scholar] [CrossRef]
- Gutiérrez-Santamaría, B.; Castañeda-Babarro, A.; Arietaleanizbeaskoa, M.S.; Mendizabal-Gallastegui, N.; Grandes, G.; Coca, A. Physiological and Mental Health Changes in Cancer Patients during the COVID-19 State of Emergency. Sport Sci. Health 2022, 19, 123–130. [Google Scholar] [CrossRef]
- Pérez-Rodrigo, C.; Gianzo Citores, M.; Hervás Bárbara, G.; Ruiz-Litago, F.; Casis Sáenz, L.; Arija, V.; López-Sobaler, A.M.; Martínez de Victoria, E.; Ortega, R.M.; Partearroyo, T.; et al. Patterns of Change in Dietary Habits and Physical Activity during Lockdown in Spain Due to the COVID-19 Pandemic. Nutrients 2021, 13, 300. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, M.; Langiano, E.; Falese, L.; De Marco, A.; De Vito, E. Quality of Life and Psychosocial Impacts of the Different Restrictive Measures during One Year into the COVID-19 Pandemic on Patients with Cancer in Italy: An Ecological Study. Int. J. Environ. Res. Public Health 2021, 18, 7161. [Google Scholar] [CrossRef]
- Lamblin, G.; Chene, G.; Leaune, E.; Philip, C.A.; Moret, S.; Nohuz, E.; Golfier, F.; Cortet, M. The Psychological Impact of Therapeutic Changes during the COVID-19-Lockdown for Gynaecological and Breast Cancer Patients. J. Gynecol. Obstet. Hum. Reprod. 2022, 51, 102311. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, A.L.; Lynch, B.M.; Owen, N.; Aitken, J.F. Lifestyle Factors Associated Concurrently and Prospectively with Co-Morbid Cardiovascular Disease in a Population-Based Cohort of Colorectal Cancer Survivors. Eur. J. Cancer 2011, 47, 267–276. [Google Scholar] [CrossRef]
- Strongman, H.; Gadd, S.; Matthews, A.; Mansfield, K.E.; Stanway, S.; Lyon, A.R.; Dos-Santos-Silva, I.; Smeeth, L.; Bhaskaran, K. Medium and Long-Term Risks of Specific Cardiovascular Diseases in Survivors of 20 Adult Cancers: A Population-Based Cohort Study Using Multiple Linked UK Electronic Health Records Databases. Lancet 2019, 394, 1041–1054. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Friedenreich, C.M.; Yang, L. Association of Daily Sitting Time and Leisure-Time Physical Activity with Survival among US Cancer Survivors. JAMA Oncol. 2022, 8, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S.C. Physical Activity and Mortality in Cancer Survivors: A Systematic Review and Meta-Analysis. JNCI Cancer Spectr. 2020, 4, pkz080. [Google Scholar] [CrossRef]
