Sexual Functioning in Female Patients Undergoing Surgical Treatment for Colorectal Cancer—A Single-Center, Prospective Triple Timepoint Yearly Follow-Up

 , , ,
, , ,
Abstract
:1. Introduction
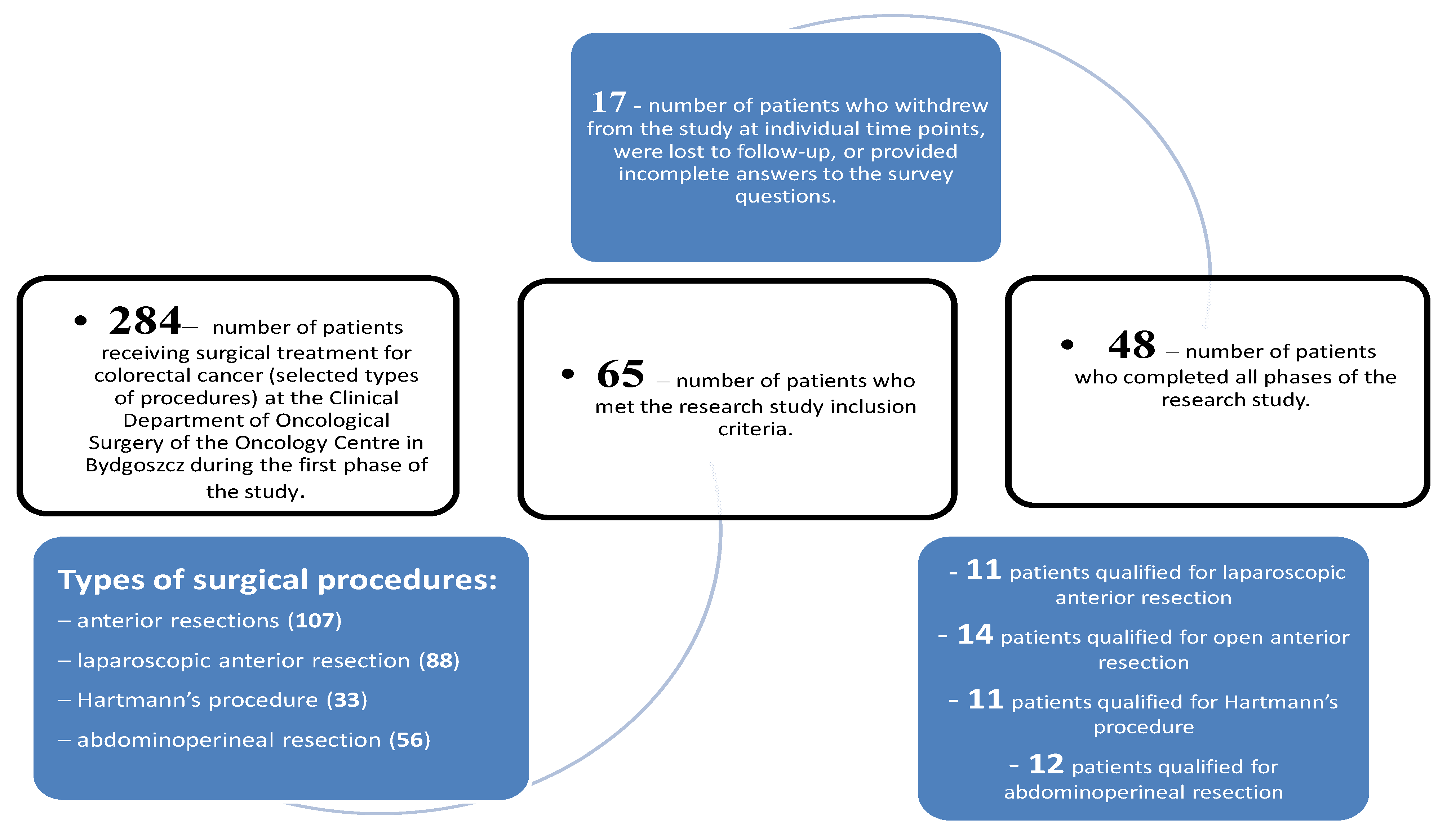
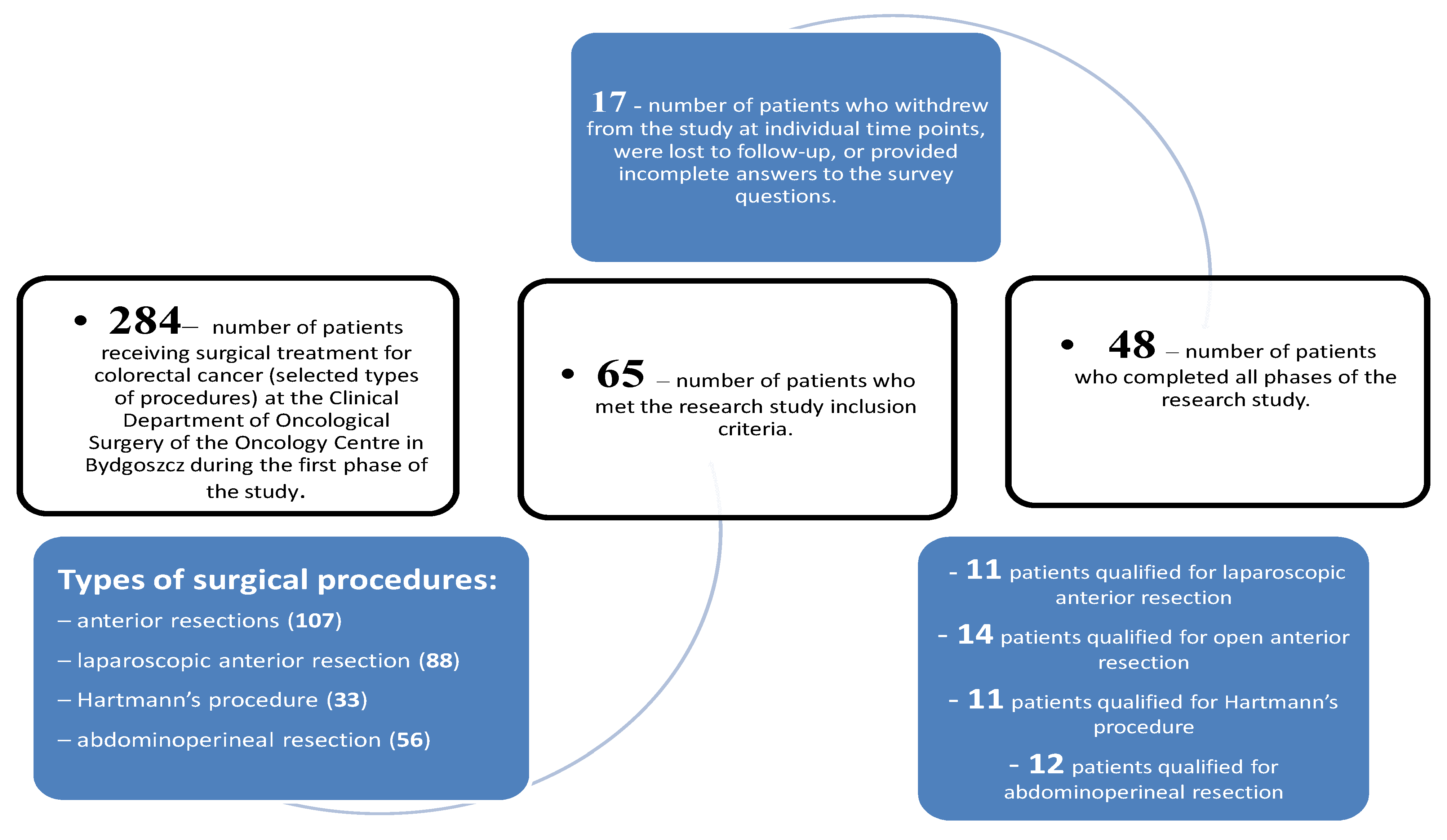
2. Material and Methods
- −
- good overall health status (Eastern Cooperative Oncology Group [ECOG] score of 0–1);
- −
- voluntary, written consent to participate in the study,
- −
- hospitalization at the Clinical Department of Oncological Surgery of the Franciszek Łukaszczyk Oncology Centre in Bydgoszcz at the time of recruitment;
- −
- no distant metastases;
- −
- age of up to 70 years;
- −
- patients married or staying in partnership for at least 12 months prior to the surgery.
- −
- class 3 obesity (Body Mass Index of >40);
- −
- concomitance of other serious diseases (>ASA II);
- −
- TNM (tumor, nodes, metastases) stage IV disease;
- −
- continuity of the digestive tract being restored during the study.
3. Results
4. Discussion
5. Conclusions
- The quality of their sexual live as self-assessed by patients with stoma was significantly worse than that in patients in whom gastrointestinal tract continuity had been maintained.
- Irrespective of the study group, deterioration in the quality of sexual life was observed six months after the treatment. One year after the surgery, the results were showing an upward trend; however, they remained lower than the baseline values in patients with stomia while exceeding the baseline scores in all subscales in patients in whom no stoma was required.
- Marital status and age were the demographic variables responsible for significant differentiation of satisfaction with sexual life. Better quality of sexual functioning was reported by younger and/or married patients.
