Outcomes of Intercalary Endoprostheses as a Treatment for Metastases in the Femoral and Humeral Diaphysis

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
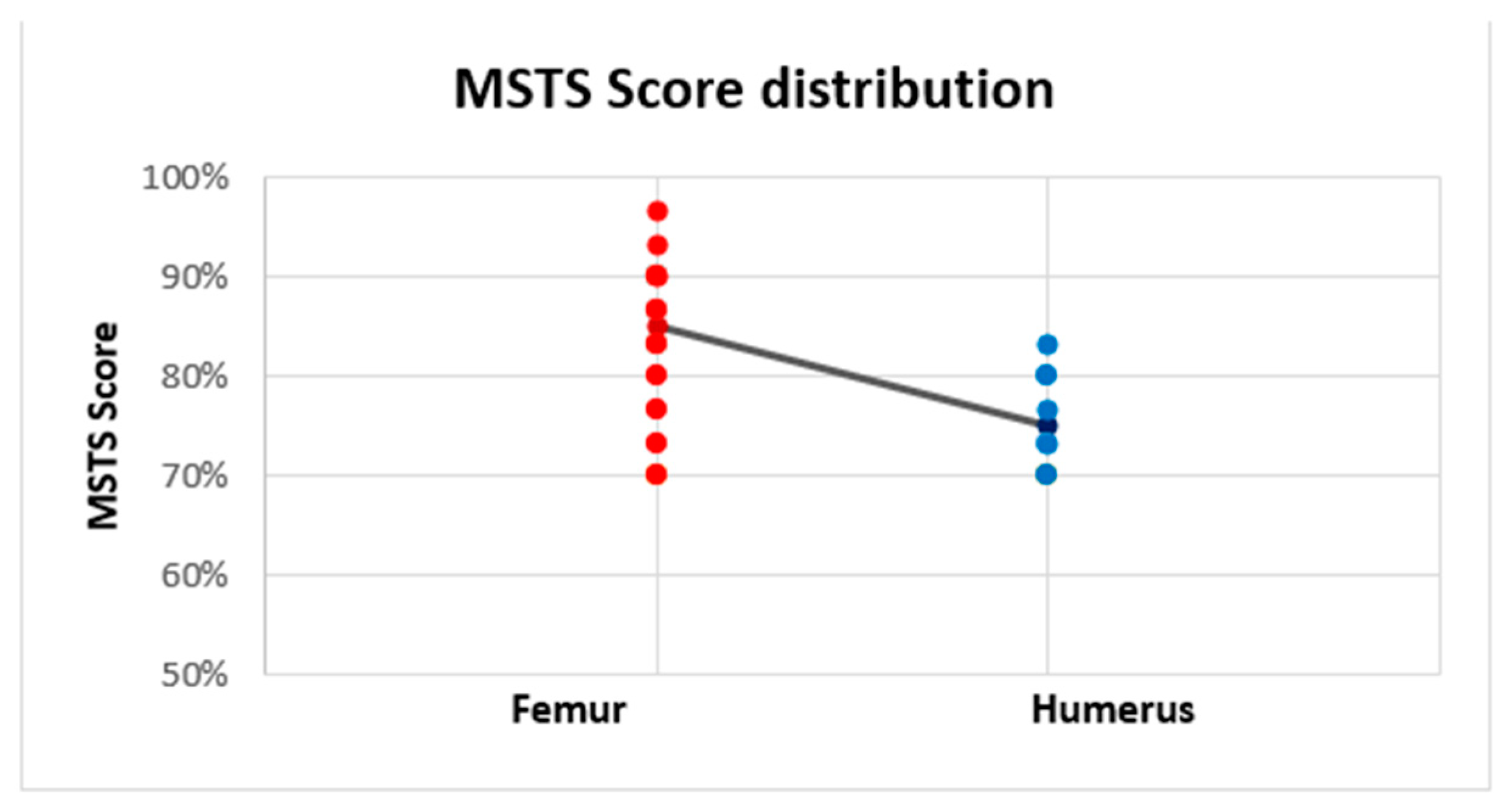
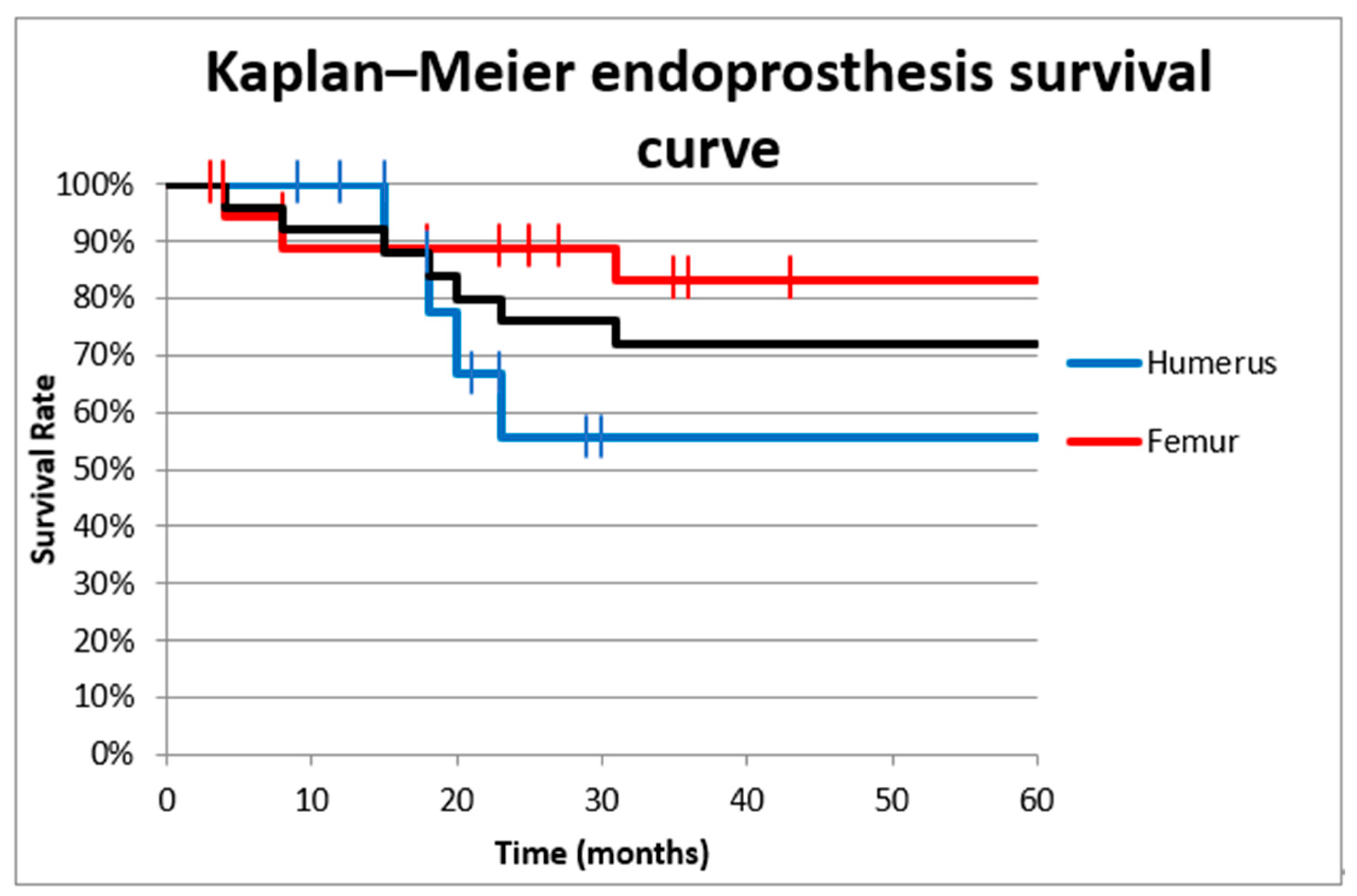
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsukamoto, S.; Kido, A.; Tanaka, Y.; Facchini, G.; Peta, G.; Rossi, G.; Mavrogenis, A.F. Current Overview of Treatment for Metastatic Bone Disease. Curr. Oncol. 2021, 28, 3347–3372. [Google Scholar] [CrossRef] [PubMed]
- Hamada, K.; Naka, N.; Tamiya, H.; Ozaki, R.; Outani, H.; Fujimoto, T.; Hashimoto, N.; Yoshikawa, H.; Araki, N. Intercalary Endoprosthetic Reconstruction for Impending Pathological Fractures in Patients with Femoral Diaphyseal Bone Metastases. Eur. J. Orthop. Surg. Traumatol. 2009, 19, 547–551. [Google Scholar] [CrossRef]
- Lesenský, J.; Mavrogenis, A.F. Cement Intercalary Reconstruction After Bone Tumor Resection. Orthopedics 2021, 44, e593–e599. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, J.J.; van der Linden, Y.M.; van der Wal, C.W.P.G.; Jutte, P.C.; van der Velden, J.M.; Smolle, M.A.; van der Zwaal, P.; Koper, P.; Bakri, L.; de Pree, I.; et al. An Easy-to-Use Prognostic Model for Survival Estimation for Patients with Symptomatic Long Bone Metastases. J. Bone Jt. Surg. 2018, 100, 196–204. [Google Scholar] [CrossRef]
- Piccioli, A.; Spinelli, M.S.; Forsberg, J.A.; Wedin, R.; Healey, J.H.; Ippolito, V.; Daolio, P.A.; Ruggieri, P.; Maccauro, G.; Gasbarrini, A.; et al. How Do We Estimate Survival? External Validation of a Tool for Survival Estimation in Patients with Metastatic Bone Disease—Decision Analysis and Comparison of Three International Patient Populations. BMC Cancer 2015, 15, 424. [Google Scholar] [CrossRef]
- Ellis, P.M. The Importance of Multidisciplinary Team Management of Patients with Non-Small-Cell Lung Cancer. Curr. Oncol. 2012, 19, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Z.; Ye, Z.; Yan, T.; Tang, X.; Guo, W.; Yang, R. Intercalary Prosthetic Replacement Is a Reliable Solution for Metastatic Humeral Shaft Fractures: Retrospective, Observational Study of a Single Center Series. World J. Surg. Oncol. 2021, 19, 140. [Google Scholar] [CrossRef]
