Effectiveness of Immune Checkpoint Inhibitor with Anti-PD-1 Monotherapy or in Combination with Ipilimumab in Younger versus Older Adults with Advanced Melanoma

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Outcomes of Interest
2.3. Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Treatments
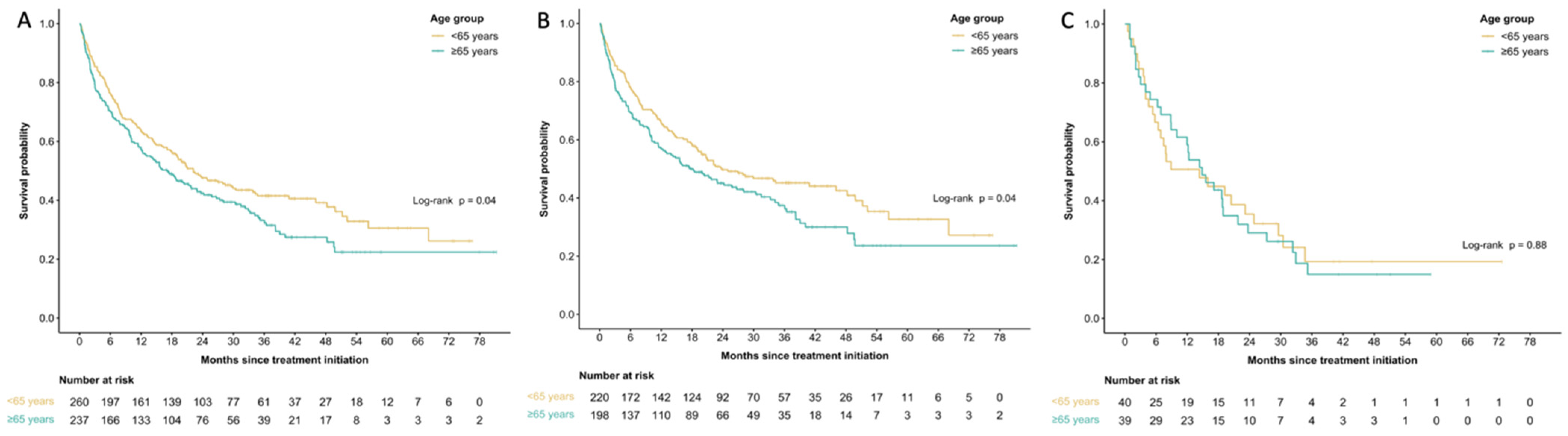
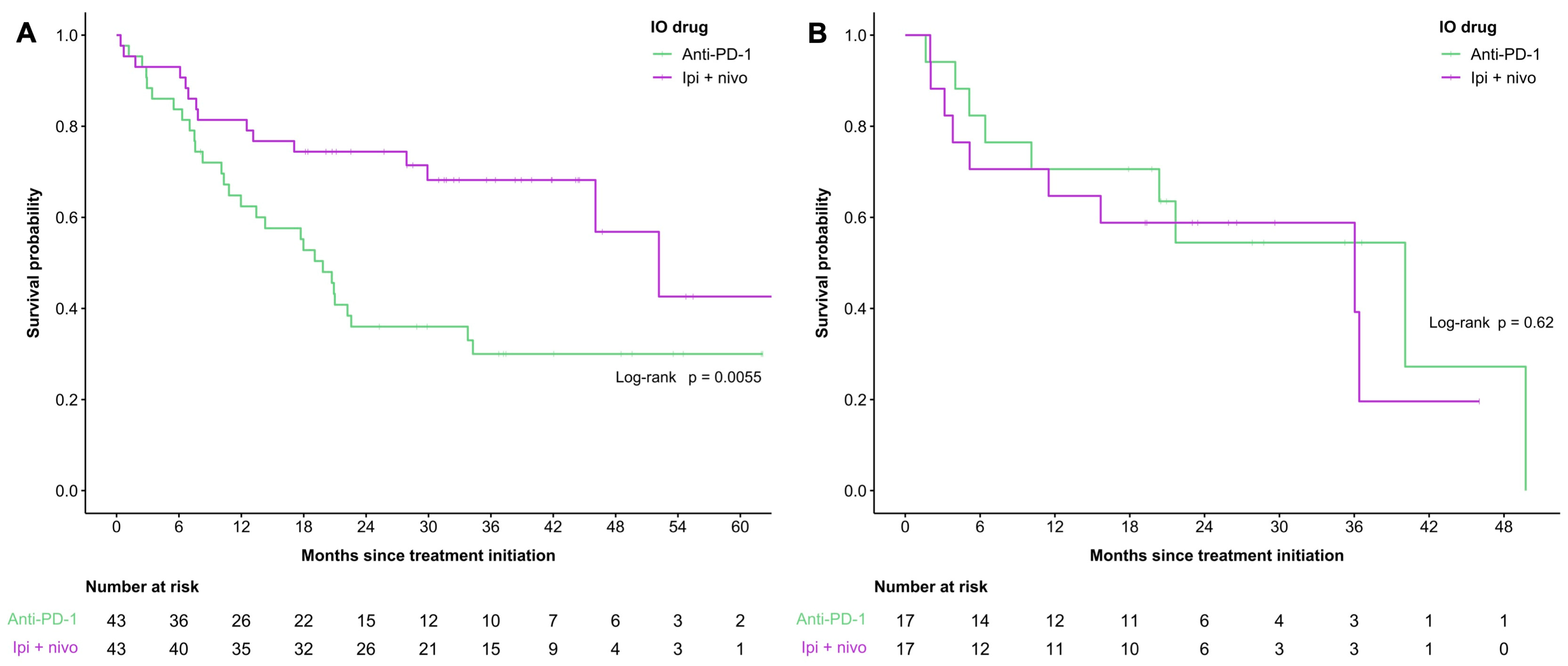
3.3. Survival
3.4. Efficacy
3.5. Analysis of Clinical Factors Associated with Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Guy, G.P.; Thomas, C.C.; Thompson, T.; Watson, M.; Massetti, G.M.; Richardson, L.C. Vital signs: Melanoma incidence and mortality trends and projections—United States, 1982–2030. Morb. Mortal. Wkly. Rep. 2015, 64, 591–596. [Google Scholar] [CrossRef]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Barsouk, A. Epidemiology of Melanoma. Med. Sci. 2021, 9, 63. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Long-Term Outcomes with Nivolumab Plus Ipilimumab or Nivolumab Alone Versus Ipilimumab in Patients with Advanced Melanoma. J. Clin. Oncol. 2022, 40, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef]
- Elias, R.; Giobbie-Hurder, A.; McCleary, N.J.; Ott, P.; Hodi, F.S.; Rahma, O. Efficacy of PD-1 & PD-L1 inhibitors in older adults: A meta-analysis. J. Immunother. Cancer 2018, 6, 26. [Google Scholar] [PubMed]
- Bhandari, S.; Gill, A.S.; Perez, C.A.; Jain, D. Management of immunotherapy toxicities in older adults. Semin. Oncol. 2018, 45, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Joshi, K.P.; Atwal, D.; Ravilla, R.; Tao, J.; Su, J.; Makhoul, I.; Hutchins, L.F.; Mahmoud, F.A. Outcomes of immunotherapy in advanced melanoma in relation to age. J. Clin. Oncol. 2018, 36, 187. [Google Scholar] [CrossRef]
- Elder, D.E.; Bastian, B.C.; Cree, I.A.; Massi, D.; Scolyer, R.A. The 2018 World Health Organization classification of cutaneous, mucosal, and uveal melanoma detailed analysis of 9 distinct subtypes defined by their evolutionary pathway. Arch. Pathol. Lab. Med. 2020, 144, 500–522. [Google Scholar] [CrossRef]
- Li, P.; Yang, X.; Feng, Y.; Wu, L.; Ma, W.; Ding, G.; Wei, Y.; Sun, L. The impact of immunosenescence on the efficacy of immune checkpoint inhibitors in melanoma patients: A meta-analysis. Onco Targets Ther. 2018, 11, 7521–7527. [Google Scholar] [CrossRef] [PubMed]
