Conventional versus Reduced-Frequency Follow-Up in Early-Stage Melanoma Survivors: A Systematic Review with Meta-Analysis

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Terms
2.2. Assessment of Eligibility
2.3. Extraction of Data
2.4. Outcomes of Interest
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
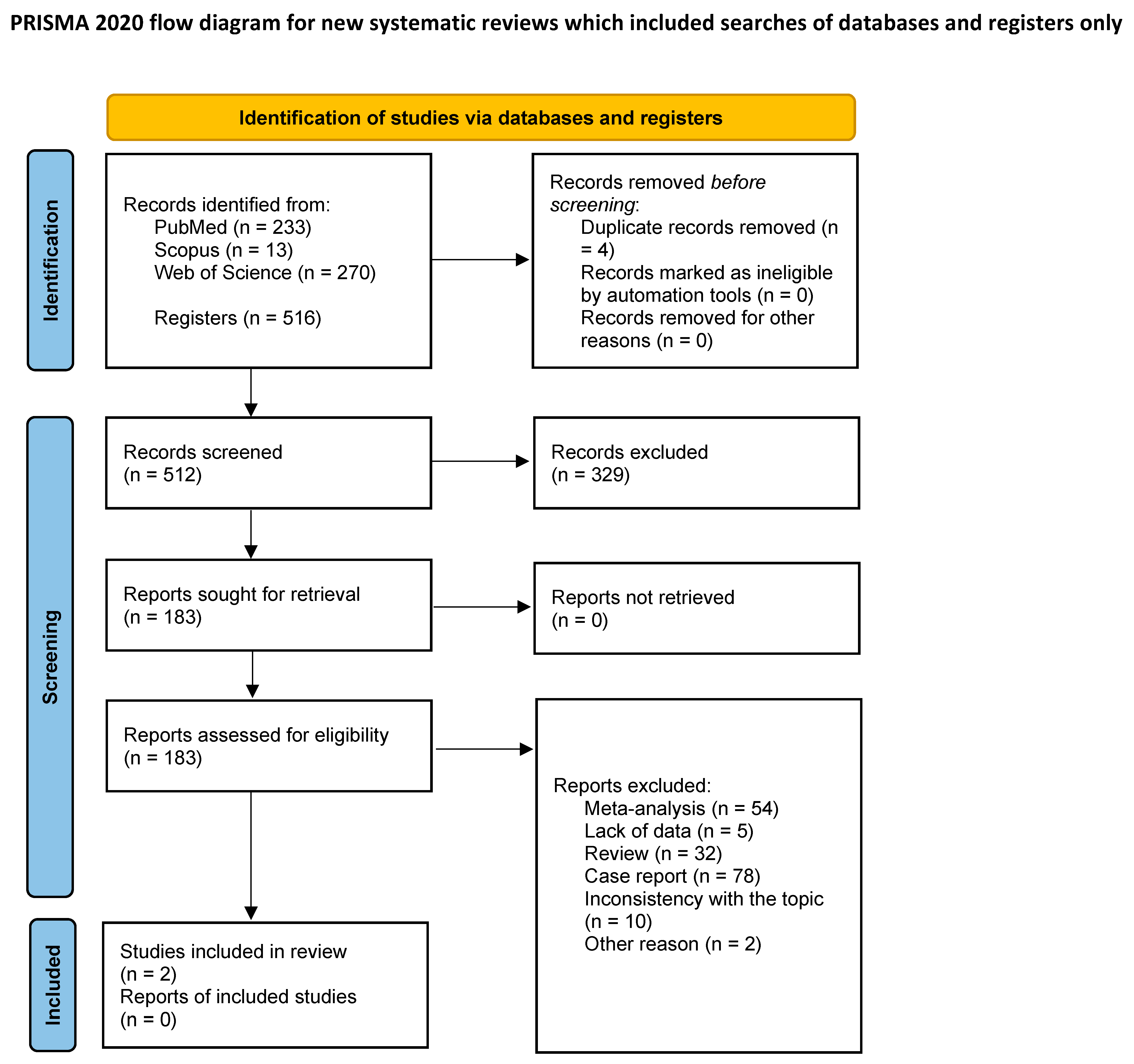
3.1. Article Selection
3.2. Characteristics of the Articles
3.3. Characteristics of the Patients
3.4. Melanoma Recurrence
3.5. 3-Year Melanoma Survival
3.6. Assessment of Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Michielin, O.A.; van Akkooi, P.; Lorigan, P.A.; Ascierto, R.; Dummer, C.; Robert, A.; Arance, C.U.; Blank, V.; Chiarion Sileni, M.; Donia, M.B.; et al. ESMO consensus conference recommenda-tions on the management of locoregional melanoma: Under the auspices of the ESMO Guidelines Committee. Ann. Oncol. 2020, 31, 1449–1461. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Cancer (UK). Melanoma: Assessment and Management; National Institute for Health and Care Excellence (NICE): London, UK; Manchester, UK, 2015. [Google Scholar]
- Wysocki, W.M.; Grela-Wojewoda, A.; Jankowski, M. Fallen dogmas: Recent advances in locoregionally advanced melanoma. Pol. Arch. Intern. Med. 2021, 131, 464–468. [Google Scholar] [CrossRef] [PubMed]
- Trotter, S.C.; Sroa, N.; Winkelmann, R.R.; Olencki, T.; Bechtel, M. A Global Review of Melanoma Follow-up Guidelines. J. Clin. Aesthetic Dermatol. 2013, 6, 18–26. [Google Scholar]
- Rutkowski, P.; Lugowska, I. Follow-up in melanoma patients. Memo 2014, 7, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Hengge, U.R.; Wallerand, A.; Stutzki, A.; Kockel, N. Cost-effectiveness of reduced fol-low-up in malignant melanoma. J. Der Dtsch. Dermatol. Ges. J. Ger. Soc. Dermatol. JDDG 2007, 5, 898–907. [Google Scholar] [CrossRef]
- Turner, R.M.; Bell, K.J.; Morton, R.L.; Hayen, A.; Francken, A.B.; Howard, K.; Armstrong, B.; Thompson, J.F.; Irwig, L. Optimizing the frequency of follow-up visits for patients treated for localized primary cutaneous melanoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 4641–4646. [Google Scholar] [CrossRef] [PubMed]
- Wevers, K.P.; Hoekstra-Weebers, J.E.; Speijers, M.J.; Bergman, W.; Gruis, N.A.; Hoekstra, H.J. Cutaneous melanoma: Medical specialists’ opinions on follow-up and sentinel lymph node bi-opsy. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2014, 40, 1276–1283. [Google Scholar] [CrossRef] [PubMed]
- Elmas, Ö.F.; Demirbaş, A.; Düzayak, S.; Atasoy, M.; Türsen, Ü.; Lotti, T. Melanoma and COVID-19: A narrative review focused on treatment. Dermatol. Ther. 2020, 33, e14101. [Google Scholar] [CrossRef]
