Significance of the Number and the Location of Metastatic Lymph Nodes in Locally Recurrent or Persistent Cervical Cancer Patients Treated with Salvage Hysterectomy plus Lymphadenectomy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Initial Diagnosis and Radiotherapy
2.3. Salvage Surgery
2.4. Assessment of Surgical Complications
2.5. Follow-Up
2.6. Statistical Analysis
3. Results
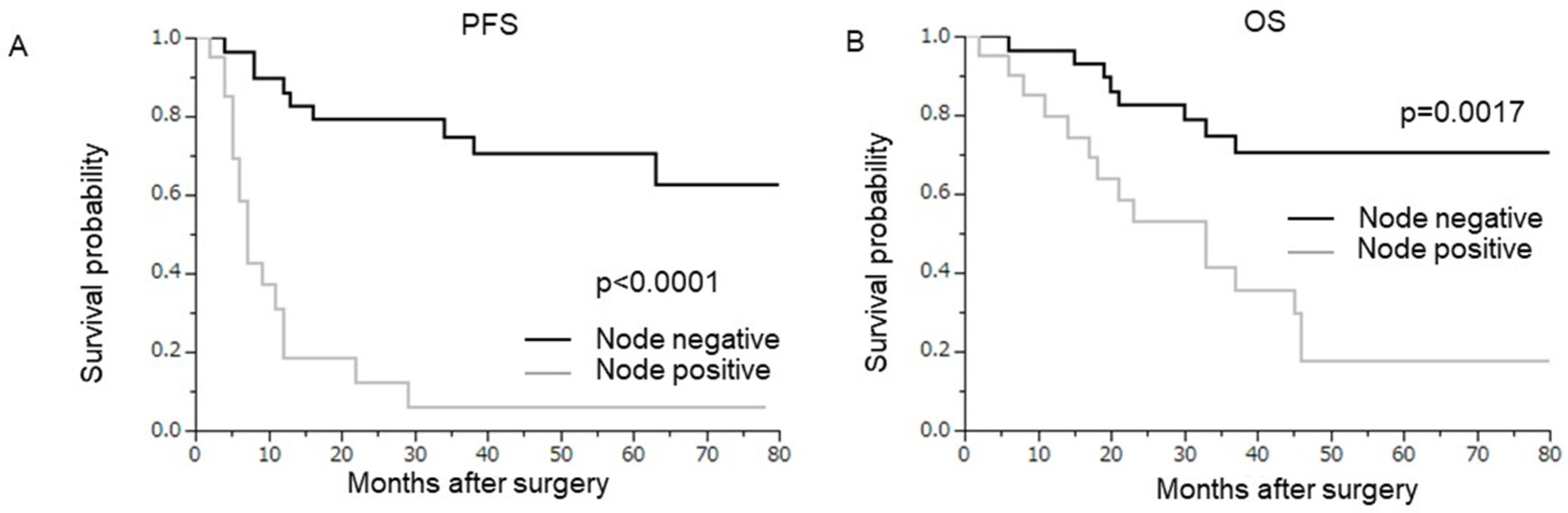
3.1. Prognostic Significance of Nodal Metastasis
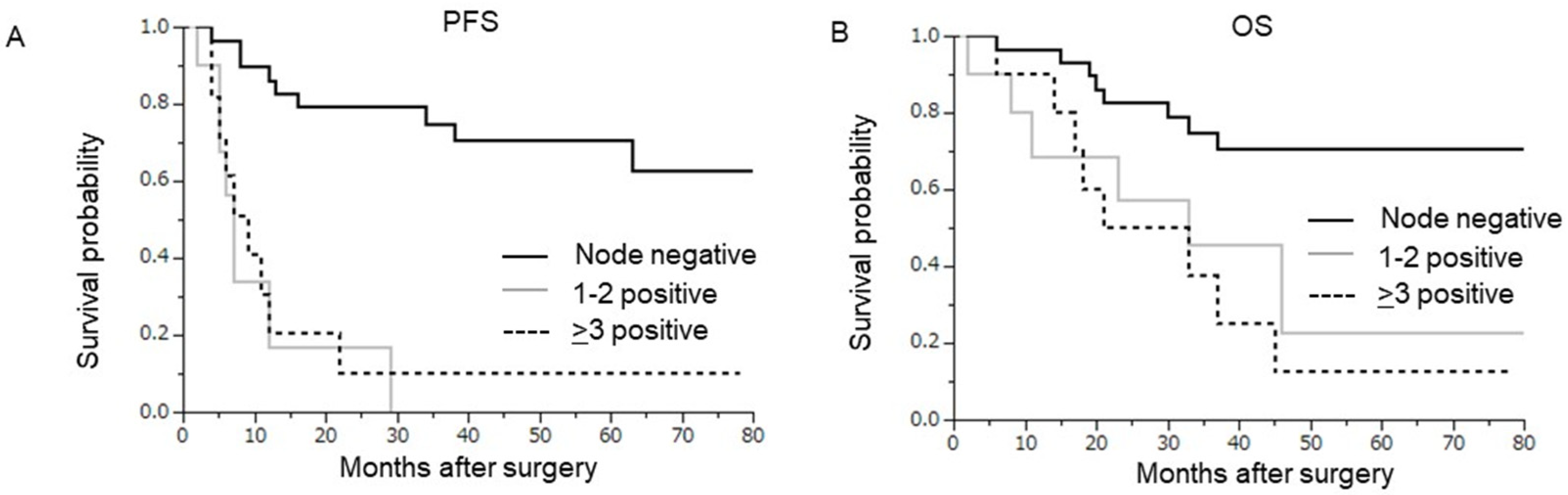
3.2. Prognostic Significance of the Number of Lymph Node Metastases
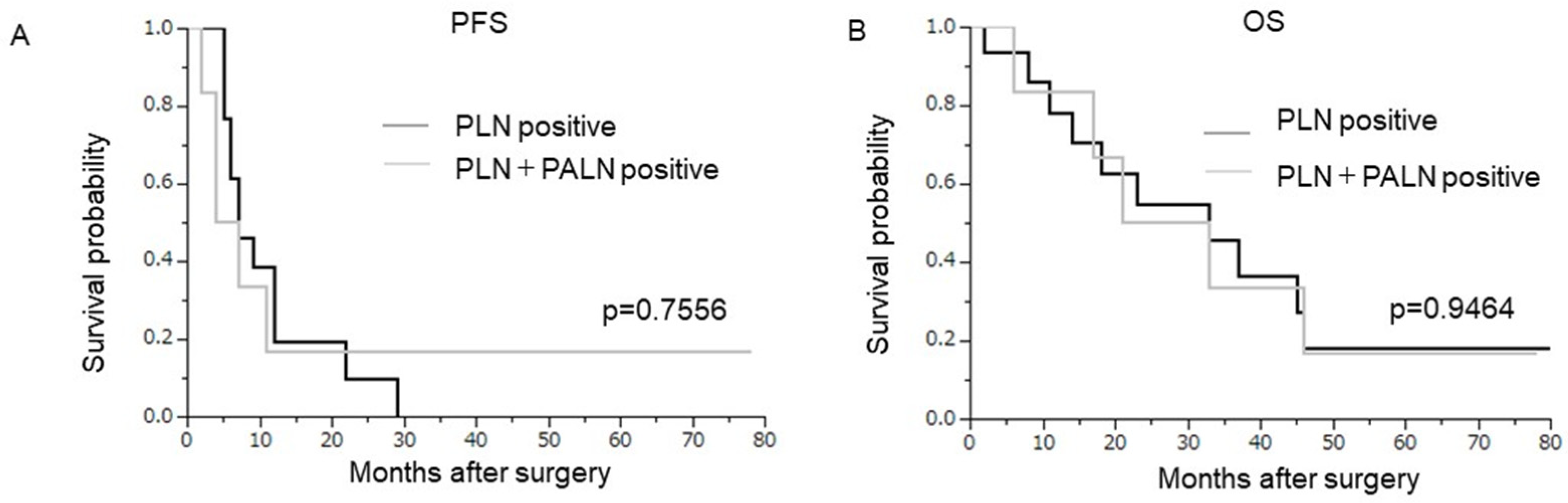
3.3. Prognostic Significance of the Location of Lymph Node Metastases
3.4. Site of Recurrence after Salvage Surgery According to Lymph Node Metastasis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mabuchi, S.; Kawano, M.; Takahashi, R.; Kuroda, H. Management of Metastatic and Recurrent Cervical Cancer. In Handbook of Gynecology; Shoupe, D., Ed.; Springer: Cham, Switzerland, 2016. [Google Scholar] [CrossRef]
- Hong, J.H.; Tsai, C.S.; Lai, C.H.; Chang, T.C.; Wang, C.C.; Chou, H.H.; Lee, S.P.; Hsueh, S. Recurrent squamous cell carcinoma of cervix after definitive radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Tewari, K.S.; Sill, M.W.; Long, H.J., 3rd; Penson, R.T.; Huang, H.; Ramondetta, L.M.; Landrum, L.M.; Oaknin, A.; Reid, T.J.; Leitao, M.M.; et al. Improved survival with bevacizumab in advanced cervical cancer. N. Engl. J. Med. 2014, 370, 734–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boers, A.; Arts, H.J.; Klip, H.; Nijhuis, E.R.; Pras, E.; Hollema, H.; Wisman, G.B.; Nijman, H.W.; Mourits, M.J.; Reyners, A.K.; et al. Radical surgery in patients with residual disease after (chemo)radiation for cervical cancer. Int. J. Gynecol. Cancer 2014, 24, 1276–1285. [Google Scholar] [CrossRef]
- Maneo, A.; Landoni, F.; Cormio, G.; Colombo, A.; Mangioni, C. Radical hysterectomy for recurrent or persistent cervical cancer following radiation therapy. Int. J. Gynecol. Cancer 1999, 9, 295–301. [Google Scholar] [CrossRef]
