Treatment Patterns and Outcomes of Patients with Grade 4 Glioma Treated with Radiation during the COVID-19 Pandemic


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Treatment
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment Details
3.3. Direct Influence of COVID on Management during the COVID Era
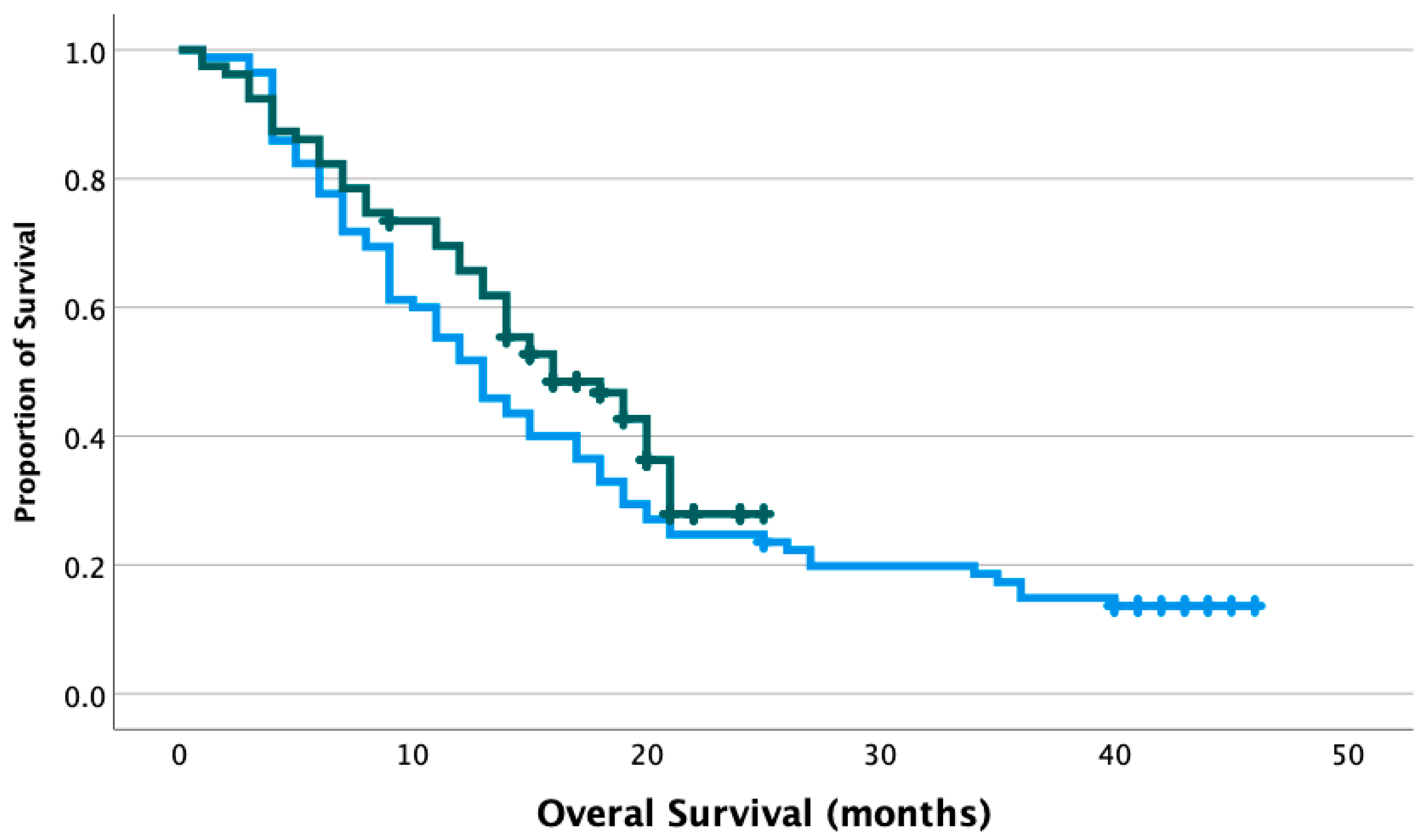
3.4. Survival between Eras
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bardin, A.; Buja, A.; Amidei, C.B.; Paganini, M.; Favaro, A.; Saia, M.; Baldo, V. Elderly People’s Access to Emergency Departments during the COVID-19 Pandemic: Results from a Large Population-Based Study in Italy. J. Clin. Med. 2021, 10, 5563. [Google Scholar] [CrossRef] [PubMed]
- Parmar, A.; Eskander, A.; Sander, B.; Naimark, D.; Irish, J.C.; Chan, K.K. Impact of cancer surgery slowdowns on patient survival during the COVID-19 pandemic: A microsimulation modelling study. CMAJ 2022, 194, E408–E414. [Google Scholar] [CrossRef] [PubMed]
- Lunski, M.J.; Burton, J.; Tawagi, K.; Maslov, D.; Simenson, V.; Barr, D.; Yuan, H.; Johnson, D.; Matrana, M.; Cole, J.; et al. Multivariate mortality analyses in COVID-19: Comparing patients with cancer and patients without cancer in Louisiana. Cancer 2021, 127, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Bertuzzi, A.F.; Ciccarelli, M.; Marrari, A.; Gennaro, N.; Dipasquale, A.; Giordano, L.; Cariboni, U.; Quagliuolo, V.L.; Alloisio, M.; Santoro, A. Impact of active cancer on COVID-19 survival: A matched-analysis on 557 consecutive patients at an Academic Hospital in Lombardy, Italy. Br. J. Cancer 2021, 125, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Tabernero, J.; Bower, M.; Scotti, L.; Patel, M.; Colomba, E.; Dolly, S.; Loizidou, A.; Chester, J.; Mukherjee, U.; et al. Prevalence and impact of COVID-19 sequelae on treatment and survival of patients with cancer who recovered from SARS-CoV-2 infection: Evidence from the OnCovid retrospective, multicentre registry study. Lancet Oncol. 2021, 22, 1669–1680. [Google Scholar] [CrossRef]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhenn, P.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef]
- Bernhardt, D.; Wick, W.; Weiss, S.E.; Sahgal, A.; Lo, S.S.; Suh, J.H.; Chang, E.L.; Foote, M.; Perry, J.; Meyer, B.; et al. Neuro-oncology Management During the COVID-19 Pandemic With a Focus on WHO Grade III and IV Gliomas. Neuro Oncol. 2020, 22, 928–935. [Google Scholar] [CrossRef]
