Regional Chemotherapy Is a Valuable Second-Line Approach in Metastatic Esophageal Cancer after Failure to First-Line Palliative Treatment


Abstract
:1. Introduction
2. Patients and Methods
2.1. Characterization of the Study Population
2.2. Cytotoxic Drugs and Methods
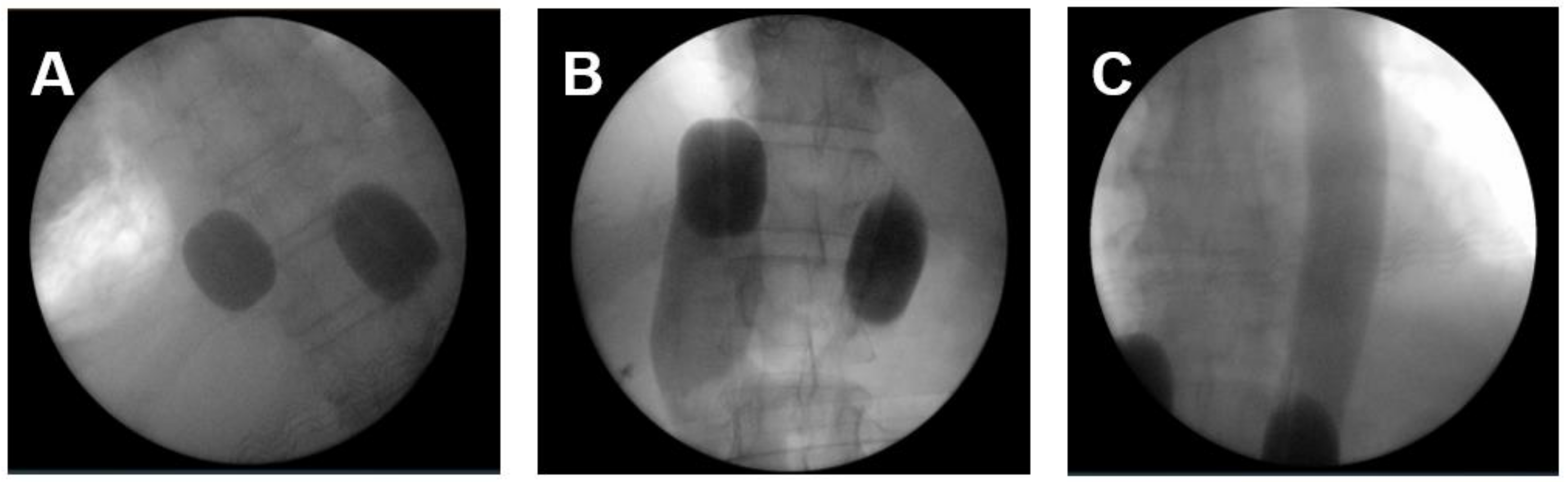
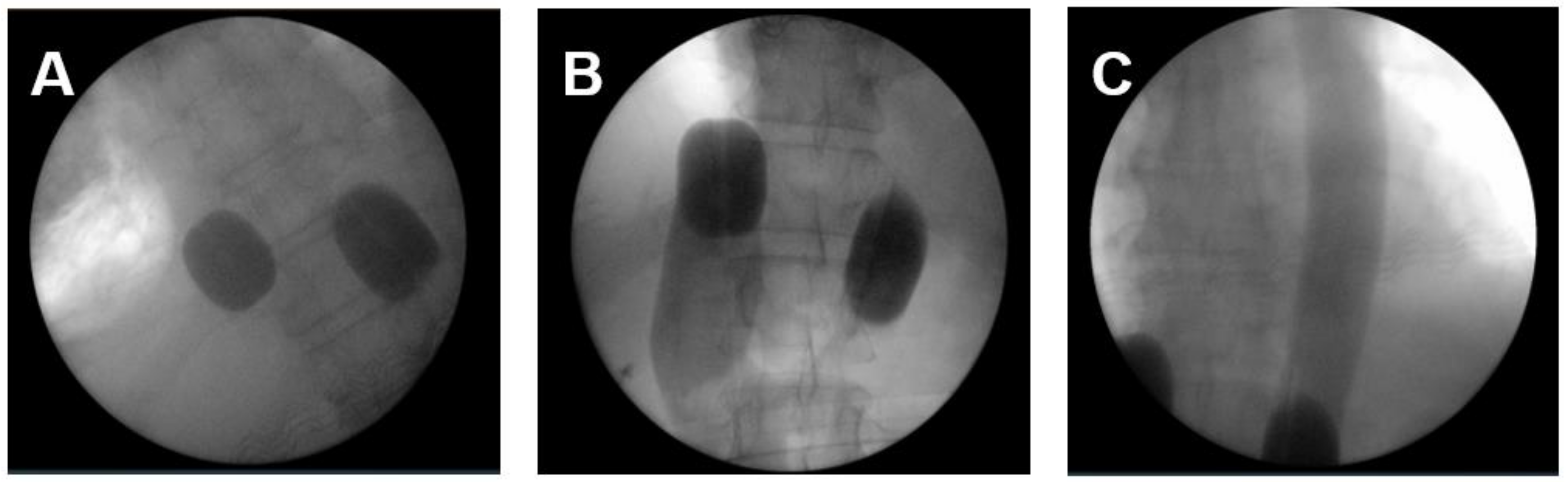
2.2.1. Regional Chemotherapy Techniques
2.2.2. Cytotoxic Drugs
2.2.3. Treatment Cycles
2.3. Statistical Analysis
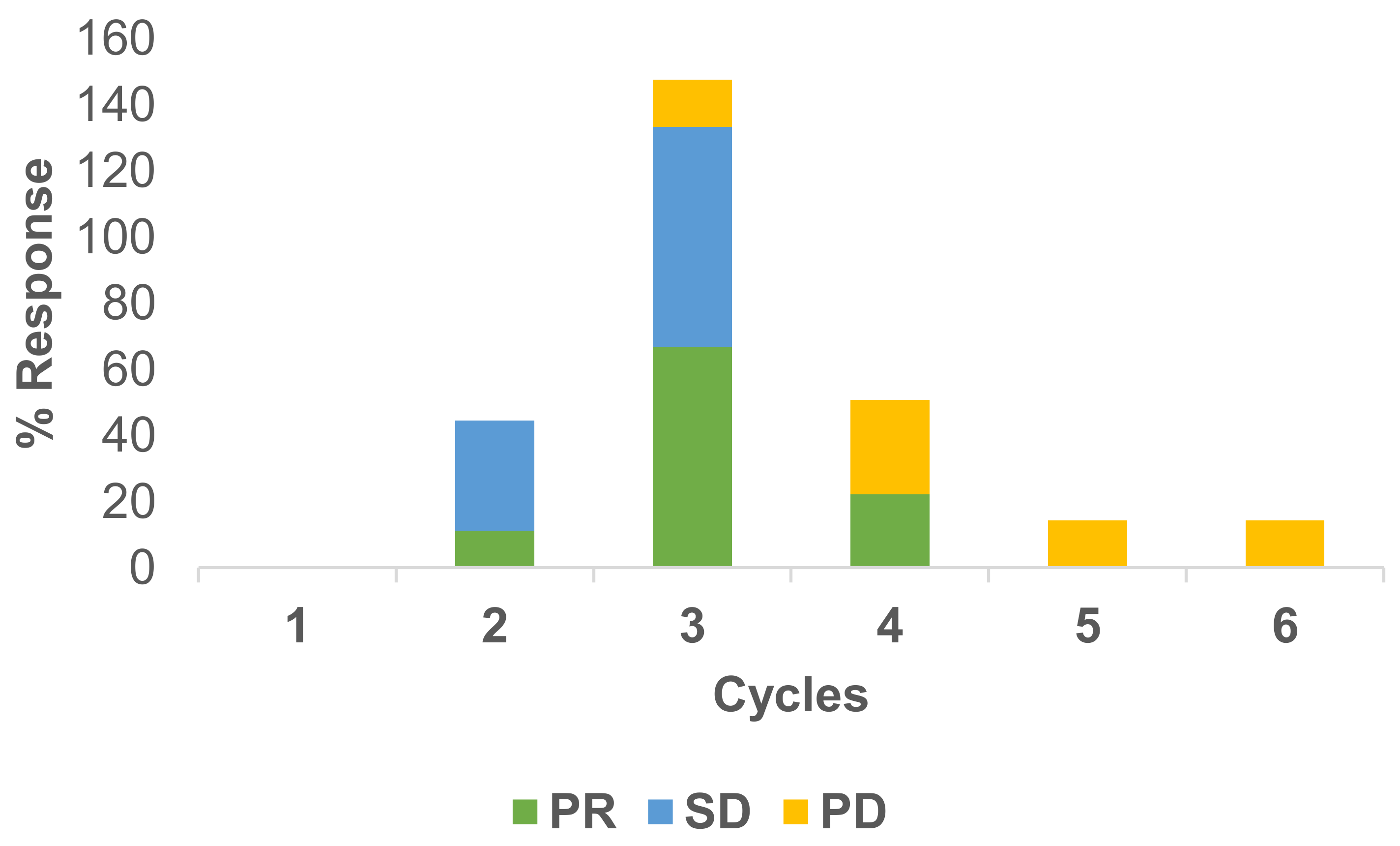
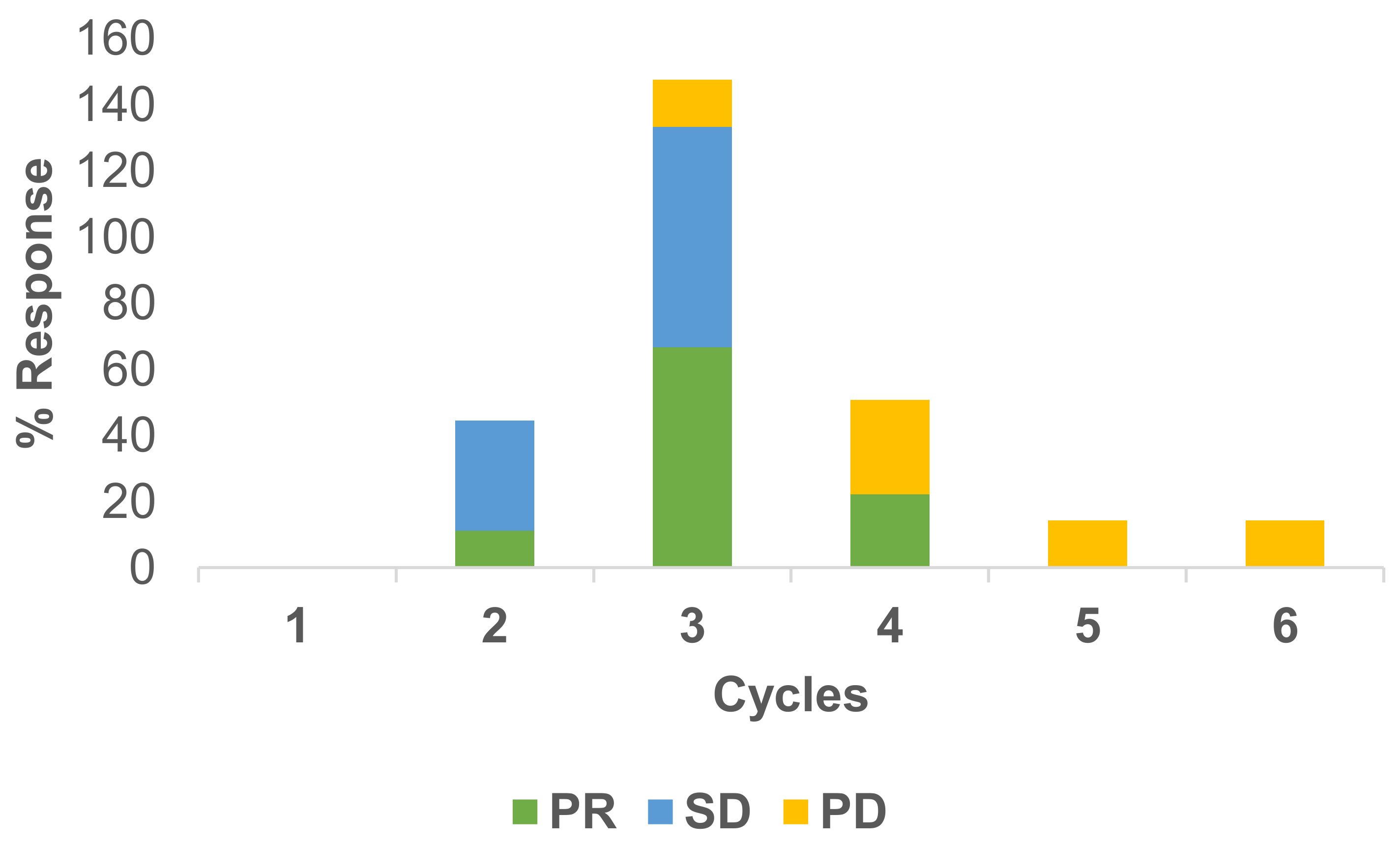
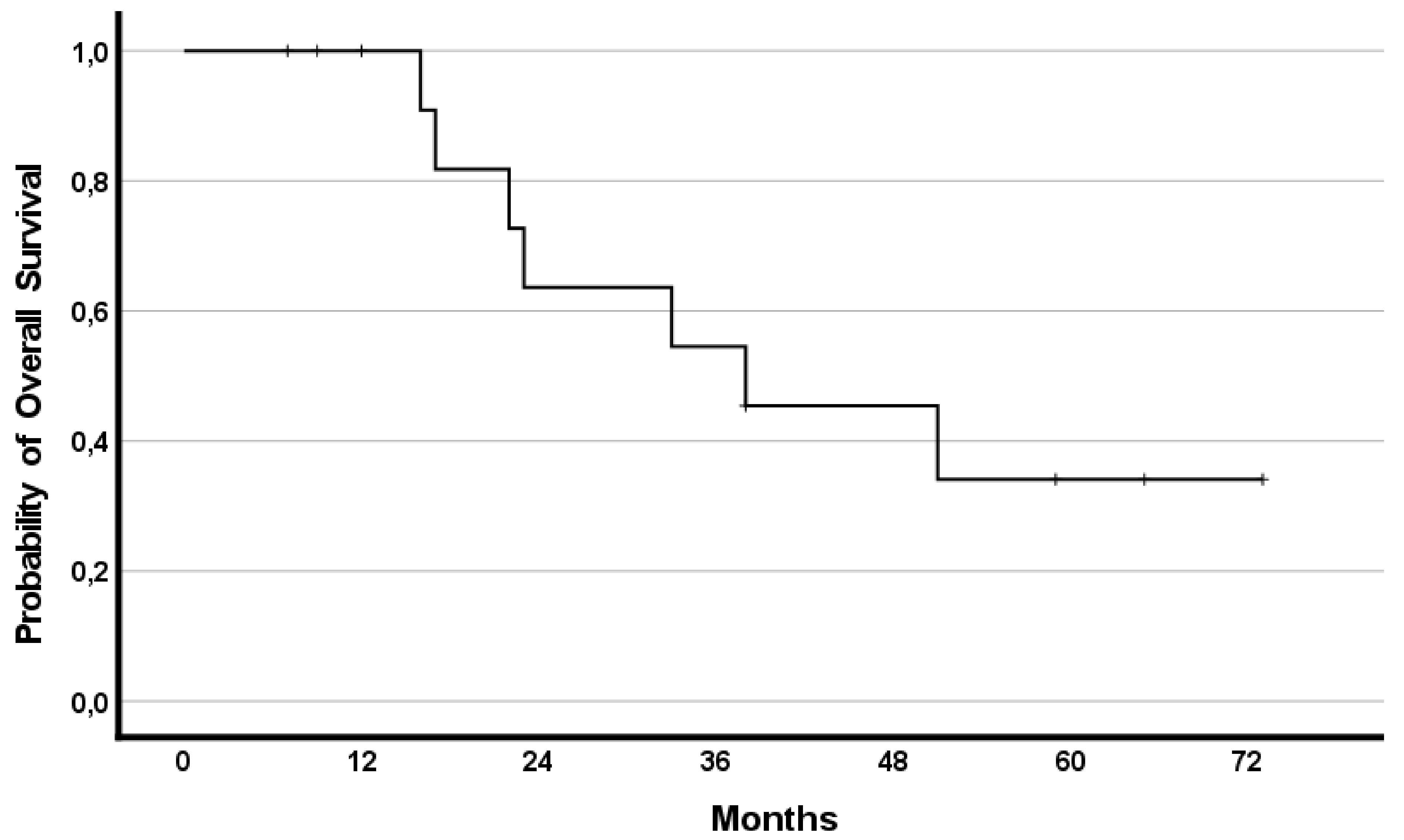
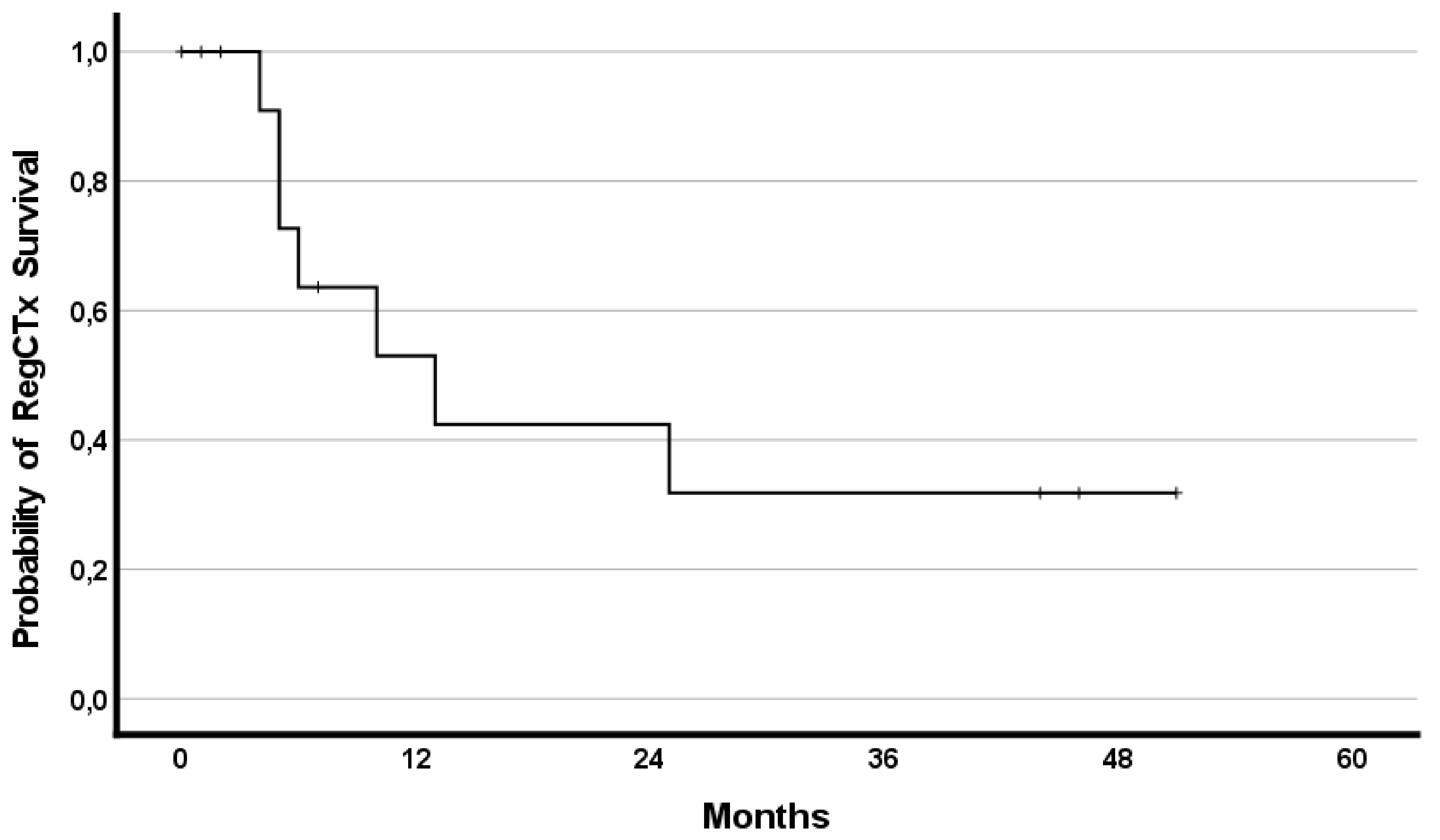
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamangar, F.; Nasrollahzadeh, D.; Safiri, S.; Sepanlou, S.G.; Fitzmaurice, C.; Ikuta, K.S.; Bisignano, C.; Islami, F.; Roshandel, G.; Lim, S.S.; et al. The global, regional, and national burden of oesophageal cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 582–597. [Google Scholar] [CrossRef]
- Corona, E.; Yang, L.; Esrailian, E.; Ghassemi, K.A.; Conklin, J.L.; May, F.P. Trends in Esophageal Cancer Mortality and Stage at Diagnosis by Race and Ethnicity in the United States. Cancer Causes Control 2021, 32, 883–894. [Google Scholar] [CrossRef]
- Ikeda, G.; Yamamoto, S.; Kato, K. The safety of current treatment options for advanced esophageal cancer after first-line chemotherapy. Expert Opin. Drug Saf. 2022, 21, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Rustgi, A.K.; El-Serag, H.B. Esophageal carcinoma. N. Engl. J. Med. 2014, 371, 2499–2509. [Google Scholar] [CrossRef]
- Porschen, R.; Fischbach, W.; Gockel, I.; Hollerbach, S.; Holscher, A.; Jansen, P.L.; Miehlke, S.; Pech, O.; Stahl, M.; Thuss-Patience, P.; et al. S3-Leitlinie—Diagnostik und Therapie der Plattenepithelkarzinome und Adenokarzinome des Ösophagus. Z Gastroenterol. 2019, 57, 336–418. [Google Scholar] [CrossRef] [Green Version]