- Neoadjuvant radiotherapy was the clinical variable responsible for significant differentiation of satisfaction with sexual life. Worse quality of life results related to sexual functioning were reported by patients who had received neoadjuvant radiotherapy prior to the surgery.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canty, J.; Stabile, C.; Milli, L.; Seidel, B.; Goldfrank, D.; Carter, J. Sexual function in women with colorectal/anal cancer. Sex. Med. Rev. 2019, 7, 202–222. [Google Scholar] [CrossRef] [PubMed]
- SvanstromRojvall, A.; Buchli, C.; Bottai, M.; Ahlberg, M.; Flöter-Rådestad, A.; Martling, A.; Segelman, J. Effect of radio-therapy for rectal cancer on female sexual function: A prospective cohort study. J. Br. Surg. 2020, 107, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Ho, V.P.; Lee, Y.; Stein, S.L.; Temple, L.K.F. Sexual function after treatment for rectal cancer: A review. Dis. Colon Rectum 2011, 54, 113–125. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Colorectal Cancer Facts and Figures, 2011–2013; American Cancer Society: Atlanta, GA, USA, 2011. [Google Scholar]
- Li, C.C.; Rew, L. A feminist perspective on sexuality and bodyimage in females with colorectal cancer: An integrative review. J. Wound Ostomy Cont. Nurs. 2010, 37, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Reese, J.B.; Porter, L.S.; Somers, T.J.; Keefe, F.J. Pilot feasibility study of a telephone-based couples intervention for physical intimacy and sexual concerns in colorectal cancer. J. Sex. Marital Ther. 2012, 38, 402–417. [Google Scholar] [CrossRef] [PubMed]
- Ayalon, R.; Bachner, Y.G. Medical, social, and personal factors as correlates of quality of life among older cancer patients with permanent stoma. Eur. J. Oncol. Nurs. 2019, 38, 50–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thyø, A.; Laurberg, S.; Emmertsen, K.J. Impact of bowel and stoma dysfunction on female sexuality after treatment for rectal cancer. Color. Dis. 2020, 22, 894–905. [Google Scholar] [CrossRef] [PubMed]
- Sharpe, L.; Patel, D.; Clarke, S. The relationship between body image disturbance and distress in colorectal cancer patients with and without stomas. J. Psychosom. Res. 2011, 70, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.M.; Santos, M.A.D.; Rosado, S.R.; Galvao, C.M.; Sonobe, H.M. Psychological aspects of patients with intestinal stoma: Integrative review. Rev. Lat. Am. Enferm. 2017, 25, 2950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albaugh, J.A.; Tenfelde, S.; Hayden, D.M. Sexual Dysfunction and Intimacy for Ostomates. Clin. Colon Rectal Surg. 2017, 30, 201–216. [Google Scholar] [PubMed]
- Traa, M.J.; Roukema, J.A.; De Vries, J.; Rutten, H.J.T.; Langenhoff, B.; Jansen, W.; Den Oudsten, B.L. Biopsychosocial predictors of sexual function and quality of sexual life: A study among patients with colorectal cancer. Transl. Androl. Urol. 2015, 4, 206–217. [Google Scholar] [PubMed]
- Traa, M.J.; De Vries, J.; Roukema, J.A.; Den Oudsten, B.L. Sexual (dys) function and the quality of sexual life in patients with colorectal cancer: A systematic review. Ann. Oncol. 2012, 23, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.M.; Marijen, C.A.M.; Maas, C.P.; Putter, H.; Rutten, H.J.; Stiggelbout, A.M.; Meershoek–Klein Kranenbarg, E.; van de Velde, C.J.H. Risk factors for sexual dysfunction after rectal cancer treatment. EJC 2009, 45, 1578–1588. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, Y.; Ussher, J.; Gilbert, E.; Perz, J.; Sandoval, M.; Sundquist, K. Changes in sexuality and intimacy after the diagnosis and treatment of cancer: The experience of partners in a sexual relationship with a person with cancer. Cancer Nurs. 2009, 32, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Zutshi, M.; Hull, T.; Shedda, S.; Lavery, I.; Hammel, J. Gender differences in mortality, quality of life and function after restorative procedures for rectal cancer. Colorectal Dis. 2013, 15, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, R.T.; Vollenhoven, B.J.; Weston, G.C. The effects of chemotherapy and radiotherapy on fertility in premenopausal women. Obstet. Gynecol. Surv. 2011, 66, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Svanström Röjvall, A.; Buchli, C.; FlöterRådestad, A.; Martling, A.; Segelman, J. Impact of Androgens on Sexual Function in Women With Rectal Cancer–A Prospective Cohort Study. J. Sex. Med. 2021, 18, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Welzel, G.; Hagele, V.; Wenz, F.; Mai, S.K. Quality of life outcomes in patients with anal cancer after combined radiochemotherapy. Strahlenther. Und Onkol. 2011, 187, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Haviland, J.; Sodergren, S.; Calman, L.; Corner, J.; Din, A.; Fenlon, D.; Grimmett, C.; Richardson, A.; Smith, P.W.; Winter, J. Social support following diagnosis and treatment for colorectal cancer and associations with health-related quality of life: Results from the UK ColoREctal Wellbeing (CREW) cohort study. Psychooncology 2017, 26, 2276–2284. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | No Stoma (A1) | Stoma (A2) | chi2/Fisher’s Test (p) | |||
|---|---|---|---|---|---|---|
| N | % | N | % | |||
| Type of surgery | Anterior resection | 14 | 56% | 0 | 0% | <0.0001 |
| Laparoscopic anterior resection | 11 | 44% | 0 | 0% | ||
| Abdominoperineal resection | 0 | 0% | 12 | 52.17% | ||
| Hartmann’s procedure | 0 | 0% | 11 | 47.83% | ||
| Neoadjuvant treatment | none | 9 | 36% | 0 | 0% | 0.0004 |
| chemotherapy | 0 | 0% | 3 | 13.04% | ||
| radiochemotherapy | 11 | 44% | 7 | 30.43% | ||
| radiotherapy | 5 | 20% | 13 | 56.52% | ||
| Adjuvant treatment | none | 17 | 68% | 15 | 65.22% | 0.6623 |
| chemotherapy | 7 | 28% | 5 | 21.74% | ||
| radiochemotherapy | 1 | 4% | 3 | 13.04% | ||
| Post-surgical complications | none | 21 | 84% | 18 | 78.26% | 0.7195 |
| observed | 4 | 16% | 5 | 21.74% | ||
| TNM stage of the disease (I–III) | I | 9 | 36% | 7 | 30.43% | 0.7717 |
| IIA | 8 | 32% | 11 | 47.83% | ||
| IIB | 1 | 4% | 0 | 0% | ||
| IIIB | 3 | 12% | 3 | 13.04% | ||
| IIIC | 4 | 16% | 2 | 8.7% | ||
| Educational background | elementary | 2 | 8% | 4 | 17.39% | 0.6834 |
| vocational | 5 | 20% | 3 | 13.04% | ||
| secondary | 12 | 48% | 12 | 52.17% | ||
| higher | 6 | 24% | 4 | 17.39% | ||
| Area of residence | urban | 19 | 76% | 16 | 69.57% | 0.6163 |
| rural | 6 | 24% | 7 | 30.43% | ||
| Employment status | retired/on disablement pension | 20 | 80% | 16 | 69.57% | 0.7369 |
| regular employment/company owner | 4 | 16% | 6 | 26.09% | ||
| housekeeping | 1 | 4% | 1 | 4.35% | ||
| Parity | 0 | 1 | 4% | 2 | 8.7% | 0.7051 |
| 1 | 3 | 12% | 2 | 8.7% | ||
| 2 | 15 | 60% | 12 | 52.17% | ||
| 3 | 4 | 16% | 4 | 17.39% | ||
| 4 | 1 | 4% | 1 | 4.35% | ||
| 5 | 0 | 0% | 2 | 8.7% | ||
| 7 | 1 | 4% | 0 | 0% | ||
| Marital status | married | 22 | 88% | 14 | 60.87% | 0.0301 |
| in partnership | 3 | 12% | 9 | 39.13% | ||
| Socioeconomic status | very good | 1 | 4% | 1 | 4.35% | 0.6812 |
| good | 12 | 48% | 8 | 34.78% | ||
| average | 11 | 44% | 14 | 60.87% | ||