- Raffiq, A.; Seng, L.B.; San, L.S.; Zakaria, Z.; Yee, A.S.; Fitzrol, D.N.; Hassan, W.M.N.W.; Idris, Z.; Ghani, A.R.I.; Rosman, A.K.; et al. COVID-19 Pandemic and Its Impact on Neurosurgery Practice in Malaysia: Academic Insights, Clinical Experience and Protocols from March till August 2020. Malays. J. Med. Sci. 2020, 27, 141–195. [Google Scholar] [CrossRef]
- Simonelli, M.; Franceschi, E.; Lombardi, G. Neuro-Oncology During the COVID-19 Outbreak: A Hopeful Perspective at the End of the Italian Crisis. Front. Med. (Lausanne) 2020, 7, 594610. [Google Scholar] [CrossRef]
- Noticewala, S.S.; Ludmir, E.B.; Bishop, A.J.; Chung, C.; Ghia, A.J.; Grosshans, D.; McGovern, S.; Paulino, A.D.L.C.; Wang, C.; Woodhouse, K.D.; et al. Radiation for Glioblastoma in the Era of Coronavirus Disease 2019 (COVID-19): Patient Selection and Hypofractionation to Maximize Benefit and Minimize Risk. Adv. Radiat. Oncol. 2020, 5, 743–745. [Google Scholar] [CrossRef]
- Kamson, O.D.; Grossman, S.A. The Role of Temozolomide in Patients With Newly Diagnosed Wild-Type IDH, Unmethylated MGMTp Glioblastoma During the COVID-19 Pandemic. JAMA Oncol. 2021, 7, 675–676. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef]
- Richards, M.; Anderson, M.; Carter, P.; Ebert, B.L.; Mossialos, E. The impact of the COVID-19 pandemic on cancer care. Nat. Cancer 2020, 1, 565–567. [Google Scholar] [CrossRef]
- Ali, M.; Wani, S.U.D.; Masoodi, M.H.; Khan, N.A.; Shivakumar, H.; Osmani, R.M.A.; Khan, K.A. Global Effect of COVID-19 Pandemic on Cancer Patients and its Treatment: A Systematic Review. Clin. Complement. Med. Pharmacol. 2022, 2, 100041. [Google Scholar] [CrossRef]
- Pietruszewska, W.; Burduk, P.; Rosiak, O.; Podlawska, P.; Zakrzewski, B.; Barańska, M.; Kowalczyk, M.; Piątkowski, J.; Śmigielski, G.; Solarz, P.; et al. Impact of COVID-19 on Head and Neck Cancer Advancement Measured by Increasing Numbers of Urgent Dyspnea Cases-What Could Be Improved in the Event of Subsequent Pandemics? J. Clin. Med. 2022, 11, 6385. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, R.; Zadeh, G.; Sheehan, J.P.; Aghi, M.K. Inpatient and outpatient case prioritization for patients with neuro-oncologic disease amid the COVID-19 pandemic: General guidance for neuro-oncology practitioners from the AANS/CNS Tumor Section and Society for Neuro-Oncology. J. Neurooncol. 2020, 147, 525–529. [Google Scholar] [CrossRef] [PubMed]
- Resende, C.A.; Cruz, H.M.F.; e Silva, M.C.; Paes, R.D.; Dienstmann, R.; Barrios, C.H.; Goncalves, A.C.; Cascelli, F.G.; Souto, A.K.; Oliveira, L.C.; et al. Impact of the COVID-19 Pandemic on Cancer Staging: An Analysis of Patients With Breast Cancer From a Community Practice in Brazil. JCO Glob. Oncol. 2022, 8, e2200289. [Google Scholar] [CrossRef]