- Errani, C.; Mavrogenis, A.F.; Cevolani, L.; Spinelli, S.; Piccioli, A.; Maccauro, G.; Baldini, N.; Donati, D. Treatment for Long Bone Metastases Based on a Systematic Literature Review. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 205–211. [Google Scholar] [CrossRef]
- Errani, C.; Cosentino, M.; Ciani, G.; Ferra, L.; Alfaro, P.A.; Bordini, B.; Donati, D.M. C-Reactive Protein and Tumour Diagnosis Predict Survival in Patients Treated Surgically for Long Bone Metastases. Int. Orthop. (SICOT) 2021, 45, 1337–1346. [Google Scholar] [CrossRef]
- Ruatta, F.; Derosa, L.; Escudier, B.; Colomba, E.; Guida, A.; Baciarello, G.; Loriot, Y.; Fizazi, K.; Albiges, L. Prognosis of Renal Cell Carcinoma with Bone Metastases: Experience from a Large Cancer Centre. Eur. J. Cancer 2019, 107, 79–85. [Google Scholar] [CrossRef]
- Feyer, P.C.; Steingraeber, M. Radiotherapy of Bone Metastasis in Breast Cancer Patients—Current Approaches. Breast Care 2012, 7, 108–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zekry, K.M.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Alkhooly, A.Z.A.; Abd-Elfattah, A.S.; Elsaid, A.N.S.; Ahmed, A.R.; Tsuchiya, H. Reconstruction of Intercalary Bone Defect after Resection of Malignant Bone Tumor. J. Orthop. Surg. 2019, 27, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Büyükdoğan, K.; Göker, B.; Tokgözoğlu, M.; İnan, U.; Özkan, K.; Çolak, T.S.; Aslan, L.; Deveci, M.A.; Ayvaz, M. Preliminary Results of a New Intercalary Modular Endoprosthesis for the Management of Diaphyseal Bone Metastases. Jt. Dis. Relat. Surg. 2021, 32, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Ahlmann, E.R.; Menendez, L.R. Intercalary Endoprosthetic Reconstruction for Diaphyseal Bone Tumours. J. Bone Jt. Surg. 2006, 88-B, 1487–1491. