Pain Relief after Stereotactic Radiotherapy of Pancreatic Adenocarcinoma: An Updated Systematic Review

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Results
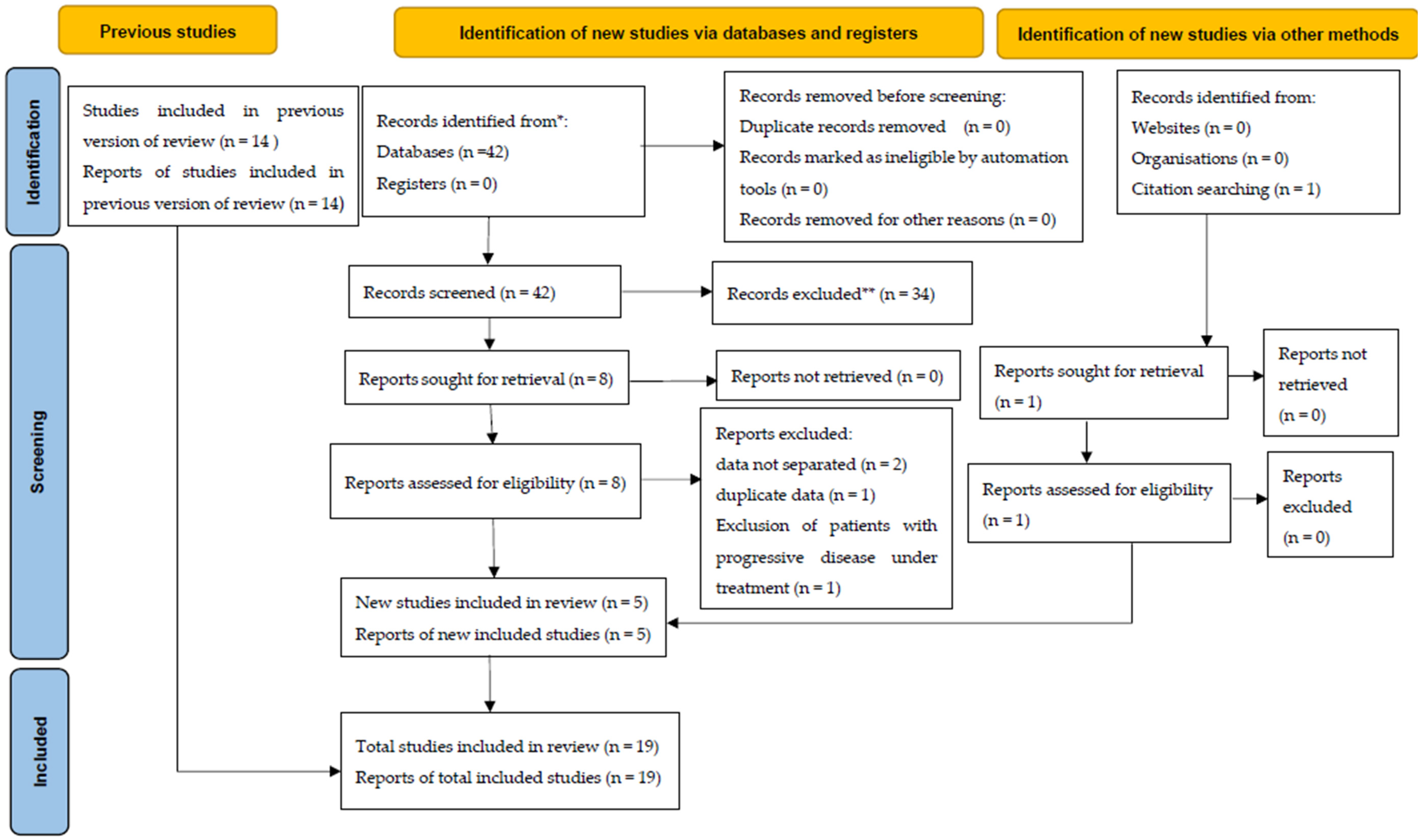
2.1. Search Results
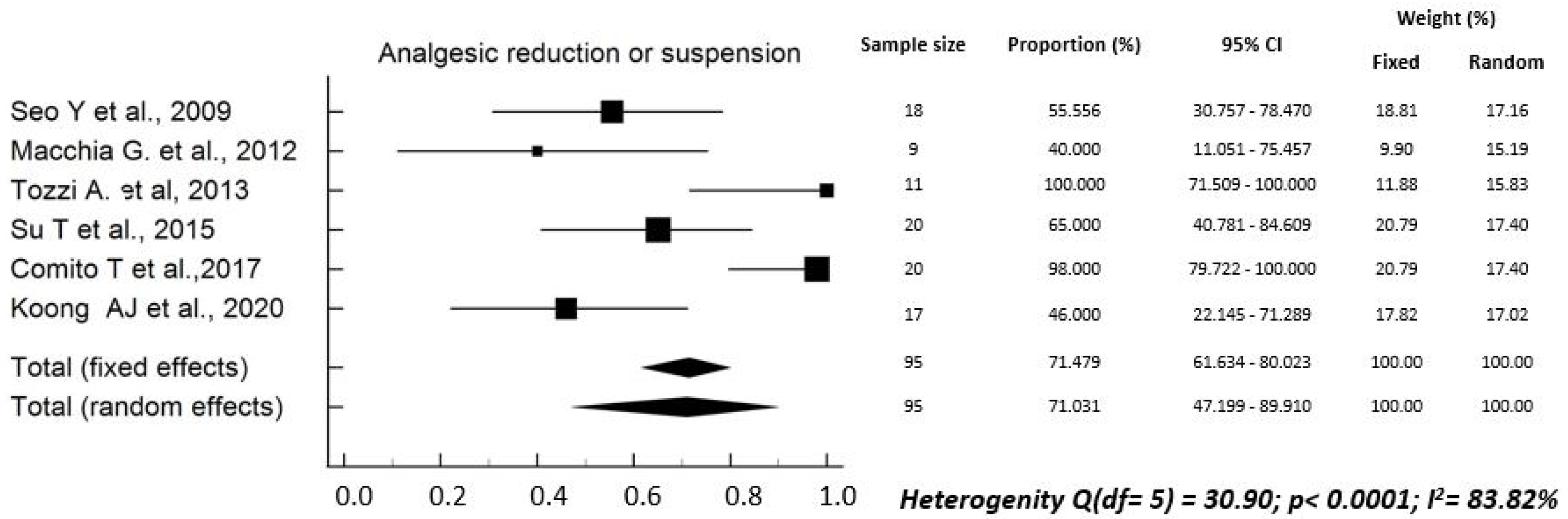
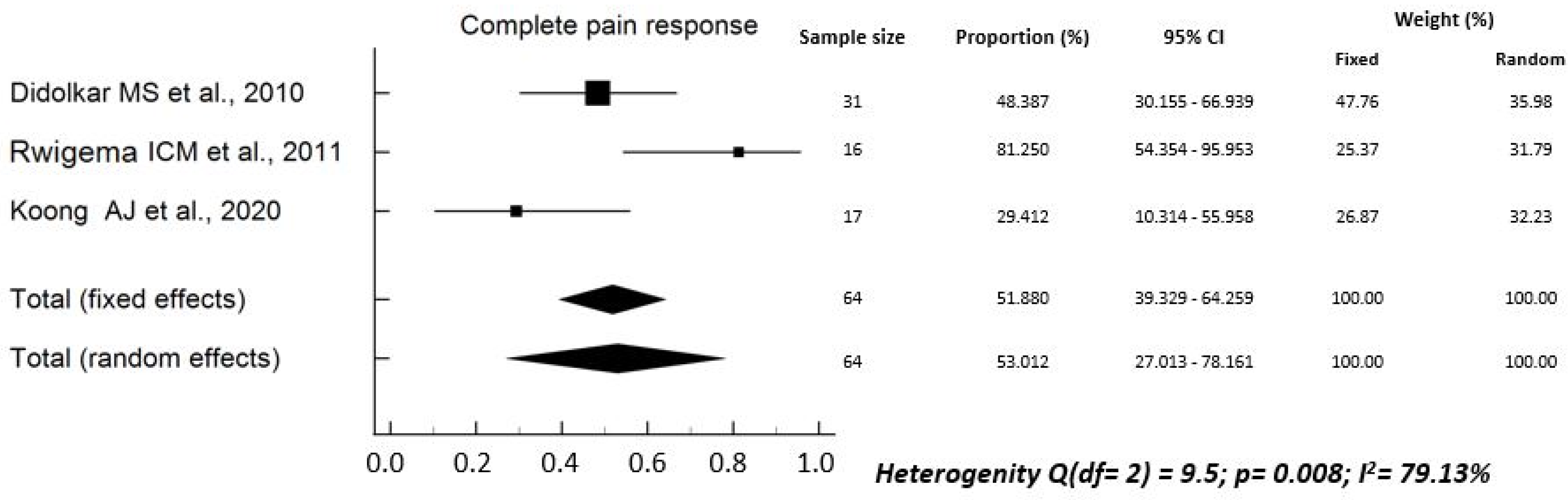
2.2. Pain Relief
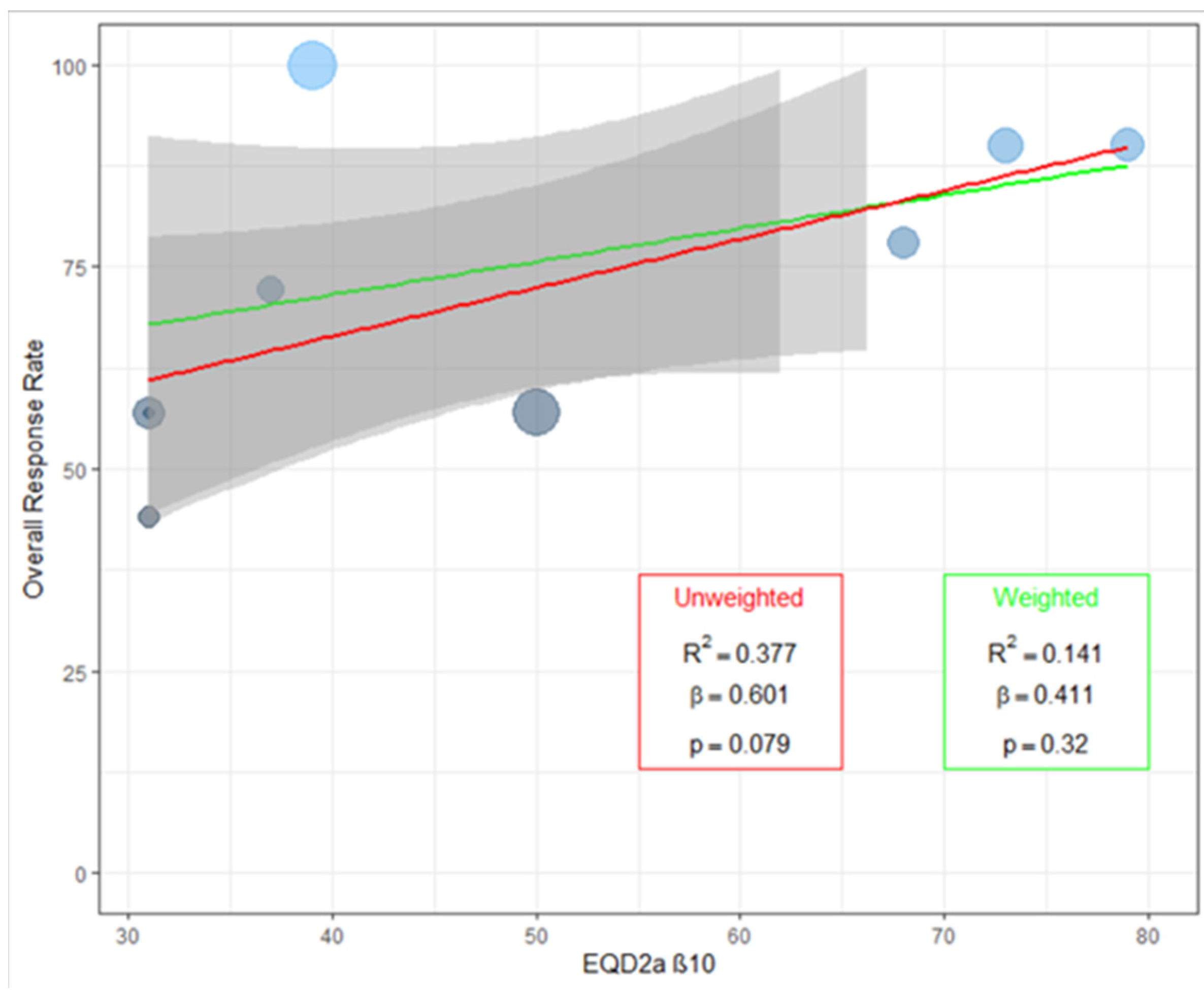
2.3. Impact of Radiotherapy Dose on Pain Relief
2.4. Pain-Free Survival
2.5. Toxicity
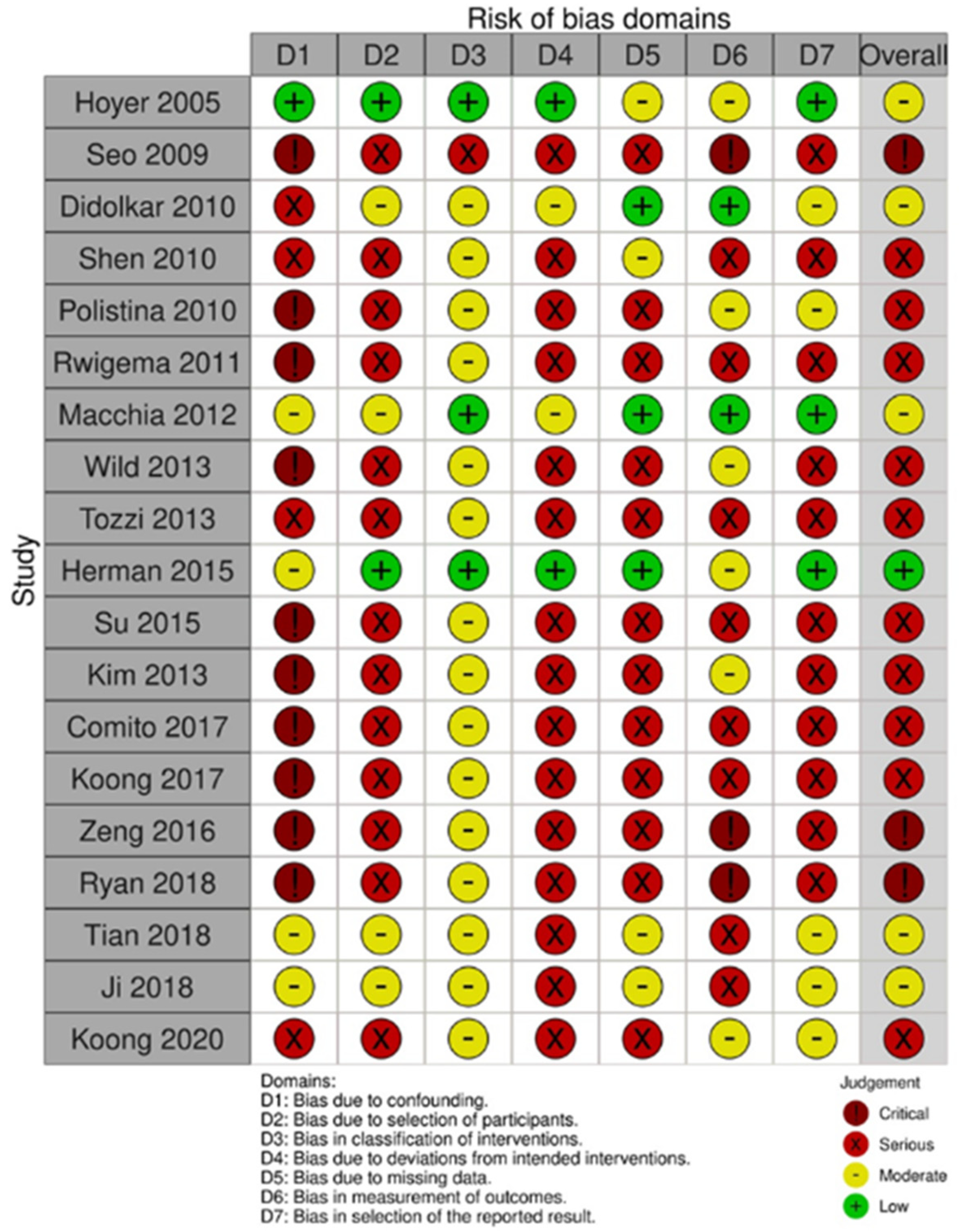
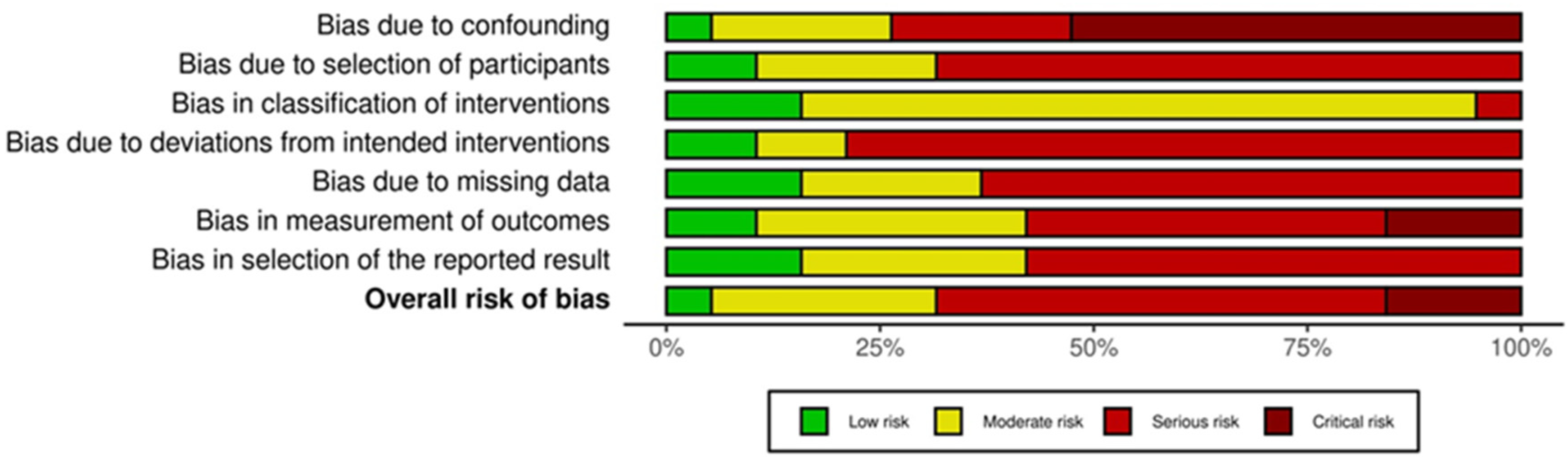
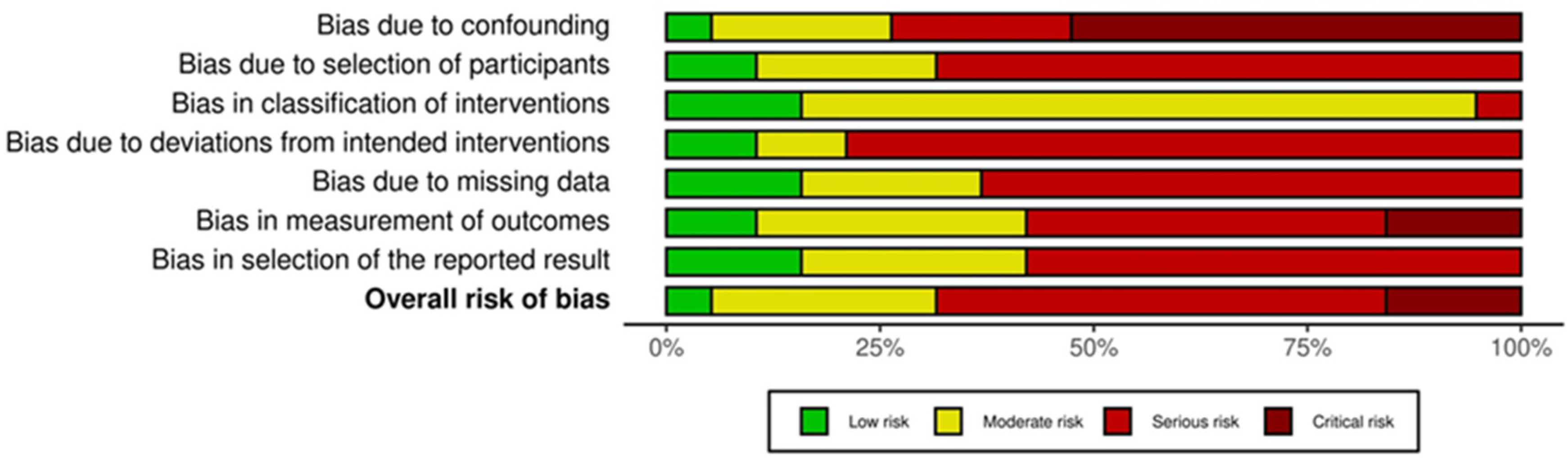
2.6. Quality Assessment of the Analyzed Studies
3. Discussion
4. Materials and Methods
4.1. Endpoints
4.2. Selection Criteria