- Marushchak, O.; Hazan, E.; Kriegel, D.A. Analyzing Controversies in Management and Surveillance of Early-Stage Melanoma. Oncol. Ther. 2020, 8, 191–196. [Google Scholar] [CrossRef]
- Richter, K.; Stefura, T.; Kłos, N.; Tempski, J.; Kołodziej-Rzepa, M.; Kisielewski, M.; Wojewoda, T.; Wysocki, W.M. Conventional versus reduced-frequency follow-up in early-stage melanoma survivors: A systematic review with meta-analysis. PROSPERO Int. Prospect. Regist. Syst. Rev. 2022, CRD42022366378. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef] [PubMed]
- Deckers, E.A.; Hoekstra-Weebers, J.; Damude, S.; Francken, A.B.; Ter Meulen, S.; Bastiaannet, E.; Hoekstra, H.J. The MELFO Study: A Multicenter, Prospective, Randomized Clinical Trial on the Effects of a Reduced Stage-Adjusted Follow-Up Schedule on Cutaneous Melanoma IB-IIC Pa-tients-Results After 3 Years. Ann. Surg. Oncol. 2020, 27, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Moncrieff, M.D.; Underwood, B.; Garioch, J.J.; Heaton, M.; Patel, N.; Bastiaannet, E.; Hoekstra-Weebers, J.; Hoekstra, H.J. The MelFo Study UK: Effects of a Reduced-Frequency, Stage-Adjusted Follow-Up Schedule for Cutaneous Melanoma 1B to 2C Patients After 3-Years. Ann. Surg. Oncol. 2020, 27, 4109–4119. [Google Scholar] [CrossRef] [PubMed]
- Richter, K.; Stefura, T.; Macheta, K.; Tempski, J.; Kazoń, J.; Szeremeta, M.; Klimont, P.; Kołodziej-Rzepa, M.; Wojewoda, T.; Wysocki, W.M. Does It Really Pay-Off? Comparison of Lymphadenectomy versus Observational Approach in Skin Melanoma with Positive Sentinel Node Biopsy: Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 3880. [Google Scholar] [CrossRef] [PubMed]
- Jassem, J.; Kowalczyk, A.; Biesiada, A.; Duchnowska, R.; Dziadziuszko, R.; Masztalerz-Migas, A.; Kawecki, A.; Krzakowski, M.; Potemski, P.; Rutkowski, P.; et al. Post-treatment follow-up in common solid malignancies: Expert panel recommendations. Nowotw. J. Oncol. 2022, 72, 360–383. [Google Scholar] [CrossRef]
- Leiter, U.; Eigentler, T.K.; Forschner, A.; Pflugfelder, A.; Weide, B.; Held, L.; Meier, F.; Garbe, C. Excision guidelines and follow-up strategies in cutaneous melanoma: Facts and controversies. Clin. Dermatol. 2010, 28, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Read, R.L.; Madronio, C.M.; Cust, A.E.; Goumas, C.; Watts, C.G.; Menzies, S.; Curtin, A.M.; Mann, G.; Thompson, J.F.; Morton, R.L. Follow-Up Recommendations after Diagnosis of Primary Cutaneous Melanoma: A Population-Based Study in New South Wales, Australia. Ann. Surg. Oncol. 2018, 25, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Rychetnik, L.; McCaffery, K.; Morton, R.L.; Thompson, J.F.; Menzies, S.W.; Irwig, L. Follow-up of early stage melanoma: Specialist clinician perspectives on the functions of follow-up and implications for ex-tending follow-up intervals. J. Surg. Oncol. 