- Coleman, R.L.; Keeney, E.D.; Freedman, R.S.; Burke, T.W.; Eifel, P.J.; Rutledge, F.N. Radical hysterectomy for recurrent carcinoma of the uterine cervix after radiotherapy. Gynecol. Oncol. 1994, 55, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Mabuchi, S.; Kozasa, K.; Kimura, T. Radical hysterectomy after radiotherapy for recurrent or persistent cervical cancer. Int. J. Gynaecol. Obstet. 2017, 139, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Mabuchi, S.; Matsumoto, Y.; Komura, N.; Sawada, M.; Tanaka, M.; Yokoi, E.; Kozasa, K.; Yoshimura, A.; Kuroda, H.; Kimura, T. The efficacy of surgical treatment of recurrent or persistent cervical cancer that develops in a previously irradiated field: A monoinstitutional experience. Int. J. Clin. Oncol. 2017, 22, 927–936. [Google Scholar] [CrossRef]
- Takekuma, M.; Takahashi, F.; Mabuchi, S.; Kudaka, W.; Horie, K.; Ikeda, M.; Shikama, A.; Mitsuhashi, A.; Nagao, S.; Suzuki, S.; et al. Propensity score-matched analysis of systemic chemotherapy versus salvage hysterectomy for persistent cervical cancer after definitive radiotherapy/concurrent chemoradiotherapy. BMC Cancer 2020, 20, 1169. [Google Scholar] [CrossRef]
- Chiva, L.M.; Lapuente, F.; González-Cortijo, L.; González-Martín, A.; Rojo, A.; García, J.F.; Carballo, N. Surgical treatment of recurrent cervical cancer: State of the art and new achievements. Gynecol. Oncol. 2008, 110, S60–S66. [Google Scholar] [CrossRef]
- Berek, J.S.; Howe, C.; Lagasse, L.D.; Hacker, N.F. Pelvic exenteration for recurrent gynecologic malignancy: Survival and morbidity analysis of the 45-year experience at UCLA. Gynecol. Oncol. 2005, 99, 153–159. [Google Scholar] [CrossRef]
- Mabuchi, S.; Shimura, K.; Matsumoto, Y. The significance of post-radiotherapy parametrial involvement and the necessity of parametrial resection in locally-recurrent or persistent cervical cancer developed after radiotherapy. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102190. [Google Scholar] [CrossRef] [PubMed]
- Delgado, G.; Bundy, B.; Zaino, R.; Sevin, B.U.; Creasman, W.T.; Major, F. Prospective surgical-pathological study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: A Gynecologic Oncology Group study. Gynecol. Oncol. 1990, 38, 352–357. [Google Scholar] [CrossRef]
- Sakuragi, N.; Kato, T.; Shimada, C.; Kaneuchi, M.; Todo, Y.; Mitamura, T.; Takeda, M.; Kudo, M.; Murakami, G.; Watari, H. Oncological Outcomes After Okabayashi-Kobayashi Radical Hysterectomy for Early and Locally Advanced Cervical Cancer. JAMA Netw. Open 2020, 3, e204307. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.; Eom, K.Y.; Kim, Y.S.; Park, W.; Chun, M.; Lee, J.; Kim, Y.B.; Yoon, W.S.; Kim, J.H.; Choi, J.H.; et al. The Prognostic Impact of the Number of Metastatic Lymph Nodes and a New Prognostic Scoring System for Recurrence in Early-Stage Cervical Cancer with High Risk Factors: A Multicenter Cohort Study (KROG 15-04). Cancer Res. Treat. 2018, 50, 964–974. [Google Scholar] [CrossRef] [PubMed]
- Okazawa, M.; Mabuchi, S.; Isohashi, F.; Suzuki, O.; Ohta, Y.; Fujita, M.; Yoshino, K.; Enomoto, T.; Kamiura, S.; Kimura, T. The prognostic significance of multiple pelvic node metastases in cervical cancer patients treated with radical hysterectomy plus adjuvant chemoradiotherapy. Int. J. Gynecol. Cancer 2012, 22, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Mabuchi, S.; Okazawa, M.; Isohashi, F.; Ohta, Y.; Maruoka, S.; Yoshioka, Y.; Enomoto, T.; Morishige, K.; Kamiura, S.; Kimura, T. Postoperative whole pelvic radiotherapy plus concurrent chemotherapy versus extended-field irradiation for early-stage cervical cancer patients with multiple pelvic lymph node metastases. Gynecol. Oncol. 2011, 120, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli, F.A.; Stratton, M.R. (Eds.) Tumours of the Uterine Cervix. WHO Classifcation of Tumours: Pathology and Genetics of Tumours of the Breast and Female Genital Organs; IARC Press: Lyon, France, 2002; pp. 259–289. [Google Scholar]
- Mabuchi, S.; Isohashi, F.; Maruoka, S.; Hisamatsu, T.; Takiuchi, T.; Yoshioka, Y.; Kimura, T. Post-treatment follow-up procedures in cervical cancer patients previously treated with radiotherapy. Arch. Gynecol. Obstet. 2012, 286, 179–185. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Mabuchi, S.; Isohashi, F.; Komura, N.; Ogawa, K.; Kimura, T. Impact of a reduction in follow-up frequency on life expectancy in uterine cervical cancer patients. Int. J. Clin. Oncol. 2020, 25, 1170–1177. [Google Scholar] [CrossRef]
- Querleu, D.; Cibula, D.; Abu-Rustum, N.R. 2017 Update on the Querleu-Morrow Classification of Radical Hysterectomy. Ann. Surg. Oncol. 2017, 24, 3406–3412. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of Surgical Complications: A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2014, 240, 205–213. [Google Scholar] [CrossRef]