- Lordick, F.; Mariette, C.; Haustermans, K.; Obermannova, R.; Arnold, D.; Committee, E.G. Oesophageal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v50–v57. [Google Scholar] [CrossRef]
- Muro, K.; Lordick, F.; Tsushima, T.; Pentheroudakis, G.; Baba, E.; Lu, Z.; Cho, B.C.; Nor, I.M.; Ng, M.; Chen, L.T.; et al. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic oesophageal cancer: A JSMO-ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann. Oncol. 2019, 30, 34–43. [Google Scholar] [CrossRef]
- Kojima, T.; Shah, M.A.; Muro, K.; Francois, E.; Adenis, A.; Hsu, C.H.; Doi, T.; Moriwaki, T.; Kim, S.B.; Lee, S.H.; et al. Randomized Phase III KEYNOTE-181 Study of Pembrolizumab Versus Chemotherapy in Advanced Esophageal Cancer. J. Clin. Oncol. 2020, 38, 4138–4148. [Google Scholar] [CrossRef]
- Kato, K.; Cho, B.C.; Takahashi, M.; Okada, M.; Lin, C.Y.; Chin, K.; Kadowaki, S.; Ahn, M.J.; Hamamoto, Y.; Doki, Y.; et al. Nivolumab versus chemotherapy in patients with advanced oesophageal squamous cell carcinoma refractory or intolerant to previous chemotherapy (ATTRACTION-3): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 1506–1517. [Google Scholar] [CrossRef]
- Shitara, K.; Ozguroglu, M.; Bang, Y.J.; Di Bartolomeo, M.; Mandala, M.; Ryu, M.H.; Fornaro, L.; Olesinski, T.; Caglevic, C.; Chung, H.C.; et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): A randomised, open-label, controlled, phase 3 trial. Lancet 2018, 392, 123–133. [Google Scholar] [CrossRef]
- Aigner, K.R.; Gailhofer, S.; Selak, E.; Aigner, K. Intra-arterial infusion chemotherapy versus isolated upper abdominal perfusion for advanced pancreatic cancer: A retrospective cohort study on 454 patients. J. Cancer Res. Clin. Oncol. 2019, 145, 2855–2862. [Google Scholar] [CrossRef] [Green Version]