- Ben-Betzalel, G.; Steinberg-Silman, Y.; Stoff, R.; Asher, N.; Shapira-Frommer, R.; Schachter, J.; Markel, G. Immunotherapy comes of age in octagenarian and nonagenarian metastatic melanoma patients. Eur. J. Cancer. 2019, 108, 61–68. [Google Scholar] [CrossRef]
- Nishijima, T.F.; Muss, H.B.; Shachar, S.S.; Moschos, S.J. Comparison of efficacy of immune checkpoint inhibitors (ICIs) between younger and older patients: A systematic review and meta-analysis. Cancer Treat. Rev. 2016, 45, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Kugel, C.H.; Douglass, S.M.; Webster, M.R.; Kaur, A.; Liu, Q.; Yin, X.; Weiss, S.A.; Darvishian, F.; Al-Rohil, R.N.; Ndoye, A.; et al. Age correlates with response to anti-PD1, reflecting age-related differences in intratumoral effector and regulatory T-cell populations. Clin. Cancer Res. 2018, 24, 5347–5356. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Cham, Switzerland, 2017. [Google Scholar]
- Balch, C.M.; Soong, S.J.; Gershenwald, J.E.; Thompson, J.F.; Coit, D.G.; Atkins, M.B.; Ding, S.; Cochran, A.J.; Eggermont, A.M.; Flaherty, K.T.; et al. Age as a Prognostic Factor in Patients with Localized Melanoma and Regional Metastases Data Management and Analysis Seng-jaw. Ann. Surg. Oncol. 2013, 20, 3961–3968. [Google Scholar] [CrossRef]
- Lasithiotakis, K.; Leiter, U.; Meier, F.; Eigentler, T.; Metzler, G.; Moehrle, M.; Breuninger, H.; Garbe, C. Age and gender are significant independent predictors of survival in primary cutaneous melanoma. Cancer 2008, 112, 1795–1804. [Google Scholar] [CrossRef]
- Macdonald, J.B.; Dueck, A.C.; Gray, R.J.; Wasif, N.; Swanson, D.L.; Sekulic, A.; Pockaj, B.A. Malignant melanoma in the elderly: Different regional disease and poorer prognosis. J. Cancer 2011, 2, 538–543. [Google Scholar] [CrossRef]
- Pollack, L.A.; Li, J.; Berkowitz, Z.; Weir, H.K.; Wu, X.-C.; Ajani, U.A.; Ekwueme, D.U.; Li, C.; Pollack, B.P. Melanoma survival in the United States, 1992 to 2005. J. Am. Acad. Dermatol. 2011, 65, S78.e1–S78.e10. [Google Scholar] [CrossRef] [PubMed]
