State of the Art in Combination Immuno/Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis

 , ,
, ,  , and
, and
Abstract
:1. Introduction
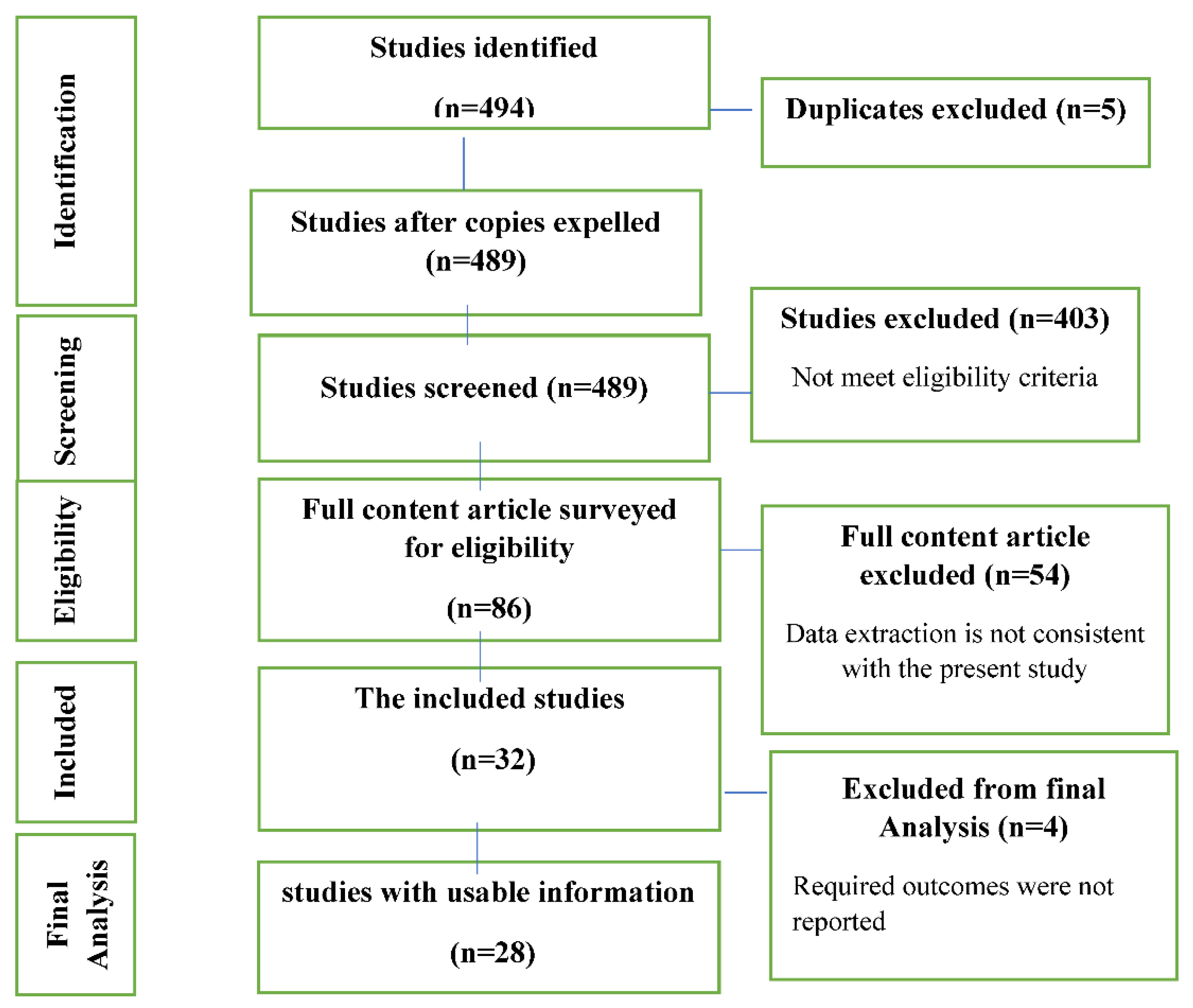
2. Methods
2.1. Search Strategy
2.2. Selection Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Data Extraction and Method of Analysis
3. Results
3.1. Characteristics
3.2. Bias Assessment
4. Toxicity
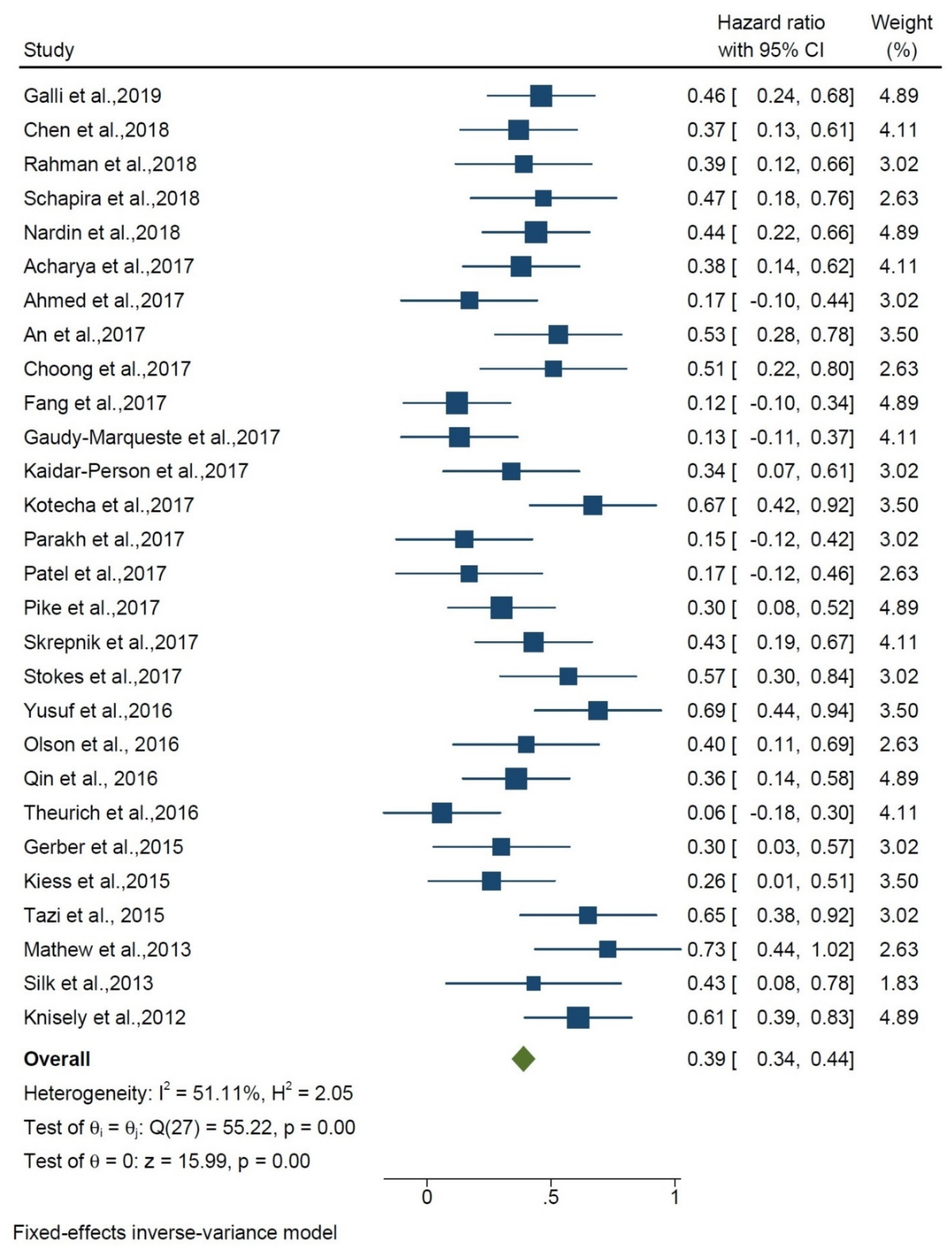
5. Overall Survival of Radiotherapy + Immunotherapy vs. Radiotherapy Alone
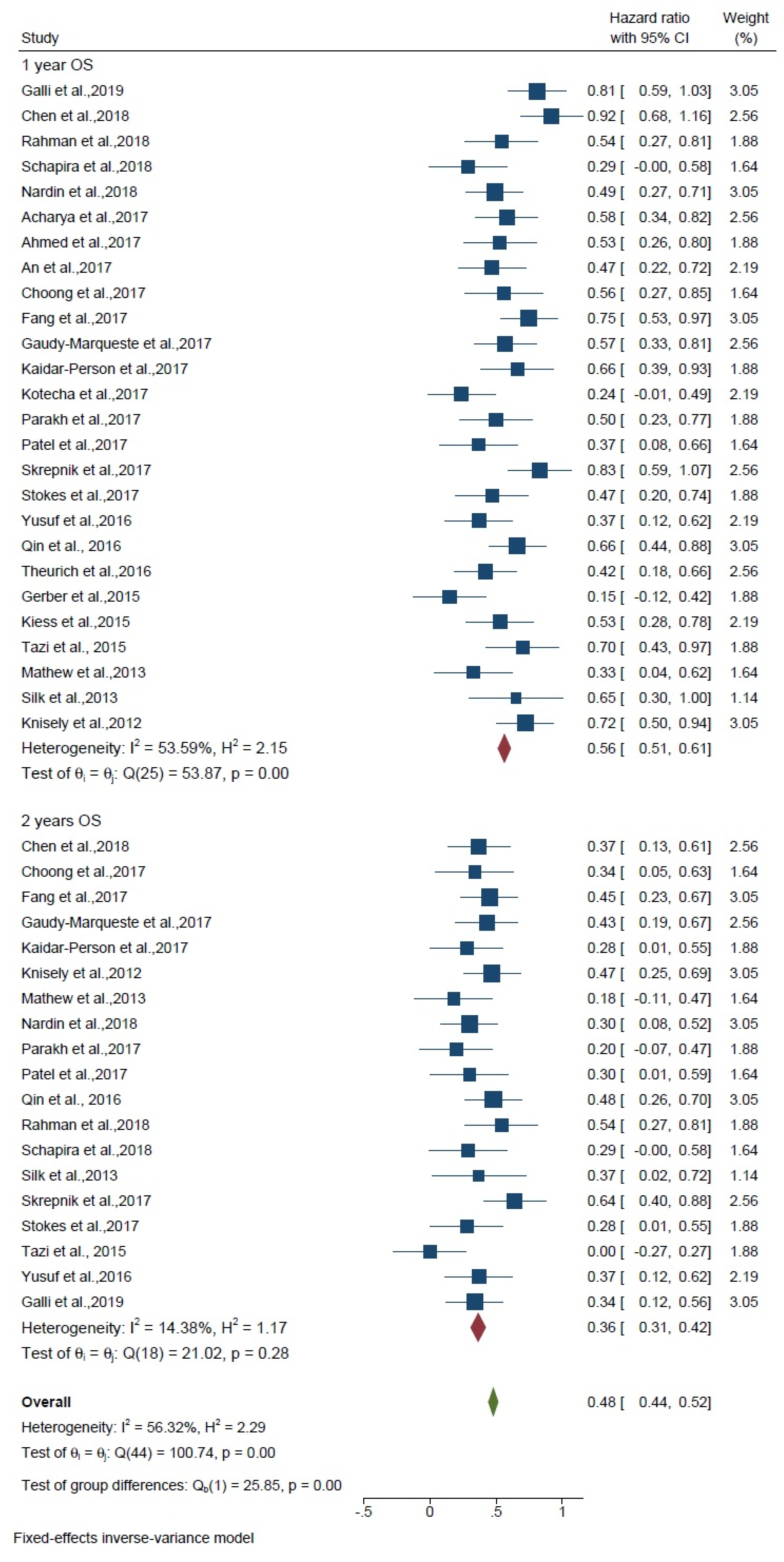
6. Overall Survival of 1 and 2 Years
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kraft, J.; Mayinger, M.; Willmann, J.; Brown, M.; Tanadini-Lang, S.; Wilke, L.; Guckenberger, M.; Andratschke, N. Management of multiple brain metastases: A patterns of care survey within the German Society for Radiation Oncology. J. Neuro-Oncol. 2021, 152, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Tabouret, E.; Chinot, O.; Metellus, P.; Tallet, A.; Viens, P.; Goncalves, A. Recent trends in epidemiology of brain metastases: An overview. Anticancer Res. 2012, 32, 4655–4662. [Google Scholar] [PubMed]
- Woehrer, A. Epidemiology of Nervous System Involvement in Patients with Cancer. Eff. Cancer Treat. Nerv. Syst. 2020, 1, 17. [Google Scholar]
- Iyengar, P.; Kavanagh, B.D.; Wardak, Z.; Smith, I.; Ahn, C.; Gerber, D.E.; Dowell, J.; Hughes, R.; Abdulrahman, R.; Camidge, D.R.; et al. Phase II trial of stereotactic body radiation therapy combined with erlotinib for patients with limited but progressive metastatic non-small-cell lung cancer. J. Clin. Oncol. 2014, 32, 3824–3830. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Kim, I.A. Evolving treatment strategies of brain metastases from breast cancer: Current status and future direction. Ther. Adv. Med. Oncol. 2020, 12, 1758835920936117. [Google Scholar] [CrossRef] [PubMed]
- Tsakonas, G.; De Petris, L.; Ekman, S. Management of brain metastasized non-small cell lung cancer (NSCLC)–From local treatment to new systemic therapies. Cancer Treat. Rev. 2017, 54, 122–131. [Google Scholar] [CrossRef]
- Matsui, Y. Current Multimodality Treatments against Brain Metastases from Renal Cell Carcinoma. Cancers 2020, 12, 2875. [Google Scholar] [CrossRef]