- Kuhlen, R.; Winklmair, C.; Schmithausen, D.; Schick, J.; Scriba, P. The Effects of the COVID-19 Pandemic and Lockdown on Routine Hospital Care for Other Illnesses. Dtsch. Arztebl. Int. 2020, 117, 488–489. [Google Scholar] [CrossRef]
- Norman, S.; Ramos, A.; Larsen, A.M.G.; Bander, E.; Goldberg, J.; Parker, W.; Juthani, R.G. Impact of the COVID-19 pandemic on neuro-oncology outcomes. J. Neurooncol. 2021, 154, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Mazidimoradi, A.; Hadavandsiri, F.; Momenimovahed, Z.; Salehiniya, H. Impact of the COVID-19 Pandemic on Colorectal Cancer Diagnosis and Treatment: A Systematic Review. J. Gastrointest. Cancer 2021, 1–17. [Google Scholar] [CrossRef]
- Patt, D.; Gordan, L.; Diaz, M.; Okon, T.; Grady, L.; Harmison, M.; Markward, N.; Sullivan, M.; Peng, J.; Zhou, A. Impact of COVID-19 on Cancer Care: How the Pandemic Is Delaying Cancer Diagnosis and Treatment for American Seniors. JCO Clin. Cancer Inform. 2020, 4, 1059–1071. [Google Scholar] [CrossRef] [PubMed]
- Amoo, M.; Horan, J.; Gilmartin, B.; Nolan, D.; Corr, P.; MacNally, S.; Husien, M.B.; Javadpour, M. The provision of neuro-oncology and glioma neurosurgery during the SARS-CoV-2 pandemic: A single national tertiary centre experience. Ir. J. Med. Sci. 2021, 190, 905–911. [Google Scholar] [CrossRef]
- Dannhoff, G.; Cebula, H.; Chibbaro, S.; Ganau, M.; Todeschi, J.; Mallereau, C.H.; Pottecher, J.; Proust, F.; Ollivier, I. Investigating the real impact of COVID-19 pandemic on the daily neurosurgical practice? Neurochirurgie 2021, 67, 99–103. [Google Scholar] [CrossRef]
- de Castro, D.G.; Matiello, J.; Roa, W.; Ghosh, S.; Kepka, L.; Kumar, N.; Sinaika, V.; Lomidze, D.; Hentati, D.; Rosenblatt, E.; et al. Survival Outcomes With Short-Course Radiation Therapy in Elderly Patients With Glioblastoma: Data From a Randomized Phase 3 Trial. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 931–938. [Google Scholar] [CrossRef]
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Johnson, B.A.; Waddimba, A.C.; Ogola, G.O.; Fleshman, J.W.; Preskitt, J.T. A systematic review and meta-analysis of surgery delays and survival in breast, lung and colon cancers: Implication for surgical triage during the COVID-19 pandemic. Am. J. Surg. 2021, 222, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.J.; Brennan, M.C.; Li, M.; Church, E.W.; Brandmeir, N.J.; Rakszawski, K.L.; Patel, A.S.; Rizk, E.B.; Suki, D.; Sawaya, R.; et al. Association of the Extent of Resection With Survival in Glioblastoma: A Systematic Review and Meta-analysis. JAMA Oncol. 2016, 2, 1460–1469. [Google Scholar] [CrossRef]