- Mabuchi, S.; Isohashi, F.; Yoshioka, Y.; Temma, K.; Takeda, T.; Yamamoto, T.; Enomoto, T.; Morishige, K.; Inoue, T.; Kimura, T. Prognostic factors for survival in patients with recurrent cervical cancer previously treated with radiotherapy. Int. J. Gynecol. Cancer 2010, 20, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.C.; Hentschel, B.; Fischer, U.; Peter, D.; Bilek, K. Detection of micrometastases in pelvic lymph nodes in patients with carcinoma of the cervix uteri using step sectioning: Frequency, topographic distribution and prognostic impact. Gynecol. Oncol. 2008, 111, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Mabuchi, S.; Yamamoto, M.; Murata, H.; Yokoe, T.; Hamanishi, J.; Terai, Y.; Imatake, H.; Mabuchi, Y.; Mori, T.; Kitada, F.; et al. Bevacizumab-associated events in Japanese women with cervical cancer: A multi-institutional survey of Obstetrical Gynecological Society of Kinki district, Japan. Int. J. Clin. Oncol. 2021, 26, 598–605. [Google Scholar] [CrossRef]
- Colombo, N.; Dubot, C.; Lorusso, D.; Caceres, M.V.; Hasegawa, K.; Shapira-Frommer, R.; Tewari, K.S.; Salman, P.; Hoyos Usta, E.; Yañez, E.; et al. Pembrolizumab for Persistent, Recurrent, or Metastatic Cervical Cancer. N. Engl. J. Med. 2021, 385, 1856–1867. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 50) n (%) | ||
|---|---|---|
| Initial characteristics | ||
| Initial stage a | IB1-IIA2 | 5 (10.0) |
| IIB-IIIA | 22 (44.0) | |
| IIIB-IVA | 17 (34.0) | |
| IVB | 6 (12.0) | |
| Histology | SCC | 30 (60.0) |
| AC | 20 (40.0) | |
| Types of radiotherapy | Pelvic EBRT+ICBT | 44 (88.0) |
| EFRT+ICBT | 4 (8.0) | |
| Pelvic ERBT alone | 2 (4.0) | |
| Concurrent chemotherapy | Yes | 48 (96.0) |
| No | 2 (4.0) | |
| Post-recurrence characteristics | ||
| Age | Median (range) | 53.5 (26–82) |
| ≤39 | 8 (16.0) | |
| 40–64 | 35 (70.0) | |
| 65≤ | 7 (14.0) | |
| Disease status | Recurrent cancer | 13 (26.0) |
| Persistent cancer | 37 (74.0) | |
| BMI | Median (range) | 20.4 (13.6–32.2) |
| <20.0 | 23 (46.0) | |
| ≥20.0 | 27 (54.0) | |
| Tumor diameter (mm) b | Median (range) | 30 (5–75) |
| <10 | 12 (24.0) | |
| 10–20 | 4 (8.0) | |
| 20≤ | 34 (68.0) | |
| NAC | No | 47 (94.0) |
| Yes | 3 (6.0) | |
| Hysterectomy performed | Type A | 3 (6.0) |
| Type B or greater | 47 (94.0) | |
| Lymphadenectomy performed | PLND | 24 (48.0) |
| PLND+PALND | 26 (52.0) | |
| Pathological findings from salvage surgery | ||
| Parametrial invasion | Negative | 35 (70.0) |
| Positive | 15 (30.0) | |
