Survival Benefit of Surgical Treatment for Elderly Patients with Intrahepatic Cholangiocarcinoma: A Retrospective Cohort Study in the SEER Database by Propensity Score Matching Analysis

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Study Cohort
2.2. Tumor Grade Multiple Imputation
2.3. Propensity Scores Matching Analysis
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinicopathologic Characteristics
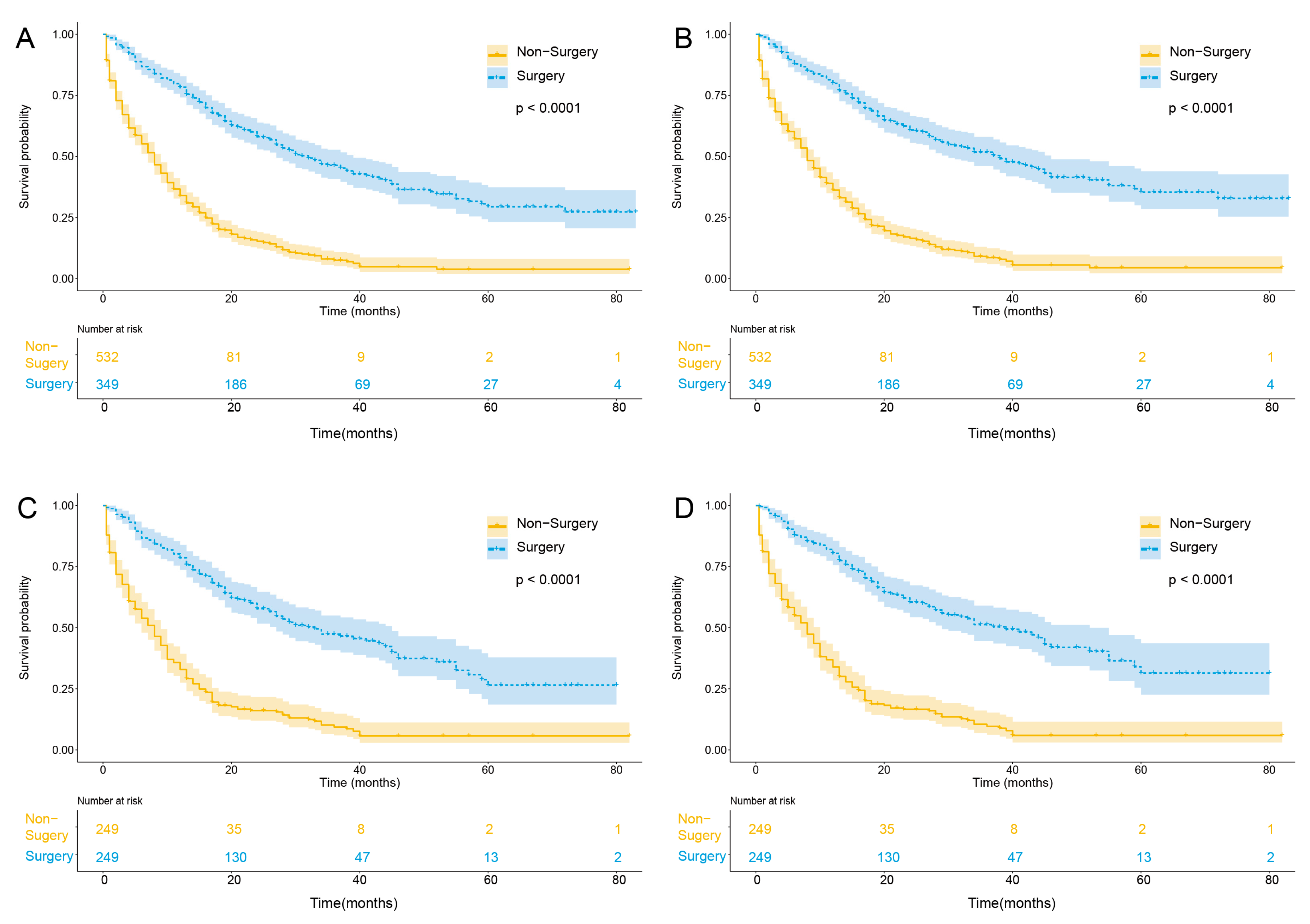
3.2. Surgery Benefit for Patients with Nonmetastatic ICC
3.3. Surgery Benefit for Patients with N0 and N1 Stage ICC
3.4. Surgery Benefit for Patients above 80 Years Old
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Florio, A.A.; Ferlay, J.; Znaor, A.; Ruggieri, D.; Alvarez, C.S.; Laversanne, M.; Bray, F.; McGlynn, K.A.; Petrick, J.L. Global trends in intrahepatic and extrahepatic cholangiocarcinoma incidence from 1993 to 2012. Cancer 2020, 126, 2666–2678. [Google Scholar] [CrossRef]
- Patel, T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology 2001, 33, 1353–1357. [Google Scholar] [CrossRef]
- Khan, S.A.; Taylor-Robinson, S.D.; Toledano, M.B.; Beck, A.; Elliott, P.; Thomas, H.C. Changing international trends in mortality rates for liver, biliary and pancreatic tumours. J. Hepatol. 2002, 37, 806–813. [Google Scholar] [CrossRef]
- McGlynn, K.A.; Tarone, R.E.; El-Serag, H.B. A comparison of trends in the incidence of hepatocellular carcinoma and intrahepatic cholangiocarcinoma in the United States. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1198–1203. [Google Scholar] [CrossRef]
- Saha, S.K.; Zhu, A.X.; Fuchs, C.S.; Brooks, G.A. Forty-Year Trends in Cholangiocarcinoma Incidence in the U.S.: Intrahepatic Disease on the Rise. Oncologist 2016, 21, 594–599. [Google Scholar] [CrossRef]
- Zhang, H.; Yang, T.; Wu, M.; Shen, F. Intrahepatic cholangiocarcinoma: Epidemiology, risk factors, diagnosis and surgical management. Cancer Lett. 2016, 379, 198–205. [Google Scholar] [CrossRef]
- Shaib, Y.H.; El-Serag, H.B.; Davila, J.A.; Morgan, R.; McGlynn, K.A. Risk factors of intrahepatic cholangiocarcinoma in the United States: A case-control study. Gastroenterology 2005, 128, 620–626. [Google Scholar] [CrossRef]
- England, K.; Azzopardi-Muscat, N. Demographic trends and public health in Europe. Eur. J. Public Health 2017, 27, 9–13. [Google Scholar] [CrossRef]
- Partridge, L.; Deelen, J.; Slagboom, P.E. Facing up to the global challenges of ageing. Nature 2018, 561, 45–56. [Google Scholar] [CrossRef]
- Tyson, G.L.; El-Serag, H.B. Risk factors for cholangiocarcinoma. Hepatology 2011, 54, 173–184. [Google Scholar] [CrossRef]
- Aljiffry, M.; Abdulelah, A.; Walsh, M.; Peltekian, K.; Alwayn, I.; Molinari, M. Evidence-based approach to cholangiocarcinoma: A systematic review of the current literature. J. Am. Coll. Surg. 2009, 208, 134–147. [Google Scholar] [CrossRef]