- Strudel, M.; Festino, L.; Vanella, V.; Beretta, M.; Marincola, F.M.; Ascierto, P.A. Melanoma: Prognostic Factors and Factors Predictive of Response to Therapy. Curr. Med. Chem. 2020, 27, 2792–2813. [Google Scholar] [CrossRef]
- Hayward, N.K.; Wilmott, J.S.; Waddell, N.; Johansson, P.A.; Field, M.A.; Nones, K.; Patch, A.-M.; Kakavand, H.; Alexandrov, L.B.; Burke, H.; et al. Whole-genome landscapes of major melanoma subtypes. Nature 2017, 545, 175–180. [Google Scholar] [CrossRef]
- McGranahan, N.; Furness, A.J.; Rosenthal, R.; Ramskov, S.; Lyngaa, R.; Saini, S.K.; Jamal-Hanjani, M.; Wilson, G.A.; Birkbak, N.J.; Hiley, C.T.; et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 2016, 351, 1463–1469. [Google Scholar] [CrossRef]
- Lim, S.J.; Kim, J.M.; Lee, W.S.; Kwon, W.S.; Kim, T.S.; Park, K.H.; Chung, H.C.; Rha, S.Y. Abstract 4055: Immune checkpoint protein expression is up-regulated in tumor-bearing elderly mice. Cancer Res. 2015, 75, 4055. [Google Scholar] [CrossRef]
- Kaunitz, G.J.; Cottrell, T.R.; Lilo, M.; Muthappan, V.; Esandrio, J.; Berry, S.; Xu, H.; Ogurtsova, A.; Anders, R.A.; Fischer, A.H.; et al. Melanoma subtypes demonstrate distinct PD-L1 expression profiles. Lab. Investig. 2017, 97, 1063–1071. [Google Scholar] [CrossRef]
- Betof, A.S.; Nipp, R.D.; Giobbie-Hurder, A.; Johnpulle, R.A.N.; Rubin, K.; Rubinstein, S.M.; Flaherty, K.T.; Lawrence, D.P.; Johnson, D.B.; Sullivan, R.J. Impact of Age on Outcomes with Immunotherapy for Patients with Melanoma. Oncologist 2017, 22, 963–971. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Mezquita, L.; Auclin, E.; Ferrara, R.; Charrier, M.; Remon, J.; Planchard, D.; Ponce, S.; Ares, L.P.; Leroy, L.; Audigier-Valette, C.; et al. Association of the Lung Immune Prognostic Index with Immune Checkpoint Inhibitor Outcomes in Patients with Advanced Non-Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Meyers, D.E.; Stukalin, I.; Vallerand, I.A.; Lewinson, R.T.; Suo, A.; Dean, M.; North, S.; Pabani, A.; Cheng, T.; Heng, D.Y.; et al. The lung immune prognostic index discriminates survival outcomes in patients with solid tumors treated with immune checkpoint inhibitors. Cancers 2019, 11, 1713. [Google Scholar] [CrossRef]