- Lakoski, S.G.; Willis, B.L.; Barlow, C.E.; Leonard, D.; Gao, A.; Radford, N.B.; Farrell, S.W.; Douglas, P.S.; Berry, J.D.; DeFina, L.F.; et al. Midlife Cardiorespiratory Fitness, Incident Cancer, and Survival After Cancer in Men: The Cooper Center Longitudinal Study. JAMA Oncol. 2015, 1, 231–237. [Google Scholar] [CrossRef]
- Narici, M.; De Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G.; et al. Impact of Sedentarism Due to the COVID-19 Home Confinement on Neuromuscular, Cardiovascular and Metabolic Health: Physiological and Pathophysiological Implications and Recommendations for Physical and Nutritional Countermeasures. Eur. J. Sport Sci. 2021, 21, 614–635. [Google Scholar] [CrossRef]
- Miotto, P.M.; McGlory, C.; Bahniwal, R.; Kamal, M.; Phillips, S.M.; Holloway, G.P. Supplementation with Dietary ω-3 Mitigates Immobilization-Induced Reductions in Skeletal Muscle Mitochondrial Respiration in Young Women. FASEB J. 2019, 33, 8232–8240. [Google Scholar] [CrossRef]
- Dirks, M.L.; Miotto, P.M.; Goossens, G.H.; Senden, J.M.; Petrick, H.L.; van Kranenburg, J.; van Loon, L.J.C.; Holloway, G.P. Short-Term Bed Rest-Induced Insulin Resistance Cannot Be Explained by Increased Mitochondrial H(2) O(2) Emission. J. Physiol. 2020, 598, 123–137. [Google Scholar] [CrossRef]
- Florido, R.; Daya, N.R.; Ndumele, C.E.; Koton, S.; Russell, S.D.; Prizment, A.; Blumenthal, R.S.; Matsushita, K.; Mok, Y.; Felix, A.S.; et al. Cardiovascular Disease Risk Among Cancer Survivors: The Atherosclerosis Risk in Communities (ARIC) Study. J. Am. Coll. Cardiol. 2022, 80, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. American Cancer Society Nutrition and Physical Activity Guideline for Cancer Survivors. CA. Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef] [PubMed]
- Salam, A.; Woodman, A.; Chu, A.; Al-Jamea, L.H.; Islam, M.; Sagher, M.; Sager, M.; Akhtar, M. Effect of Post-Diagnosis Exercise on Depression Symptoms, Physical Functioning and Mortality in Breast Cancer Survivors: A Systematic Review and Meta-Analysis of Randomized Control Trials. Cancer Epidemiol. 2022, 77, 102111. [Google Scholar] [CrossRef] [PubMed]
- Fardman, A.; Banschick, G.D.; Rabia, R.; Percik, R.; Fourey, D.; Segev, S.; Klempfner, R.; Grossman, E.; Maor, E. Cardiorespiratory Fitness and Survival Following Cancer Diagnosis. Eur. J. Prev. Cardiol. 2021, 28, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Gilchrist, S.C.; Barac, A.; Ades, P.A.; Alfano, C.M.; Franklin, B.A.; Jones, L.W.; La Gerche, A.; Ligibel, J.A.; Lopez, G.; Madan, K.; et al. Cardio-Oncology Rehabilitation to Manage Cardiovascular Outcomes in Cancer Patients and Survivors: A Scientific Statement from the American Heart Association. Circulation 2019, 139, e997–e1012. [Google Scholar] [CrossRef] [PubMed]
