The Chemo-Gut Pilot Study: Associations between Gut Microbiota, Gastrointestinal Symptoms, and Psychosocial Health Outcomes in a Cross-Sectional Sample of Young Adult Cancer Survivors

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
1.1. Chemotherapy Impacts the Gut Microbiota
1.2. Chemotherapy Compromises the GI Tract
1.3. Chemotherapy Impacts Psychosocial Health
1.4. Present Study
2. Materials and Methods
2.1. Participants
2.2. Sample Size and Power Calculation
2.3. Demographics and Clinical Data
2.4. Procedure
2.5. Psychological and Gastrointestinal Outcomes
2.6. Gut Microbiota Profiling and Analysis
2.7. Bioinformatics and Data Analysis
3. Results
3.1. Aim 1: Study Feasibility and Participant Characteristics
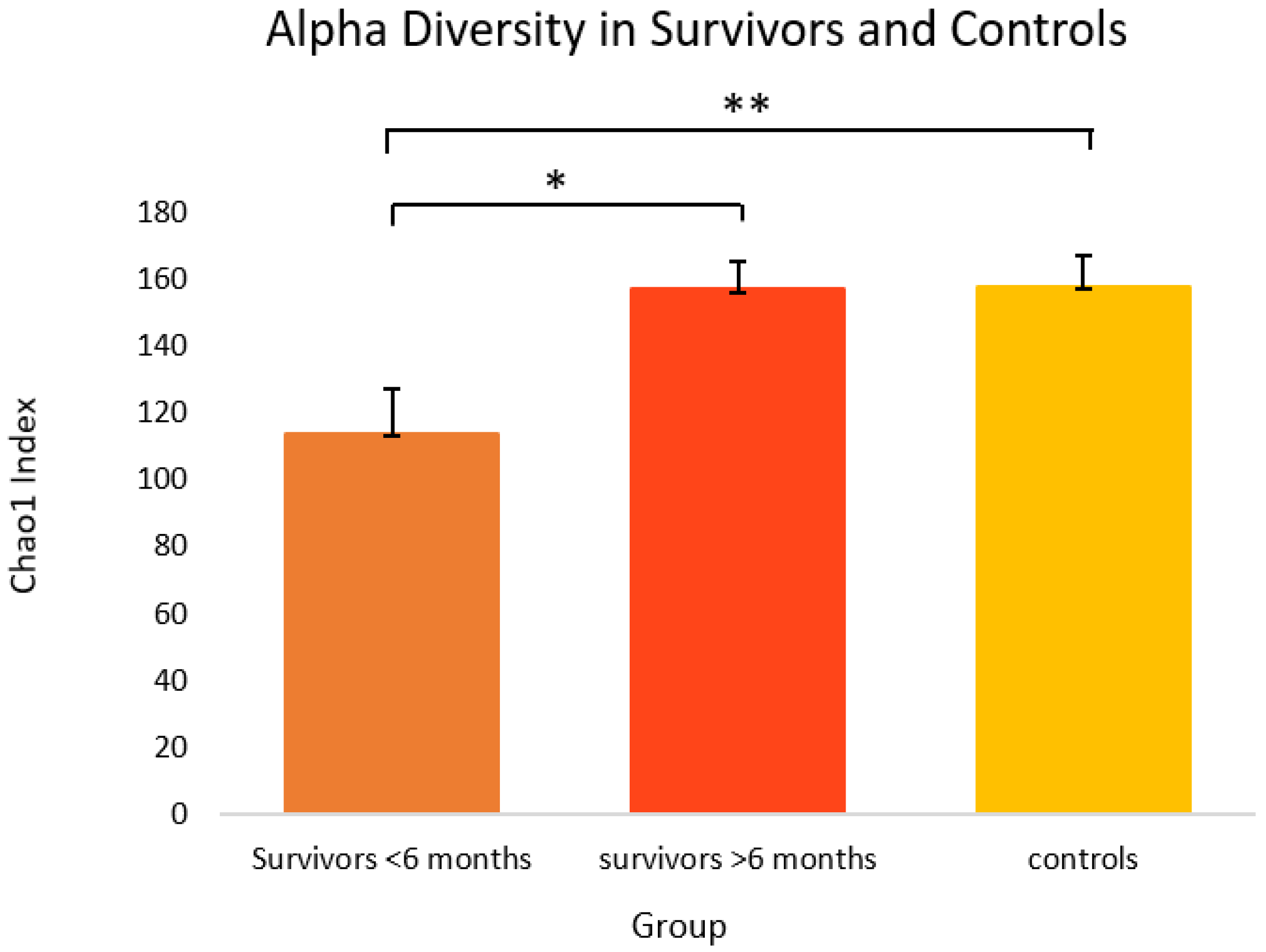
3.2. Aim 2: Relationships between Cancer Treatment-Related Factors and Gut Microbiota Alpha Diversity
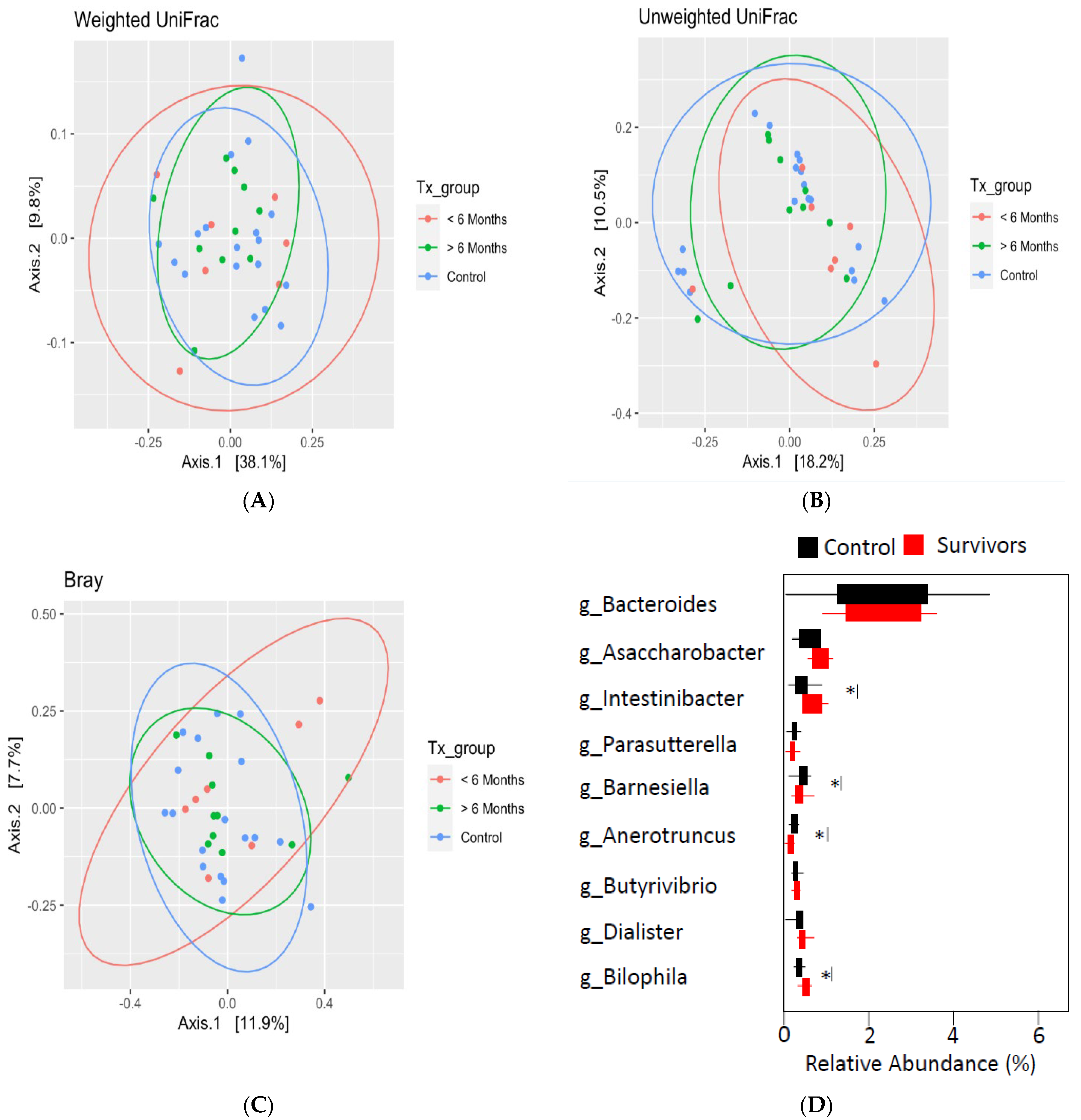
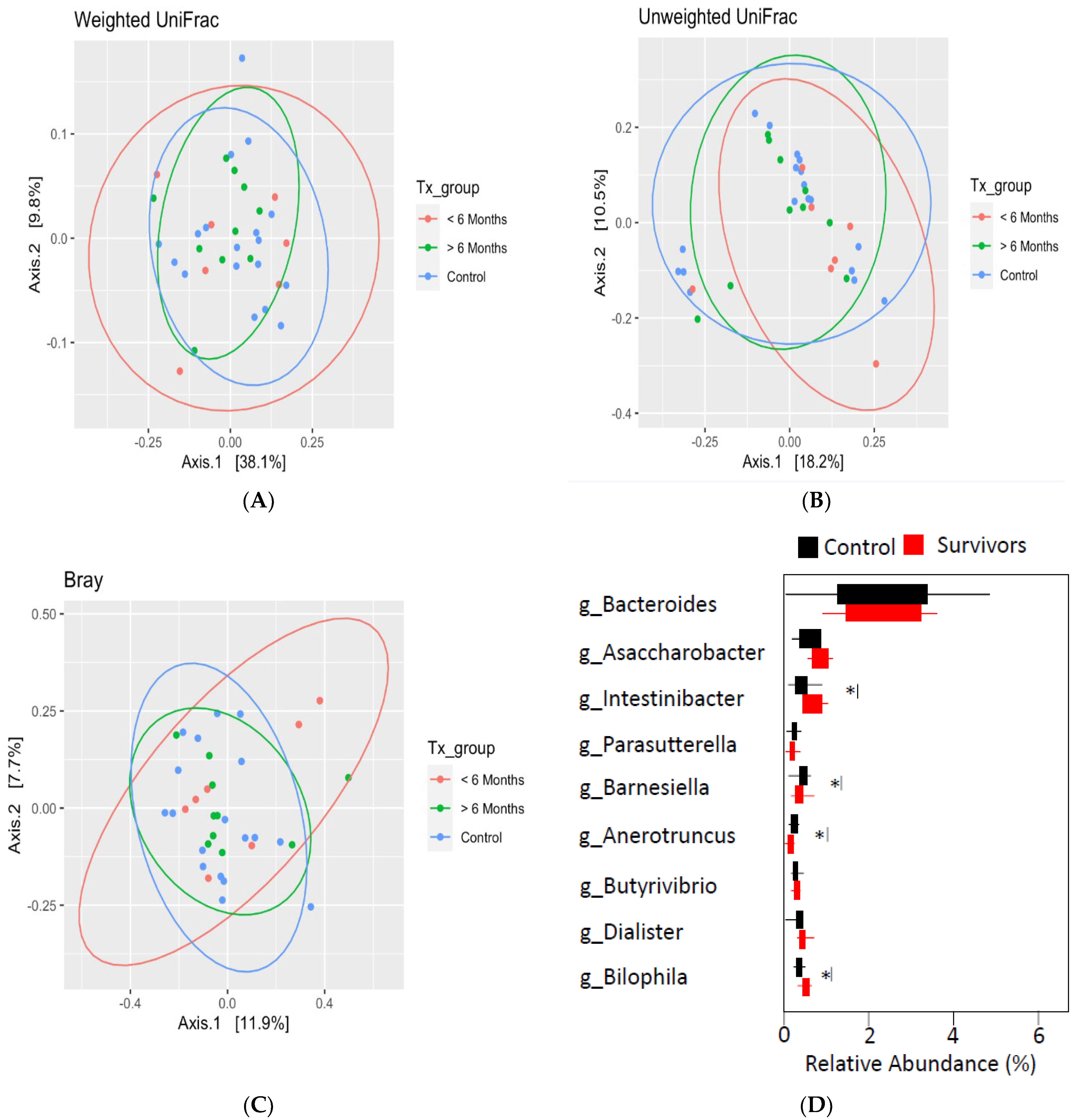
3.3. Aim 3: Gut Microbiota Taxonomic Composition in Cancer Survivors and Healthy Controls
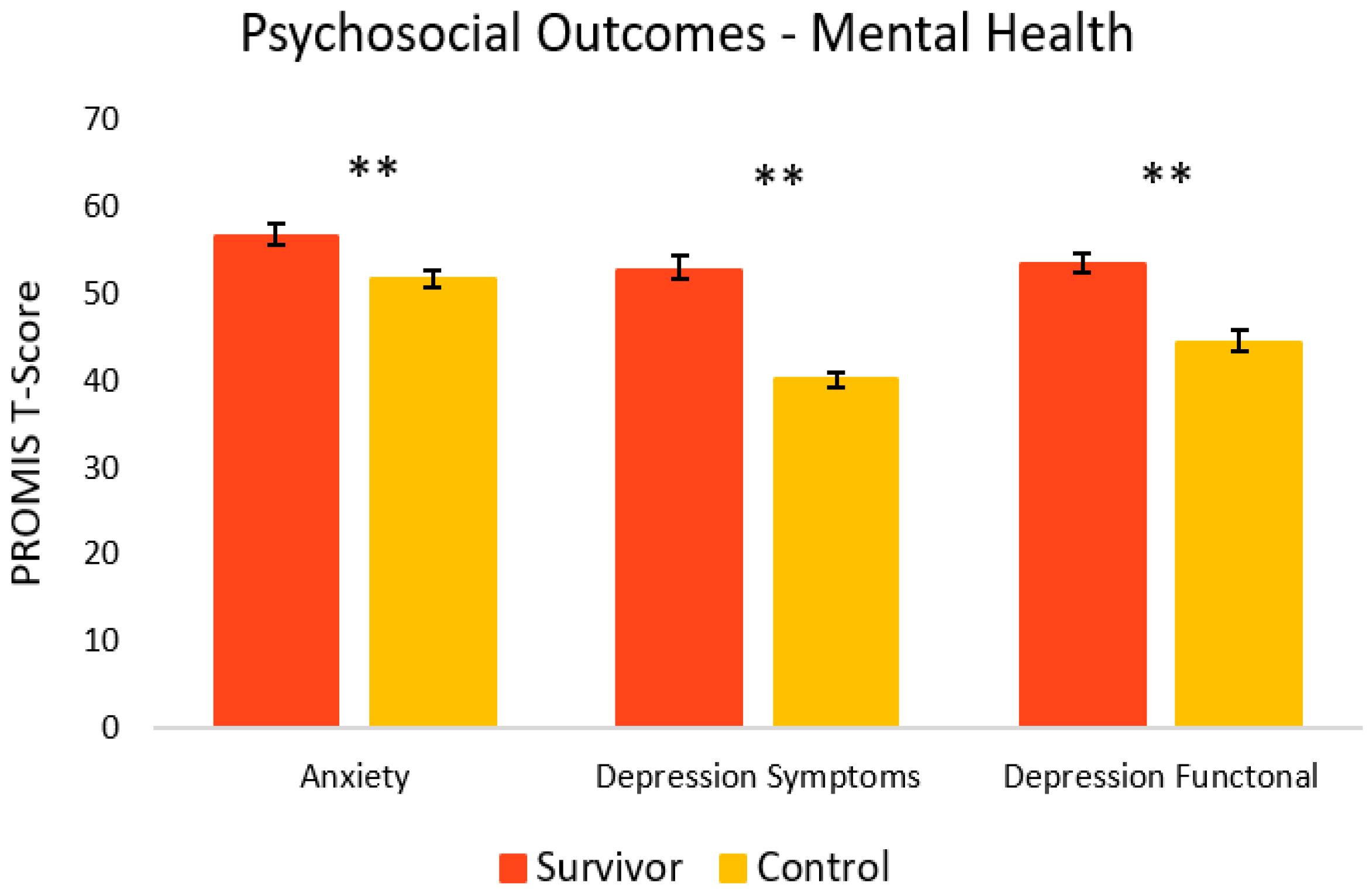
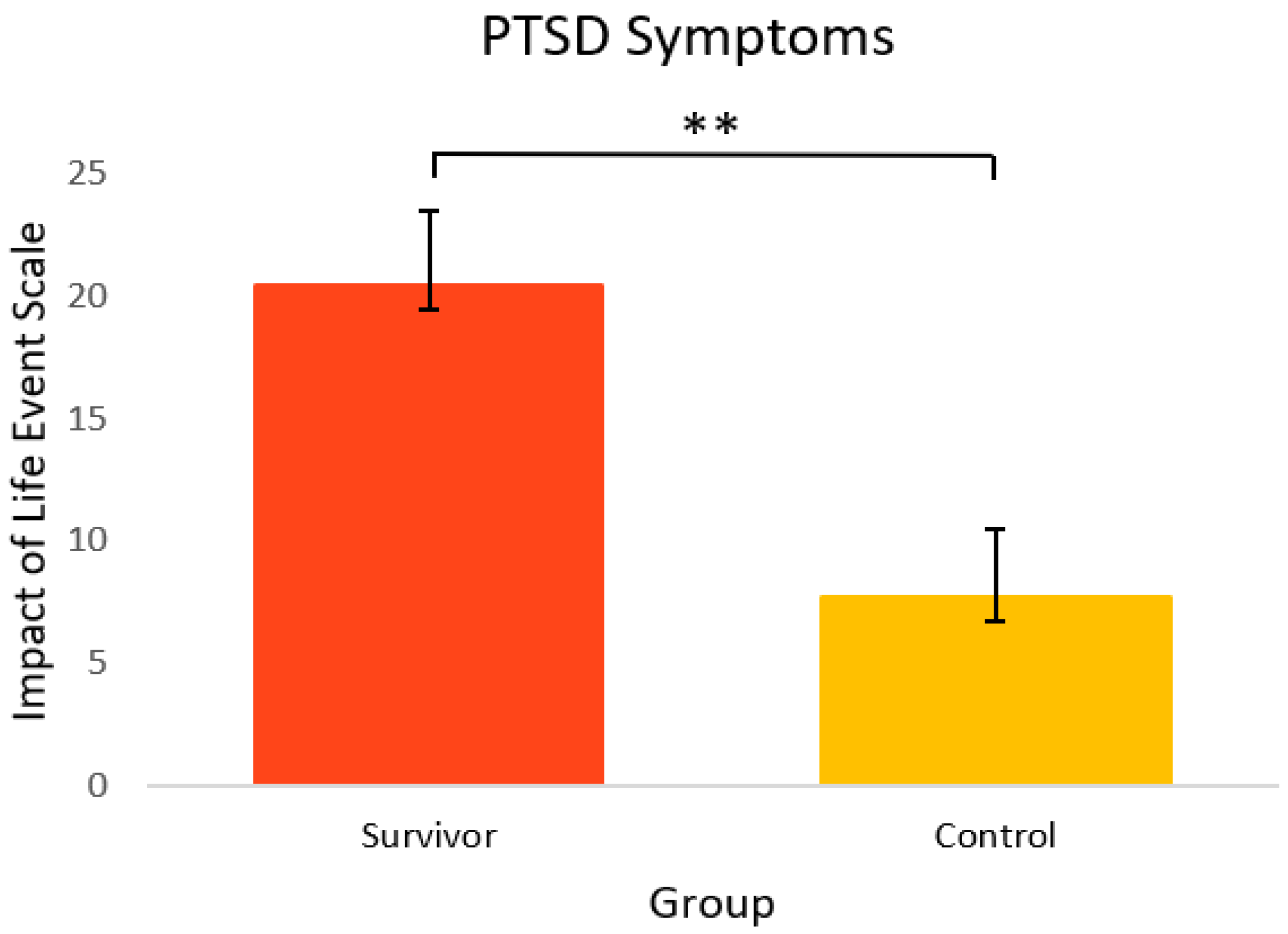
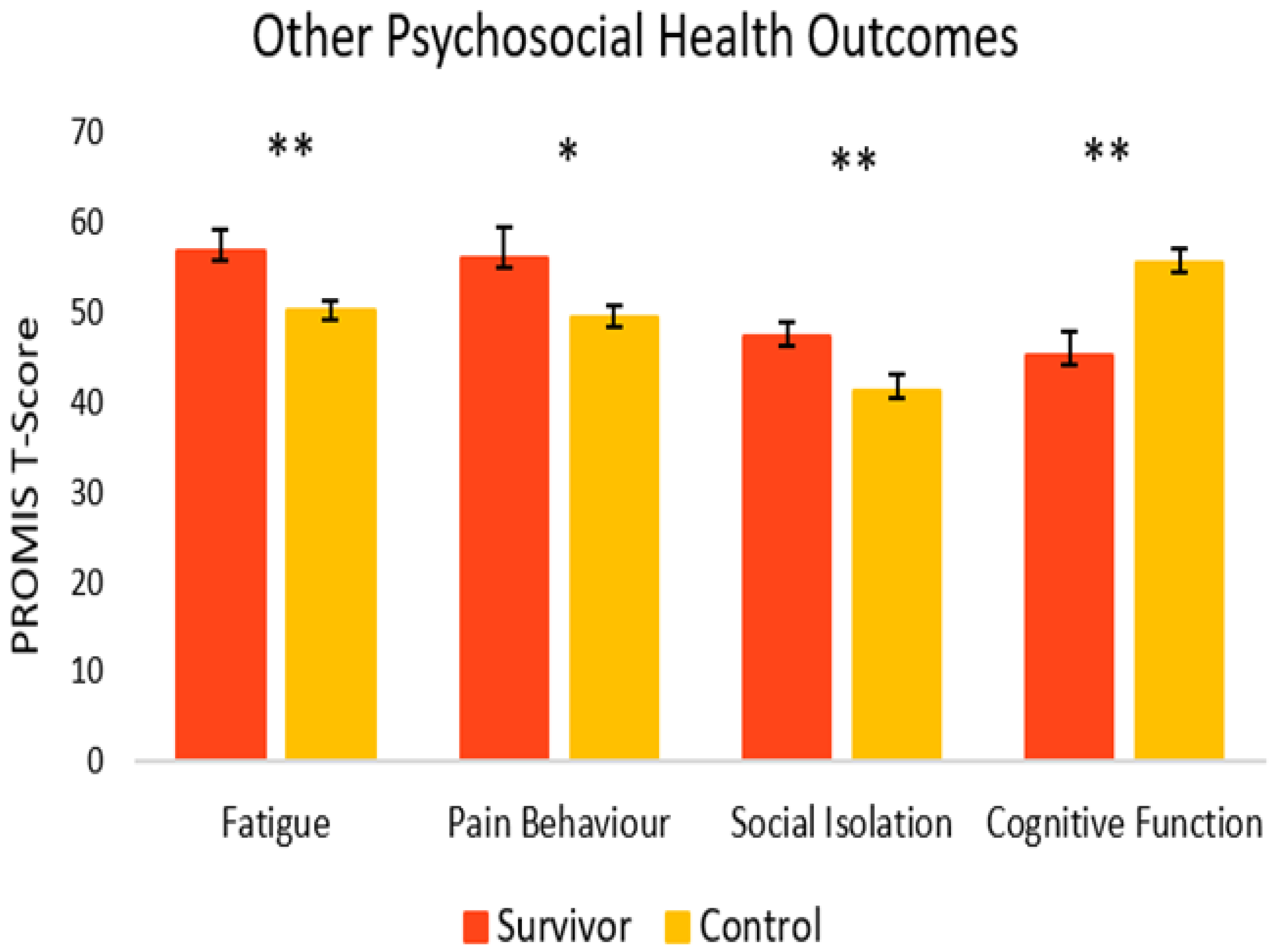