- Howley, F.; Lavan, A.; Connolly, E.; McMahon, G.; Mehmood, M.; Briggs, R. Trends in emergency department use by older people during the COVID-19 pandemic. Eur. Geriatr. Med. 2021, 12, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- Battisti, N.M.L.; Mislang, A.R.; Cooper, L.; O’Donovan, A.; Audisio, R.A.; Cheung, K.-L.; Sarrió, R.G.; Stauder, R.; Soto-Perez-De-Celis, E.; Jaklitsch, M.; et al. Adapting care for older cancer patients during the COVID-19 pandemic: Recommendations from the International Society of Geriatric Oncology (SIOG) COVID-19 Working Group. J. Geriatr. Oncol. 2020, 11, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.R.; Laperriere, N.; O’Callaghan, C.J.; Brandes, A.A.; Menten, J.; Phillips, C.; Fay, M.; Nishikawa, R.; Cairncross, J.G.; Roa, W.; et al. Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma. N. Engl. J. Med. 2017, 376, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- Chahal, M.; Thiessen, B.; Mariano, C. Treatment of Older Adult Patients with Glioblastoma: Moving towards the Inclusion of a Comprehensive Geriatric Assessment for Guiding Management. Curr. Oncol. 2022, 29, 360–376. [Google Scholar] [CrossRef] [PubMed]
- Zou, Y.; Zhang, J.; Zhang, T.; Feng, Y.; Xiong, Z.; Xu, C.; Gong, P.; Si, J.; Chen, J. Characteristics and operation outcomes of neuro-oncology patients after COVID-19 pandemic—A case series. Interdiscip. Neurosurg. 2021, 25, 101172. [Google Scholar] [CrossRef] [PubMed]
- Carai, A.; Locatelli, F.; Mastronuzzi, A. Delayed referral of pediatric brain tumors during COVID-19 pandemic. Neuro Oncol. 2020, 22, 1884–1886. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pre-COVID Era | COVID Era | p-Value | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Characteristic | |||||
| Number of patients | 85 | 100 | 79 | 100 | |
| Mean age (range) | 59 | (27–84) | 56 | (24–84) | 0.058 |
| Age ≥ 65 | 25 | 29.4 | 13 | 16.5 | 0.037 |
| Sex (F) | 25 | 29.4 | 28 | 35.4 | 0.255 |
| Comorbidities | 0.785 | ||||
| 0 | 31 | 36.5 | 33 | 41.8 | |
| 1 | 21 | 24.7 | 18 | 22.8 | |
| ≥2 | 33 | 38.8 | 28 | 35.4 | |
| ECOG | 0.119 | ||||
| 0 | 21 | 24.7 | 11 | 13.9 | |
| 1 | 36 | 42.4 | 42 | 53.2 | |
| ≥2 | 16 | 18.8 | 21 | 26.6 | |
| Unknown | 12 | 14.1 | 5 | 6.3 | |
| IDH mutation | 0.304 | ||||
| Yes | 2 | 2.4 | 4 | 5.1 | |