4.3. Literature Search and Data Extraction
4.4. Statistical Analysis
4.5. Quality Assessment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Lee, K.G.; Roy, V.; Laszlo, M.; Atkins, K.M.; Lin, K.J.; Tomassian, S.; Hendifar, A.E. Symptom Management in Pancreatic Cancer. Curr. Treat. Options Oncol. 2021, 22, 8. [Google Scholar] [CrossRef]
- Carrato, A.; Melisi, D.; Prager, G.; Westphalen, C.B.; Ferreras, A.; D’Esquermes, N.; Taieb, J.; Mercadé, T.M. Chart review of diagnostic methods, baseline characteristics and symptoms for European patients with pancreatic cancer. Future Oncol. 2021, 17, 1843–1854. [Google Scholar] [CrossRef]
- Koulouris, A.I.; Banim, P.; Hart, A.R. Pain in Patients with Pancreatic Cancer: Prevalence, Mechanisms, Management and Future Developments. Dig. Dis. Sci. 2017, 62, 861–870. [Google Scholar] [CrossRef]
- Coveler, A.L.; Mizrahi, J.; Eastman, B.; Apisarnthanarax, S.J.; Dalal, S.; McNearney, T.; Pant, S. Precision Promise Consortium. Pancreas Cancer-Associated Pain Management. Oncologist 2021, 26, e971–e982. [Google Scholar]
- Costamagna, G.; Alevras, P.; Palladino, F.; Rainoldi, F.; Mutignani, M.; Morganti, A. Endoscopic pancreatic stenting in pancreatic cancer. Can. J. Gastroenterol. 1999, 13, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Drewes, A.M.; Campbell, C.M.; Ceyhan, G.O.; Delhaye, M.; Garg, P.K.; van Goor, H.; Laquente, B.; Morlion, B.; Olesen, S.S.; Singh, V.K.; et