- Hurria, A.; Jones, L.; Muss, H.B. Cancer Treatment as an Accelerated Aging Process: Assessment, Biomarkers, and Interventions. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e516–e522. [Google Scholar] [CrossRef]
- Jones, L.W.; Courneya, K.S.; Mackey, J.R.; Muss, H.B.; Pituskin, E.N.; Scott, J.M.; Hornsby, W.E.; Coan, A.D.; Herndon, J.E., 2nd; Douglas, P.S.; et al. Cardiopulmonary Function and Age-Related Decline across the Breast Cancer Survivorship Continuum. J. Clin. Oncol. 2012, 30, 2530–2537. [Google Scholar] [CrossRef]
- Bleyer, A.; Barr, R. Cancer in Young Adults 20 to 39 Years of Age: Overview. Semin. Oncol. 2009, 36, 194–206. [Google Scholar] [CrossRef]
- Guevara, M.; Molinuevo, A.; Salmerón, D.; Marcos-Gragera, R.; Carulla, M.; Chirlaque, M.-D.; Rodríguez Camblor, M.; Alemán, A.; Rojas, D.; Vizcaíno Batllés, A.; et al. Cancer Survival in Adults in Spain: A Population-Based Study of the Spanish Network of Cancer Registries (REDECAN). Cancers 2022, 14, 2441. [Google Scholar] [CrossRef]
- Warner, E.L.; Kent, E.E.; Trevino, K.M.; Parsons, H.M.; Zebrack, B.J.; Kirchhoff, A.C. Social Well-Being among Adolescents and Young Adults with Cancer: A Systematic Review. Cancer 2016, 122, 1029–1037. [Google Scholar] [CrossRef]
- Lindenmann, J.; Fink-Neuboeck, N.; Fediuk, M.; Maier, A.; Kovacs, G.; Balic, M.; Smolle, J.; Smolle-Juettner, F.M. Preoperative Peak Oxygen Consumption: A Predictor of Survival in Resected Lung Cancer. Cancers 2020, 12, 836. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.-Y.; Lee, Y.-H.; Chan, J.-C.; Chiou, P.-Y.; Chou, X.-Y.; Chiu, W.-T.; Hung, C.-T. Effects of Exercise Interventions on Social and Cognitive Functioning of Men with Prostate Cancer: A Meta-Analysis. Support. Care Cancer 2020, 28, 2043–2057. [Google Scholar] [CrossRef] [PubMed]
- Cannavino, J.; Brocca, L.; Sandri, M.; Grassi, B.; Bottinelli, R.; Pellegrino, M.A. The Role of Alterations in Mitochondrial Dynamics and PGC-1α over-Expression in Fast Muscle Atrophy Following Hindlimb Unloading. J. Physiol. 2015, 593, 1981–1995. [Google Scholar] [CrossRef] [PubMed]
- Hood, D.A.; Memme, J.M.; Oliveira, A.N.; Triolo, M. Maintenance of Skeletal Muscle Mitochondria in Health, Exercise, and Aging. Annu. Rev. Physiol. 2019, 81, 19–41. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Sample N = 171 | Age Category 18–30 N = 18 | Age Category 31–40 N = 63 | Age Category 40–45 N = 90 | |||||