- Torok, J.A.; Salama, J.K. Combining immunotherapy and radiotherapy for the STAR treatment. Nat. Rev. Clin. Oncol. 2019, 16, 666–667. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Frontera, O.A.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; Frontera, O.A.; Melichar, B.; Powles, T.; Donskov, F.; Plimack, E.R.; Barthélémy, P.; Hammers, H.J. Survival outcomes and independent response assessment with nivolumab plus ipilimumab versus sunitinib in patients with advanced renal cell carcinoma: 42-month follow-up of a randomized phase 3 clinical trial. J. Immunother. Cancer 2020, 8, e000891. [Google Scholar] [CrossRef]
- Tannir, N.M.; Signoretti, S.; Choueiri, T.K.; McDermott, D.F.; Motzer, R.J.; Flaifel, A.; Pignon, J.-C.; Ficial, M.; Frontera, O.A.; George, S. Efficacy and safety of nivolumab plus ipilimumab versus sunitinib in first-line treatment of patients with advanced sarcomatoid renal cell carcinoma. Clin. Cancer Res. 2021, 27, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Gettinger, S.; Horn, L.; Jackman, D.; Spigel, D.; Antonia, S.; Hellmann, M.; Powderly, J.; Heist, R.; Sequist, L.V.; Smith, D.C. Five-year follow-up of nivolumab in previously treated advanced non–small-cell lung cancer: Results from the CA209-003 study. J. Clin. Oncol. 2018, 36, 1675–1684. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.; Duan, Q.; Lei, G.; Liu, Z. A Rare EGFR R748T Mutation in a Squamous Cell Lung Carcinoma Patient with PD-L1 High Expression and Response to Immuno-Chemo Combination Therapy. 2020. Available online: https://www.researchsquare.com/article/rs-68851/v1 (accessed on 3 April 2022).
- Goldberg, S.B.; Gettinger, S.N.; Mahajan, A.; Chiang, A.C.; Herbst, R.S.; Sznol, M.; Tsiouris, A.J.; Cohen, J.; Vortmeyer, A.; Jilaveanu, L. Pembrolizumab for patients with melanoma or non-small-cell lung cancer and untreated brain metastases: Early analysis of a non-randomised, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 976–983. [Google Scholar] [CrossRef] [Green Version]
- Long, G.V.; Atkinson, V.; Lo, S.; Sandhu, S.; Guminski, A.D.; Brown, M.P.; Wilmott, J.S.; Edwards, J.; Gonzalez, M.; Scolyer, R.A. Combination nivolumab and ipilimumab or nivolumab alone in melanoma brain metastases: A multicentre randomised phase 2 study. Lancet Oncol. 2018, 19, 672–681. [Google Scholar] [CrossRef]