- Banales, J.A.-O.; Marin, J.A.-O.; Lamarca, A.A.-O.; Rodrigues, P.A.-O.; Khan, S.A.; Roberts, L.A.-O.; Cardinale, V.; Carpino, G.A.-O.; Andersen, J.A.-O.; Braconi, C.A.-O.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Sahara, K.; Wu, L.; Moris, D.; Bagante, F.; Guglielmi, A.; Aldrighetti, L.; Weiss, M.; Bauer, T.W.; Alexandrescu, S.; et al. Very Early Recurrence After Liver Resection for Intrahepatic Cholangiocarcinoma: Considering Alternative Treatment Approaches. JAMA Surg. 2020, 155, 823–831. [Google Scholar] [CrossRef]
- Toyoda, J.; Sahara, K.; Tsilimigras, D.I.; Miyake, K.; Yabushita, Y.; Homma, Y.; Kumamoto, T.; Matsuyama, R.; Pawlik, T.M. Survival Benefit of Primary Tumor Resection Among Elderly Patients with Pancreatic Neuroendocrine Tumors. World J. Surg. 2021, 45, 3643–3651. [Google Scholar] [CrossRef]
- Oishi, K.; Itamoto, T.; Kohashi, T.; Matsugu, Y.; Nakahara, H.; Kitamoto, M. Safety of hepatectomy for elderly patients with hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 15028–15036. [Google Scholar] [CrossRef]
- Notarnicola, M.; Felli, E.; Roselli, S.; Altomare, D.F.; De Fazio, M.; de’Angelis, N.; Piardi, T.; Acquafredda, S.; Ammendola, M.; Verbo, A.; et al. Laparoscopic liver resection in elderly patients: Systematic review and meta-analysis. Surg. Endosc. 2019, 33, 2763–2773. [Google Scholar] [CrossRef]
- Kishida, N.; Hibi, T.; Itano, O.; Okabayashi, K.; Shinoda, M.; Kitago, M.; Abe, Y.; Yagi, H.; Kitagawa, Y. Validation of hepatectomy for elderly patients with hepatocellular carcinoma. Ann. Surg. Oncol. 2015, 22, 3094–3101. [Google Scholar] [CrossRef]
- Kemeny, M.M.; Busch-Devereaux, E.; Merriam, L.T.; O’Hea, B.J. Cancer surgery in the elderly. Hematol./Oncol. Clin. N. Am. 2000, 14, 169–192. [Google Scholar] [CrossRef]
- Oresanya, L.B.; Lyons, W.L.; Finlayson, E. Preoperative assessment of the older patient: A narrative review. JAMA 2014, 311, 2110–2120. [Google Scholar] [CrossRef]
- Lubin, M.F. Is age a risk factor for surgery? Med. Clin. N. Am. 1993, 77, 327–333. [Google Scholar] [CrossRef]
- Mohr, D.N. Estimation of surgical risk in the elderly: A correlative review. J. Am. Geriatr. Soc. 1983, 31, 99–102. [Google Scholar] [CrossRef]
- Vitale, A.; Spolverato, G.; Bagante, F.; Gani, F.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; Sandroussi, C.; et al. A multi-institutional analysis of elderly patients undergoing a liver resection for intrahepatic cholangiocarcinoma. J. Surg. Oncol. 2016, 113, 420–426. [Google Scholar] [CrossRef]
- de la Fuente, S.G.; Bennett, K.M.; Scarborough, J.E. Functional status determines postoperative outcomes in elderly patients undergoing hepatic resections. J. Surg. Oncol. 2013, 107, 865–870. [Google Scholar] [CrossRef]