al. Pain in pancreatic ductal adenocarcinoma: A multidisciplinary, International guideline for optimized management. Pancreatology 2018, 18, 446–457. [Google Scholar] [CrossRef]
- Nagels, W.; Pease, N.; Bekkering, G.; Cools, F.; Dobbels, P. Celiac plexus neurolysis for abdominal cancer pain: A systematic review. Pain Med. 2013, 14, 1140–1163. [Google Scholar] [CrossRef] [Green Version]
- Morganti, A.G.; Trodella, L.; Valentini, V.; Barbi, S.; Macchia, G.; Mantini, G.; Turriziani, A.; Cellini, N. Pain relief with short-term irradiation in locally advanced carcinoma of the pancreas. J. Palliat. Care 2003, 19, 258–262. [Google Scholar] [CrossRef]
- Ceha, H.M.; van Tienhoven, G.; Gouma, D.J.; Veenhof, C.H.; Schneider, C.J.; Rauws, E.A.; Phoa, S.S.; González González, D. Feasibility and efficacy of high dose conformal radiotherapy for patients with locally advanced pancreatic carcinoma. Cancer 2000, 89, 2222–2229. [Google Scholar] [CrossRef]
- Wolny-Rokicka, E.; Sutkowski, K.; Grządziel, A.; Dorsz, Ż.; Tukiendorf, A.; Lipiński, J.; Wydmański, J. Tolerance and efficacy of palliative radiotherapy for advanced pancreatic cancer: A retrospective analysis of single-institutional experiences. Mol. Clin. Oncol. 2016, 4, 1088–1092. [Google Scholar] [CrossRef] [Green Version]
- Lischalk, J.W.; Burke, A.; Chew, J.; Elledge, C.; Gurka, M.; Marshall, J.; Pishvaian, M.; Collins, S.; Unger, K. Five-Fraction Stereotactic Body Radiation Therapy (SBRT) and Chemotherapy for the Local Management of Metastatic Pancreatic Cancer. J. Gastrointest. Cancer 2018, 49, 116–123. [Google Scholar] [CrossRef]
- Buwenge, M.; Macchia, G.; Arcelli, A.; Frakulli, R.; Fuccio, L.; Guerri, S.; Grassi, E.; Cammelli, S.; Cellini, F.; Morganti, A.G. Stereotactic radiotherapy of pancreatic cancer: A systematic review on pain relief. J. Pain Res. 2018, 11, 2169–2178. [Google Scholar] [CrossRef] [Green Version]
- National Library of Medicine. PubMed.gov. Available online: https://pubmed.ncbi.nlm.nih.gov/?term=stereotactic+radiotherapy+pancrea*&filter=dates.2018%2F1%2F1-2020%2F12%2F31&sort=pubdate&size=200 (accessed on 30 December 2020).