| No | 78 | 91.8 | 70 | 88.6 | |
| Unknown | 5 | 5.9 | 5 | 6.3 | |
| MGMT methylation | 0.34 | ||||
| Yes | 25 | 29.4 | 25 | 31.6 | |
| No | 27 | 31.8 | 34 | 43.0 | |
| Unknown | 33 | 38.8 | 20 | 25.3 | |
| Average mass diameter in cm | 4.1 | 4.6 | 0.078 | ||
| Pre-COVID Era | COVID Era | p-Value | |
|---|---|---|---|
| Mean | Mean | ||
| Time from symptom onset to imaging (days) | 31 | 28 | 0.751 |
| Time from imaging to surgery (days) | 13 | 13 | 0.936 |
| Time from surgery to onc consultation (weeks) | 3 | 3 | 0.768 |
| Time from surgery to RT (weeks) | 6 | 6 | 0.475 |
| Pre-COVID Era | COVID Era | ||||
|---|---|---|---|---|---|
| N | % | N | % | p-Value | |
| Extent of surgery | 0.037 | ||||
| Gross total resection | 48 | 56.5 | 29 | 36.7 | |
| Partial resection | 26 | 30.6 | 33 | 41.8 | |
| Biopsy | 11 | 12.9 | 17 | 21.5 | |
| Radiation treatment | 0.321 | ||||
| 60 Gy | 74 | 87.1 | 65 | 82.3 | |
| 40–45 Gy | 2 | 2.4 | 0 | 0.0 | |
| 25 Gy | 8 | 9.4 | 12 | 15.2 | |
| Unfinished | 1 | 1.2 | 2 | 2.5 | |
| Concurrent TMZ with RT | 0.268 | ||||
| No | 9 | 10.6 | 14 | 17.7 | |
| Yes | 71 | 83.5 | 63 | 79.7 | |
| Unfinished | 5 | 5.9 | 2 | 2.5 | |
| Adjuvant TMZ prescribed | 0.374 | ||||
| No | 28 | 32.9 | 21 | 26.6 | |
| Yes | 57 | 67.1 | 58 | 73.4 | |
| Adjuvant TMZ completed (when prescribed) | 0.304 | ||||
| No | 32 | 56.1 | 27 | 46.6 | |
| Yes | 25 | 43.9 | 31 | 53.4 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chahal, M.; Aljawi, G.; Harrison, R.; Nichol, A.; Thiessen, B. Treatment Patterns and Outcomes of Patients with Grade 4 Glioma Treated with Radiation during the COVID-19 Pandemic. Curr. Oncol. 2023, 30, 3091-3101. https://doi.org/10.3390/curroncol30030234
Chahal M, Aljawi G, Harrison R, Nichol A, Thiessen B. Treatment Patterns and Outcomes of Patients with Grade 4 Glioma Treated with Radiation during the COVID-19 Pandemic. Current Oncology. 2023; 30(3):3091-3101. https://doi.org/10.3390/curroncol30030234
Chicago/Turabian StyleChahal, Manik, Ghufran Aljawi, Rebecca Harrison, Alan Nichol, and Brian Thiessen. 2023. "Treatment Patterns and Outcomes of Patients with Grade 4 Glioma Treated with Radiation during the COVID-19 Pandemic" Current Oncology 30, no. 3: 3091-3101. https://doi.org/10.3390/curroncol30030234
APA StyleChahal, M., Aljawi, G., Harrison, R., Nichol, A., & Thiessen, B. (2023). Treatment Patterns and Outcomes of Patients with Grade 4 Glioma Treated with Radiation during the COVID-19 Pandemic. Current Oncology, 30(3), 3091-3101. https://doi.org/10.3390/curroncol30030234