|---|---|---|---|---|---|---|---|---|
| Female | Male | Female | Male | Female | Male | Female | Male | |
| Age | 39.2 ± 5.6 | 37.9 ± 7.6 | 26.5 ± 2.9 | 23.3 ± 3 | 36.6 ± 2.8 | 37 ± 2.9 | 43.3 ± 1.4 | 43.3 ± 1.9 |
| Level of Physical Activity | ||||||||
| Low levels | ||||||||
| Before COVID | 44 (25.7) | 8 (4.7) | 4 (2.7) | 1 (4.2) | 16 (10.9) | 1 (4.2) | 24 (16.3) | 6 (25) |
| During COVID | 74 (43.3) | 13 (7.6) | 5 (3.4) | 2 (8.3) | 28 (19) | 6 (25) | 41 (50.3) | 5 (20.8) |
| After COVID | 47 (27.5) | 11 (6.4) | 4 (2.7) | 2 (8.3) | 13 (8.8) | 2 (8.3) | 30 (20.4) | 7 (29.2) |
| Moderate levels | ||||||||
| Before COVID | 54 (31.6) | 8 (4.7) | 5 (3.4) | 2 (8.3) | 21 (14.3) | 3 (12.5) | 28 (19) | 3 (12.5) |
| During COVID | 35 (20.5) | 5 (2.9) | 5 (3.4) | 1 (4.2) | 11 (7.5) | 2 (8.3) | 19 (12.9) | 2 (8.3) |
| After COVID | 44 (25.7) | 4 (2.3) | 6 (4.1) | 0 (0) | 18 (12.2) | 2 (8.3) | 20 (13.6) | 2 (8.3) |
| Hight levels | ||||||||
| Before COVID | 49 (28.8) | 8 (4.7) | 5 (3.4) | 1 (4.2) | 18 (12.2) | 4 (16.7) | 26 (17.7) | 3 (12.5) |
| During COVID | 38 (22.2) | 6 (3.5) | 4 (2.7) | 1 (4.2) | 16 (10.9) | 0 (0) | 18 (12.2) | 5 (20.8) |
| After COVID | 56 (32.7) | 9 (5.3) | 4 (2.7) | 2 (8.3) | 24 (16.3) | 4 (16.7) | 28 (19) | 3 (12.5) |
| Total of physical activity | ||||||||
| Before COVID | 1861.2 ± 1491.6 | 1720.4 ± 1056.7 | 2097.4 ± 2058.2 | 1759.9 ± 1274.5 | 1780.6 ± 1326.5 | 2069.3 ± 1143.2 | 1875.6 ± 1501.5 | 1474.8 ± 951.4 |
| During COVID | 1353.3 ± 1696.2 | 1281.2 ± 1418.7 | 2137.1 ± 2077.3 | 1288.5 ± 1070.9 | 1299.4 ± 1516.9 | 287.1 ± 369.9 | 1250.5 ± 1728.8 | 1941.5 ± 1616.8 |
| After COVID | 2067.4 ± 1931 | 1666.6 ± 1394.8 | 2245.4 ± 1436.3 | 1262.3 ± 1457.7 | 2049.4 ± 1470 | 1856.6 ± 1354.5 | 2048.2 ± 2133.6 | 1674.6 ± 1495.8 |
| Light physical activity | ||||||||
| Before COVID | 754.3 ± 492.7 | 575.4 ± 433.9 | 820.3 ± 546.3 | 754.9547.3 | 770.4 ± 480.5 | 569.3 ± 463.6 | 731.1 ± 496.5 | 519.8 ± 400.1 |
| During COVID | 391.6 ± 567.3 | 418.7 ± 560 | 572.8 ± 663.7 | 148.5 ± 171.5 | 364.5 ± 546.9 | 167.1 ± 341.9 | 378.2 ± 565.2 | 676.5 ± 654.4 |
| After COVID | 724.9 ± 498.5 | 546.5 ± 428.4 | 809.7 ± 600.2 | 272.3 ± 336.9 | 793.8 ± 473.4 | 581.6 ± 328.1 | 661.3 ± 494.3 | 614.6 ± 501 |
| Moderate physical activity | ||||||||
| Before COVID | 708.9 ± 645.2 | 662.5 ± 592.2 | 792.8 ± 729.2 | 945 ± 849.1 | 725.5 ± 649.6 | 705 ± 599.8 | 682.3 ± 633.6 | 540 ± 511 |