- Guadagni, S.; Clementi, M.; Valenti, M.; Fiorentini, G.; Cantore, M.; Kanavos, E.; Caterino, G.P.; Di Giuro, G.; Amicucci, G. Hypoxic abdominal stop-flow perfusion in the treatment of advanced pancreatic cancer: A phase II evaluation/trial. Eur. J. Surg. Oncol. 2007, 33, 72–78. [Google Scholar] [CrossRef]
- Aigner, K.; Vashist, Y.K.; Selak, E.; Gailhofer, S.; Aigner, K.R. Efficacy of Regional Chemotherapy Approach in Peritoneal Metastatic Gastric Cancer. J. Clin. Med. 2021, 10, 5322. [Google Scholar] [CrossRef]
- Laface, C.; Laforgia, M.; Molinari, P.; Foti, C.; Ambrogio, F.; Gadaleta, C.D.; Ranieri, G. Intra-Arterial Infusion Chemotherapy in Advanced Pancreatic Cancer: A Comprehensive Review. Cancers 2022, 14, 450. [Google Scholar] [CrossRef]
- Veelken, R.; Maiwald, B.; Strocka, S.; Petersen, T.O.; Moche, M.; Ebel, S.; Denecke, T.; Rehak, M.; Struck, M.F.; Forstmeyer, D.; et al. Repeated percutaneous hepatic perfusion with melphalan can maintain long-term response in patients with liver cancers. Cardiovasc. Interv. Radiol. 2022, 45, 218–222. [Google Scholar] [CrossRef]
- Aigner, K.R. Intra-arterial infusion: Overview and novel approaches. Semin. Surg. Oncol. 1998, 14, 248–253. [Google Scholar] [CrossRef]
- Aigner, K.R.; Selak, E.; Aigner, K. Short-term intra-arterial infusion chemotherapy for head and neck cancer patients maintaining quality of life. J. Cancer Res. Clin. Oncol. 2019, 145, 261–268. [Google Scholar] [CrossRef] [Green Version]
- Guadagni, S.; Aigner, K.; Zoras, O.; Masedu, F.; Fiorentini, G.; Ricevuto, E.; Deraco, M.; Clementi, M. Isolated thoracic perfusion in lung metastases from breast cancer: A retrospective observational study. Updates Surg. 2019, 71, 165–177. [Google Scholar] [CrossRef]
