Robot-Assisted Radical Prostatectomy for Potential Cancer Control in Patients with Metastatic Prostate Cancer

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Histopathology
2.3. Follow-Up
2.4. Endpoints and Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Surgical and Pathological Outcomes
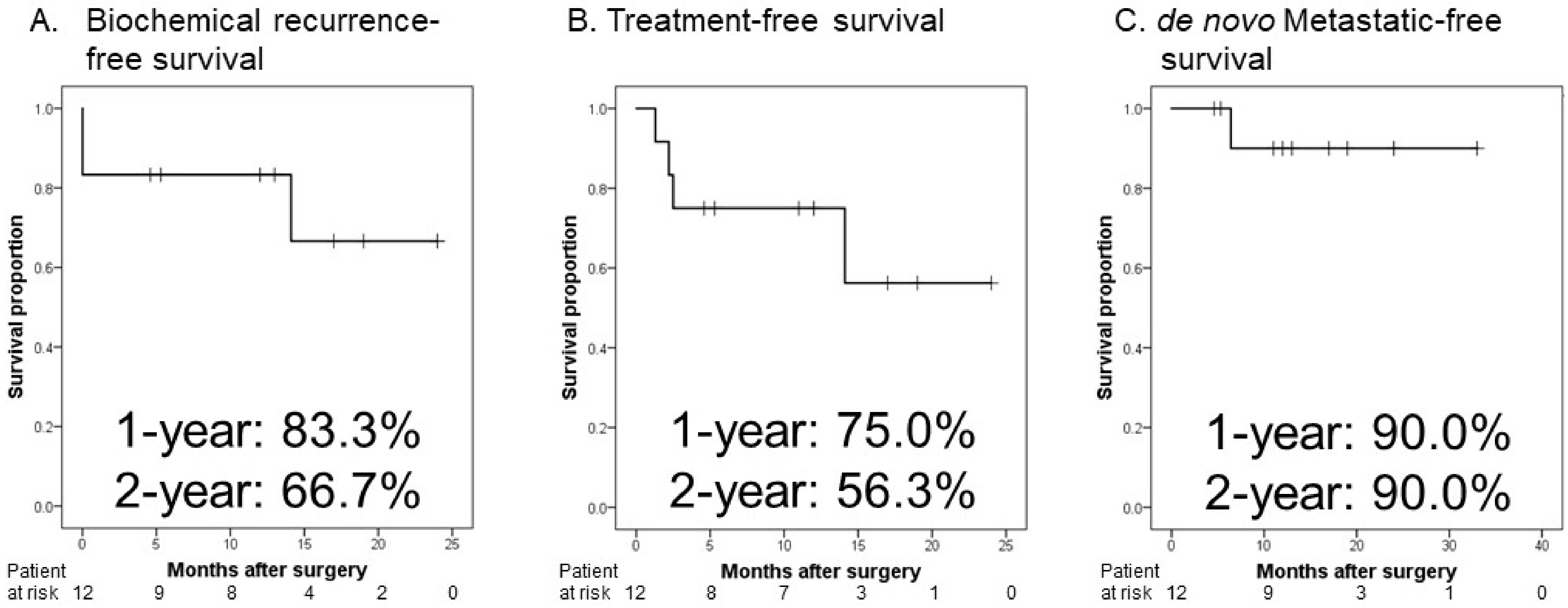
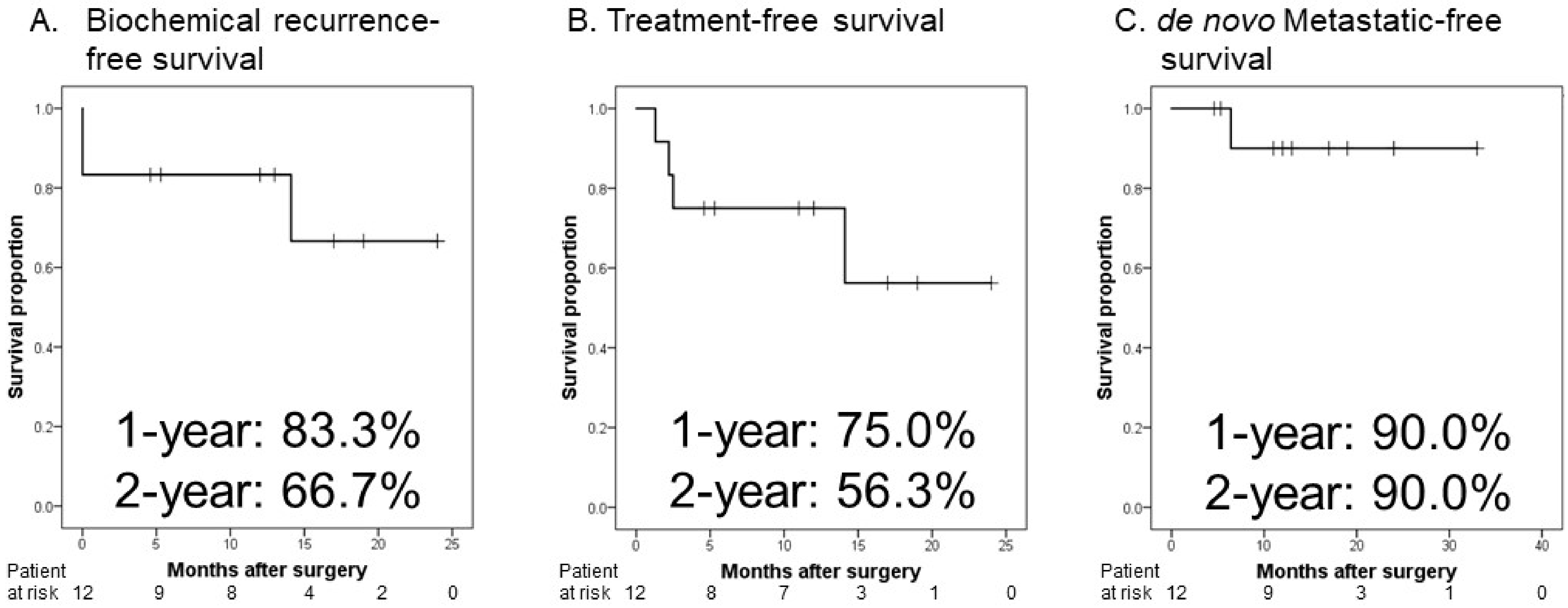
3.3. Oncological Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Prostate Cancer. NCCN Guidelines® 2022. Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 12 March 2022).
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; Spears, M.R.; Clarke, N.W.; Dearnaley, D.P.; De Bono, J.S.; Gale, J.; Hetherington, J.; Hoskin, P.J.; Jones, R.J.; Laing, R.; et al. Survival with Newly Diagnosed Metastatic Prostate Cancer in the “Docetaxel Era”: Data from 917 Patients in the Control Arm of the STAMPEDE Trial (MRC PR08, CRUK/06/019). Eur. Urol. 2015, 67, 1028–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Culp, S.H.; Schellhammer, P.F.; Williams, M.B. Might men diagnosed with metastatic prostate cancer benefit from definitive treatment of the primary tumor? A SEER-based study. Eur. Urol. 2014, 65, 1058–1066. [Google Scholar] [CrossRef] [PubMed]
- Satkunasivam, R.; Kim, A.E.; Desai, M.; Nguyen, M.M.; Quinn, D.I.; Ballas, L.; Lewinger, J.P.; Stern, M.C.; Hamilton, A.S.; Aron, M.; et al. Radical Prostatectomy or External Beam Radiation Therapy vs No Local Therapy for Survival Benefit in Metastatic Prostate Cancer: A SEER-Medicare Analysis. J. Urol. 2015, 194, 378–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, I.M.; Tangen, C.; Basler, J.; Crawford, E.D. Impact of previous local treatment for prostate cancer on subsequent metastatic disease. J. Urol. 2002, 168, 1008–1012. [Google Scholar] [CrossRef]
- Blanchard, P.; Bossi, A.; Fizazi, K. Radiation therapy to the primary in metastatic prostate cancer: Palliation only or altering tumor biology? Curr. Opin. Urol. 2017, 27, 580–586. [Google Scholar] [CrossRef]
- Predina, J.D.; Kapoor, V.; Judy, B.F.; Cheng, G.; Fridlender, Z.G.; Albelda, S.M.; Singhal, S. Cytoreduction surgery reduces systemic myeloid suppressor cell populations and restores intratumoral immunotherapy effectiveness. J. Hematol. Oncol. 2012, 5, 34. [Google Scholar] [CrossRef] [Green Version]