3.4. Aim 4: Outcomes for GI Symptoms and Psychosocial Health in Cancer Survivors and Healthy Controls
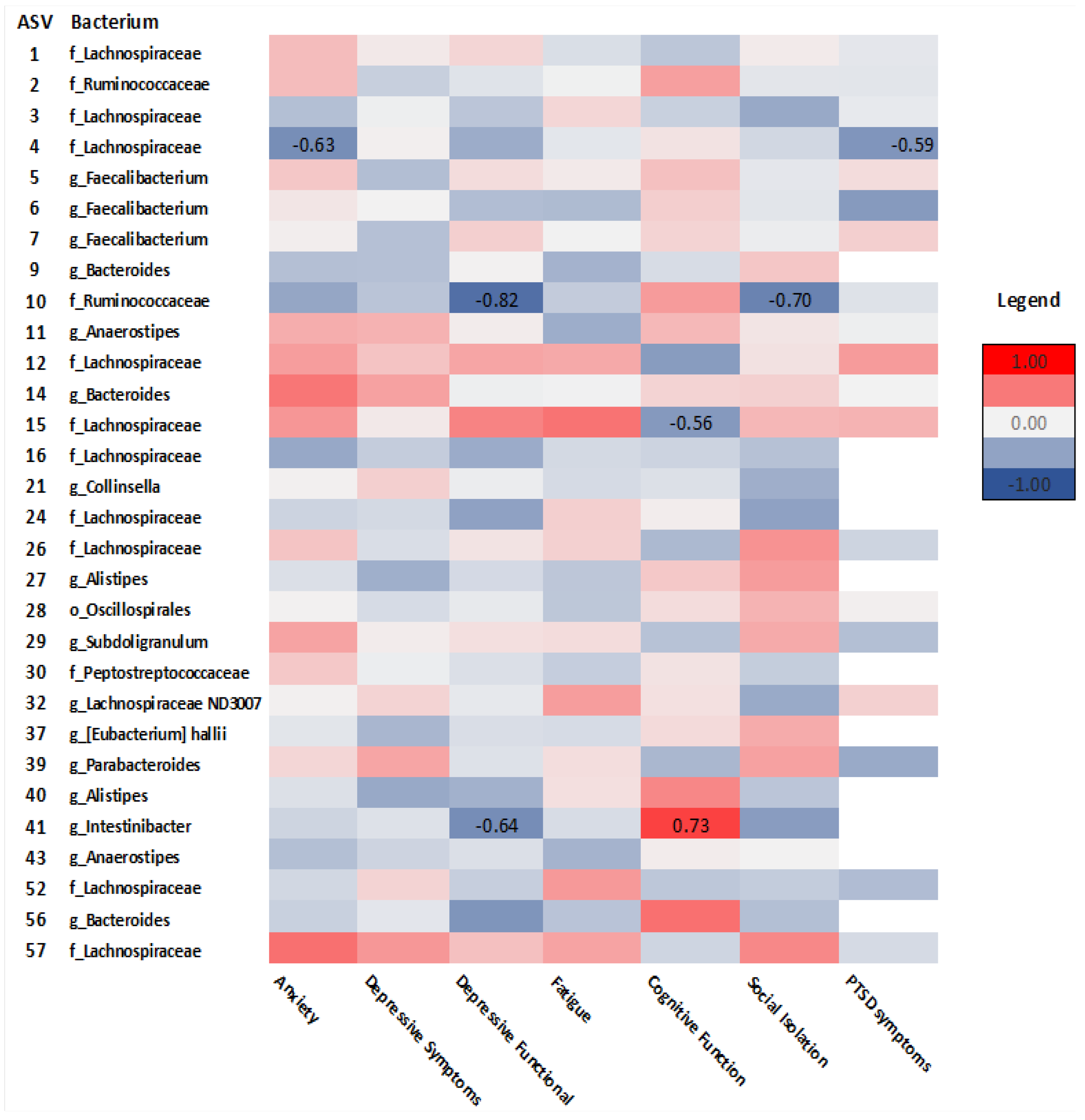
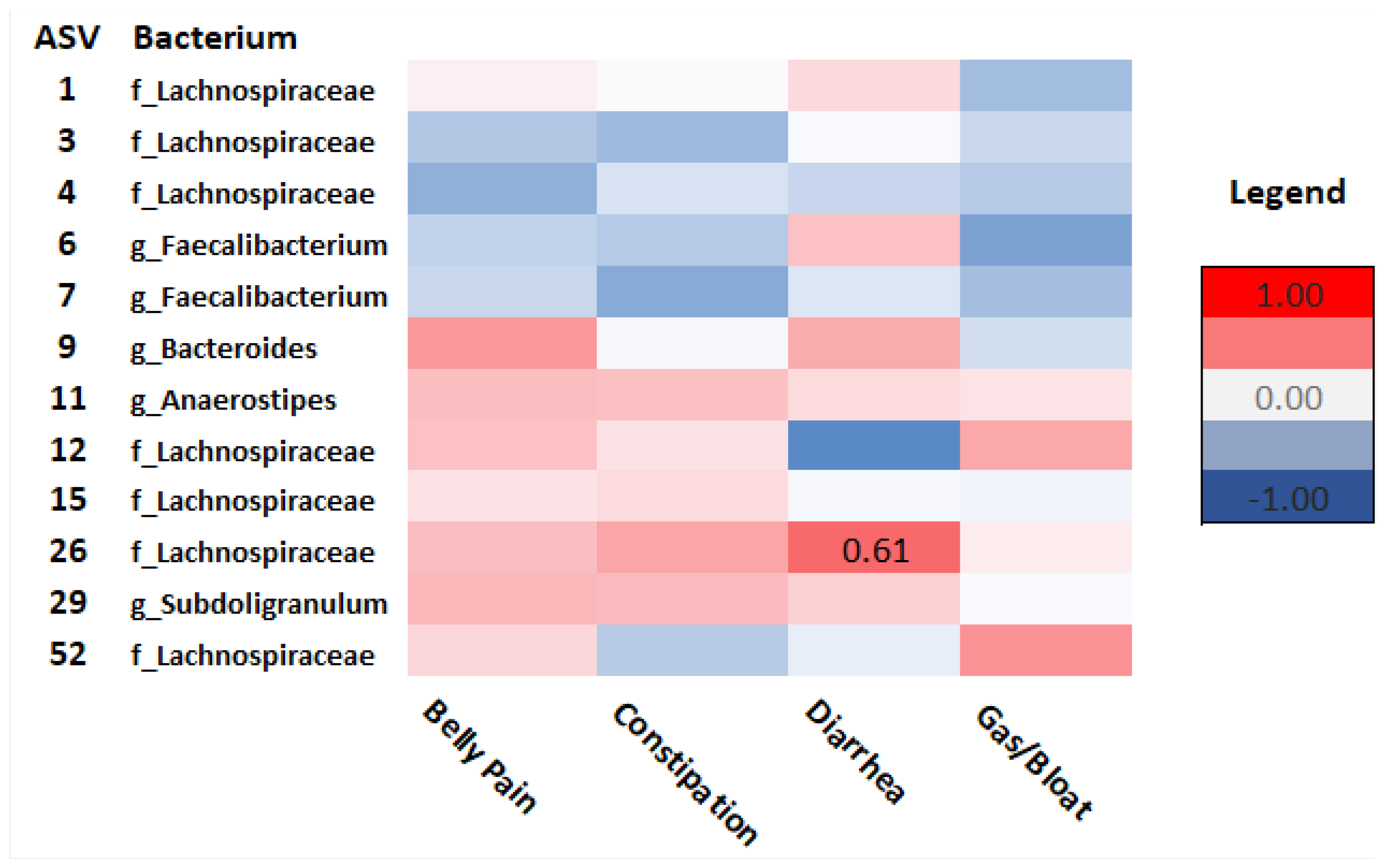
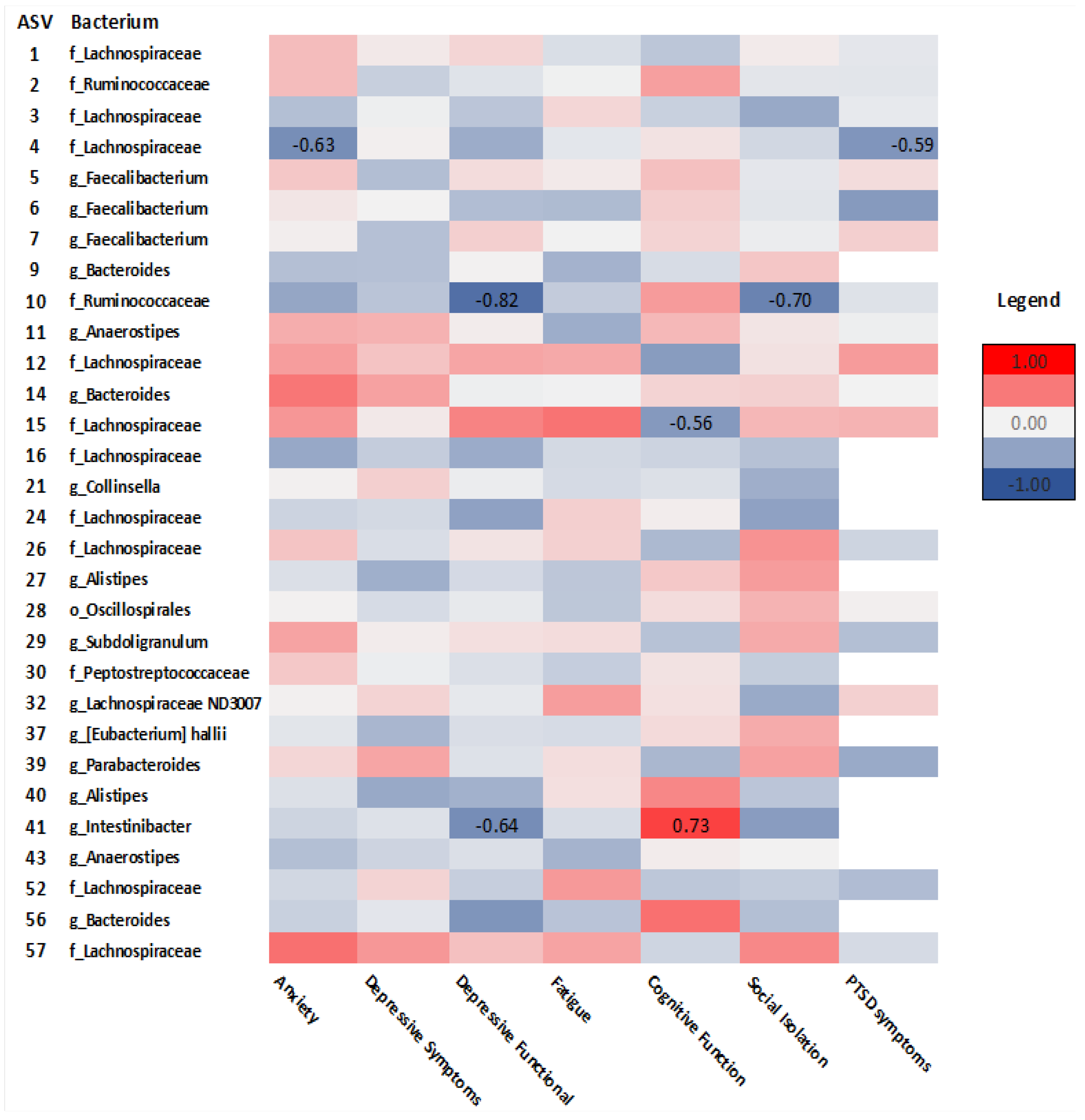
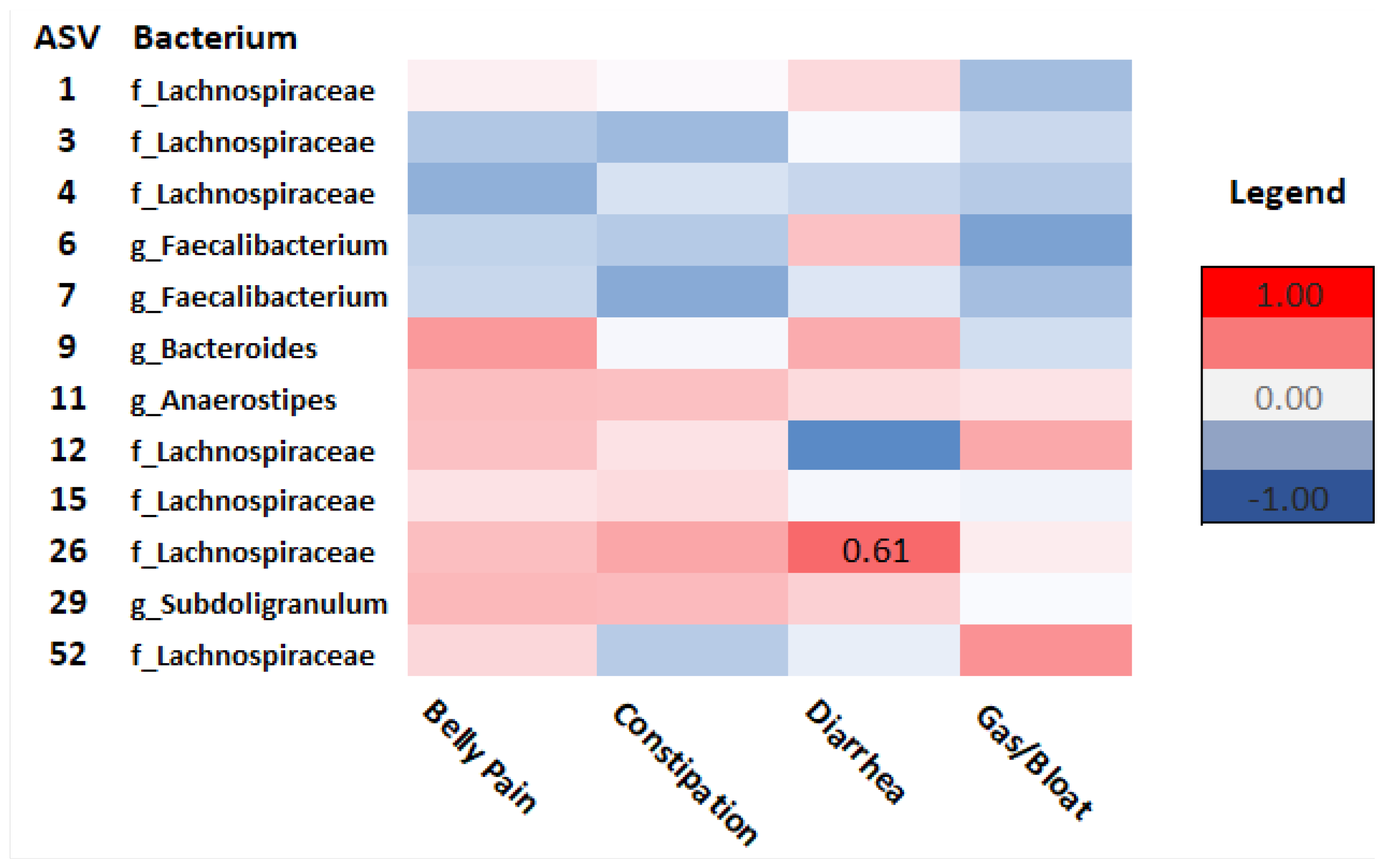
3.5. Aim 5: Associations between Gut Microbiota Alpha Diversity, Taxonomic Composition, GI Symptoms and Psychosocial Health Outcomes in Cancer Survivors
4. Discussion
4.1. Study Feasibility
4.2. Gut Microbiota in Cancer Survivors and Healthy Peers
4.3. GI and Psychosocial Symptoms
4.4. Relationships between Gut Microbiota, GI, and Psychosocial Symptoms
4.5. Limitations
4.6. Implications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Dinan, T.G.; Cryan, J.F. The Microbiome-Gut-Brain Axis in Health and Disease. Gastroenterol. Clin. N. Am. 2017, 46, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Levy, M.; Kolodziejczyk, A.A.; Thaiss, C.A.; Elinav, E. Dysbiosis and the immune system. Nat. Rev. Immunol. 2017, 17, 219–232. [Google Scholar] [CrossRef]
- Cryan, J.F.; Dinan, T.G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat. Rev. Neurosci. 2012, 13, 701–712. [Google Scholar] [CrossRef]