- Aigner, K.R.; Selak, E.; Gailhofer, S. Isolated thoracic perfusion with chemofiltration for progressive malignant pleural mesothelioma. Onco. Targets Ther. 2017, 10, 3049–3057. [Google Scholar] [CrossRef] [Green Version]
- Teicher, B.A.; Lazo, J.S.; Sartorelli, A.C. Classification of antineoplastic agents by their selective toxicities toward oxygenated and hypoxic tumor cells. Cancer Res. 1981, 41, 73–81. [Google Scholar] [PubMed]
- Aigner, K.R.; Knapp, N. Toxicity Profiles with Systemic versus Regional Chemotherapy, 2nd ed.; Stephens, F.O., Ed.; Springer: Berlin/Heidelberg, Germany, 2016; p. 506. [Google Scholar]
- Bolger, J.C.; Donohoe, C.L.; Lowery, M.; Reynolds, J.V. Advances in the curative management of oesophageal cancer. Br. J. Cancer 2022, 126, 706–717. [Google Scholar] [CrossRef] [PubMed]
- Van Rossum, P.S.N.; Mohammad, N.H.; Vleggaar, F.P.; van Hillegersberg, R. Treatment for unresectable or metastatic oesophageal cancer: Current evidence and trends. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 235–249. [Google Scholar] [CrossRef] [PubMed]
- Ku, G.Y. Systemic therapy for esophageal cancer: Chemotherapy. Chin. Clin. Oncol. 2017, 6, 49. [Google Scholar] [CrossRef]
- Bleiberg, H.; Conroy, T.; Paillot, B.; Lacave, A.J.; Blijham, G.; Jacob, J.H.; Bedenne, L.; Namer, M.; De Besi, P.; Gay, F.; et al. Randomised phase II study of cisplatin and 5-fluorouracil (5-FU) versus cisplatin alone in advanced squamous cell oesophageal cancer. Eur. J. Cancer 1997, 33, 1216–1220. [Google Scholar] [CrossRef]
- Hiramoto, S.; Kato, K.; Shoji, H.; Okita, N.; Takashima, A.; Honma, Y.; Iwasa, S.; Hamaguchi, T.; Yamada, Y.; Shimada, Y.; et al. A retrospective analysis of 5-fluorouracil plus cisplatin as first-line chemotherapy in the recent treatment strategy for patients with metastatic or recurrent esophageal squamous cell carcinoma. Int. J. Clin. Oncol. 2018, 23, 466–472. [Google Scholar] [CrossRef]