- Trino, E.; Mantovani, C.; Badellino, S.; Ricardi, U.; Filippi, A.R. Radiosurgery/stereotactic radiotherapy in combination with immunotherapy and targeted agents for melanoma brain metastases. Expert Rev. Anticancer Ther. 2017, 17, 347–356. [Google Scholar] [CrossRef]
- Weichselbaum, R.R.; Liang, H.; Deng, L.; Fu, Y.-X. Radiotherapy and immunotherapy: A beneficial liaison? Nat. Rev. Clin. Oncol. 2017, 14, 365. [Google Scholar] [CrossRef]
- Demaria, S.; Bhardwaj, N.; McBride, W.H.; Formenti, S.C. Combining radiotherapy and immunotherapy: A revived partnership. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 655–666. [Google Scholar] [CrossRef] [Green Version]
- Dahl, O.; Dale, J.E.; Brydøy, M. Rationale for combination of radiation therapy and immune checkpoint blockers to improve cancer treatment. Acta Oncol. 2019, 58, 9–20. [Google Scholar] [CrossRef] [Green Version]
- van Vulpen, M.; Kal, H.B.; Taphoorn, M.J.; El Sharouni, S.Y. Changes in blood-brain barrier permeability induced by radiotherapy: Implications for timing of chemotherapy? Oncol. Rep. 2002, 9, 683–688. [Google Scholar] [CrossRef] [Green Version]
- Khalifa, J.; Amini, A.; Popat, S.; Gaspar, L.E.; Faivre-Finn, C. Brain metastases from NSCLC: Radiation therapy in the era of targeted therapies. J. Thorac. Oncol. 2016, 11, 1627–1643. [Google Scholar] [CrossRef] [Green Version]
- He, Z.-Y.; Li, M.-F.; Lin, J.-H.; Lin, D.; Lin, R.-J. Comparing the efficacy of concurrent EGFR-TKI and whole-brain radiotherapy vs EGFR-TKI alone as a first-line therapy for advanced EGFR-mutated non-small-cell lung cancer with brain metastases: A retrospective cohort study. Cancer Manag. Res. 2019, 11, 2129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franceschini, D.; Franzese, C.; Navarria, P.; Ascolese, A.M.; De Rose, F.; Del Vecchio, M.; Santoro, A.; Scorsetti, M. Radiotherapy and immunotherapy: Can this combination change the prognosis of patients with melanoma brain metastases? Cancer Treat. Rev. 2016, 50, 1–8. [Google Scholar] [CrossRef]
- Galli, G.; Cavalieri, S.; Di Guardo, L.; Cimminiello, C.; Nichetti, F.; Corti, F.; Garcia, M.A.; Pappalardi, B.; Fallai, C.; De Braud, F. Combination of immunotherapy and brain radiotherapy in metastatic melanoma: A retrospective analysis. Oncol. Res. Treat. 2019, 42, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement (Chinese edition). J. Chin. Integr. Med. 2009, 7, 889–896. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 3 April 2022).