- Petra, A.I.; Panagiotidou, S.; Hatziagelaki, E.; Stewart, J.M.; Conti, P.; Theoharides, T.C. Gut-Microbiota-Brain Axis and Its Effect on Neuropsychiatric Disorders With Suspected Immune Dysregulation. Clin. Ther. 2015, 37, 984–995. [Google Scholar] [CrossRef] [Green Version]
- Rinninella, E.; Raoul, P.; Cintoni, M.; Franceschi, F.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. What is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases. Microorganisms 2019, 7, 14. [Google Scholar] [CrossRef] [Green Version]
- Grant, C.V.; Loman, B.R.; Bailey, M.T.; Pyter, L.M. Manipulations of the gut microbiome alter chemotherapy-induced inflammation and behavioral side effects in female mice. Brain Behav. Immun. 2021, 95, 401–412. [Google Scholar] [CrossRef]
- Huang, Y.; Yang, W.; Liu, H.; Duan, J.; Zhang, Y.; Liu, M.; Li, H.; Hou, Z.; Wu, K.K. Effect of high-dose methotrexate chemotherapy on intestinal Bifidobacteria, Lactobacillus and Escherichia coli in children with acute lymphoblastic leukemia. Exp. Biol. Med. 2012, 237, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Montassier, E.; Gastinne, T.; Vangay, P.; Al-Ghalith, G.A.; des Varannes, S.B.; Massart, S.; Moreau, P.; Potel, G.; de