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.; Ahlmann, E.R.; Allison, D.C.; Wang, L.; Menendez, L.R. Endoprostheses Last Longer Than Intramedullary Devices in Proximal Femur Metastases. Clin. Orthop. Relat. Res. 2012, 470, 684–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakellariou, V.I.; Mavrogenis, A.F.; Babis, G.C.; Soucacos, P.N.; Magnissalis, E.A.; Papagelopoulos, P.J. Comparison of Four Reconstructive Methods for Diaphyseal Defects of the Humerus After Tumor Resection. J. Appl. Biomech. 2012, 28, 568–578. [Google Scholar] [CrossRef]
- Pazourek, L.; Tomáš, T.; Mahdal, M.; Janíček, P.; Černý, J.; Ondrůšek, Š. Use of Solid Intercalary Allografts for Reconstruction Following the Resection of Primary Bone Tumors. Acta Chir. Orthop. Traumatol. Cechoslov. 2018, 85, 171–178. [Google Scholar]
- Aponte-Tinao, L.; Farfalli, G.L.; Ritacco, L.E.; Ayerza, M.A.; Muscolo, L.D. Intercalary Femur Allografts Are an Acceptable Alternative After Tumor Resection. Clin. Orthop. Relat. Res. 2012, 470, 728–734. [Google Scholar] [CrossRef] [Green Version]
- Ruggieri, P.; Mavrogenis, A.F.; Bianchi, G.; Sakellariou, V.I.; Mercuri, M.; Papagelopoulos, P.J. Outcome of the Intramedullary Diaphyseal Segmental Defect Fixation System for Bone Tumors: Segmental Defect Fixation System. J. Surg. Oncol. 2011, 104, 83–90. [Google Scholar] [CrossRef]
- Benevenia, J.; Kirchner, R.; Patterson, F.; Beebe, K.; Wirtz, D.C.; Rivero, S.; Palma, M.; Friedrich, M.J. Outcomes of a Modular Intercalary Endoprosthesis as Treatment for Segmental Defects of the Femur, Tibia, and Humerus. Clin. Orthop. Relat. Res. 2016, 474, 539–548. [Google Scholar] [CrossRef] [Green Version]
- Streitbürger, A.; Hardes, J.; Nottrott, M.; Guder, W.K. Reconstruction Survival of Segmental Megaendoprostheses: A Retrospective Analysis of 28 Patients Treated for Intercalary Bone Defects after Musculoskeletal Tumor Resections. Arch. Orthop. Traumatol. Surg. 2022, 142, 41–56. [Google Scholar] [CrossRef] [PubMed]
- Henderson, E.R.; Groundland, J.S.; Pala, E.; Dennis, J.A.; Wooten, R.; Cheong, D.; Windhager, R.; Kotz, R.I.; Mercuri, M.; Funovics, P.T.; et al. Failure Mode Classification for Tumor Endoprostheses: Retrospective Review of Five Institutions and a Literature Review. J. Bone Jt. Surg. 2011, 93, 418–429. [Google Scholar] [CrossRef] [PubMed]