- Hayashi, K.; Ando, N.; Watanabe, H.; Ide, H.; Nagai, K.; Aoyama, N.; Takiyama, W.; Ishida, K.; Isono, K.; Makuuchi, H.; et al. Phase II evaluation of protracted infusion of cisplatin and 5-fluorouracil in advanced squamous cell carcinoma of the esophagus: A Japan Esophageal Oncology Group (JEOG) Trial (JCOG9407). Jpn. J. Clin. Oncol. 2001, 31, 419–423. [Google Scholar] [CrossRef] [Green Version]
- Iizuka, T.; Kakegawa, T.; Ide, H.; Ando, N.; Watanabe, H.; Tanaka, O.; Takagi, I.; Isono, K.; Ishida, K.; Arimori, M.; et al. Phase II evaluation of cisplatin and 5-fluorouracil in advanced squamous cell carcinoma of the esophagus: A Japanese Esophageal Oncology Group Trial. Jpn. J. Clin. Oncol. 1992, 22, 172–176. [Google Scholar]
- Al-Batran, S.E.; Hartmann, J.T.; Probst, S.; Schmalenberg, H.; Hollerbach, S.; Hofheinz, R.; Rethwisch, V.; Seipelt, G.; Homann, N.; Wilhelm, G.; et al. Phase III trial in metastatic gastroesophageal adenocarcinoma with fluorouracil, leucovorin plus either oxaliplatin or cisplatin: A study of the Arbeitsgemeinschaft Internistische Onkologie. J. Clin. Oncol. 2008, 26, 1435–1442. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Moiseyenko, V.M.; Tjulandin, S.; Majlis, A.; Constenla, M.; Boni, C.; Rodrigues, A.; Fodor, M.; Chao, Y.; Voznyi, E.; et al. Phase III study of docetaxel and cisplatin plus fluorouracil compared with cisplatin and fluorouracil as first-line therapy for advanced gastric cancer: A report of the V325 Study Group. J. Clin. Oncol. 2006, 24, 4991–4997. [Google Scholar] [CrossRef]
- Ross, P.; Nicolson, M.; Cunningham, D.; Valle, J.; Seymour, M.; Harper, P.; Price, T.; Anderson, H.; Iveson, T.; Hickish, T.; et al. Prospective randomized trial comparing mitomycin, cisplatin, and protracted venous-infusion fluorouracil (PVI 5-FU) with epirubicin, cisplatin, and PVI 5-FU in advanced esophagogastric cancer. J. Clin. Oncol. 2002, 20, 1996–2004. [Google Scholar] [CrossRef]