La Cochetiere, M.F.; Batard, E.; et al. Chemotherapy-driven dysbiosis in the intestinal microbiome. Aliment. Pharmacol. Ther. 2015, 42, 515–528. [Google Scholar] [CrossRef] [PubMed]
- Bajic, J.E.; Johnston, I.N.; Howarth, G.S.; Hutchinson, M.R. From the Bottom-Up: Chemotherapy and Gut-Brain Axis Dysregulation. Front. Behav. Neurosci. 2018, 12, 104. [Google Scholar] [CrossRef] [Green Version]
- Okubo, R.; Kinoshita, T.; Katsumata, N.; Uezono, Y.; Xiao, J.; Matsuoka, Y.J. Impact of chemotherapy on the association between fear of cancer recurrence and the gut microbiota in breast cancer survivors. Brain Behav. Immun. 2020, 85, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Grenham, S.; Clarke, G.; Cryan, J.F.; Dinan, T.G. Brain-gut-microbe communication in health and disease. Front. Physiol. 2011, 2, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loman, B.R.; Jordan, K.R.; Haynes, B.; Bailey, M.T.; Pyter, L.M. Chemotherapy-induced neuroinflammation is associated with disrupted colonic and bacterial homeostasis in female mice. Sci. Rep. 2019, 9, 16490. [Google Scholar] [CrossRef] [Green Version]