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Douglass, J.; Kleinberg, L.; Ye, X.; Marciscano, A.E.; Forde, P.M.; Brahmer, J.; Lipson, E.; Sharfman, W.; Hammers, H. Concurrent immune checkpoint inhibitors and stereotactic radiosurgery for brain metastases in non-small cell lung cancer, melanoma, and renal cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 916–925. [Google Scholar] [CrossRef]
- Diao, K.; Bian, S.X.; Routman, D.M.; Yu, C.; Kim, P.E.; Wagle, N.A.; Wong, M.K.; Zada, G.; Chang, E.L. Combination ipilimumab and radiosurgery for brain metastases: Tumor, edema, and adverse radiation effects. J. Neurosurg. 2018, 129, 1397–1406. [Google Scholar] [CrossRef] [Green Version]
- Hubbeling, H.G.; Schapira, E.F.; Horick, N.K.; Goodwin, K.E.; Lin, J.J.; Oh, K.S.; Shaw, A.T.; Mehan, W.A.; Shih, H.A.; Gainor, J.F. Safety of combined PD-1 pathway inhibition and intracranial radiation therapy in non–small cell lung cancer. J. Thorac. Oncol. 2018, 13, 550–558. [Google Scholar] [CrossRef] [Green Version]
- Rahman, R.; Cortes, A.; Niemierko, A.; Oh, K.S.; Flaherty, K.T.; Lawrence, D.P.; Sullivan, R.J.; Shih, H.A. The impact of timing of immunotherapy with cranial irradiation in melanoma patients with brain metastases: Intracranial progression, survival and toxicity. J. Neuro-Oncol. 2018, 138, 299–306. [Google Scholar] [CrossRef]
- Schapira, E.; Hubbeling, H.; Yeap, B.Y.; Mehan, W.A., Jr.; Shaw, A.T.; Oh, K.; Gainor, J.F.; Shih, H.A. Improved overall survival and locoregional disease control with concurrent PD-1 pathway inhibitors and stereotactic radiosurgery for lung cancer patients with brain metastases. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 624–629. [Google Scholar] [CrossRef]
- Nardin, C.; Mateus, C.; Texier, M.; Lanoy, E.; Hibat-Allah, S.; Ammari, S.; Robert, C.; Dhermain, F. Tolerance and outcomes of stereotactic radiosurgery combined with anti-programmed cell death-1 (pembrolizumab) for melanoma brain metastases. Melanoma Res. 2018, 28, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Mahmood, M.; Mullen, D.; Yang, D.; Tsien, C.I.; Huang, J.; Perkins, S.M.; Rich, K.; Chicoine, M.; Leuthardt, E. Distant intracranial failure in melanoma brain metastases treated with stereotactic radiosurgery in the era of immunotherapy and targeted agents. Adv. Radiat. Oncol. 2017, 2, 572–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, K.A.; Kim, S.; Arrington, J.; Naghavi, A.O.; Dilling, T.J.; Creelan, B.C.; Antonia, S.J.; Caudell, J.J.; Harrison, L.B.; Sahebjam, S. Outcomes targeting the PD-1/PD-L1 axis in conjunction with stereotactic radiation for patients with non-small cell lung cancer brain metastases. J. Neuro-Oncol. 2017, 133, 331–338. [Google Scholar] [CrossRef] [PubMed]
- An, Y.; Jiang, W.; Kim, B.Y.; Qian, J.M.; Tang, C.; Fang, P.; Logan, J.; D’Souza, N.M.; Haydu, L.E.; Wang, X.A. Stereotactic radiosurgery of early melanoma brain metastases after initiation of anti-CTLA-4 treatment is associated with improved intracranial control. Radiother. Oncol. 2017, 125, 80–88. [Google Scholar] [CrossRef]
- Anderson, E.S.; Postow, M.A.; Wolchok, J.D.; Young, R.J.; Ballangrud, Å.; Chan, T.A.; Yamada, Y.; Beal, K. Melanoma brain metastases treated with stereotactic radiosurgery and concurrent pembrolizumab display marked regression; efficacy and safety of combined treatment. J. Immunother. Cancer 2017, 5, 76. [Google Scholar] [CrossRef] [Green Version]
- Choong, E.S.; Lo, S.; Drummond, M.; Fogarty, G.B.; Menzies, A.M.; Guminski, A.; Shivalingam, B.; Clarke, K.; Long, G.V.; Hong, A.M. Survival of patients with melanoma brain metastasis treated with stereotactic radiosurgery and active systemic drug therapies. Eur. J. Cancer 2017, 75, 169–178. [Google Scholar] [CrossRef]
- Fang, P.; Jiang, W.; Allen, P.; Glitza, I.; Guha, N.; Hwu, P.; Ghia, A.; Phan, J.; Mahajan, A.; Tawbi, H. Radiation necrosis with stereotactic radiosurgery combined with CTLA-4 blockade and PD-1 inhibition for treatment of intracranial disease in metastatic melanoma. J. Neuro-Oncol. 2017, 133, 595–602. [Google Scholar] [CrossRef]
- Gaudy-Marqueste, C.; Dussouil, A.; Carron, R.; Troin, L.; Malissen, N.; Loundou, A.; Monestier, S.; Mallet, S.; Richard, M.; Regis, J. Survival of melanoma patients treated with targeted therapy and immunotherapy after systematic upfront control of brain metastases by radiosurgery. Eur. J. Cancer 2017, 84, 44–54. [Google Scholar] [CrossRef]
- Kaidar-Person, O.; Zagar, T.M.; Deal, A.; Moschos, S.J.; Ewend, M.G.; Sasaki-Adams, D.; Lee, C.B.; Collichio, F.A.; Fried, D.; Marks, L.B. The incidence of radiation necrosis following stereotactic radiotherapy for melanoma brain metastases: The potential impact of immunotherapy. Anti-Cancer Drugs 2017, 28, 669–675. [Google Scholar] [CrossRef]
- Kotecha, R.; Miller, J.A.; Venur, V.A.; Mohammadi, A.M.; Chao, S.T.; Suh, J.H.; Barnett, G.H.; Murphy, E.S.; Funchain, P.; Jennifer, S.Y. Melanoma brain metastasis: The impact of stereotactic radiosurgery, BRAF mutational status, and targeted and/or immune-based therapies on treatment outcome. J. Neurosurg. 2017, 129, 50–59. [Google Scholar] [CrossRef] [Green Version]