- Sehgal, K.; Gill, R.R.; Widick, P.; Bindal, P.; McDonald, D.C.; Shea, M.; Rangachari, D.; Costa, D.B. Association of Performance Status with Survival in Patients with Advanced Non-Small Cell Lung Cancer Treated with Pembrolizumab Monotherapy. JAMA Netw. Open. 2021, 4, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Gan, C.L.; Stukalin, I.; Meyers, D.E.; Dudani, S.; Grosjean, H.A.; Dolter, S.; Ewanchuk, B.W.; Goutam, S.; Sander, M.; Wells, C.; et al. Outcomes of patients with solid tumour malignancies treated with first-line immuno-oncology agents who do not meet eligibility criteria for clinical trials. Eur. J. Cancer 2021, 151, 115–125. [Google Scholar] [CrossRef]
- Botticelli, A.; Cirillo, A.; Scagnoli, S.; Cerbelli, B.; Strigari, L.; Cortellini, A.; Pizzuti, L.; Vici, P.; De Galitiis, F.; Di Pietro, F.R.; et al. The agnostic role of site of metastasis in predicting outcomes in cancer patients treated with immunotherapy. Vaccines 2020, 8, 203. [Google Scholar] [CrossRef]
- Tumeh, P.C.; Hellmann, M.D.; Hamid, O.; Tsai, K.K.; Loo, K.L.; Gubens, M.A.; Rosenblum, M.; Harview, C.L.; Taube, J.M.; Handley, N.; et al. Liver Metastasis and Treatment Outcome with Anti-PD-1 Monoclonal Antibody in Patients with Melanoma and NSCLC. Cancer Immunol. Res. 2017, 5, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: Implications for melanoma treatment and care. Expert. Rev. Anticancer. Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef]
- Perier-Muzet, M.; Gatt, E.; Péron, J.; Falandry, C.; Amini-Adlé, M.; Thomas, L.; Dalle, S.; Boespflug, A. Association of immunotherapy with overall survival in elderly patients with melanoma. JAMA Dermatol. 2018, 154, 82–87. [Google Scholar] [CrossRef]
- Bastholt, L.; Schmidt, H.; Bjerregaard, J.K.; Herrstedt, J.; Svane, I.M. Age favoured overall survival in a large population-based Danish patient cohort treated with anti-PD1 immune checkpoint inhibitor for metastatic melanoma. Eur. J. Cancer 2019, 119, 122–131. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | N | Overall, N = 497 | Age at Treatment Initiation, Years | p-Value | |
|---|---|---|---|---|---|
| <65, N = 260 | ≥65, N = 237 | ||||
| Sex | 497 | 0.11 | |||
| Female | 173 (34.8%) | 99 (38.1%) | 74 (31.2%) | ||
| Male | 324 (65.2%) | 161 (61.9%) | 163 (68.8%) | ||
| ECOG status | 496 | 0.11 | |||
| <2 | 429 (86.5%) | 231 (88.8%) | 198 (83.9%) | ||