- Schurman, J.V.; Singh, M.; Singh, V.; Neilan, N.; Friesen, C.A. Symptoms and subtypes in pediatric functional dyspepsia: Relation to mucosal inflammation and psychological functioning. J. Pediatr. Gastroenterol. Nutr. 2010, 51, 298–303. [Google Scholar] [CrossRef]
- Rutsch, A.; Kantsjo, J.B.; Ronchi, F. The Gut-Brain Axis: How Microbiota and Host Inflammasome Influence Brain Physiology and Pathology. Front. Immunol. 2020, 11, 604179. [Google Scholar] [CrossRef] [PubMed]
- Paray, B.A.; Albeshr, M.F.; Jan, A.T.; Rather, I.A. Leaky Gut and Autoimmunity: An Intricate Balance in Individuals Health and the Diseased State. Int. J. Mol. Sci. 2020, 21, 9770. [Google Scholar] [CrossRef]
- Foster, J.A.; Neufeld, K.M. Gut-brain axis: How the microbiome influences anxiety and depression. Trends Neurosci. 2013, 36, 305–312. [Google Scholar] [CrossRef]
- Dantzer, R.; Kelley, K.W. Twenty years of research on cytokine-induced sickness behavior. Brain Behav. Immun. 2007, 21, 153–160. [Google Scholar] [CrossRef] [Green Version]
- About Mental Health. Available online: https://www.cdc.gov/mentalhealth/learn/index.htm#:~:text=Mental%20health%20includes%20our%20emotional,childhood%20and%20adolescence%20through%20adulthood (accessed on 5 April 2022).