- Henderson, E.R.; O’Connor, M.I.; Ruggieri, P.; Windhager, R.; Funovics, P.T.; Gibbons, C.L.; Guo, W.; Hornicek, F.J.; Temple, H.T.; Letson, G.D. Classification of Failure of Limb Salvage after Reconstructive Surgery for Bone Tumours: A Modified System Including Biological and Expandable Reconstructions. Bone Jt. J. 2014, 96-B, 1436–1440. [Google Scholar] [CrossRef] [PubMed]
- Enneking, W.F.; Dunham, W.; Gebhardt, M.C.; Malawar, M.; Pritchard, D.J. A System for the Functional Evaluation of Reconstructive Procedures after Surgical Treatment of Tumors of the Musculoskeletal System. Clin. Orthop. Relat. Res. 1993, 286, 241–246. [Google Scholar] [CrossRef]
- Aldlyami, E.; Abudu, A.; Grimer, R.J.; Carter, S.R.; Tillman, R.M. Endoprosthetic Replacement of Diaphyseal Bone Defects. Long-Term Results. Int. Orthop. (SICOT) 2005, 29, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Hanna, S.A.; Sewell, M.D.; Aston, W.J.S.; Pollock, R.C.; Skinner, J.A.; Cannon, S.R.; Briggs, T.W.R. Femoral Diaphyseal Endoprosthetic Reconstruction after Segmental Resection of Primary Bone Tumours. J. Bone Jt. Surg. 2010, 92-B, 867–874. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Yu, X.; Xu, M.; Zheng, K.; Hu, Y.; Wang, F.; Lun, D. Intercalary Prosthetic Reconstruction for Pathologic Diaphyseal Humeral Fractures Due to Metastatic Tumors: Outcomes and Improvements. J. Shoulder Elb. Surg. 2018, 27, 2013–2020. [Google Scholar] [CrossRef]
- Zhao, L.; Tian, D.; Wei, Y.; Zhang, J.; Di, Z.; He, Z.; Hu, Y. Biomechanical Analysis of a Novel Intercalary Prosthesis for Humeral Diaphyseal Segmental Defect Reconstruction: Intercalary Prosthesis For Humeral Diaphyseal Defect. Orthop. Surg. 2018, 10, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, B.; Ossendorf, C.; Leerapun, T.; Sim, F.H. Intercalary Segmental Reconstruction after Bone Tumor Resection. Eur. J. Surg. Oncol. (EJSO) 2008, 34, 1271–1276. [Google Scholar] [CrossRef]