- Oken, M.M.; Creech, R.H.; Tormeym, D.C.; Horton, J.; Davis, T.T.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Buyyounouski, M.K.; Choyke, P.L.; McKenney, J.K.; Sartor, O.; Sandler, H.M.; Amin, M.B.; Kattan, M.W.; Lin, D.W. Prostate cancer—major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 245–253. [Google Scholar] [CrossRef] [Green Version]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading Committee. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Poelaert, F.; Verbaeys, C.; Rappe, B.; Kimpe, B.; Billiet, I.; Plancke, H.; Decaestecker, K.; Fonteyne, V.; Buelens, S.; Lumen, N. Cytoreductive Prostatectomy for Metastatic Prostate Cancer: First Lessons Learned from the Multicentric Prospective Local Treatment of Metastatic Prostate Cancer (LoMP) Trial. Urology 2017, 106, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Buelens, S.; Poelaert, F.; Claeys, T.; De Bleser, E.; Dhondt, B.; Verla, W.; Ost, P.; Rappe, B.; De Troyer, B.; Verbaeys, C.; et al. Multicentre, prospective study on local treatment of metastatic prostate cancer (LoMP study). BJU Int. 2021, in press. [Google Scholar] [CrossRef]
- Heidenreich, A.; Pfister, D.; Porres, D. Cytoreductive radical prostatectomy in patients with prostate cancer and low volume skeletal metastases: Results of a feasibility and case-control study. J. Urol. 2015, 193, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Won, A.C.; Gurney, H.; Marx, G.; De Souza, P.; Patel, M.I. Primary treatment of the prostate improves local palliation in men who ultimately develop castrate-resistant prostate cancer. BJU Int. 2013, 112, E250–E255. [Google Scholar] [CrossRef]
- Hussain, M.; Tangen, C.M.; Higano, C.; Schelhammer, P.F.; Faulkner, J.; Crawford, E.D.; Wilding, G.; Akdas, A.; Small, E.J.; Donnelly, B.; et al. Absolute prostate-specific antigen value after androgen deprivation is a strong independent predictor of survival in new metastatic prostate cancer: Data from Southwest Oncology Group Trial 9346 (INT-0162). J. Clin. Oncol. 2006, 24, 3984–3990. [Google Scholar] [CrossRef] [PubMed]