- Dinan, T.G.; Cryan, J.F. Melancholic microbes: A link between gut microbiota and depression? Neurogastroenterol. Motil. 2013, 25, 713–719. [Google Scholar] [CrossRef]
- Paulsen, J.A.; Ptacek, T.S.; Carter, S.J.; Liu, N.; Kumar, R.; Hyndman, L.; Lefkowitz, E.J.; Morrow, C.D.; Rogers, L.Q. Gut microbiota composition associated with alterations in cardiorespiratory fitness and psychosocial outcomes among breast cancer survivors. Support Care Cancer 2017, 25, 1563–1570. [Google Scholar] [CrossRef]
- Hemmings, S.M.J.; Malan-Muller, S.; van den Heuvel, L.L.; Demmitt, B.A.; Stanislawski, M.A.; Smith, D.G.; Bohr, A.D.; Stamper, C.E.; Hyde, E.R.; Morton, J.T.; et al. The Microbiome in Posttraumatic Stress Disorder and Trauma-Exposed Controls: An Exploratory Study. Psychosom. Med. 2017, 79, 936–946. [Google Scholar] [CrossRef] [PubMed]
- Lakhan, S.E.; Kirchgessner, A. Gut inflammation in chronic fatigue syndrome. Nutr. Metab. 2010, 7, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, C.; Fedirko, V.; Beitler, J.; Bai, J.; Peng, G.; Zhou, C.; Gu, J.; Zhao, H.; Lin, I.H.; Chico, C.E.; et al. The role of the gut microbiome in cancer-related fatigue: Pilot study on epigenetic mechanisms. Support Care Cancer 2021, 29, 3173–3182. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, C.; Corleto, J.; Ruegger, P.M.; Logan, G.D.; Peacock, B.B.; Mendonca, S.; Yamaki, S.; Adamson, T.; Ermel, R.; McKemy, D.; et al. Dominant Role of the Gut Microbiota in Chemotherapy Induced Neuropathic Pain. Sci. Rep. 2019, 9, 20324. [Google Scholar] [CrossRef] [Green Version]
- Sarkar, A.; Harty, S.; Lehto, S.M.; Moeller, A.H.; Dinan, T.G.; Dunbar, R.I.M.; Cryan, J.F.; Burnet, P.W.J. The Microbiome in Psychology and Cognitive Neuroscience. Trends Cogn. Sci. 2018, 22, 611–636. [Google Scholar] [CrossRef]
- Fond, G.; Loundou, A.; Hamdani, N.; Boukouaci, W.; Dargel, A.; Oliveira, J.; Roger, M.; Tamouza, R.; Leboyer, M.; Boyer, L. Anxiety and depression comorbidities in irritable bowel syndrome (IBS): A systematic review and meta-analysis. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 651–660. [Google Scholar] [CrossRef]
- Simpson, C.A.; Mu, A.; Haslam, N.; Schwartz, O.S.; Simmons, J.G. Feeling down? A systematic review of the gut microbiota in anxiety/depression and irritable bowel syndrome. J. Affect. Disord. 2020, 266, 429–446. [Google Scholar] [CrossRef]
- Touchefeu, Y.; Montassier, E.; Nieman, K.; Gastinne, T.; Potel, G.; des Varannes, S.B.; Le Vacon, F.; de La Cochetiere, M.F. Systematic review: The role of the gut microbiota in chemotherapy- or radiation-induced gastrointestinal mucositis—Current evidence and potential clinical applications. Aliment. Pharmacol. Ther. 2014, 40, 409–421. [Google Scholar] [CrossRef]
- Clapp, M.; Aurora, N.; Herrera, L.; Bhatia, M.; Wilen, E.; Wakefield, S. Gut microbiota’s effect on mental health: The gut-brain axis. Clin. Pract. 2017, 7, 987. [Google Scholar] [CrossRef]
- Desbonnet, L.; Garrett, L.; Clarke, G.; Kiely, B.; Cryan, J.F.; Dinan, T.G. Effects of the probiotic Bifidobacterium infantis in the maternal separation model of depression. Neuroscience 2010, 170, 1179–1188. [Google Scholar] [CrossRef]
- Hilimire, M.R.; DeVylder, J.E.; Forestell, C.A. Fermented foods, neuroticism, and social anxiety: An interaction model. Psychiatry Res. 2015, 228, 203–208. [Google Scholar] [CrossRef]
- Steenbergen, L.; Sellaro, R.; van Hemert, S.; Bosch, J.A.; Colzato, L.S. A randomized controlled trial to test the effect of multispecies probiotics on cognitive reactivity to sad mood. Brain Behav. Immun. 2015, 48, 258–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asher, A. Cognitive dysfunction among cancer survivors. Am. J. Phys. Med. Rehabil. 2011, 90 (Suppl. 1), S16–S26. [Google Scholar] [CrossRef] [PubMed]
- Seitz, D.C.; Besier, T.; Debatin, K.M.; Grabow, D.; Dieluweit, U.; Hinz, A.; Kaatsch, P.; Goldbeck, L. Posttraumatic stress, depression and anxiety among adult long-term survivors of cancer in adolescence. Eur. J. Cancer 2010, 46, 1596–1606. [Google Scholar] [CrossRef]
- Bower, J.E. Cancer-related fatigue—Mechanisms, risk factors, and treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef]
- Yi, J.C.; Syrjala, K.L. Anxiety and Depression in Cancer Survivors. Med. Clin. N. Am. 2017, 101, 1099–1113. [Google Scholar] [CrossRef]
- Prasad, P.K.; Hardy, K.K.; Zhang, N.; Edelstein, K.; Srivastava, D.; Zeltzer, L.; Stovall, M.; Seibel, N.L.; Leisenring, W.; Armstrong, G.T.; et al. Psychosocial and Neurocognitive Outcomes in Adult Survivors of Adolescent and Early Young Adult Cancer: A Report from the Childhood Cancer Survivor Study. J. Clin. Oncol. 2015, 33, 2545–2552. [Google Scholar] [CrossRef] [Green Version]
- Zebrack, B.J.; Corbett, V.; Embry, L.; Aguilar, C.; Meeske, K.A.; Hayes-Lattin, B.; Block, R.; Zeman, D.T.; Cole, S. Psychological distress and unsatisfied need for psychosocial support in adolescent and young adult cancer patients during the first year following diagnosis. Psychooncology 2014, 23, 1267–1275. [Google Scholar] [CrossRef] [Green Version]
- Cancer, C.P.A. Adolescents and Young Adults with Cancer: System Performance Report; Canadian Partnership Against Cancer: Toronto, ON, Canada, 2017. [Google Scholar]
- Deleemans, J.M.; Chleilat, F.; Reimer, R.A.; Henning, J.W.; Baydoun, M.; Piedalue, K.A.; McLennan, A.; Carlson, L.E. The chemo-gut study: Investigating the long-term effects of chemotherapy on gut microbiota, metabolic, immune, psychological and cognitive parameters in young adult Cancer survivors; study protocol. BMC Cancer 2019, 19, 1243. [Google Scholar] [CrossRef] [Green Version]
- Effect Size (Cohen’s d) Calculator for a Student t-Test. Available online: https://www.danielsoper.com/statcalc/calculator.aspx?id=48 (accessed on 12 November 2020).