- Damron, T.A.; Leerapun, T.; Hugate, R.R.; Shives, T.C.; Sim, F.H. Does the Second-Generation Intercalary Humeral Spacer Improve on the First? Clin. Orthop. Relat. Res. 2008, 466, 1309–1317. [Google Scholar] [CrossRef] [Green Version]
- Abudu, A.; Carter, S.R.; Grimer, R.J. The Outcome and Functional Results of Diaphyseal Endoprostheses after Tumour Excision. J. Bone Jt. Surg. 1996, 78, 652–657. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Location | Diagnosis | Age (Years) | Resection Length (cm) | RT | Prosthesis Type | Follow-Up (Months) | Failure Type | Time to Failure (Months) | Complications | MSTS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Femur | Renal cell carcinoma | 52 | 12 | Yes | Modular | 35 | None | 28 | ||
| 2 | Femur | Renal cell carcinoma | 71 | 15 | No | Modular | 27 | None | 29 | ||
| 3 | Femur | Renal cell carcinoma | 73 | 10 | No | Modular | 25 | None | 27 | ||
| 4 | Humerus | Lung cancer | 65 | 9 | Yes | Modular | 9 | None | 23 | ||
| 5 | Humerus | Renal cell carcinoma | 56 | 9 | No | Modular | 12 | None | 25 | ||
| 6 | Humerus | Breast cancer | 75 | 8 | No | Modular | 9 | None | 24 | ||
| 7 | Humerus | Uterine sarcoma | 49 | 10 | No | Modular | 30 | II | 23 | Aseptic loosening | 21 |
| 8a | Femur | Renal cell carcinoma | 64 | 11 | No | Individual | 8 | III | 8 | Spacer failure | 21 |
| 8b | Femur | Failed spacer | 65 | 11 | No | Individual | 94 | None | 27 | ||
| 9 | Femur | Renal cell carcinoma | 63 | 8 | No | Individual | 3 | None | 22 | ||
| 10 | Femur | Breast cancer | 79 | 15 | No | Individual | 18 | None | 26 | ||
| 11 | Femur | Melanoma | 74 | 12 | No | Individual | 105 | None | 27 | ||
| 12 | Femur | Renal cell carcinoma | 67 | 10 | No | Individual | 3 | None | 23 | ||
| 13a | Femur | Renal cell carcinoma | 68 | 15 | No | Individual | 4 | III | 4 | Spacer failure | 21 |
| 13b | Femur | Failed spacer | 68 | 15 | No | Individual | 81 | None | 27 | ||
| 14 | Femur | Renal cell carcinoma | 75 | 10 | Yes | Individual | 36 | II | 31 | Aseptic loosening | 25 |
| 15 | Femur | Colon cancer | 54 | 14 | No | Modular | 8 | None | 24 | ||