- Löppenberg, B.; Dalela, D.; Karabon, P.; Sood, A.; Sammon, J.D.; Meyer, C.P.; Sun, M.; Noldus, J.; Peabody, J.O.; Trinh, Q.D.; et al. The Impact of Local Treatment on Overall Survival in Patients with Metastatic Prostate Cancer on Diagnosis: A National Cancer Data Base Analysis. Eur. Urol. 2017, 72, 14–19. [Google Scholar] [CrossRef]
- Kim, M.Y.; Oskarsson, T.; Acharyya, S.; Nguyen, D.X.; Zhang, X.H.F.; Norton, L.; Massagué, J. Tumor self-seeding by circulating cancer cells. Cell 2009, 139, 1315–1326. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, R.N.; Riba, R.D.; Zacharoulis, S.; Bramley, A.H.; Vincent, L.; Costa, C.; MacDonald, D.D.; Jin, D.K.; Shido, K.; Kerns, S.A.; et al. VEGFR1-positive haematopoietic bone marrow progenitors initiate the pre-metastatic niche. Nature 2005, 438, 820–827. [Google Scholar] [CrossRef]
- McAllister, S.S.; Gifford, A.M.; Greiner, A.L.; Kelleher, S.P.; Saelzler, M.P.; Ince, T.A.; Reinhardt, F.; Harris, L.N.; Hylander, B.L.; Repasky, E.A.; et al. Systemic endocrine instigation of indolent tumor growth requires osteopontin. Cell 2008, 133, 994–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walz, J.; Pignot, G.; Fakhfakh, S.; Campagna, J.; Guerin, M.; Vicier, C.; Brunelle, S.; Salem, N.; Gravis, G. Metastatic hormone sensitive prostate cancer: Local treatment strategies. World J. Urol. 2021, 39, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Preisser, F.; Mazzone, E.; Nazzani, S.; Bandini, M.; Tian, Z.; Marchioni, M.; Steuber, T.; Saad, F.; Montorsi, F.; Shariat, S.F.; et al. Comparison of Perioperative Outcomes Between Cytoreductive Radical Prostatectomy and Radical Prostatectomy for Nonmetastatic Prostate Cancer. Eur. Urol. 2018, 74, 693–696. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | |
|---|---|
| Age (year, median, IQR) | 74.5 (62.0–78.8) |
| Body mass index (kg/m2, median, IQR) | 23.8 (22.5–25.0) |
| Initial PSA (ng/mL, median, IQR) | 185.300 (34.944–333.379) |
| Clinical T stage (number, %) | |
| Biopsy Gleason score (%) | |
| 4 + 3 | 2 (16.7) |
| 4 + 4 | 2 (16.7) |
| 4 + 5 | 6 (49.9) |
| 5 + 4 | 2 (16.7) |
| Clinical T stage (number, %) | |
| T2 | 5 (41.7) |
| T3 | 5 (41.7) |
| T4 | 2 (16.6) |
| Clinical N stage (number, %) | |
| N0 | 5 (41.7) |
| N1 | 7 (58.3) |
| Clinical M stage (number, %) | |
| M0 | 0 |
| M1 | 12 (100) |