| Surgical margins | Negative | 38 (76.0) |
| Close or positive | 12 (24.0) | |
| Location of lymph node metastasis | No | 29 (58.0) |
| PLN | 15 (30.0) | |
| PLN+PAN | 6 (12.0) | |
| Number of lymph node metastases | 0 | 29 (58.0) |
| 1–2 | 10 (20.0) | |
| 3≤ | 11 (22.0) | |
| Stromal invasion | Less than half | 22 (44.0) |
| More than half | 28 (56.0) | |
| LSVI | Negative | 25 (50.0) |
| Positive | 25 (50.0) | |
| Peritoneal cytology c | Negative | 44 (88.0) |
| Positive | 2 (4.0) | |
| Adjuvant treatments after surgery | No | 29 (58.0) |
| Yes | 21 (42.0) | |
| Symptom status | No | 29 (58.0) |
| Yes | 21 (42.0) |
| All Patients (n = 50) n (%) | Node-Negative Group (n = 29) n (%) | Node-Positive Group (n = 21) n (%) | p-Value | |||
|---|---|---|---|---|---|---|
| Recurrence after surgery | No | 24 (48.0) | 20 (69.0) | 4 (19.1) | 0.0005 | |
| Yes (median 34 months) | 26 (52.0) | 9 (31.0) | 17 (81.0) | |||
| Site of recurrence after surgery | Pelvis alone | 5 (19.2) | 1 (11.1) | 4 (23.5) | 0.4447 | |
| Distant alone or Pelvis+Distant | All | 21 (80.8) | 8 (88.9) | 13 (76.5) | ||
| LNs a | 6 (23.1) | 0 | 6 (35.3) | 0.0737 | ||
| Disseminations b | 6 (23.1) | 3 (33.3) | 3 (17.6) | |||
| Visceral organs c | 9 (34.6) | 5 (55.6) | 4 (23.5) | |||
| Deaths after surgery | No | 26 (52.0) | 20 (69.0) | 6 (28.6) | 0.0048 | |
| Yes (median 46 months) | 24 (48.0) | 9 (31.0) | 15 (71.4) |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Hazard Ratio | 95%CI | p-Value | Hazard Ratio | 95%CI | p-Value | ||
| Age (years) | <50 | 1 | 1 | ||||
| 50≤ | 5.24 | 1.45–23.30 | 0.0098 | 1.81 | 0.74–4.80 | 0.1996 | |
| BMI | <20.0 | 1 | |||||
| ≥20.0 | 0.67 | 0.21–2.10 | 0.4839 | ||||
| Initial stage a | IB1-IIA | 1 | |||||
| IIB-IIIA | 0.45 | 0.07–3.92 | 0.4276 | ||||
| IIIB-IVA | 0.51 | 0.06–7.51 | 0.5947 | ||||
| IVB | 8.82 | 0.74–175.2 | 0.0865 | ||||
| Histology | SCC | 1 | |||||
| Non-SCC | 1.64 | 0.30–8.87 | 0.5555 | ||||
| Disease status | Recurrent | 1 | |||||
| Persistent | 5.32 | 0.83–31.45 | 0.0756 | ||||
| Tumor diameter b | <2 cm | 1 | 1 | ||||
| ≥2 cm | 13.91 | 2.06–135.4 | 0.0058 | 5.11 | 1.45–24.32 | 0.0100 | |
| NAC | No | 1 | |||||
| Yes | 0.28 | 0.02–3.21 | 0.2997 | ||||
| Hysterectomy performed | Type A | 1 | |||||
| Type B or greater | 12.86 | 0.23–1314.91 | 0.2221 | ||||
| Lymphadenectomy performed | PLND | 1 | |||||