- Hoyer, M.; Roed, H.; Sengelov, L.; Traberg, A.; Ohlhuis, L.; Pedersen, J.; Nellemann, H.; Kiil Berthelsen, A.; Eberholst, F.; Engelholm, S.A.; et al. Phase-II study on stereotactic radiotherapy of locally advanced pancreatic carcinoma. Radiother. Oncol. 2005, 76, 48–53. [Google Scholar] [CrossRef]
- Seo, Y.; Kim, M.S.; Yoo, S.; Cho, C.; Yang, K.; Yoo, H.; Choi, C.; Lee, D.; Kim, J.; Kim, M.S.; et al. Stereotactic body radiation therapy boost in locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1456–1461. [Google Scholar] [CrossRef]
- Didolkar, M.S.; Coleman, C.W.; Brenner, M.J.; Chu, K.U.; Olexa, N.; Stanwyck, E.; Yu, A.; Neerchal, N.; Rabinowitz, S. Image-guided stereotactic radiosurgery for locally advanced pancreatic adenocarcinoma results of first 85 patients. J. Gastrointest. Surg. 2010, 14, 1547–1559. [Google Scholar] [CrossRef]
- Shen, Z.T.; Wu, X.H.; Li, B.; Wang, L.; Zhu, X.X. Preliminary efficacy of CyberKnife radiosurgery for locally advanced pancreatic cancer. Chin. J. Cancer 2010, 29, 802–809. [Google Scholar] [CrossRef]
- Polistina, F.; Costantin, G.; Casamassima, F.; Francescon, P.; Guglielmi, R.; Panizzoni, G.; Febbraro, A.; Ambrosino, G. Unresectable locally advanced pancreatic cancer: A multimodal treatment using neoadjuvant chemoradiotherapy (gemcitabine plus stereotactic radiosurgery) and subsequent surgical exploration. Ann. Surg. Oncol. 2010, 17, 2092–2101. [Google Scholar] [CrossRef]
- Rwigema, J.C.; Parikh, S.D.; Heron, D.E.; Howell, M.; Zeh, H.; Moser, A.J.; Bahary, N.; Quinn, A.; Burton, S.A. Stereotactic body radiotherapy in the treatment of advanced adenocarcinoma of the pancreas. Am. J. Clin. Oncol. 2011, 34, 63–69. [Google Scholar] [CrossRef]
- Macchia, G.; Morganti, A.G.; Cilla, S.; Ippolito, E.; Massaccesi, M.; Picardi, V.; Mattiucci, G.C.; Bonomo, P.; Tambaro, R.; Pacelli, F.; et al. Quality of life and toxicity of stereotactic radiotherapy in pancreatic tumors: A case series. Cancer Investig. 2012, 30, 149–155. [Google Scholar] [CrossRef]
- Wild, A.T.; Hiniker, S.M.; Chang, D.T.; Tran, P.T.; Khashab, M.A.; Limaye, M.R.; Laheru, D.A.; Le, D.T.; Kumar, R.; Pai, J.S.; et al. Re-irradiation with stereotactic body radiation therapy as a novel treatment option for isolated local recurrence of pancreatic cancer after multimodality therapy: Experience from two institutions. J. Gastrointest. Oncol. 2013, 4, 343–351. [Google Scholar]
- Tozzi, A.; Comito, T.; Alongi, F.; Navarria, P.; Iftode, C.; Mancosu, P.; Reggiori, G.; Clerici, E.; Rimassa, L.; Zerbi, A.; et al. SBRT in unresectable advanced pancreatic cancer: Preliminary results of a mono-institutional experience. Radiat. Oncol. 2013, 8, 148. [Google Scholar] [CrossRef] [Green Version]
- Herman, J.M.; Chang, D.T.; Goodman, K.A.; Dholakia, A.S.; Raman, S.P.; Hacker-Prietz, A.; Iacobuzio-Donahue, C.A.; Griffith, M.E.; Pawlik, T.M.; Pai, J.S.; et al. Phase 2 multi-institutional trial evaluating gemcitabine and stereotactic body radiotherapy for patients with locally advanced unresectable pancreatic adenocarcinoma. Cancer 2015, 121, 1128–1137. [Google Scholar] [CrossRef]
- Su, T.S.; Liang, P.; Lu, H.Z.; Liang, J.N.; Liu, J.M.; Zhou, Y.; Gao, Y.C.; Tang, M.Y. Stereotactic body radiotherapy using CyberKnife for locally advanced unresectable and metastatic pancreatic cancer. World J. Gastroenterol. 2015, 21, 8156–8162. [Google Scholar] [CrossRef]
- Kim, C.H.; Ling, D.C.; Wegner, R.E.; Flickinger, J.C.; Burton, S.A. Stereotactic body radiotherapy in the treatment of pancreatic adenocarcinoma in elderly patients. Radiat. Oncol. 2013, 8, 240. [Google Scholar] [CrossRef] [Green Version]