- Cunningham, D.; Starling, N.; Rao, S.; Iveson, T.; Nicolson, M.; Coxon, F.; Middleton, G.; Daniel, F.; Oates, J.; Norman, A.R.; et al. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N. Engl. J. Med. 2008, 358, 36–46. [Google Scholar] [CrossRef] [Green Version]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Wilke, H.; Muro, K.; Van Cutsem, E.; Oh, S.C.; Bodoky, G.; Shimada, Y.; Hironaka, S.; Sugimoto, N.; Lipatov, O.; Kim, T.Y.; et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1224–1235. [Google Scholar] [CrossRef]
- Ford, H.E.; Marshall, A.; Bridgewater, J.A.; Janowitz, T.; Coxon, F.Y.; Wadsley, J.; Mansoor, W.; Fyfe, D.; Madhusudan, S.; Middleton, G.W.; et al. Docetaxel versus active symptom control for refractory oesophagogastric adenocarcinoma (COUGAR-02): An open-label, phase 3 randomised controlled trial. Lancet Oncol. 2014, 15, 78–86. [Google Scholar] [CrossRef]
- Hironaka, S.; Ueda, S.; Yasui, H.; Nishina, T.; Tsuda, M.; Tsumura, T.; Sugimoto, N.; Shimodaira, H.; Tokunaga, S.; Moriwaki, T.; et al. Randomized, open-label, phase III study comparing irinotecan with paclitaxel in patients with advanced gastric cancer without severe peritoneal metastasis after failure of prior combination chemotherapy using fluoropyrimidine plus platinum: WJOG 4007 trial. J. Clin. Oncol. 2013, 31, 4438–4444. [Google Scholar] [CrossRef]
- Thuss-Patience, P.C.; Kretzschmar, A.; Bichev, D.; Deist, T.; Hinke, A.; Breithaupt, K.; Dogan, Y.; Gebauer, B.; Schumacher, G.; Reichardt, P. Survival advantage for irinotecan versus best supportive care as second-line chemotherapy in gastric cancer—A randomised phase III study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Eur. J. Cancer 2011, 47, 2306–2314. [Google Scholar] [CrossRef]