- Parakh, S.; Park, J.J.; Mendis, S.; Rai, R.; Xu, W.; Lo, S.; Drummond, M.; Rowe, C.; Wong, A.; McArthur, G. Efficacy of anti-PD-1 therapy in patients with melanoma brain metastases. Br. J. Cancer 2017, 116, 1558–1563. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, K.R.; Shoukat, S.; Oliver, D.E.; Chowdhary, M.; Rizzo, M.; Lawson, D.H.; Khosa, F.; Liu, Y.; Khan, M.K. Ipilimumab and stereotactic radiosurgery versus stereotactic radiosurgery alone for newly diagnosed melanoma brain metastases. Am. J. Clin. Oncol. 2017, 40, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Pike, L.R.; Bang, A.; Ott, P.; Balboni, T.; Taylor, A.; Catalano, P.; Rawal, B.; Spektor, A.; Krishnan, M.; Cagney, D. Radiation and PD-1 inhibition: Favorable outcomes after brain-directed radiation. Radiother. Oncol. 2017, 124, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Skrepnik, T.; Sundararajan, S.; Cui, H.; Stea, B. Improved time to disease progression in the brain in patients with melanoma brain metastases treated with concurrent delivery of radiosurgery and ipilimumab. Oncoimmunology 2017, 6, e1283461. [Google Scholar] [CrossRef] [Green Version]
- Stokes, W.A.; Binder, D.C.; Jones, B.L.; Oweida, A.J.; Liu, A.K.; Rusthoven, C.G.; Karam, S.D. Impact of immunotherapy among patients with melanoma brain metastases managed with radiotherapy. J. Neuroimmunol. 2017, 313, 118–122. [Google Scholar] [CrossRef]
- Yusuf, M.B.; Amsbaugh, M.J.; Burton, E.; Chesney, J.; Woo, S. Peri-SRS administration of immune checkpoint therapy for melanoma metastatic to the brain: Investigating efficacy and the effects of relative treatment timing on lesion response. World Neurosurg. 2017, 100, 632–640.e4. [Google Scholar] [CrossRef]
- Liniker, E.; Menzies, A.; Kong, B.; Cooper, A.; Ramanujam, S.; Lo, S.; Kefford, R.; Fogarty, G.; Guminski, A.; Wang, T. Activity and safety of radiotherapy with anti-PD-1 drug therapy in patients with metastatic melanoma. Oncoimmunology 2016, 5, e1214788. [Google Scholar] [CrossRef]
- Olson, A.C.; Thomas, S.; Qin, R.; Singh, B.; Salama, J.K.; Kirkpatrick, J.; Salama, A.K. Outcomes and toxicity of stereotactic radiosurgery for melanoma brain metastases in patients receiving ipilimumab. Melanoma Manag. 2016, 3, 177–186. [Google Scholar] [CrossRef]
- Qin, R.; Olson, A.; Singh, B.; Thomas, S.; Wolf, S.; Bhavsar, N.A.; Hanks, B.A.; Salama, J.K.; Salama, A.K. Safety and efficacy of radiation therapy in advanced melanoma patients treated with ipilimumab. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 72–77. [Google Scholar] [CrossRef]
- Theurich, S.; Rothschild, S.I.; Hoffmann, M.; Fabri, M.; Sommer, A.; Garcia-Marquez, M.; Thelen, M.; Schill, C.; Merki, R.; Schmid, T. Local tumor treatment in combination with systemic ipilimumab immunotherapy prolongs overall survival in patients with advanced malignant melanoma. Cancer Immunol. Res. 2016, 4, 744–754. [Google Scholar] [CrossRef] [Green Version]
- Gerber, N.K.; Young, R.J.; Barker, C.A.; Wolchok, J.D.; Chan, T.A.; Yamada, Y.; Friguglietti, L.; Beal, K. Ipilimumab and whole brain radiation therapy for melanoma brain metastases. J. Neuro-Oncol. 2015, 121, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Kiess, A.P.; Wolchok, J.D.; Barker, C.A.; Postow, M.A.; Tabar, V.; Huse, J.T.; Chan, T.A.; Yamada, Y.; Beal, K. Stereotactic radiosurgery for melanoma brain metastases in patients receiving ipilimumab: Safety profile and efficacy of combined treatment. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 368–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tazi, K.; Hathaway, A.; Chiuzan, C.; Shirai, K. Survival of melanoma patients with brain metastases treated with ipilimumab and stereotactic radiosurgery. Cancer Med. 2015, 4, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mathew, M.; Tam, M.; Ott, P.A.; Pavlick, A.C.; Rush, S.C.; Donahue, B.R.; Golfinos, J.G.; Parker, E.C.; Huang, P.P.; Narayana, A. Ipilimumab in melanoma with limited brain metastases treated with stereotactic radiosurgery. Melanoma Res. 2013, 23, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Silk, A.W.; Bassetti, M.F.; West, B.T.; Tsien, C.I.; Lao, C.D. Ipilimumab and radiation therapy for melanoma brain metastases. Cancer Med. 2013, 2, 899–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knisely, J.P.; James, B.Y.; Flanigan, J.; Sznol, M.; Kluger, H.M.; Chiang, V.L. Radiosurgery for melanoma brain metastases in the ipilimumab era and the possibility of longer survival. J. Neurosurg. 2012, 117, 227–233. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Jiang, W.; Brown, P.D.; Braunstein, S.; Sneed, P.; Wattson, D.A.; Shih, H.A.; Bangdiwala, A.; Shanley, R.; Lockney, N.A. Estimating survival in melanoma patients with brain metastases: An update of the graded prognostic assessment for melanoma using molecular markers (Melanoma-molGPA). Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 812–816. [Google Scholar] [CrossRef] [Green Version]