| low | 1 | 4% | 0 | 0% | ||
| Weight | Height | BMI | Hospitalization Time | Age | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| A1 | A2 | A1 | A2 | A | A2 | A1 | A2 | A1 | A2 | |
| M | 69.42 | 66.46 | 159.6 | 159.24 | 27.22 | 25.86 | 7.72 | 8.39 | 62.48 | 62.43 |
| Me | 66.6 | 65 | 160 | 158 | 25.07 | 26.04 | 7 | 7 | 65 | 66 |
| SD | 15.94 | 14.38 | 6.76 | 5.45 | 5.95 | 6.21 | 4.73 | 5.96 | 9.3234 | 9.5908 |
| Mann–Whitney’s U-test/Student’s t-test (df = 46) | t = 0.6739 | t = 0.2024 | t = 0.7770 | Z = 0.3381 | t = 0.0166 | |||||
| p = 0.5037 | p = 0.8405 | p = 0.4411 | p = 0.7353 | p = 0.9869 | ||||||
| Variables Included in the Analysis | Group | M | Me | SD | Mann–Whitney’s U-Test |
|---|---|---|---|---|---|
| I—Desire [Measurement I] | A1 | 4.85 | 4.80 | 1.05 | Z = 1.3502 p = 0.1770 |
| A2 | 4.30 | 4.20 | 1.40 | ||
| II—Arousal [Measurement I] | A1 | 4.54 | 5.70 | 2.13 | Z = 1.3427 p = 0.1794 |
| A2 | 3.72 | 4.80 | 2.43 | ||
| III—Lubrication [Measurement I] | A1 | 4.27 | 5.10 | 1.98 | Z = 0.3029 p = 0.7619 |
| A2 | 3.65 | 5.10 | 2.51 | ||
| IV—Orgasm [Measurement I] | A1 | 4.38 | 5.20 | 2.02 | Z = 1.4471 p = 0.1479 |
| A2 | 3.39 | 4.80 | 2.49 | ||
| V—Satisfaction [Measurement I] | A1 | 5.17 | 5.60 | 0.91 | Z = 0.3271 p = 0.7436 |
| A2 | 4.75 | 5.60 | 1.45 | ||
| VI—Pain/discomfort [Measurement I] | A1 | 4.16 | 4.80 | 2.10 | Z = 1.1906 p = 0.2338 |
| A2 | 3.32 | 4.00 | 2.42 | ||
| Overall FSFI score [Measurement I] | A1 | 27.37 | 30.90 | 9.36 | Z = 1.4967 p = 0.1345 |
| A2 | 23.13 | 28.70 | 11.62 | ||
| I—Desire [Measurement II] | A1 | 4.66 | 6.00 | 1.68 | Z = 1.9151 p = 0.0555 |
| A2 | 3.83 | 4.20 | 1.47 | ||
| II—Arousal [Measurement II] | A1 | 3.79 | 5.10 | 2.48 | Z = 2.7056 p = 0.0068 |
| A2 | 1.96 | 2.10 | 2.06 | ||
| III—Lubrication [Measurement II] | A1 | 3.64 | 5.10 | 2.54 | Z = 2.2882 p = 0.0221 |
| A2 | 1.80 | 0.00 | 2.41 | ||
| IV—Orgasm [Measurement II] | A1 | 3.94 | 5.60 | 2.70 | Z = 2.8509 p = 0.0044 |
| A2 | 1.70 | 0.00 | 2.36 | ||
| V—Satisfaction [Measurement II] | A1 | 4.83 | 5.20 | 1.10 | Z = 3.0704 p = 0.0021 |
| A2 | 3.63 | 3.20 | 1.34 | ||
| VI—Pain/discomfort [Measurement II] | A1 | 3.66 | 4.80 | 2.55 | Z = 2.1160 p = 0.0343 |
| A2 | 2.00 | 0.00 | 2.51 | ||
| Overall FSFI score [Measurement II] | A1 | 24.52 | 32.80 | 12.69 | Z = 2.5187 p = 0.0118 |
| A2 | 14.93 | 9.50 | 10.86 | ||
| I—Desire [Measurement III] | A1 | 5.26 | 6.00 | 1.41 | Z = 1.8930 p = 0.0584 |
| A2 | 4.62 | 4.80 | 1.58 | ||
| II—Arousal [Measurement III] | A1 | 4.70 | 6.00 | 2.24 | Z = 3.1205 p = 0.0018 |
| A2 | 2.71 | 2.70 | 2.48 | ||
| III—Lubrication [Measurement III] | A1 | 4.46 | 5.40 | 2.15 | Z = 2.4730 p = 0.0134 |
| A2 | 2.69 | 2.40 | 2.59 | ||
| IV—Orgasm [Measurement III] | A1 | 4.69 | 6.00 | 2.23 | Z = 3.0707 p = 0.0021 |
| A2 | 2.64 | 2.40 | 2.56 | ||
| V—Satisfaction [Measurement III] | A1 | 5.18 | 5.60 | 1.21 | Z = 2.0210 p = 0.0433 |
| A2 | 4.28 | 4.80 | 1.53 | ||
| VI—Pain/discomfort [Measurement III] | A1 | 4.70 | 5.60 | 2.18 | Z = 1.9836 p = 0.0473 |
| A2 | 2.97 | 3.20 | 2.80 | ||
| Overall FSFI score [Measurement III] | A1 | 29.00 | 34.90 | 10.99 | Z = 3.0268 p = 0.0025 |
| A2 | 19.91 | 18.70 | 12.76 |
| Group | Variables Included in the Analysis | M | Me | SD | Friedman’s Test | |
|---|---|---|---|---|---|---|
| No stoma (A1) | I—Desire | [Measurement I] | 4.85 | 4.80 | 1.05 | T = 5.9385 p = 0.0513 |
| [Measurement II] | 4.66 | 6.00 | 1.68 | |||
| [Measurement III] | 5.26 | 6.00 | 1.41 | |||