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program Website. Available online: http://www.seer.cancer.gov (accessed on 12 November 2019).
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- Clark, C.J.; Wood-Wentz, C.M.; Reid-Lombardo, K.M.; Kendrick, M.L.; Huebner, M.H.; Que, F.E. Lymphadenectomy in the staging and treatment of intrahepatic cholangiocarcinoma: A population-based study using the National Cancer Institute SEER database. HPB 2011, 13, 612–620. [Google Scholar] [CrossRef]
- Nathan, H.; Aloia, T.A.; Vauthey, J.-N.; Abdalla, E.K.; Zhu, A.X.; Schulick, R.D.; Choti, M.A.; Pawlik, T.M. A proposed staging system for intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2009, 16, 14–22. [Google Scholar] [CrossRef]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 81. [Google Scholar]
- Sekhon, J.S. Multivariate and Propensity Score Matching Software with Automated Balance Optimization: The Matching package for R. J. Stat. Softw. Forthcom. 2011, 42, 52. [Google Scholar] [CrossRef]
- El-Diwany, R.; Pawlik, T.M.; Ejaz, A. Intrahepatic Cholangiocarcinoma. Surg. Oncol. Clin. N. Am. 2019, 28, 587–599. [Google Scholar] [CrossRef]
- Squires, M.H.; Cloyd, J.M.; Dillhoff, M.; Schmidt, C.; Pawlik, T.M. Challenges of surgical management of intrahepatic cholangiocarcinoma. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 671–681. [Google Scholar] [CrossRef]
- Bartsch, F.; Baumgart, J.; Tripke, V.; Hoppe-Lotichius, M.; Heinrich, S.; Lang, H. Resection of intrahepatic cholangiocarcinoma in elderly patients—Is it reasonable? BMC Surg. 2019, 19, 157. [Google Scholar] [CrossRef]
- Shaib, Y.H.; Davila, J.A.; McGlynn, K.; El-Serag, H.B. Rising incidence of intrahepatic cholangiocarcinoma in the United States: A true increase? J. Hepatol. 2004, 40, 472–477. [Google Scholar] [CrossRef]
- Mizuguchi, T.; Kawamoto, M.; Meguro, M.; Okita, K.; Ota, S.; Ishii, M.; Ueki, T.; Nishidate, T.; Kimura, Y.; Furuhata, T.; et al. Impact of aging on morbidity and mortality after liver resection: A systematic review and meta-analysis. Surg. Today 2015, 45, 259–270. [Google Scholar] [CrossRef]
- Tufo, A.; Dunne, D.F.; Manu, N.; Lacasia, C.; Jones, L.; de Liguori Carino, N.; Malik, H.Z.; Poston, G.J.; Fenwick, S.W. Changing outlook for colorectal liver metastasis resection in the elderly. Eur. J. Surg. Oncol. 2019, 45, 635–643. [Google Scholar] [CrossRef]
- Uenishi, T.; Kubo, S.; Yamazaki, O.; Yamada, T.; Sasaki, Y.; Nagano, H.; Monden, M. Indications for surgical treatment of intrahepatic cholangiocarcinoma with lymph node metastases. J. Hepato-Biliary-Pancreat. Surg. 2008, 15, 417–422. [Google Scholar] [CrossRef]
- Zhou, R.; Lu, D.; Li, W.; Tan, W.; Zhu, S.; Chen, X.; Min, J.; Shang, C.; Chen, Y. Is lymph node dissection necessary for resectable intrahepatic cholangiocarcinoma? A systematic review and meta-analysis. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2019, 21, 784–792. [Google Scholar] [CrossRef]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef]