- Fertil, B.; Malaise, E.P. Intrinsic radiosensitivity of human cell lines is correlated with radioresponsiveness of human tumors: Analysis of 101 published survival curves. Int. J. Radiat. Oncol. Biol. Phys. 1985, 11, 1699–1707. [Google Scholar] [CrossRef]
- Manon, R.; O’Neill, A.; Knisely, J.; Werner-Wasik, M.; Lazarus, H.M.; Wagner, H.; Gilbert, M.; Mehta, M.; Eastern Cooperative Oncology Group. Phase II trial of radiosurgery for one to three newly diagnosed brain metastases from renal cell carcinoma, melanoma, and sarcoma: An Eastern Cooperative Oncology Group study (E 6397). J. Clin. Oncol. 2005, 23, 8870–8876. [Google Scholar] [CrossRef]
- Téglási, V.; Pipek, O.; Lózsa, R.; Berta, K.; Szüts, D.; Harkó, T.; Vadász, P.; Rojkó, L.; Döme, B.; Bagó, A.G. PD-L1 expression of lung cancer cells, unlike infiltrating immune cells, is stable and unaffected by therapy during brain metastasis. Clin. Lung Cancer 2019, 20, 363–369.e2. [Google Scholar] [CrossRef]
- Takamori, S.; Toyokawa, G.; Okamoto, I.; Takada, K.; Kinoshita, F.; Kozuma, Y.; Matsubara, T.; Haratake, N.; Akamine, T.; Mukae, N. Clinical significance of PD-L1 expression in brain metastases from non-small cell lung cancer. Anticancer Res. 2018, 38, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, D.; De Rose, F.; Cozzi, S.; Franzese, C.; Rossi, S.; Finocchiaro, G.; Toschi, L.; Santoro, A.; Scorsetti, M. The use of radiation therapy for oligoprogressive/oligopersistent oncogene-driven non small cell lung cancer: State of the art. Crit. Rev. Oncol. Hematol. 2020, 148, 102894. [Google Scholar] [CrossRef] [PubMed]
- Belgioia, L.; Desideri, I.; Errico, A.; Franzese, C.; Daidone, A.; Marino, L.; Fiore, M.; Borghetti, P.; Greto, D.; Fiorentino, A.; et al. Safety and efficacy of combined radiotherapy, immunotherapy and targeted agents in elderly patients: A literature review. Crit. Rev. Oncol. Hematol. 2019, 133, 163–170. [Google Scholar] [CrossRef]
- Diao, K.; Bian, S.X.; Routman, D.M.; Yu, C.; Ye, J.C.; Wagle, N.A.; Wong, M.K.; Zada, G.; Chang, E.L. Stereotactic radiosurgery and ipilimumab for patients with melanoma brain metastases: Clinical outcomes and toxicity. J. Neurooncol. 2018, 139, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.M.; Yu, J.B.; Kluger, H.M.; Chiang, V.L. Timing and type of immune checkpoint therapy affect the early radiographic response of melanoma brain metastases to stereotactic radiosurgery. Cancer 2016, 122, 3051–3058. [Google Scholar] [CrossRef] [Green Version]
- Bardoscia, L.; Pasinetti, N.; Triggiani, L.; Cozzi, S.; Sardaro, A. Biological Bases of Immune-Related Adverse Events and Potential Crosslinks With Immunogenic Effects of Radiation. Front. Pharmacol. 2021, 12, 746853. [Google Scholar] [CrossRef]
- Trapani, S.; Manicone, M.; Sikokis, A.; D’Abbiero, N.; Salaroli, F.; Ceccon, G.; Buti, S. Effectiveness and safety of “real” concurrent stereotactic radiotherapy and immunotherapy in metastatic solid tumors: A systematic review. Crit. Rev. Oncol. Hematol. 2019, 142, 9–15. [Google Scholar] [CrossRef]
- Lehrer, E.J.; Peterson, J.; Brown, P.D.; Sheehan, J.P.; Quinones-Hinojosa, A.; Zaorsky, N.G.; Trifiletti, D.M. Treatment of brain metastases with stereotactic radiosurgery and immune checkpoint inhibitors: An international meta-analysis of individual patient data. Radiother Oncol. 2019, 130, 104–112. [Google Scholar] [CrossRef]
- Petrelli, F.; De Stefani, A.; Trevisan, F.; Parati, C.; Inno, A.; Merelli, B.; Ghidini, M.; Bruschieri, L.; Vitali, E.; Cabiddu, M. Combination of radiotherapy and immunotherapy for brain metastases: A systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2019, 144, 102830. [Google Scholar] [CrossRef]
- Rulli, E.; Legramandi, L.; Salvati, L.; Mandala, M. The impact of targeted therapies and immunotherapy in melanoma brain metastases: A systematic review and meta-analysis. Cancer 2019, 125, 3776–3789. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N | Study. Years | Study Design | Number of Patients | Mean Age | Primary Tumor | Average Number of Metastases (% of Patients) | Size | Overall Response Rate of Brain Metastases * (%) |
|---|---|---|---|---|---|---|---|---|
| 1 | Galli et al., 2019 [24] | R | 36 | 59 | Melanoma | 8 | NR | NR |
| 2 | Chen et al., 2018 [28] | R | 79 | 59 | NSCLC, Melanoma Kidney | 2 | NR | NR |
| 3 | Diao et al., 2018 [29] | R | 59 | 61 | Melanoma | NR | NR | 76 |
| 4 | Hubbeling et al., 2018 [30] | R | 50 | 61 | NSCLC | 1: 60%; >3: 40% | MLD: 13 mm | NR |
| 5 | Rahman et al., 2018 [31] | R | 35 | 66.7 | Melanoma | 2 | MD: 9 mm | NR |
| 6 | Schapira et al., 2018 [32] | R | 37 | 63 | NSCLC | NR | MD: 6 mm | NR |
| 7 | Nardin et al., 2018 [33] | R | 25 | 58 | Melanoma | NR | MD: 16 mm | 36 |
| 8 | Acharya et al., 2017 [34] | R | 18 | 61 | Melanoma | NR | MV: 362 mm3 | NR |
| 9 | Ahmed et al., 2017 [35] | R | 17 | 60 | NSCLC | NR | NR | NR |
| 10 | An et al., 2017 [36] | R | 99 | 62 | Melanoma | 2 | MV: 1.45 mm3 | NR |
| 11 | Anderson et al., 2017 [37] | R | 21 | 67 | Melanoma | 1.5 | MD: 10 mm | 32 |