| During COVID | 356.7 ± 612.5 | 320 ± 490.2 | 591.4 ± 818.9 | 210 ± 344.7 | 309.8 ± 567.5 | 311.2 ± 289.5 | 347.7 ± 600.5 | 570 ± 568.3 |
| After COVID | 665.7 ± 714.9 | 562.5 ± 565 | 492.9 ± 762.7 | 450 ± 521.9 | 660 ± 665.3 | 817.5 ± 634.9 | 700.8 ± 744.2 | 430 ± 515.4 |
| Hight physical activity | ||||||||
| Before COVID | 702.9 ± 874.4 | 755 ± 609.3 | 874.3 ± 1197.6 | 690 ± 521.9 | 632.7 ± 825.1 | 1065 ± 740.9 | 721.5 ± 849.1 | 570 ± 493.8 |
| During COVID | 635.9 ± 913.4 | 480 ± 683.4 | 1191.4 ± 1096.3 | 480 ± 678.8 | 654.5 ± 896.1 | 900 ± 254.6 | 523.1 ± 864 | 740 ± 790.8 |
| After COVID | 890.6 ± 1224.5 | 715 ± 765.1 | 1097.1 ± 1612.6 | 720 ± 831.4 | 840 ± 985.8 | 795 ± 818.8 | 889.2 ± 1308.9 | 660 ± 775.2 |
| Secondary outcomes | ||||||||
| Weight (kg) | ||||||||
| Before COVID | 64.3 ± 12.5 | 79.3 ± 12.6 | 59.9 ± 8.2 | 73.5 ± 6.8 | 63.6 ± 11.1 | 81 ± 9.9 | 65.6 ± 13.9 | 80.3 ± 15.5 |
| During COVID | 64.8 ± 12.9 | 79.3 ± 12.7 | 59.7 ± 8.1 | 72.8 ± 5.9 | 64.5 ± 12.6 | 79.6 ± 10.7 | 66.1 ± 13.8 | 81.3 ± 15.3 |
| After COVID | 64.7 ± 13.3 | 79.6 ± 12.6 | 58.7 ± 7.7 | 73.3 ± 6.6 | 64.5 ± 12.7 | 79.9 ± 10.6 | 65.9 ± 14.2 | 81.6 ± 15.1 |
| BMI (kg/m2) | ||||||||
| Before COVID | 24.2 ± 4.3 | 24.6 ± 5.2 | 21.8 ± 2.7 | 21.3 ± 2.2 | 24.2 ± 3.5 | 25 ± 6 | 24.7 ± 4.8 | 25.5 ± 5.3 |
| During COVID | 24.2 ± 4.1 | 24.3 ± 4.8 | 22.1 ± 2.9 | 20.5 ± 1.9 | 23.9 ± 3.6 | 24.1 ± 2.8 | 24.7 ± 4.5 | 25.8 ± 5.9 |
| After COVID | 25.1 ± 4.3 | 25.3 ± 4.6 | 23.5 ± 3.2 | 20.8 ± 2.3 | 25.1 ± 4 | 24.1 ± 2.2 | 25.4 ± 4.7 | 27.6 ± 5.1 |
| Sitting time (hours/day) | ||||||||
| Before COVID | 6.9 ± 3.6 | 6.9 ± 3.1 | 7.1 ± 3.7 | 8.2 ± 5.5 | 6.9 ± 3.3 | 7 ± 3 | 6.9 ± 3.7 | 6.5 ± 2.4 |
| During COVID | 9.4 ± 4.2 | 8.7 ± 3.6 | 11.3 ± 4.1 | 11.5 ± 5.8 | 10.2 ± 4.7 | 9.3 | 8.5 ± 3.8 | 7.4 ± 2.9 |
| After COVID | 7.2 ± 3.8 | 7.5 ± 4.5 | 9.4 ± 5.1 | 11.3 ± 10 | 7.8 ± 3.8 | 6.8 ± 3.1 | 6.5 ± 3.3 | 6.5 ± 1.8 |
| Eq5d index value | ||||||||
| Before COVID | 0.902 ± 0.1 | 0.908 ± 0.1 | 0.903 ± 0.1 | 927 ± 0.1 | 0.915 ± 0.1 | 0.897 ± 0.2 | 0.893 ± 0.1 | 0.909 ± 0.1 |
| During COVID | 0.842 ± 0.1 | 0.884 ± 0.1 | 0.804 ± 0.2 | 0.910 ± 0.1 | 0.838 ± 0.2 | 0.876 ± 0.1 | 0.853 ± 0.1 | 0.88 ± 0.1 |
| After COVID | 0.882 ± 0.1 | 0.86 ± 0.2 | 0.835 ± 0.2 | 0.811 ± 0.3 | 0.892 ± 0.1 | 0.892 ± 0.1 | 0.883 ± 0.1 | 0.855 ± 0.1 |
| Eq5d percentage of health (%) | ||||||||
| Before COVID | 75.9 ± 21.8 | 79 ± 18.9 | 75.2 ± 29.9 | 87.5 ± 12.6 | 78.1 ± 19.8 | 66.3 ± 24.6 | 74.6 ± 21.7 | 84.7 ± 11.9 |