| ≥2 | 67 (13.5%) | 29 (11.2%) | 38 (16.1%) | ||
| Melanoma type | 497 | 0.74 | |||
| Cutaneous | 418 (84.1%) | 220 (84.6%) | 198 (83.5%) | ||
| Non-cutaneous | 79 (15.9%) | 40 (15.4%) | 39 (16.5%) | ||
| BRAF mutation | 415 | 0.001 | |||
| No | 264 (63.6%) | 123 (56.2%) | 141 (71.9%) | ||
| Yes | 151 (36.4%) | 96 (43.8%) | 55 (28.1%) | ||
| LDH | 404 | 0.99 | |||
| Normal | 273 (67.6%) | 144 (67.6%) | 129 (67.5%) | ||
| Elevated >ULN | 131 (32.4%) | 69 (32.4%) | 62 (32.5%) | ||
| dNLR | 477 | 0.09 | |||
| ≤3 | 385 (80.7%) | 210 (83.7%) | 175 (77.4%) | ||
| >3 | 92 (19.3%) | 41 (16.3%) | 51 (22.6%) | ||
| Number of organ sites with metastasis | 497 | 0.98 | |||
| <3 | 331 (66.6%) | 173 (66.5%) | 158 (66.7%) | ||
| ≥3 | 166 (33.4%) | 87 (33.5%) | 79 (33.3%) | ||
| M stage | 497 | 0.71 | |||
| 1a/1b | 241 (48.5%) | 124 (47.7%) | 117 (49.4%) | ||
| 1c/1d | 256 (51.5%) | 136 (52.3%) | 120 (50.6%) | ||
| Autoimmune condition | 496 | 0.13 | |||
| No | 438 (88.3%) | 235 (90.4%) | 203 (86.0%) | ||
| Yes | 58 (11.7%) | 25 (9.6%) | 33 (14.0%) | ||
| IO drug | 492 | <0.001 | |||
| Anti-PD-1 * | 368 (74.8%) | 156 (60.9%) | 212 (89.8%) | ||
| Ipilimumab + nivolumab | 124 (25.2%) | 100 (39.1%) | 24 (10.2%) | ||
| Treatment line | 497 | 0.007 | |||
| First | 351 (70.6%) | 170 (65.4%) | 181 (76.4%) | ||
| Other | 146 (29.4%) | 90 (34.6%) | 56 (23.6%) | ||
| Characteristic | Univariate Cox Regression Model | Multivariate Cox Regression Model | ||||||
|---|---|---|---|---|---|---|---|---|
| Age < 65 Years | Age ≥ 65 Years | Age < 65 Years | Age ≥ 65 Years | |||||
| OS HR (95% CI) | p-Value | OS HR (95% CI) | p-Value | OS HR (95% CI) | p-Value | OS HR (95% CI) | p-Value | |
| Sex | ||||||||
| Female (reference) vs. Male | 1.18 (0.82–1.70) | 0.38 | 0.96 (0.64–1.42) | 0.83 | 1.36 (0.90–2.07) | 0.15 | 0.93 (0.59–1.48) | 0.77 |
| dNLR | ||||||||
| ≤3 (reference) vs. >3 | 2.50 (1.61–3.87) | <0.001 | 1.80 (1.20–2.70) | 0.005 | 1.88 (1.12–3.18) | 0.02 | 1.35 (0.83–2.18) | 0.23 |
| LDH | ||||||||
| Normal (reference) vs. Elevated | 2.22 (1.49–3.30) | <0.001 | 2.38 (1.59–3.55) | <0.001 | 2.00 (1.31–3.06) | 0.001 | 2.09 (1.37–3.18) | <0.001 |
| ECOG status | ||||||||