- Shitara, K.; Doi, T.; Dvorkin, M.; Mansoor, W.; Arkenau, H.T.; Prokharau, A.; Alsina, M.; Ghidini, M.; Faustino, C.; Gorbunova, V.; et al. Trifluridine/tipiracil versus placebo in patients with heavily pretreated metastatic gastric cancer (TAGS): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2018, 19, 1437–1448. [Google Scholar] [CrossRef]
- Bando, H.; Shimodaira, H.; Fujitani, K.; Takashima, A.; Yamaguchi, K.; Nakayama, N.; Takahashi, T.; Oki, E.; Azuma, M.; Nishina, T.; et al. A phase II study of nab-paclitaxel in combination with ramucirumab in patients with previously treated advanced gastric cancer. Eur. J. Cancer 2018, 91, 86–91. [Google Scholar] [CrossRef] [Green Version]
- Ajani, J.A.; D’Amico, T.A.; Almhanna, K.; Bentrem, D.J.; Chao, J.; Das, P.; Denlinger, C.S.; Fanta, P.; Farjah, F.; Fuchs, C.S.; et al. Gastric Cancer, Version 3.2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2016, 14, 1286–1312. [Google Scholar] [CrossRef]
- Moehler, M.; Al-Batran, S.E.; Andus, T.; Arends, J.; Arnold, D.; Baretton, G.; Bornschein, J.; Budach, W.; Daum, S.; Dietrich, C.; et al. S3-Leitlinie Magenkarzinom—Diagnostik und Therapie der Adenokarzinome des Magens und des ösophagogastralen Übergangs—Langversion 2.0—August 2019. AWMF-Registernummer: 032/009OL. Z Gastroenterol. 2019, 57, 1517–1632. [Google Scholar] [CrossRef] [PubMed]
- Aigner, K.R.; Selak, E.; Gailhofer, S.; Aigner, K. Hypoxic Isolated Abdominal Perfusion (HAP) chemotherapy for non-operable advanced staged ovarian cancer with peritoneal carcinosis: An experience in 45 platinum-refractory ovarian cancer patients. Indian J. Surg. Oncol. 2019, 10, 506–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient’s Characteristics | ||
|---|---|---|
| Variable | N | % |
| All | 14 | 100 |
| Age, median years; range | 55 | 35–68 |