| II—Arousal | [Measurement I] | 4.54 | 5.70 | 2.13 | T = 6.08 p = 0.0478 | |
| [Measurement II] | 3.79 | 5.10 | 2.48 | |||
| [Measurement III] | 4.70 | 6.00 | 2.24 | |||
| III—Lubrication | [Measurement I] | 4.27 | 5.10 | 1.98 | T = 3.4865 p = 0.175 | |
| [Measurement II] | 3.64 | 5.10 | 2.54 | |||
| [Measurement III] | 4.46 | 5.40 | 2.15 | |||
| IV—Orgasm | [Measurement I] | 4.38 | 5.20 | 2.02 | T = 4.9143 p = 0.0857 | |
| [Measurement II] | 3.94 | 5.60 | 2.70 | |||
| [Measurement III] | 4.69 | 6.00 | 2.23 | |||
| V—Satisfaction | [Measurement I] | 5.17 | 5.60 | 0.91 | T = 4.0256 p = 0.1336 | |
| [Measurement II] | 4.83 | 5.20 | 1.10 | |||
| [Measurement III] | 5.18 | 5.60 | 1.21 | |||
| VI—Pain/discomfort | [Measurement I] | 4.16 | 4.80 | 2.10 | T = 7.9143 p = 0.0191 | |
| [Measurement II] | 3.66 | 4.80 | 2.55 | |||
| [Measurement III] | 4.70 | 5.60 | 2.18 | |||
| Overall FSFI score | [Measurement I] | 27.37 | 30.90 | 9.36 | T = 7.4382 p = 0.0243 | |
| [Measurement II] | 24.52 | 32.80 | 12.69 | |||
| [Measurement III] | 29.00 | 34.90 | 10.99 | |||
| Stoma (A2) | I—Desire | [Measurement I] | 4.30 | 4.20 | 1.40 | T = 4.6944 p = 0.0956 |
| [Measurement II] | 3.83 | 4.20 | 1.47 | |||
| [Measurement III] | 4.62 | 4.80 | 1.58 | |||
| II—Arousal | [Measurement I] | 3.72 | 4.80 | 2.43 | T = 11.5143 p = 0.0032 | |
| [Measurement II] | 1.96 | 2.10 | 2.06 | |||
| [Measurement III] | 2.71 | 2.70 | 2.48 | |||
| III—Lubrication | [Measurement I] | 3.65 | 5.10 | 2.51 | T = 10.5538 p = 0.0051 | |
| [Measurement II] | 1.80 | 0.00 | 2.41 | |||
| [Measurement III] | 2.69 | 2.40 | 2.59 | |||
| IV—Orgasm | [Measurement I] | 3.39 | 4.80 | 2.49 | T = 9.0313 p = 0.0109 | |
| [Measurement II] | 1.70 | 0.00 | 2.36 | |||
| [Measurement III] | 2.64 | 2.40 | 2.56 | |||
| V—Satisfaction | [Measurement I] | 4.75 | 5.60 | 1.45 | T = 5.8611 p = 0.0534 | |
| [Measurement II] | 3.63 | 3.20 | 1.34 | |||
| [Measurement III] | 4.28 | 4.80 | 1.53 | |||
| VI—Pain/discomfort | [Measurement I] | 3.32 | 4.00 | 2.42 | T = 5.7288 p = 0.057 | |
| [Measurement II] | 2.00 | 0.00 | 2.51 | |||
| [Measurement III] | 2.97 | 3.20 | 2.80 | |||
| Overall FSFI score | [Measurement I] | 23.13 | 28.70 | 11.62 | T = 8.5122 p = 0.0142 | |
| [Measurement II] | 14.93 | 9.50 | 10.86 | |||
| [Measurement III] | 19.91 | 18.70 | 12.76 | |||
| Variables Included in the Analysis | r | p | |
|---|---|---|---|
| Weight | FSFI [Measurement I] | −0.0052 | 0.9721 |
| FSFI [Measurement II] | 0.1164 | 0.4309 | |
| FSFI [Measurement III] | 0.0104 | 0.9440 | |
| Height | FSFI [Measurement I] | 0.1487 | 0.3132 |
| FSFI [Measurement II] | 0.0748 | 0.6132 | |
| FSFI [Measurement III] | 0.0803 | 0.5877 | |
| BMI | FSFI [Measurement I] | −0.0920 | 0.5339 |
| FSFI [Measurement II] | 0.1746 | 0.2352 | |
| FSFI [Measurement III] | 0.0368 | 0.8037 | |
| Hospitalization time | FSFI [Measurement I] | −0.1914 | 0.1924 |
| FSFI [Measurement II] | 0.0277 | 0.8518 | |
| FSFI [Measurement III] | 0.0794 | 0.5918 | |
| Parity | FSFI [Measurement I] | 0.0981 | 0.5070 |
| FSFI [Measurement II] | 0.1149 | 0.4367 | |
| FSFI [Measurement III] | 0.0809 | 0.5847 | |
| Age | FSFI [Measurement I] | −0.1521 | 0.3020 |
| FSFI [Measurement II] | −0.3329 | 0.0208 | |
| FSFI [Measurement III] | −0.1246 | 0.3987 | |
| Variables Included in the Analysis | Data Filter | M | Me | SD | Mann–Whitney’s U-Test\Kruskall-Wallis Test |
|---|---|---|---|---|---|
| Type of surgery | |||||
| FSFI [Measurement I] | Anterior resection | 28.09 | 31.50 | 8.89 | H = 9.4569 p = 0.0238 |
| Laparoscopic anterior resection | 26.45 | 30.80 | 10.30 | ||