- Endo, I.; Gonen, M.; Yopp, A.C.; Dalal, K.M.; Zhou, Q.; Klimstra, D.; D’Angelica, M.; DeMatteo, R.P.; Fong, Y.; Schwartz, L.; et al. Intrahepatic cholangiocarcinoma: Rising frequency, improved survival, and determinants of outcome after resection. Ann. Surg. 2008, 248, 84–96. [Google Scholar] [CrossRef]
- Le Roy, B.; Gelli, M.; Pittau, G.; Allard, M.A.; Pereira, B.; Serji, B.; Vibert, E.; Castaing, D.; Adam, R.; Cherqui, D.; et al. Neoadjuvant chemotherapy for initially unresectable intrahepatic cholangiocarcinoma. Br. J. Surg. 2018, 105, 839–847. [Google Scholar] [CrossRef]
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma—Evolving concepts and therapeutic strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95–111. [Google Scholar] [CrossRef]
- Yuan, L.; Luo, X.; Lu, X.; Huang, B.; Cai, Q. Liver resection for intrahepatic cholangiocarcinoma in AJCC-stage IV: An evaluation of the survival benefit and prognostic accuracy of current AJCC staging system on N and M classification. Oncol. Rep. 2016, 36, 2663–2672. [Google Scholar] [CrossRef][Green Version]


{kind=link}
| Characteristic | Unmatched | Matched | ||||||
|---|---|---|---|---|---|---|---|---|
| ALL | Non-Surgery | Surgery | p-Value | ALL | Non-Surgery | Surgery | p-Value | |
| (n = 881) | (n = 532) | (n = 349) | (n = 498) | (n = 249) | (n = 249) | |||
| Age, years | 70.9 ± 7.52 | 71.8 ± 7.96 | 69.5 ± 6.59 | <0.001 | 70.3 (6.91) | 70.4 (7.31) | 70.1 (6.50) | 0.632 |
| Gender | 0.074 | 0.654 | ||||||
| Female | 453 (51.4) | 287 (53.9) | 166 (47.6) | 258 (51.8) | 132 (53.0) | 126 (50.6) | ||
| Male | 428 (48.6) | 245 (46.1) | 183 (52.4) | 240 (48.2) | 117 (47.0) | 123 (49.4) | ||
| Ethnicity | 0.839 | 0.912 | ||||||
| White | 706 (80.1) | 428 (80.5) | 278 (79.7) | 396 (79.5) | 197 (79.1) | 199 (79.9) | ||
| Non-white | 175 (19.9) | 104 (19.5) | 71 (20.3) | 102 (20.5) | 52 (20.9) | 50 (20.1) | ||
| Grade | <0.001 | 0.927 | ||||||
| Well-moderately | 505 (57.3) | 278 (52.3) | 227 (65.0) | 306 (61.4) | 154 (61.8) | 152 (61.0) | ||
| Poorly-undifferentially | 376 (42.7) | 254 (47.7) | 122 (35.0) | 192 (38.6) | 95 (38.2) | 97 (39.0) | ||
| TNM stage | <0.001 | 0.398 | ||||||
| IA | 133 (15.1) | 54 (10.2) | 79 (22.6) | 77 (15.5) | 31 (12.4) | 46 (18.5) | ||
| IB | 133 (15.1) | 85 (16.0) | 48 (13.8) | 70 (14.1) | 37 (14.9) | 33 (13.3) | ||
| II | 319 (36.2) | 212 (39.8) | 107 (30.7) | 182 (36.5) | 97 (39.0) | 85 (34.1) | ||
| IIIA | 14 (1.6) | 8 (1.5) | 6 (1.7) | 11 (2.2) | 6 (2.4) | 5 (2.0) | ||
| IIIB | 282 (32.0) | 173 (32.5) | 109 (31.2) | 158 (31.7) | 78 (31.3) | 80 (32.1) | ||
| Chemotherapy | 0.008 | 0.589 | ||||||
| No | 483 (54.8) | 272 (51.1) | 211 (60.5) | 273 (54.8) | 140 (56.2) | 133 (53.4) | ||