| Metastatic sites (number, %) | |
| Lymph nodes | 7 (58.3) |
| Bone | 12 (100) |
| Number of bone metastasis (%) | |
| 1 | 5 (41.7) |
| 3 | 5 (41.7) |
| ≥5 | 2 (16.6) |
| Neoadjuvant therapy (number, 5) | |
| Combined androgen blockade | 4 (33.3) |
| ARPI | 3 (25.0) |
| Chemohormonal therapy | 5 (41.7) |
| Duration of neoadjuvant therapy (months, median, IQR) | 7.3 (6.1–27.2) |
| Variables | |
|---|---|
| Proximate PSA before RARP (ng/mL, median, IQR) | 0.017 (0.007–0.194) |
| Console time (min, median, IQR) | 85.0 (70.3–112.0) |
| EBL (mL, median, IQR) | 23 (7–45) |
| pathological T stage (number, %) | |
| T0 | 5 (41.7) |
| T2 | 5 (41.7) |
| T3 | 2 (16.7) |
| Pathological Gleason score (%) | |
| 0 | 5 (41.7) |
| 3 + 4 | 1 (8.3) |
| 4 + 3 | 2 (16.7) |
| 5 + 3 | 1 (8.3) |
| Positive surgical margin (number, %) | 1 (8.3) |
| Adjuvant ADT (number, %) | 3 (25.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takagi, K.; Kawase, M.; Kato, D.; Kawase, K.; Takai, M.; Iinuma, K.; Nakane, K.; Hagiwara, N.; Yamada, T.; Tomioka, M.; et al. Robot-Assisted Radical Prostatectomy for Potential Cancer Control in Patients with Metastatic Prostate Cancer. Curr. Oncol. 2022, 29, 2864-2870. https://doi.org/10.3390/curroncol29040233
Takagi K, Kawase M, Kato D, Kawase K, Takai M, Iinuma K, Nakane K, Hagiwara N, Yamada T, Tomioka M, et al. Robot-Assisted Radical Prostatectomy for Potential Cancer Control in Patients with Metastatic Prostate Cancer. Current Oncology. 2022; 29(4):2864-2870. https://doi.org/10.3390/curroncol29040233
Chicago/Turabian StyleTakagi, Kimiaki, Makoto Kawase, Daiki Kato, Kota Kawase, Manabu Takai, Koji Iinuma, Keita Nakane, Noriyasu Hagiwara, Toru Yamada, Masayuki Tomioka, and et al. 2022. "Robot-Assisted Radical Prostatectomy for Potential Cancer Control in Patients with Metastatic Prostate Cancer" Current Oncology 29, no. 4: 2864-2870. https://doi.org/10.3390/curroncol29040233
APA StyleTakagi, K., Kawase, M., Kato, D., Kawase, K., Takai, M., Iinuma, K., Nakane, K., Hagiwara, N., Yamada, T., Tomioka, M., & Koie, T. (2022). Robot-Assisted Radical Prostatectomy for Potential Cancer Control in Patients with Metastatic Prostate Cancer. Current Oncology, 29(4), 2864-2870. https://doi.org/10.3390/curroncol29040233