| <2 (reference) vs. ≥2 | 2.30 (1.39–3.80) | 0.001 | 3.05 (1.95–4.75) | <0.001 | 1.30 (0.69–2.44) | 0.42 | 2.86 (1.61–5.08) | <0.001 |
| M stage | ||||||||
| 1a/1b (reference) vs. 1c/1d | 2.31 (1.61–3.32) | <0.001 | 1.51 (1.06–2.15) | 0.02 | 1.53 (1.00–2.36) | 0.05 | 1.24 (0.80–1.92) | 0.34 |
| BRAF mutation | ||||||||
| No (reference) vs. Yes | 1.35 (0.93–1.96) | 0.12 | 1.10 (0.73–1.65) | 0.66 | ||||
| IO drug | ||||||||
| Anti-PD-1 (reference) vs. Ipilimumab + nivolumab | 0.47 (0.32–0.71) | <0.001 | 0.68 (0.36–1.31) | 0.25 | 0.51 (0.30–0.87) | 0.01 | 1.35 (0.66–2.75) | 0.41 |
| Treatment line | ||||||||
| First (reference) vs. Other | 2.49 (1.74–3.56) | <0.001 | 1.68 (1.15–2.45) | 0.007 | 1.73 (1.08–2.78) | 0.02 | 1.84 (1.14–2.99) | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woo, T.E.; Stukalin, I.; Ding, P.Q.; Goutam, S.; Sander, M.; Ewanchuk, B.; Cheung, W.Y.; Heng, D.Y.C.; Cheng, T. Effectiveness of Immune Checkpoint Inhibitor with Anti-PD-1 Monotherapy or in Combination with Ipilimumab in Younger versus Older Adults with Advanced Melanoma. Curr. Oncol. 2023, 30, 8936-8947. https://doi.org/10.3390/curroncol30100646
Woo TE, Stukalin I, Ding PQ, Goutam S, Sander M, Ewanchuk B, Cheung WY, Heng DYC, Cheng T. Effectiveness of Immune Checkpoint Inhibitor with Anti-PD-1 Monotherapy or in Combination with Ipilimumab in Younger versus Older Adults with Advanced Melanoma. Current Oncology. 2023; 30(10):8936-8947. https://doi.org/10.3390/curroncol30100646
Chicago/Turabian StyleWoo, Taylor E., Igor Stukalin, Philip Q. Ding, Siddhartha Goutam, Michael Sander, Benjamin Ewanchuk, Winson Y. Cheung, Daniel Y. C. Heng, and Tina Cheng. 2023. "Effectiveness of Immune Checkpoint Inhibitor with Anti-PD-1 Monotherapy or in Combination with Ipilimumab in Younger versus Older Adults with Advanced Melanoma" Current Oncology 30, no. 10: 8936-8947. https://doi.org/10.3390/curroncol30100646
APA StyleWoo, T. E., Stukalin, I., Ding, P. Q., Goutam, S., Sander, M., Ewanchuk, B., Cheung, W. Y., Heng, D. Y. C., & Cheng, T. (2023). Effectiveness of Immune Checkpoint Inhibitor with Anti-PD-1 Monotherapy or in Combination with Ipilimumab in Younger versus Older Adults with Advanced Melanoma. Current Oncology, 30(10), 8936-8947. https://doi.org/10.3390/curroncol30100646