| During COVID | 69.3 ± 23.1 | 67.5 ± 20.8 | 65.8 ± 30.9 | 72.5 ± 17 | 72.1 ± 22.8 | 59.4 ± 26.1 | 67.9 ± 21.9 | 71.9 ± 17.9 |
| After COVID | 72.4 ± 21.6 | 65.8 ± 25.6 | 68.4 ± 26.9 | 57.5 ± 44.3 | 75.1 ± 22.3 | 63.8 ± 25.7 | 71.3 ± 20.1 | 70 ± 19 |
| Fatigue total | ||||||||
| Before COVID | 37.6 ± 8.9 | 35.5 ± 9.4 | 39.5 ± 6.3 | 36.8 ± 10.2 | 37.6 ± 9.5 | 38.3 ± 11.2 | 37.3 ± 0.1 | 33.3 ± 8.2 |
| During COVID | 34.5 ± 11.7 | 33 ± 13 | 31.6 ± 15.4 | 32.8 ± 23.4 | 34.1 ± 13.1 | 33 ± 12.6 | 35.3 ± 9.8 | 33.2 ± 10.2 |
| After COVID | 36.4 ± 10 | 34.3 ± 11.1 | 33.4 ± 13.2 | 33.5 ± 16.3 | 36.7 ± 10.9 | 36.5 ± 11.2 | 36.7 ± 8.6 | 33.1 ± 9.9 |
| Breast Cancer N = 114 | Other Tumours N = 57 | With Treatment N = 75 | No Treatment N = 96 | |
|---|---|---|---|---|
| Age | 39.9 (4.8) | 37.1 (7.3) | 38.8 (5.9) | 39.2 (5.9) |
| Gender | ||||
| Female | 113 (66.08) | 34 (19.88) | 65 (38) | 82 (48) |
| Male | 1 (.58) | 23 (13.45) | 10 (5.8) | 14 (8.2) |
| Level of physical activity | ||||
| Low levels | ||||
| Before COVID | 35 (20.5) | 17 (9.9) | 19 (11.1) | 33 (19.3) |
| During COVID | 58 (33.9) | 29 (17) | 31 (18.1) | 56 (32.7) |
| After COVID | 38 (22.2) | 20 (11.7) | 20 (11.7) | 38 (22.2) |
| Moderate levels | ||||
| Before COVID | 44 (25.7) | 22 (12.9) | 34 (19.9) | 28 (16.4) |
| During COVID | 26 (15.2) | 14 (8.2) | 19 (11.1) | 21 (12.3) |
| After COVID | 32 (18.7) | 16 (9.4) | 20 (11.7) | 28 (16.4) |
| Hight levels | ||||
| Before COVID | 35 (20.5) | 22 (12.9) | 22 (12.9) | 35 (20.5) |
| During COVID | 30 (17.5) | 14 (8.2) | 25 (14.6) | 19 (11.1) |
| After COVID | 44 (25.7) | 21 (12.3) | 35 (20.5) | 30 (17.5) |
| Total of physical activity | ||||
| Before COVID | 1757.8 ± 1366.6 | 2008,9 ± 1567 | 1836.4 ± 1346.3 | 1845.4 ± 1510.7 |
| During COVID | 1346.1 ± 1701.8 | 1337.1 ± 1576.7 | 1545.2 ± 1794.5 | 1185.3 ± 1531.2 |
| After COVID | 2114.5 ± 1981.5 | 1804.6 ± 1612.4 | 2298.6 ± 1929.2 | 1786.7 ± 1796.2 |
| Light physical activity | ||||
| Before COVID | 742.5 ± 478.1 | 702.5 ± 509.8 | 820.4 ± 469.9 | 657.9 ± 491.9 |
| During COVID | 407.72 ± 559.8 | 370.8 ± 578.7 | 458 ± 584.6 | 346.5 ± 546.8 |
| After COVID | 730.8 ± 479.6 | 638.3 ± 514.8 | 749.8 ± 491.7 | 661 ± 491.6 |
| Moderate physical activity | ||||
| Before COVID | 664.7 ± 625.1 | 777.9 ± 658.1 | 780 ± 654 | 641.9 ± 619.3 |
| During COVID | 377.4 ± 625.4 | 300 ± 532.9 | 444 ± 664.5 | 279.4 ± 528.3 |
| After COVID | 690 ± 727.4 | 573.7 ± 625.1 | 764 ± 772.6 | 563.1 ± 618.3 |