| 16 | Femur | Renal cell carcinoma | 78 | 9 | No | Modular | 23 | None | 26 | ||
| 17 | Humerus | Breast cancer | 57 | 8 | No | Modular | 29 | II | 20 | Aseptic loosening | 22 |
| 18 | Femur | Renal cell carcinoma | 59 | 16 | Yes | Modular | 43 | None | 27 | ||
| 19 | Femur | Renal cell carcinoma | 61 | 15 | No | Modular | 36 | None | 26 | ||
| 20 | Humerus | Renal cell carcinoma | 62 | 9 | No | Modular | 18 | None | 23 | ||
| 21 | Humerus | Melanoma | 53 | 10 | No | Individual | 21 | II | 15 | Aseptic loosening | 22 |
| 22 | Femur | Renal cell carcinoma | 59 | 12 | No | Modular | 65 | None | 27 | ||
| 23 | Femur | Lung cancer | 66 | 11 | Yes | Modular | 23 | None | 25 | ||
| 24 | Humerus | Lung cancer | 71 | 9 | No | Modular | 15 | None | 25 | ||
| 25 | Humerus | Breast cancer | 55 | 10 | Yes | Modular | 24 | II | 18 | Aseptic loosening | 21 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahdal, M.; Pazourek, L.; Apostolopoulos, V.; Adámková Krákorová, D.; Staniczková Zambo, I.; Tomáš, T. Outcomes of Intercalary Endoprostheses as a Treatment for Metastases in the Femoral and Humeral Diaphysis. Curr. Oncol. 2022, 29, 3519-3530. https://doi.org/10.3390/curroncol29050284
Mahdal M, Pazourek L, Apostolopoulos V, Adámková Krákorová D, Staniczková Zambo I, Tomáš T. Outcomes of Intercalary Endoprostheses as a Treatment for Metastases in the Femoral and Humeral Diaphysis. Current Oncology. 2022; 29(5):3519-3530. https://doi.org/10.3390/curroncol29050284
Chicago/Turabian StyleMahdal, Michal, Lukáš Pazourek, Vasileios Apostolopoulos, Dagmar Adámková Krákorová, Iva Staniczková Zambo, and Tomáš Tomáš. 2022. "Outcomes of Intercalary Endoprostheses as a Treatment for Metastases in the Femoral and Humeral Diaphysis" Current Oncology 29, no. 5: 3519-3530. https://doi.org/10.3390/curroncol29050284
APA StyleMahdal, M., Pazourek, L., Apostolopoulos, V., Adámková Krákorová, D., Staniczková Zambo, I., & Tomáš, T. (2022). Outcomes of Intercalary Endoprostheses as a Treatment for Metastases in the Femoral and Humeral Diaphysis. Current Oncology, 29(5), 3519-3530. https://doi.org/10.3390/curroncol29050284