- Christianson, S.; Marren, J. The Impact of Event Scale—Revised (IES-R). Medsurg. Nurs. 2012, 21, 321–322. [Google Scholar]
- PROMIS® Patient-Reported Outcomes Measurement Information System®. Available online: https://www.promishealth.org/57461-2/ (accessed on 23 January 2022).
- Cessna, J.M.; Jim, H.S.; Sutton, S.K.; Asvat, Y.; Small, B.J.; Salsman, J.M.; Zachariah, B.; Fishman, M.; Field, T.; Fernandez, H.; et al. Evaluation of the psychometric properties of the PROMIS Cancer Fatigue Short Form with cancer patients. J. Psychosom. Res. 2016, 81, 9–13. [Google Scholar] [CrossRef] [Green Version]
- Spiegel, B.M.; Hays, R.D.; Bolus, R.; Melmed, G.Y.; Chang, L.; Whitman, C.; Khanna, P.P.; Paz, S.H.; Hays, T.; Reise, S.; et al. Development of the NIH Patient-Reported Outcomes Measurement Information System (PROMIS) gastrointestinal symptom scales. Am. J. Gastroenterol. 2014, 109, 1804–1814. [Google Scholar] [CrossRef] [Green Version]
- Kochar, B.; Martin, C.F.; Kappelman, M.D.; Spiegel, B.M.; Chen, W.; Sandler, R.S.; Long, M.D. Evaluation of Gastrointestinal Patient Reported Outcomes Measurement Information System (GI-PROMIS) Symptom Scales in Subjects with Inflammatory Bowel Diseases. Am. J. Gastroenterol. 2018, 113, 72–79. [Google Scholar] [CrossRef]
- Chleilat, F.; Klancic, T.; Ma, K.; Schick, A.; Nettleton, J.E.; Reimer, R.A. Human Milk Oligosaccharide Supplementation Affects Intestinal Barrier Function and Microbial Composition in the Gastrointestinal Tract of Young Sprague Dawley Rats. Nutrients 2020, 12, 1532. [Google Scholar] [CrossRef]
- Chleilat, F.; Schick, A.; Deleemans, J.M.; Ma, K.; Alukic, E.; Wong, J.; Noye Tuplin, E.W.; Nettleton, J.E.; Reimer, R.A. Paternal high protein diet modulates body composition, insulin sensitivity, epigenetics, and gut microbiota intergenerationally in rats. FASEB J. 2021, 35, e21847. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [Green Version]
- Martin, M. Cutadapt removes adapter sequences from high-throughput sequencing reads. EMBnet. J. 2011, 17, 3. [Google Scholar] [CrossRef]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glockner, F.O. The SILVA ribosomal RNA gene database project: Improved data processing and web-based tools. Nucleic Acids. Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef]
- Wright, E.S. DECIPHER: Harnessing local sequence context to improve protein multiple sequence alignment. BMC Bioinform. 2015, 16, 322. [Google Scholar] [CrossRef] [Green Version]
- McMurdie, P.J.; Holmes, S. Phyloseq: An R package for reproducible interactive analysis and graphics of microbiome census data. PLoS ONE 2013, 8, e61217. [Google Scholar] [CrossRef] [Green Version]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef] [Green Version]
- May, J.O.; Looney, S.W. Sample Size Charts for Spearman and Kendall Coefficients. Biom. Biostat. 2020, 11, 1–7. [Google Scholar]
- Brenner, D.R.; Tepylo, K.; Eny, K.M.; Cahill, L.E.; El-Sohemy, A. Comparison of body mass index and waist circumference as predictors of cardiometabolic health in a population of young Canadian adults. Diabetol. Metab. Syndr. 2010, 2, 28. [Google Scholar] [CrossRef] [Green Version]
- Deleemans, J.M.; Toivonen, K.; Reimer, R.A.; Carlson, L.E. The Chemo-Gut Study: A cross-sectional survey Exploring Physical, Mental, and Gastrointestinal Health Outcomes in Cancer Survivors. In Global Advances in Medicine and Health, in Review; submitted 13 December 2021; Sage Journals: Thousand Oaks, CA, USA, 2022. [Google Scholar]
- Wang, A.; Ling, Z.; Yang, Z.; Kiela, P.R.; Wang, T.; Wang, C.; Cao, L.; Geng, F.; Shen, M.; Ran, X.; et al. Gut microbial dysbiosis may predict diarrhea and fatigue in patients undergoing pelvic cancer radiotherapy: A pilot study. PLoS ONE 2015, 10, e0126312. [Google Scholar] [CrossRef] [Green Version]
- Andreyev, H.J.; Davidson, S.E.; Gillespie, C.; Allum, W.H.; Swarbrick, E. British Society of G, Association of Colo-Proctology of Great B, Ireland, Association of Upper Gastrointestinal S, Faculty of Clinical Oncology Section of the Royal College of R: Practice guidance on the management of acute and chronic gastrointestinal problems arising as a result of treatment for cancer. Gut 2012, 61, 179–192. [Google Scholar]
- O’Reilly, M.; Mellotte, G.; Ryan, B.; O’Connor, A. Gastrointestinal side effects of cancer treatments. Ther. Adv. Chronic. Dis. 2020, 11, 2040622320970354. [Google Scholar] [CrossRef]
- Lee, Y.J.; Arguello, E.S.; Jenq, R.R.; Littmann, E.; Kim, G.J.; Miller, L.C.; Ling, L.; Figueroa, C.; Robilotti, E.; Perales, M.A.; et al. Protective Factors in the Intestinal Microbiome Against Clostridium difficile Infection in Recipients of Allogeneic Hematopoietic Stem Cell Transplantation. J. Infect. Dis. 2017, 215, 1117–1123. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Ling, Z.; Zhang, Y.; Mao, H.; Ma, Z.; Yin, Y.; Wang, W.; Tang, W.; Tan, Z.; Shi, J.; et al. Altered fecal microbiota composition in patients with major depressive disorder. Brain Behav. Immun. 2015, 48, 186–194. [Google Scholar] [CrossRef] [Green Version]
- Naseribafrouei, A.; Hestad, K.; Avershina, E.; Sekelja, M.; Linlokken, A.; Wilson, R.; Rudi, K. Correlation between the human fecal microbiota and depression. Neurogastroenterol. Motil. 2014, 26, 1155–1162. [Google Scholar] [CrossRef]
- Baker, J.M.; Al-Nakkash, L.; Herbst-Kralovetz, M.M. Estrogen-gut microbiome axis: Physiological and clinical implications. Maturitas 2017, 103, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Sampsell, K.; Hao, D.; Reimer, R.A. The Gut Microbiota: A Potential Gateway to Improved Health Outcomes in Breast Cancer Treatment and Survivorship. Int. J. Mol. Sci. 2020, 21, 9239. [Google Scholar] [CrossRef]
- Gonzalez-Mercado, V.J.; Lim, J.; Marrero, S.; Pedro, E.; Saligan, L.N. Gut microbiota and fatigue in rectal cancer patients: A cross-sectional pilot study. Support Care Cancer 2021, 29, 4615–4621. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Mercado, V.J.; Lim, J.; Saligan, L.N.; Perez, N.; Rodriguez, C.; Bernabe, R.; Ozorio, S.; Pedro, E.; Sepehri, F.; Aouizerat, B. Gut Microbiota and Depressive Symptoms at the End of CRT for Rectal Cancer: A Cross-Sectional Pilot Study. Depress Res. Treat 2021, 2021, 7967552. [Google Scholar] [CrossRef] [PubMed]