| 12 | Choong et al., 2017 [38] | R | 39 | 64 | Melanoma | 2 | NR | NR |
| 13 | Fang et al., 2017 [39] | R | 137 | 57 | Melanoma | MV: 122 mm3 | NR | |
| 14 | Gaudy-Marqueste et al., 2017 [40] | R | 56 | 54.3 | Melanoma | 1: 30.3%; >3: 43.5% | NR | NR |
| 15 | Kaidar-Person et al., 2017 [41] | R | 29 | 57 | Melanoma | NR | MLD: 15 mm | NR |
| 16 | Kotecha et al., 2017 [42] | R | 32 | 57 | Melanoma | 1: 34%; >3: 34% | MD: 9 mm | NR |
| 17 | Parakh et al., 2017 [43] | R | 66 | 62 | Melanoma | 1: 10%; 2–4: 52%; >4: 38% | MSD: 23.5 mm | 29 |
| 18 | Patel et al., 2017 [44] | R | 20 | 56.5 | Melanoma | 1–3: 90%; ≥3: 10% | NR | NR |
| 19 | Pike et al., 2017 [45] | R | 85 | 63 | NSCLC Melanoma RCC | NR | NR | NR |
| 20 | Skrepnik et al., 2017 [46] | R | 25 | 68.5 | Melanoma | NR | NR | 4 |
| 21 | Stokes et al., 2017 [47] | R | 185 | Melanoma | NR | NR | NR | |
| 22 | Yusuf et al., 2016 [48] | R | 18 | 63.8 | Melanoma | NR | MD: 7.9 mm | NR |
| 23 | Liniker et al., 2016 [49] | R | 27 | 63 | Melanoma | 7 | 33 | |
| 24 | Olson et al., 2016 [50] | R | 26 | 63 | Melanoma | NR | NR | NR |
| 25 | Qin et al., 2016 [51] | R | 44 | 58 | Melanoma | NR | NR | 64.5 |
| 26 | Theurich et al., 2016 [52] | R | 46 | 62 | Melanoma | NR | NR | NR |
| 27 | Gerber et al., 2015 [53] | R | 13 | 64 | Melanoma | NR | NR | 11 |
| 28 | Kiess et al., 2015 [54] | R | 46 | 57 | Melanoma | NR | MD: 8 mm | 75 |
| 29 | Tazi et al., 2015 [55] | R | 10 | 65 | Melanoma | NR | NR | NR |
| 30 | Mathew et al., 2013 [56] | R | 25 | 62 | Melanoma | >1: 84%; >4: 24% | MV: 0.6 mm3 | NR |
| 31 | Silk et al., 2013 [57] | R | 33 | 56 | Melanoma | 1–3 | NR | 27 |
| 32 | Knisely et al., 2012 [58] | R | 27 | 53 | Melanoma | NR | NR | NR |
| N | Study. Years | Radiotherapy Type (%) | Dose (Gy) | Timing Radiotherapy (%) | Immunotherapy Drug | Number of Cycles | Main Toxicities (%) |
|---|---|---|---|---|---|---|---|
| 1 | Galli et al., 2019 [24] | SRS WBRT | SRS: 20–24 WBRT: 30 | Concurrent: 100 | Anti-CTLA4: 36 Anti-PD1: 4 BRAFi ± MEKi: 28 | NR | NR |
| 2 | Chen et al., 2018 [28] | SRS (100) | 20 | Concurrent: 100 | PI, NIVO or PEMBRO: NR | NR | Radionecrosis (3) |
| 3 | Diao et al., 2018 [29] | SRS (100) | 20 | Concurrent: 100 | IPI: 100 | 4 | Radionecrosis (2), hemorrhage (18) |
| 4 | Hubbeling et al., 2018 [30] | WBRT (58) or PBI (16) or SRS (70) | 30 | Before: 60 | NIVO: 78; PEMBRO: 16; ATEZO: 8 | 9 | Overall G3-4 (9) (SRS) & (10) (WBRT); |
| 5 | Rahman et al., 2018 [31] | SRS (100) | 18 | 100: concurrent | IPI: 68; PEMBRO: 20; IPI + NIVO: 6; NIVO: 3; Other: 3 | NR | Radionecrosis (14.3) |
| 6 | Schapira et al., 2018 [32] | SRS (100) | 18 | NIVO: 83.8 | 7 | G3: ataxia (4.2), headache (4.2) | |
| 7 | Nardin et al., 2018 [33] | SRS (100) | 20 | Before: 36 Concurrent: 38 After: 26 | PEMBRO: 100 | NR | G3 radionecrosis (12) |
| 8 | Acharya et al., 2017 [34] | SRS: 100 | 20 | Concurrent: 6 After: 94 | NIVO, PEMBRO or IPI: NR | 4 | Radionecrosis: 1 |
| 9 | Ahmed et al., 2017 [35] | SRS: 82 SRT: 18 | SRS: 20 SRT: 25 | Before: 47 Concurrent: 27 After: 26 | NIVO: 65 DURVALUMAB: 35 | NR | NR |
| 10 | An et al., 2017 [36] | SRS: 100 | 20 | After: 100 | IPI: 100 PEMBRO: 100 | NR | NR |
| 11 | Anderson et al.,2017 [37] | WBRT (14); SRS (52); Post surgery (33) | 30 | Concurrent: 100 | PEMBRO: 100 | 4 | NR |
| 12 | Choong et al., 2017 [38] | WBRT (38.9) SRS (73.1) | NR | Concurrent: 100 | IPI: 72; anti-PD-1: 28 | NR | Radionecrosis (2.8) |
| 13 | Fang et al., 2017 [39] | SRS or WBRT + SRS (100) | 20 | Before: 39 | IPI: 87; PEMBRO: 9; | NR | Radionecrosis (27) |
| 14 | Gaudy-Marqueste et al., 2017 [40] | SRS (100) | NR | After: 61 Before: 47 | IPI: 49; PEMBRO: 40 | NR | NR |
| 15 | Kaidar-Person et al., 2017 [41] | SRS (100) | 21 | Before: 55 | IPI: 65.5 | NR | Radionecrosis (27.6); hemorrhage (24) |
| 16 | Kotecha et al., 2017 [42] | SRS (100) | NR | Before: 100 | PD-1 or IPI: 100 | NR | Radionecrosis (2) |
| 17 | Parakh et al., 2017 [43] | SRS (23) WBRT(30) Chir + RT (46) | NR | Before: 100 | NIVO, PEMBRO: NR | NR | NR |
| 18 | Patel et al., 2017 [44] | SRS (100) | 20 | Before: 35 Concurrent: 5 After: 60 | IPI: 100 | NR | Radionecrosis (30) |
| 19 | Pike et al., 2017 [45] | WBRT (36) SRS (73) | WBRT: 30 SRS: 20 | Before: 78 After: 59 | PEMBRO, NIVO or IPI: NR | 2 | NR |
| 20 | Skrepnik et al., 2017 [46] | SRS (100) | 21 | NR | IPI: 100 | 4 | NR |
| 21 | Stokes et al., 2017 [47] | SRS (50.3), WBRT (49.7) | NR | Not specified | NR | NR | |
| 22 | Yusuf et al., 2016 [48] | SRS (100); WBRT (5.6) | 18 | Concurrent or after: 39 Before: 61 | Anti-PD-1: 72 IPI: 28 | NR | Radionecrosis (3.4) |
| 23 | Liniker et al., 2016 [49] | WBRT (78) SRS (22) | WBRT: 30 SRS: NR | Concurrent: 52 | NIVO: 20 | NR | G ≥ 3–4 (WBRT): cognitive changes (5), Stevens–Johnson syndrome (5), nausea (5), rash (10) |
| 24 | Olson et al., 2016 [50] | SRS (100) | 20 | Before or Concurrent: 54 After: 46 | IPI: 100 | 4 | G3 CNS toxicities (11), radionecrosis (7) |
| 25 | Qin et al., 2016 [51] | SRS (100) | 20 | Before: 100 | IPI: 100 | >1 | Dermatologic (27), gastrointestinal (18), fatigue (11), nausea (9), anorexia (5) |