| Hight physical activity | ||||
| Before COVID | 631.6 ± 808.5 | 867 ± 888.8 | 622.4 ± 809.7 | 778.8 ± 862.5 |
| During COVID | 608.42 ± 911.8 | 625.3 ± 835.6 | 726.4 ± 933.3 | 526.3 ± 839.3 |
| After COVID | 903.2 ± 1255.4 | 791.6 ± 986.1 | 1019.2 ± 1253 | 746.3 ± 1093.9 |
| secondary outcomes | ||||
| Weight (kg) | ||||
| Before COVID | 63.4 ± 12 | 72 ± 14.8 | 64 ± 12.4 | 68.3 ± 14.2 |
| During COVID | 64.5 ± 12.6 | 71.6 ± 15 | 64.7 ± 12.6 | 68.7 ± 14.6 |
| After COVID | 64.5 ± 13.2 | 71.4 ± 15 | 64.6 ± 12.7 | 68.5 ± 15.1 |
| BMI (kg/m2) | ||||
| Before COVID | 24.3 ± 4.5 | 24.3 ± 4.2 | 24.6 ± 4.5 | 24.1 ± 4.3 |
| During COVID | 24.1 ± 4.2 | 24.4 ± 4.2 | 24.3 ± 4.4 | 24.1 ± 4.1 |
| After COVID | 25.1 ± 4.5 | 25.3 ± 3.9 | 25.4 ± 5.5 | 24.9 ± 4 |
| Sitting time (hours/day) | ||||
| Before COVID | 7 ± 3.2 | 6.7 ± 4 | 6.8 ± 3.7 | 7 ± 3.8 |
| During COVID | 8.9 ± 3.7 | 9.9 ± 4.9 | 8.6 ± 3.3 | 9.9 ± 4.7 |
| After COVID | 7.1 ± 3.6 | 7.7 ± 4.5 | 7 ± 3.4 | 7.5 ± 4.2 |
| Eq-5d index value | ||||
| Before COVID | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.93 ± 0.1 | 0.9 ± 0.1 |
| During COVID | 0.86 ± 0.2 | 0.83 ± 0.2 | 0.9 ± 0.2 | 0.8 ± 0.2 |
| After COVID | 0.901 ± 0.1 | 0.9 ± 0.2 | 0.9 ± 0.1 | 0.9 ± 0.1 |
| Eq-5d percentage of health (%) | ||||
| Before COVID | 75.5 ± 21.4 | 78.1 ± 21.5 | 74.7 ± 22.7 | 77.8 ± 20.4 |
| During COVID | 68.3 ± 23.5 | 70.5 ± 21.4 | 66.1 ± 25.5 | 71.3 ± 20.4 |
| After COVID | 72.2 ± 21.1 | 70.1 ± 24.6 | 71 ± 23 | 71.9 ± 21.8 |
| Fatigue total | ||||
| Before COVID | 37.6 ± 8.9 | 36.7 ± 9.2 | 39 ± 8.2 | 35.9 ± 9.5 |
| During COVID | 35.9 ± 10.8 | 31.2 ± 13.4 | 37.3 ± 10.4 | 32 ± 12.5 |
| After COVID | 37.1 ± 9.3 | 33.9 ± 115 | 38.4 ± 10.4 | 34.3 ± 9.7 |
| Before–During Lockdown | Before–After Lockdown | During–After Lockdown | ||||
|---|---|---|---|---|---|---|
| DifM (95% CI) | p Value | DifM (95% CI) | p Value | DifM (95% CI) | p Value | |
| Physical activity levels | ||||||
| Total Activity (METS) | −498.3 (−800.97 to −195.68) | 0.0001 * | 169.7 (−121.11 to 460.53) | 0.480 | 668.04 (384.2 to 951.88) | 0.0001 * |
| High (METS) | −96.1 (−258.90 to 66.62) | 0.465 | 155.8 (−43.87 to 355.45) | 0.183 | 251.9 (75.99 to 427.87) | 0.002 * |
| Moderate (METS) | −350 (−491.54 to −210.21) | 0.0001 * | −51.2 (−182.18 to 79.72) | 1.00 | 299.7 (174.50 to 424.80) | 0.0001 * |
| Light (METS) | −333.8 (−455.92 to −211.61) | 0.0001 * | −29.2 (−119.32 to 60.85) | 1.000 | 304.5 (211.61 to 455.92) | 0.0001 * |
| Anthropometric measures | ||||||