| PLND+PALND | 1.41 | 0.65–3.23 | 0.3884 | ||||
| Parametrial invasion | Negative | 1 | |||||
| Positive | 0.35 | 0.04–2.36 | 0.2805 | ||||
| Surgical margins | Negative | 1 | 1 | ||||
| Close or positive | 11.41 | 1.32–121.03 | 0.0268 | 4.49 | 1.27–16.94 | 0.0197 | |
| Lymph node metastasis | Negative | 1 | 1 | ||||
| Positive | 7.57 | 3.27–18.67 | <0.0001 | 5.36 | 1.41–6.66 | 0.0020 | |
| Stromal invasion | Less than half | 1 | 1 | ||||
| More than half | 6.89 | 1.02–50.42 | 0.0472 | 2.44 | 0.79–8.51 | 0.1240 | |
| LSVI | Negative | 1 | |||||
| Positive | 1.45 | 0.13–13.98 | 0.7556 | ||||
| Peritoneal cytology c | Negative | 1 | 1 | ||||
| Positive | 51.9 | 4.17–1277.18 | 0.0014 | 1.79 | 0.39–12.99 | 0.4759 | |
| Adjuvant treatments after hysterectomy | No | 1 | |||||
| Yes | 1.75 | 0.27–10.55 | 0.5460 | ||||
| Symptom status | No | 1 | |||||
| Yes | 1.32 | 0.31–5.80 | 0.6966 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mabuchi, S.; Komura, N.; Kodama, M.; Maeda, M.; Matsumoto, Y.; Kamiura, S. Significance of the Number and the Location of Metastatic Lymph Nodes in Locally Recurrent or Persistent Cervical Cancer Patients Treated with Salvage Hysterectomy plus Lymphadenectomy. Curr. Oncol. 2022, 29, 4856-4867. https://doi.org/10.3390/curroncol29070385
Mabuchi S, Komura N, Kodama M, Maeda M, Matsumoto Y, Kamiura S. Significance of the Number and the Location of Metastatic Lymph Nodes in Locally Recurrent or Persistent Cervical Cancer Patients Treated with Salvage Hysterectomy plus Lymphadenectomy. Current Oncology. 2022; 29(7):4856-4867. https://doi.org/10.3390/curroncol29070385
Chicago/Turabian StyleMabuchi, Seiji, Naoko Komura, Michiko Kodama, Michihide Maeda, Yuri Matsumoto, and Shoji Kamiura. 2022. "Significance of the Number and the Location of Metastatic Lymph Nodes in Locally Recurrent or Persistent Cervical Cancer Patients Treated with Salvage Hysterectomy plus Lymphadenectomy" Current Oncology 29, no. 7: 4856-4867. https://doi.org/10.3390/curroncol29070385
APA StyleMabuchi, S., Komura, N., Kodama, M., Maeda, M., Matsumoto, Y., & Kamiura, S. (2022). Significance of the Number and the Location of Metastatic Lymph Nodes in Locally Recurrent or Persistent Cervical Cancer Patients Treated with Salvage Hysterectomy plus Lymphadenectomy. Current Oncology, 29(7), 4856-4867. https://doi.org/10.3390/curroncol29070385