| 26 | Theurich et al., 2016 [52] | WBRT (62); SRS (62) | 30 (WBRT); 20 (SRS) | NR | IPI: 89 (11 received RT in other sites + SNC RT) | 4 | Overall G3-4 (0) |
| 28 | Gerber et al., 2015 [53] | WBRT (100) | 30 | Before: 23 Concurrent: 46 After: 53 | IPI: 100 | 4 | G3-4 Cognitive changes (8) |
| 29 | Kiess et al., 2015 [54] | SRS (100) | 21 | Before: 41 Concurrent: 33 | PI: 100 | NR | Radionecrosis (11) |
| 30 | Tazi et al., 2015 [55] | SRS (100) | Before or Concurrent: 100 | IPI: 100 | 4 | Overall G3-4 (10); | |
| 31 | Mathew et al., 2013 [56] | SRS (100) | 20 | Before: 16 | IPI: 100 | 4 | Intracranial hemorrhage (28), radionecrosis (0) |
| 32 | Silk et al., 2013 [57] | WBRT (48.5) SRS (51.5) | NR | Before: 64 After: 36 | IPI: 100 | NR | NR |
| 33 | Knisely et al., 2012 [58] | SRS (100) SRS (100) | NR | 26: SRS after IT 41: SRS after IT 59: SRS before IT | IPI: 100 | NR | Radionecrosis (11) |
| Study. Years | Selection (5 Score) | Comparability (2 Score) | Outcome (2 Score) | Total Score | ||||
|---|---|---|---|---|---|---|---|---|
| Representative Sample | Sample Size | No Respondents | Ascertainment of the Exposure | Based on Design and Analysis | Assessment of Outcome | Statistical Test | ||
| Galli et al., 2019 [24] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| Chen et al., 2018 [28] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| Diao et al., 2018 [29] | 1 | 1 | 0 | 2 | 2 | 1 | 1 | 8 |
| Hubbeling et al., 2018 [30] | 1 | 1 | 0 | 0 | 2 | 1 | 0 | 5 |
| Rahman et al., 2018 [31] | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 8 |
| Schapira et al., 2018 [32] | 1 | 1 | 0 | 1 | 2 | 1 | 0 | 6 |
| Nardin et al., 2018 [33] | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 5 |
| Acharya et al., 2017 [34] | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 6 |
| Ahmed et al., 2017 [35] | 1 | 1 | 0 | 0 | 2 | 1 | 0 | 5 |
| An et al., 2017 [36] | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 5 |
| Anderson et al., 2017 [37] | 1 | 1 | 0 | 2 | 2 | 1 | 1 | 8 |
| Choong et al., 2017 [38] | 1 | 1 | 0 | 2 | 2 | 1 | 0 | 7 |
| Fang et al., 2017 [39] | 1 | 1 | 0 | 2 | 2 | 1 | 1 | 8 |
| Gaudy-Marqueste et al., 2017 [40] | 1 | 1 | 0 | 2 | 2 | 1 | 1 | 8 |
| Kaidar-Person et al., 2017 [41] | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 6 |
| Kotecha et al., 2017 [42] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 6 |
| Parakh et al., 2017 [43] | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 6 |
| Patel et al., 2017 [44] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Pike et al., 2017 [45] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 7 |
| Skrepnik et al., 2017 [46] | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 6 |
| Stokes et al., 2017 [47] | 1 | 1 | 0 | 2 | 2 | 1 | 1 | 8 |
| Yusuf et al., 2016 [48] | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 7 |
| Liniker et al., 2016 [49] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| Olson et al., 2016 [50] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 8 |
| Qin et al., 2016 [51] | 1 | 1 | 0 | 2 | 2 | 1 | 1 | 8 |
| Theurich et al., 2016 [52] | 1 | 1 | 0 | 0 | 2 | 1 | 0 | 5 |
| Gerber et al., 2015 [53] | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 8 |
| Kiess et al., 2015 [54] | 1 | 1 | 0 | 1 | 2 | 1 | 0 | 6 |
| Tazi et al., 2015 [55] | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 5 |
| Mathew et al., 2013 [56] | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 6 |
| Silk et al., 2013 [57] | 1 | 1 | 0 | 0 | 2 | 1 | 0 | 5 |
| Knisely et al., 2012 [58] | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Najafi, M.; Jahanbakhshi, A.; Gomar, M.; Iotti, C.; Giaccherini, L.; Rezaie, O.; Cavallieri, F.; Deantonio, L.; Bardoscia, L.; Botti, A.; et al. State of the Art in Combination Immuno/Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis. Curr. Oncol. 2022, 29, 2995-3012. https://doi.org/10.3390/curroncol29050244
Najafi M, Jahanbakhshi A, Gomar M, Iotti C, Giaccherini L, Rezaie O, Cavallieri F, Deantonio L, Bardoscia L, Botti A, et al. State of the Art in Combination Immuno/Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis. Current Oncology. 2022; 29(5):2995-3012. https://doi.org/10.3390/curroncol29050244
Chicago/Turabian StyleNajafi, Masoumeh, Amin Jahanbakhshi, Marzieh Gomar, Cinzia Iotti, Lucia Giaccherini, Omid Rezaie, Francesco Cavallieri, Letizia Deantonio, Lilia Bardoscia, Andrea Botti, and et al. 2022. "State of the Art in Combination Immuno/Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis" Current Oncology 29, no. 5: 2995-3012. https://doi.org/10.3390/curroncol29050244
APA StyleNajafi, M., Jahanbakhshi, A., Gomar, M., Iotti, C., Giaccherini, L., Rezaie, O., Cavallieri, F., Deantonio, L., Bardoscia, L., Botti, A., Sardaro, A., Cozzi, S., & Ciammella, P. (2022). State of the Art in Combination Immuno/Radiotherapy for Brain Metastases: Systematic Review and Meta-Analysis. Current Oncology, 29(5), 2995-3012. https://doi.org/10.3390/curroncol29050244