- Forbes, J.D.; Chen, C.Y.; Knox, N.C.; Marrie, R.A.; El-Gabalawy, H.; de Kievit, T.; Alfa, M.; Bernstein, C.N.; Van Domselaar, G. A comparative study of the gut microbiota in immune-mediated inflammatory diseases-does a common dysbiosis exist? Microbiome 2018, 6, 221. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liu, F.; Ling, Z.; Tong, X.; Xiang, C. Human intestinal lumen and mucosa-associated microbiota in patients with colorectal cancer. PLoS ONE 2012, 7, e39743. [Google Scholar] [CrossRef] [PubMed]
- Sears, C.L.; Garrett, W.S. Microbes, microbiota, and colon cancer. Cell Host Microbe 2014, 15, 317–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deleemans, J.M.; Gajtani, Z.; Baydoun, M.; Reimer, R.A.; Piedalue, K.A.; Carlson, L.E. The Use of Prebiotic and Probiotic Interventions for Treating Gastrointestinal and Psychosocial Health Symptoms in Cancer Patients and Survivors: A Systematic Review. Integr. Cancer Ther. 2021, 20, 15347354211061733. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Variable | ||
|---|---|---|
| Survivors (n = 17) | Controls (n = 18) | |
| Current Age in Years | M = 32.0 (±5.8) | M = 28.3 (±5.3) |
| % (n) | % (n) | |
| Sex | ||
| Male | 35.3 (6) | 44.4 (10) |
| Female | 64.7 (11) | 55.6 (8) |
| Ethnicity | ||
| Caucasian/white | 58.8 (10) | 77.8 (14) |
| First Nations | 0 | 0 |
| African American/Black | 0 | 0 |
| South Asian/Chinese/Filipino | 5.9 (1) | 11.1 (2) |
| Indian-subcontinent | 11.8 (2) | 5.6 (1) |
| Other | 23.5 (4) | 5.6 (1) |
| Education | ||
| High school | 11.8 (2) | 5.6 (1) |
| Trade school | 17.6 (3) | 5.6 (1) |
| Community College | 23.5 (4) | 5.6 (1) |
| University (undergraduate) | 35.3 (6) | 50.0 (9) |
| University (professional/post-grad) | 11.8 (2) | 33.3 (6) |
| Income | ||
| less than $30,000 | 29.4 (5) | 38.9 (7) |
| $30,000 to less than $50,000 | 11.8 (2) | 5.6 (1) |
| $50,000 to less than $80,000 | 41.2 (7) | 11.1 (2) |
| $80,000 to less than $120,000 | 11.8 (2) | 27.8 (5) |
| greater than $120,000 | 5.9 (1) | 16.7 (3) |
| Marital Status | ||
| Single (never legally married) | 41.2 (7) | 50.0 (9) |
| Married | 35.3 (6) | 16.7 (3) |
| Common-law | 23.5 (4) | 27.8 (5) |
| Divorced | 0 | 0 |
| Separated | 0 | 5.6 (1) |
| Living Situation | ||
| Living with a partner | 58.8 (10) | 55.6 (10) |
| Living with roommate(s) | 11.8 (2) | 5.6 (1) |
| Living with family | 23.5 (4) | 22.2 (4) |
| Living alone | 5.9 (1) | 16.7 (3) |
| Community | ||
| Metropolitan | 100 (17) | 94.4 (17) |
| Regional/remote | 0 | 5.6 (1) |
| Cancer Variables (Survivors n = 17) | ||
|---|---|---|
| Age at Diagnosis (Years) | M = 30.1 (±6.0) | |
| % (n) | ||
| Cancer Type | ||
| Breast | 11.8 (2) | |
| Hodgkin Lymphoma | 41.2 (7) | |
| Non-Hodgkin Lymphoma | 23.5 (4) | |
| Sarcoma (bone and soft tissue) | 11.8 (2) | |
| Other | 11.8 (2) | |
| Cancer Stage | ||
| I | 23.5 (4) | |
| II | 11.8 (2) | |
| III | 17.6 (3) | |
| IV | 29.4 (5) | |
| Unsure | 17.6 (3) | |
| Treatment Related Variables (survivors n = 17) | ||
| Time off treatment (months) | M = 16.9 (±16.4) | |
| Time off treatment category | ||
| ≤6 months | 41.2 (7) | |
| >6 months | 58.8 (10) | |
| Chemotherapy (yes) | 100 (17) | |
| Surgery (yes) | 35.3 (6) | |
| Radiation (yes) | 17.6 (3) | |
| Hormone Therapy (yes) | 11.8 (2) | |
| Immunotherapy (yes) | 5.9 (1) | |
| Mucositis (during and/or after treatment) (yes) | 23.5 (4) | |
| Health Related Variables | Survivors (n = 17) % (n) | Controls (n = 18) % (n) |
| Probiotics (within ≤2 years) (yes) | 23.5 (4) | 38.9 (7) |
| Antibiotics (within ≤2 years) (yes) | 52.9 (9) | 50.0 (9) |
| Corticosteroid medication (within ≤2 years) (yes) | 23.5 (4) | 5.6 (1) |
| Smoking | ||
| No | 94.1 (16) | 72.2 (13) |
| Yes | 0 | 11.1 (2) |
| Sometimes | 5.9 (1) | 16.7 (3) |
| Breastfed as infant (yes) | 58.8 (10) | 100 (18) |
| Birth delivery mode | ||
| Vaginally | 64.7 (11) | 88.9 (16) |
| Caesarean section | 29.4 (5) | 11.2 (2) |
| Unsure | 5.9 (1) | 0 |
| Body Mass Index (BMI) | M = 25.6 (±6.0) | M = 24.4 (±2.8) |
| Waist to Hip Ratio (WHR) | M = 0.85 (±0.1) | M = 0.82 (±0.1) |
| WHR risk category | ||
| Low | 41.2 (7) | 88.9 (16) |
| Moderate | 11.8 (2) | 5.6 (1) |
| High | 17.6 (3) | 0 |
| Missing | 29.4 (5) | 5.6 (1) |
| Psychosocial Outcomes | Chao1 | Shannon Index |
|---|---|---|
| Anxiety | r = −0.11, p = 0.53 | r = −0.12, p = 0.51 |
| Depressive symptoms | r= −0.13, p= 0.45 | r = −0.15, p = 0.40 |
| Depressive functional | r = −0.47, p = 0.004 | r = −0.39, p = 0.022 |
| PTSD symptoms | r = −0.18, p = 0.39 | r = −0.18, p = 0.41 |
| Fatigue | r = 0.10, p = 0.57 | r = 0.13, p = 0.44 |
| Social isolation | r = −0.09, p = 0.61 | r = −0.08, p = 0.67 |
| Pain behavior | r = −0.23, p = 0.60 | r = −0.17, p = 0.50 |
| Cognitive function | r = 0.34, p = 0.048 | r = 0.33, p = 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deleemans, J.M.; Chleilat, F.; Reimer, R.A.; Baydoun, M.; Piedalue, K.-A.; Lowry, D.E.; Henning, J.-W.; Carlson, L.E. The Chemo-Gut Pilot Study: Associations between Gut Microbiota, Gastrointestinal Symptoms, and Psychosocial Health Outcomes in a Cross-Sectional Sample of Young Adult Cancer Survivors. Curr. Oncol. 2022, 29, 2973-2994. https://doi.org/10.3390/curroncol29050243
Deleemans JM, Chleilat F, Reimer RA, Baydoun M, Piedalue K-A, Lowry DE, Henning J-W, Carlson LE. The Chemo-Gut Pilot Study: Associations between Gut Microbiota, Gastrointestinal Symptoms, and Psychosocial Health Outcomes in a Cross-Sectional Sample of Young Adult Cancer Survivors. Current Oncology. 2022; 29(5):2973-2994. https://doi.org/10.3390/curroncol29050243
Chicago/Turabian StyleDeleemans, Julie M., Faye Chleilat, Raylene A. Reimer, Mohamad Baydoun, Katherine-Ann Piedalue, Dana E. Lowry, Jan-Willem Henning, and Linda E. Carlson. 2022. "The Chemo-Gut Pilot Study: Associations between Gut Microbiota, Gastrointestinal Symptoms, and Psychosocial Health Outcomes in a Cross-Sectional Sample of Young Adult Cancer Survivors" Current Oncology 29, no. 5: 2973-2994. https://doi.org/10.3390/curroncol29050243
APA StyleDeleemans, J. M., Chleilat, F., Reimer, R. A., Baydoun, M., Piedalue, K.-A., Lowry, D. E., Henning, J.-W., & Carlson, L. E. (2022). The Chemo-Gut Pilot Study: Associations between Gut Microbiota, Gastrointestinal Symptoms, and Psychosocial Health Outcomes in a Cross-Sectional Sample of Young Adult Cancer Survivors. Current Oncology, 29(5), 2973-2994. https://doi.org/10.3390/curroncol29050243