| Yes | 398 (45.2) | 260 (48.9) | 138 (39.5) | 225 (45.2) | 109 (43.8) | 116 (46.6) | ||
| Radiotherapy | 0.005 | 0.514 | ||||||
| No | 727 (82.5) | 423 (79.5) | 304 (87.1) | 430 (86.3) | 218 (87.6) | 212 (85.1) | ||
| Yes | 154 (17.5) | 109 (20.5) | 45 (12.9) | 68 (13.7) | 31 (12.4) | 37 (14.9) | ||
| Above 60 Years Old | Above 65 Years Old | Above 70 Years Old | Above 75 Years Old | |||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| OS (surgery vs. non-surgery) | ||||||||
| Unmatched | 0.237 (0.196–0.286) | <0.001 | 0.211 (0.168–0.264) | <0.001 | 0.184 (0.138–0.244) | <0.001 | 0.196 (0.137–0.280) | <0.001 |
| Matched | 0.258 (0.205–0.324) | <0.001 | 0.227 (0.172–0.298) | <0.001 | 0.233 (0.171–0.318) | <0.001 | 0.222 (0.148–0.334) | <0.001 |
| CSS (surgery vs. non-surgery) | ||||||||
| Unmatched | 0.228 (0.187–0.278) | <0.001 | 0.198 (0.156–0.251) | <0.001 | 0.206 (0.153–0.277) | <0.001 | 0.190 (0.129–0.279) | <0.001 |
| Matched | 0.239 (0.188–0.303) | <0.001 | 0.217 (0.163–0.539) | <0.001 | 0.209 (0.150–0.291) | <0.001 | 0.457 (0.251–0.832) | <0.001 |
| Above 60 Years Old | Above 65 Years Old | Above 70 Years Old | Above 75 Years Old | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 3-Year | 5-Year | 3-Year | 5-Year | 3-Year | 5-Year | 3-Year | 5-Year | |||||||||
| Estimated Rate (%) | p-Value | Estimated Rate (%) | p-Value | Estimated Rate (%) | p-Value | Estimated Rate (%) | p-Value | Estimated Rate (%) | p-Value | Estimated Rate (%) | p-Value | Estimated Rate (%) | p-Value | Estimated Rate (%) | p-Value | |
| OS | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | NA | |||||||||
| Non-surgery | 9.4 (6.0–14.8) | 5.7 (2.9–11.2) | 8.1 (4.5–14.5) | 3.0 (0.6–15.1) | 5.3 (2.1–13.3) | 2.2 (0.3–14.1) | ||||||||||
| Surgery | 47.4 (40.8–55.0) | 26.5 (18.6–37.9) | 42.8 (35.6–51.4) | 29.0 (20.7–40.8) | 43.3 (35.2–53.2) | 31.3 (22.7–43.3) | 38.4 (28.1–52.5) | 31.9 (21.3–47.9) | ||||||||
| CSS | 0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | NA | |||||||||
| Non-surgery | 9.7 (6.1–15.3) | 5.9 (3.0–11.6) | 8.5 (4.7–15.2) | 3.2 (0.6–15.9) | 5.7 (2.3–14.2) | 2.7 (0.4–17.2) | ||||||||||
| Surgery | 51.3 (44.6–59.0) | 31.4 (22.6–43.6) | 47.7 (40.3–56.3) |
33.8 (24.6–46.5) | 51.2 (42.8–61.3) | 38.6 (28.7–51.9) | 43.0 (32.2–57.4) | 38.7 (27.1–55.2) | ||||||||
| Above 60 Years Old | Above 65 Years Old | Above 70 Years Old | Above 75 Years Old | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | Univariable | Multivariable | Univariable | Multivariable | Univariable | Multivariable | |||||||||
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | |
| N0 | ||||||||||||||||
| OS (Surgery vs. non-surgery) | 0.240 (0.190–0.305) | <0.001 | 0.242 (0.192–0.307) | <0.001 | 0.209 (0.159–0.275) | <0.001 | 0.218 (0.165–0.289) | <0.001 | 0.226 (0.157–0.324) | <0.001 | 0.221 (0.153–0.320) | <0.001 | 0.197 (0.122–0.317) | <0.001 | 0.181 (0.109–0.299) | <0.001 |