2013, 107, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Watts, C.G.; Dieng, M.; Morton, R.L.; Mann, G.J.; Menzies, S.W.; Cust, A.E. Clinical practice guidelines for identification, screening and follow-up of individuals at high risk of primary cutaneous melanoma: A systematic review. Br. J. Dermatol. 2015, 172, 33. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Title | The MELFO Study: A Multicenter, Prospective, Randomized Clinical Trial on the Effects of a Reduced Stage-Adjusted Follow-Up Schedule on Cutaneous Melanoma IB–IIC Patients—Results after 3 Years [13] | The MelFo Study UK: Effects of a Reduced-Frequency, Stage-Adjusted Follow-Up Schedule for Cutaneous Melanoma 1B to 2C Patients after 3-Years [14] |
|---|---|---|
| Publication year | 2020 | 2020 |
| Study design | RCT | RCT |
| Country | Netherlands | UK |
| Sample (n) | 180 | 207 |
| Sex (% of women) | 52 | 47.8 |
| Median age | 57 | 62 |
| Ulceration (n) | 25 | 41 |
| Breslow < 1 mm | 8 | 47 |
| Recurrence total | 25 | 35 |
| HR—3-year disease free | 1.24 | 0.81 |
| HR for overall survival—95% CI | 1.06 | 1.21 |
| HR for recurrence free survival 95% Cl | 0.71 | 1.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richter, K.; Stefura, T.; Kłos, N.; Tempski, J.; Kołodziej-Rzepa, M.; Kisielewski, M.; Wojewoda, T.; Wysocki, W.M. Conventional versus Reduced-Frequency Follow-Up in Early-Stage Melanoma Survivors: A Systematic Review with Meta-Analysis. Curr. Oncol. 2023, 30, 3366-3372. https://doi.org/10.3390/curroncol30030256
Richter K, Stefura T, Kłos N, Tempski J, Kołodziej-Rzepa M, Kisielewski M, Wojewoda T, Wysocki WM. Conventional versus Reduced-Frequency Follow-Up in Early-Stage Melanoma Survivors: A Systematic Review with Meta-Analysis. Current Oncology. 2023; 30(3):3366-3372. https://doi.org/10.3390/curroncol30030256
Chicago/Turabian StyleRichter, Karolina, Tomasz Stefura, Nikola Kłos, Jonasz Tempski, Marta Kołodziej-Rzepa, Michał Kisielewski, Tomasz Wojewoda, and Wojciech M. Wysocki. 2023. "Conventional versus Reduced-Frequency Follow-Up in Early-Stage Melanoma Survivors: A Systematic Review with Meta-Analysis" Current Oncology 30, no. 3: 3366-3372. https://doi.org/10.3390/curroncol30030256
APA StyleRichter, K., Stefura, T., Kłos, N., Tempski, J., Kołodziej-Rzepa, M., Kisielewski, M., Wojewoda, T., & Wysocki, W. M. (2023). Conventional versus Reduced-Frequency Follow-Up in Early-Stage Melanoma Survivors: A Systematic Review with Meta-Analysis. Current Oncology, 30(3), 3366-3372. https://doi.org/10.3390/curroncol30030256