| Weight (Kg) | 0.47 (−0.12 to 1.06) | 0.169 | 0.35 (−0.42 to 1.12) | 0.809 | −0.12 (−0.55 to 0.31) | 1.00 |
| BMI (kg/m2) | −0.08 (0.334 to −0.498) | 1.00 | 0.85 (0.27 to 1.4) | 0.002 * | 0.93 (0.4 to 1.5) | 0.0001 * |
| Patients reported outcomes | ||||||
| Sitting time (hours) | 2.4 (1.6 to 3.1) | 0.001 * | 0.363 (−0.31 to 1.04) | 0.582 | −2 (−2.6 to −1.4) | 0.001 * |
| EQ5D index value | −0.5 (−0.922 to −0.884) | 0.0001 * | −0.02 (−0.874 to −0.823) | 0.110 | 0.03 (−0.900 to −0.858) | 0.004 * |
| EQ5D percentage of health (%) | −7.4 (−3.811 to −10.9) | 0.0001 * | −4.9 (−1.3 to −8.5) | 0.004 * | 2.5 (5.1 to −0.14) | 0.069 |
| Fatigue Total | −2.9 (−4.75 to −1.24) | 0.0001 * | −1.2 (−2.89 to 0.41) | 0.211 | 1.8 (.24 to 3.27) | 0.0017 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellanos-Montealegre, M.; Rivera-Theruel, F.; García-Coll, V.; Rioja-Collado, N.; Gil-Herrero, L.; López-Tarruella, S.; Montealegre Sanz, M.; Cerezo González, S.; Fernández Aramburo, A.; Ruiz-Casado, A.; et al. Impact of the COVID-19 Lockdown on Physical Activity Levels and Health Parameters in Young Adults with Cancer. Curr. Oncol. 2023, 30, 5395-5408. https://doi.org/10.3390/curroncol30060409
Castellanos-Montealegre M, Rivera-Theruel F, García-Coll V, Rioja-Collado N, Gil-Herrero L, López-Tarruella S, Montealegre Sanz M, Cerezo González S, Fernández Aramburo A, Ruiz-Casado A, et al. Impact of the COVID-19 Lockdown on Physical Activity Levels and Health Parameters in Young Adults with Cancer. Current Oncology. 2023; 30(6):5395-5408. https://doi.org/10.3390/curroncol30060409
Chicago/Turabian StyleCastellanos-Montealegre, Mónica, Fernando Rivera-Theruel, Virginia García-Coll, Natalia Rioja-Collado, Lucía Gil-Herrero, Sara López-Tarruella, María Montealegre Sanz, Sara Cerezo González, Antonio Fernández Aramburo, Ana Ruiz-Casado, and et al. 2023. "Impact of the COVID-19 Lockdown on Physical Activity Levels and Health Parameters in Young Adults with Cancer" Current Oncology 30, no. 6: 5395-5408. https://doi.org/10.3390/curroncol30060409
APA StyleCastellanos-Montealegre, M., Rivera-Theruel, F., García-Coll, V., Rioja-Collado, N., Gil-Herrero, L., López-Tarruella, S., Montealegre Sanz, M., Cerezo González, S., Fernández Aramburo, A., Ruiz-Casado, A., Laundos, R., & Casla-Barrio, S. (2023). Impact of the COVID-19 Lockdown on Physical Activity Levels and Health Parameters in Young Adults with Cancer. Current Oncology, 30(6), 5395-5408. https://doi.org/10.3390/curroncol30060409