| CSS (Surgery vs. non-surgery) | 0.221 (0.173–0.283) | <0.001 | 0.225 (0.116–0.289) | <0.001 | 0.186 (0.139–0.248) | <0.001 | 0.197 (0.147–0.265) | <0.001 | 0.203 (0.139–0.298) | <0.001 | 0.214 (0.145–0.315) | <0.001 | 0.186 (0.114–0.304 | <0.001 | 0.173 (0.104–0.290) | <0.001 |
| N1 | ||||||||||||||||
| OS (Surgery vs. non-surgery) | 0.597 (0.405–0.879) | 0.009 | 0.494 (0.333–0.733) | <0.001 | 0.508 (0.321–0.803) | 0.004 | 0.342 (0.211–0.554) | <0.001 | 0.399 (0.239–0.667) | <0.001 | 0.300 (0.177–0.508) | <0.001 | 0.741 (0.393–1.398) | 0.355 | ||
| CSS (Surgery vs. non-surgery) | 0.587 (0.394–0.875) | 0.009 | 0.482 (0.321–0.724) | <0.001 | 0.510 (0.315–0.824) | 0.006 | 0.357 (0.215–0.592) | <0.001 | 0.384 (0.222–0.666) | <0.001 | 0.297 (0.169–0.522) | <0.001 | 0.743 (0.374–1.478) | 0.398 | ||
| M0 | N0 | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| OS (surgery vs. non-surgery) | ||||
| Unmatched | 0.309 (0.182–0.525) | <0.001 | 0.261 (0.139–0.488) | <0.001 |
| Matched | 0.220 (0.111–0.437) | <0.001 | 0.201 (0.089–0.454) | <0.001 |
| CSS (surgery vs. non-surgery) | ||||
| Unmatched | 0.320 (0.182–0.563) | <0.001 | 0.278 (0.144–0.536) | <0.001 |
| Matched | 0.260 (0.127–0.531) | <0.001 | 0.216 (0.095–0.493) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, K.; Yu, H.; Yang, J.; Bo, Z.; Jin, C.; Wu, L.; Wang, Y.; Chen, G. Survival Benefit of Surgical Treatment for Elderly Patients with Intrahepatic Cholangiocarcinoma: A Retrospective Cohort Study in the SEER Database by Propensity Score Matching Analysis. Curr. Oncol. 2023, 30, 2642-2652. https://doi.org/10.3390/curroncol30030201
Chen K, Yu H, Yang J, Bo Z, Jin C, Wu L, Wang Y, Chen G. Survival Benefit of Surgical Treatment for Elderly Patients with Intrahepatic Cholangiocarcinoma: A Retrospective Cohort Study in the SEER Database by Propensity Score Matching Analysis. Current Oncology. 2023; 30(3):2642-2652. https://doi.org/10.3390/curroncol30030201
Chicago/Turabian StyleChen, Kaiyu, Haitao Yu, Jinhuan Yang, Zhiyuan Bo, Chen Jin, Lijun Wu, Yi Wang, and Gang Chen. 2023. "Survival Benefit of Surgical Treatment for Elderly Patients with Intrahepatic Cholangiocarcinoma: A Retrospective Cohort Study in the SEER Database by Propensity Score Matching Analysis" Current Oncology 30, no. 3: 2642-2652. https://doi.org/10.3390/curroncol30030201
APA StyleChen, K., Yu, H., Yang, J., Bo, Z., Jin, C., Wu, L., Wang, Y., & Chen, G. (2023). Survival Benefit of Surgical Treatment for Elderly Patients with Intrahepatic Cholangiocarcinoma: A Retrospective Cohort Study in the SEER Database by Propensity Score Matching Analysis. Current Oncology, 30(3), 2642-2652. https://doi.org/10.3390/curroncol30030201