| abdominoperineal resection | 16.13 | 7.50 | 12.23 | ||
| Hartmann’s procedure | 30.77 | 31.70 | 3.11 | ||
| FSFI [Measurement II] | Anterior resection | 24.64 | 32.80 | 12.44 | H = 6.6092 p = 0.0855 |
| Laparoscopic anterior resection | 24.35 | 32.90 | 13.61 | ||
| abdominoperineal resection | 15.79 | 8.35 | 12.89 | ||
| Hartmann’s procedure | 13.99 | 9.50 | 8.66 | ||
| FSFI [Measurement III] | Anterior resection | 30.11 | 35.35 | 10.70 | H = 11.7098 p = 0.0084 |
| Laparoscopic anterior resection | 27.58 | 34.20 | 11.70 | ||
| abdominoperineal resection | 15.32 | 7.80 | 12.41 | ||
| Hartmann’s procedure | 24.93 | 30.80 | 11.67 | ||
| Neoadjuvant treatment | |||||
| FSFI [Measurement I] | none | 25.90 | 30.40 | 11.24 | H = 2.1982 p = 0.5323 |
| radiotherapy | 22.55 | 28.30 | 11.72 | ||
| chemotherapy | 29.10 | 29.60 | 2.88 | ||
| radiochemotherapy | 27.22 | 31.90 | 9.94 | ||
| FSFI [Measurement II] | none | 24.11 | 32.80 | 12.51 | H = 10.4742 p = 0.0149 |
| radiotherapy | 12.11 | 7.20 | 10.79 | ||
| chemotherapy | 18.60 | 18.70 | 0.56 | ||
| radiochemotherapy | 25.86 | 32.80 | 11.97 | ||
| FSFI [Measurement III] | none | 25.34 | 34.90 | 15.08 | H = 8.1351 p = 0.0433 |
| radiotherapy | 18.64 | 14.45 | 13.02 | ||
| chemotherapy | 22.50 | 18.70 | 7.20 | ||
| radiochemotherapy | 30.66 | 34.85 | 8.89 | ||
| Adjuvant treatment | |||||
| FSFI [Measurement I] | none | 25.04 | 29.80 | 10.91 | H = 0.3516 p = 0.8388 |
| chemotherapy | 25.14 | 30.75 | 11.83 | ||
| radiochemotherapy | 28.33 | 27.80 | 2.82 | ||
| FSFI [Measurement II] | none | 21.61 | 27.35 | 13.03 | H = 2.6381 p = 0.2674 |
| chemotherapy | 16.53 | 8.20 | 13.42 | ||
| radiochemotherapy | 16.60 | 18.35 | 4.03 | ||
| FSFI [Measurement III] | none | 24.70 | 31.95 | 13.13 | H = 0.7292 p = 0.6945 |
| chemotherapy | 24.18 | 30.15 | 13.14 | ||
| radiochemotherapy | 25.60 | 24.75 | 8.54 | ||
| Post-surgical complications | |||||
| FSFI [Measurement I] | none | 25.94 | 30.70 | 10.07 | Z = 0.5549 p = 0.5790 |
| observed | 22.72 | 28.70 | 13.05 | ||
| FSFI [Measurement II] | none | 18.84 | 18.00 | 12.55 | Z = 0.9552 p = 0.3395 |
| observed | 24.60 | 32.80 | 12.91 | ||
| FSFI [Measurement III] | none | 23.46 | 30.80 | 12.99 | Z = 1.2429 p = 0.2139 |
| observed | 29.77 | 32.10 | 9.78 | ||
| Disease staging (I–III) | |||||
| FSFI [Measurement I] | I | 24.69 | 29.10 | 11.04 | H = 3.2311 p = 0.3573 |
| IIA | 25.82 | 30.00 | 10.21 | ||
| IIIB | 28.55 | 32.90 | 11.46 | ||
| IIIC | 25.45 | 29.95 | 10.09 | ||
| FSFI [Measurement II] | I | 23.69 | 32.85 | 13.53 | H = 5.9091 p = 0.1161 |
| IIA | 18.08 | 18.00 | 11.71 | ||
| IIIB | 24.30 | 32.80 | 13.31 | ||
| IIIC | 13.47 | 7.80 | 11.39 | ||
| FSFI [Measurement III] | I | 25.23 | 31.05 | 11.94 | H = 0.4719 p = 0.9250 |
| IIA | 23.40 | 31.10 | 13.18 | ||
| IIIB | 24.37 | 32.45 | 15.07 | ||
| IIIC | 26.58 | 35.05 | 14.08 | ||
| Educational background | |||||
| FSFI [Measurement I] | elementary | 21.10 | 26.00 | 11.05 | H = 3.6209 p = 0.3054 |
| vocational | 27.64 | 30.85 | 8.37 | ||
| secondary | 26.42 | 31.30 | 10.70 | ||
| higher | 23.45 | 30.15 | 12.21 | ||
| FSFI [Measurement II] | elementary | 11.48 | 8.60 | 7.75 | H = 5.9592 p = 0.1136 |
| vocational | 25.56 | 33.00 | 12.54 | ||
| secondary | 21.20 | 23.50 | 12.66 | ||
| higher | 17.42 | 9.00 | 13.70 | ||
| FSFI [Measurement III] | elementary | 22.65 | 24.90 | 12.81 | H = 0.5749 p = 0.9021 |
| vocational | 26.05 | 31.45 | 12.28 | ||
| secondary | 24.87 | 31.10 | 12.86 | ||
| higher | 24.18 | 32.70 | 13.93 | ||