| Sex | ||
| female | 2 | 14.3 |
| male | 12 | 85.7 |
| Primary metastatic | 9 | 64.3 |
| Relapse | 5 | 35.7 |
| Metastatic site | ||
| liver | 5 | 35.7 |
| lymph nodes | 8 | 57.1 |
| lungs | 8 | 57.1 |
| bone | 2 | 14.3 |
| brain | 2 | 14.3 |
| others | 2 | 14.3 |
| local relapse | 3 | 21.4 |
| Previous therapy | ||
| Resection primary tumor | 5 | 35.7 |
| Systemic chemotherapy | 14 | 100 |
| Radiotherapy | 8 | 57.1 |
| Stent | 2 | 14.3 |
| Metastasectomy | 2 | 14.3 |
| Regional chemotherapy | ||
| Total Cycles | 51 | 100 |
| Art. Infusion | 12 | 23.5 |
| UAP | 3 | 5.8 |
| ITP | 36 | 70.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vashist, Y.; Aigner, K.; Dam, M.; Gailhofer, S.; Aigner, K.R. Regional Chemotherapy Is a Valuable Second-Line Approach in Metastatic Esophageal Cancer after Failure to First-Line Palliative Treatment. Curr. Oncol. 2022, 29, 4868-4878. https://doi.org/10.3390/curroncol29070386
Vashist Y, Aigner K, Dam M, Gailhofer S, Aigner KR. Regional Chemotherapy Is a Valuable Second-Line Approach in Metastatic Esophageal Cancer after Failure to First-Line Palliative Treatment. Current Oncology. 2022; 29(7):4868-4878. https://doi.org/10.3390/curroncol29070386
Chicago/Turabian StyleVashist, Yogesh, Kornelia Aigner, Miriam Dam, Sabine Gailhofer, and Karl R. Aigner. 2022. "Regional Chemotherapy Is a Valuable Second-Line Approach in Metastatic Esophageal Cancer after Failure to First-Line Palliative Treatment" Current Oncology 29, no. 7: 4868-4878. https://doi.org/10.3390/curroncol29070386
APA StyleVashist, Y., Aigner, K., Dam, M., Gailhofer, S., & Aigner, K. R. (2022). Regional Chemotherapy Is a Valuable Second-Line Approach in Metastatic Esophageal Cancer after Failure to First-Line Palliative Treatment. Current Oncology, 29(7), 4868-4878. https://doi.org/10.3390/curroncol29070386