| Area of residence | |||||
| FSFI [Measurement I] | urban | 25.62 | 30.70 | 10.64 | Z = 0.5338 p = 0.5935 |
| rural | 24.59 | 29.50 | 10.92 | ||
| FSFI [Measurement II] | urban | 20.14 | 19.10 | 12.63 | Z = 0.1515 p = 0.8796 |
| rural | 19.35 | 10.60 | 13.33 | ||
| FSFI [Measurement III] | urban | 23.69 | 30.30 | 12.86 | Z = 0.4877 p = 0.6257 |
| rural | 27.23 | 32.90 | 12.01 | ||
| Employment status | |||||
| FSFI [Measurement I] | retired/on disablement pension | 24.58 | 29.60 | 10.92 | H = 1.3071 p = 0.5202 |
| regular employment/company owner | 27.02 | 31.25 | 10.61 | ||
| housekeeping | 30.60 | 30.60 | 1.56 | ||
| FSFI [Measurement II] | retired/on disablement pension | 18.17 | 10.00 | 12.83 | H = 2.9775 p = 0.2257 |
| regular employment/company owner | 25.02 | 28.40 | 11.88 | ||
| housekeeping | 25.95 | 25.95 | 9.69 | ||
| FSFI [Measurement III] | retired/on disablement pension | 25.33 | 31.15 | 12.24 | H = 1.8582 p = 0.3949 |
| regular employment/company owner | 20.51 | 24.15 | 14.49 | ||
| housekeeping | 33.05 | 33.05 | 3.18 | ||
| Marital status | |||||
| FSFI [Measurement I] | married | 27.76 | 31.75 | 9.15 | Z = 2.9533 p = 0.0031 |
| in partnership | 18.07 | 17.35 | 11.74 | ||
| FSFI [Measurement II] | married | 24.04 | 32.00 | 11.89 | Z = 3.8386 p = 0.0001 |
| in partnership | 7.58 | 6.40 | 3.96 | ||
| FSFI [Measurement III] | married | 27.20 | 33.55 | 12.12 | Z = 2.5981 p = 0.0094 |
| in partnership | 16.98 | 14.45 | 11.25 | ||
| Socioeconomic status | |||||
| FSFI [Measurement I] | average | 22.67 | 27.10 | 11.32 | H = 4.3520 p = 0.1135 |
| good | 29.04 | 31.95 | 8.15 | ||
| very good | 19.70 | 19.70 | 20.51 | ||
| FSFI [Measurement II] | average | 16.05 | 9.50 | 11.97 | H = 4.3976 p = 0.1109 |
| good | 22.84 | 28.40 | 12.74 | ||
| very good | 32.70 | 32.70 | 2.12 | ||
| FSFI [Measurement III] | average | 21.61 | 27.60 | 12.89 | H = 3.0044 p = 0.2226 |
| good | 26.90 | 31.50 | 12.20 | ||
| very good | 34.80 | 34.80 | 0.85 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarkowska, M.; Głowacka-Mrotek, I.; Skonieczny, B.; Nowikiewicz, T.; Tarkowski, M.; Jankowski, M.; Zegarski, W.; Jarzemski, P. Sexual Functioning in Female Patients Undergoing Surgical Treatment for Colorectal Cancer—A Single-Center, Prospective Triple Timepoint Yearly Follow-Up. Curr. Oncol. 2022, 29, 3291-3305. https://doi.org/10.3390/curroncol29050269
Tarkowska M, Głowacka-Mrotek I, Skonieczny B, Nowikiewicz T, Tarkowski M, Jankowski M, Zegarski W, Jarzemski P. Sexual Functioning in Female Patients Undergoing Surgical Treatment for Colorectal Cancer—A Single-Center, Prospective Triple Timepoint Yearly Follow-Up. Current Oncology. 2022; 29(5):3291-3305. https://doi.org/10.3390/curroncol29050269
Chicago/Turabian StyleTarkowska, Magdalena, Iwona Głowacka-Mrotek, Bartosz Skonieczny, Tomasz Nowikiewicz, Michał Tarkowski, Michał Jankowski, Wojciech Zegarski, and Piotr Jarzemski. 2022. "Sexual Functioning in Female Patients Undergoing Surgical Treatment for Colorectal Cancer—A Single-Center, Prospective Triple Timepoint Yearly Follow-Up" Current Oncology 29, no. 5: 3291-3305. https://doi.org/10.3390/curroncol29050269
APA StyleTarkowska, M., Głowacka-Mrotek, I., Skonieczny, B., Nowikiewicz, T., Tarkowski, M., Jankowski, M., Zegarski, W., & Jarzemski, P. (2022). Sexual Functioning in Female Patients Undergoing Surgical Treatment for Colorectal Cancer—A Single-Center, Prospective Triple Timepoint Yearly Follow-Up. Current Oncology, 29(5), 3291-3305. https://doi.org/10.3390/curroncol29050269