- Comito, T.; Cozzi, L.; Zerbi, A.; Franzese, C.; Clerici, E.; Tozzi, A.; Iftode, C.; Navarria, P.; D’Agostino, G.; Fogliata, A.; et al. Clinical results of stereotactic body radiotherapy (SBRT) in the treatment of isolated local recurrence of pancreatic cancer after R0 surgery: A retrospective study. Eur. J. Surg. Oncol. 2017, 43, 735–742. [Google Scholar] [CrossRef]
- Koong, A.J.; Toesca, D.A.S.; von Eyben, R.; Pollom, E.L.; Chang, D.T. Re-irradiation with stereotactic body radiation therapy after prior conventional fractionation radiation for locally recurrent pancreatic adenocarcinoma. Adv. Radiat. Oncol. 2017, 18, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Zeng, X.L.; Wang, H.H.; Meng, M.B.; Wu, Z.Q.; Song, Y.C.; Zhuang, H.Q.; Qian, D.; Li, F.T.; Zhao, L.J.; Yuan, Z.Y.; et al. Stereotactic body radiation therapy for patients with recurrent pancreatic adenocarcinoma at the abdominal lymph nodes or postoperative stump including pancreatic stump and other stump. OncoTargets Ther. 2016, 9, 3985–3992. [Google Scholar]
- Ryan, J.F.; Rosati, L.M.; Groot, V.P.; Le, D.T.; Zheng, L.; Laheru, D.A.; Shin, E.J.; Jackson, J.; Moore, J.; Narang, A.K.; et al. Stereotactic body radiation therapy for palliative management of pancreatic adenocarcinoma in elderly and medically inoperable patients. Oncotarget 2018, 9, 16427–16436. [Google Scholar] [CrossRef] [Green Version]
- Tian, Q.; Zhang, F.; Wang, Y. Clinical assessment of palliative radiotherapy for pancreatic cancer. Cancer Radiother. 2018, 22, 778–783. [Google Scholar] [CrossRef]
- Ji, K.; Shao, Y.J.; Hao, J.L.; Cheng, X.J.; Guan, B.Q.; Liu, W.S.; Chen, L.; Wang, X.; Song, Y.C.; Wang, K.; et al. Celiac Plexus Block After Stereotactic Body Radiotherapy Improves Pain Relief in Locally Advanced Pancreatic Cancer. J. Pain Res. 2020, 13, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Koong, A.J.; Toesca, D.A.S.; Baclay, J.R.M.; Pollom, E.L.; von Eyben, R.; Koong, A.C.; Chang, D.T. The Utility of Stereotactic Ablative Radiation Therapy for Palliation of Metastatic Pancreatic Adenocarcinoma. Pract. Radiat. Oncol. 2020, 10, 274–281. [Google Scholar] [CrossRef]
- Rao, A.D.; Sugar, E.A.; Chang, D.T.; Goodman, K.A.; Hacker-Prietz, A.; Rosati, L.M.; Columbo, L.; O’Reilly, E.; Fisher, G.A.; Zheng, L.; et al. Patient-reported outcomes of a multicenter phase 2 study investigating gemcitabine and stereotactic body radiation therapy in locally advanced pancreatic cancer. Pract. Radiat. Oncol. 2016, 6, 417–424. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.C.; Jen, Y.M.; Li, M.H.; Chao, H.L.; Tsai, J.T. Comparing outcomes of stereotactic body radiotherapy with intensity-modulated radiotherapy for patients with locally advanced unresectable pancreatic cancer. Eur. J. Gastroenterol. Hepatol. 2015, 27, 259–264. [Google Scholar] [CrossRef]
- Arcelli, A.; Buwenge, M.; Macchia, G.; Bertini, F.; Guido, A.; Deodato, F.; Cilla, S.; Scotti, V.; Rosetto, M.E.; Djan, I.; et al. Stereotactic body radiotherapy vs conventionally fractionated chemoradiation in locally advanced pancreatic cancer: A multicenter case-control study (PAULA-1). Cancer Med. 2020, 9, 7879–7887. [Google Scholar] [CrossRef]
- Park, J.J.; Hajj, C.; Reyngold, M.; Shi, W.; Zhang, Z.; Cuaron, J.J.; Crane, C.H.; O’Reilly, E.M.; Lowery, M.A.; Yu, K.H.; et al. Stereotactic body radiation vs. intensity-modulated radiation for unresectable pancreatic cancer. Acta Oncol. 2017, 56, 1746–1753. [Google Scholar] [CrossRef]
- Serrano, P.E.; Herman, J.M.; Griffith, K.A.; Zalupski, M.M.; Kim, E.J.; Bekaii-Saab, T.S.; Ben-Josef, E.; Dawson, L.A.; Ringash, J.; Wei, A.C. Quality of life in a prospective, multicenter phase 2 trial of neoadjuvant full-dose gemcitabine, oxaliplatin, and radiation in patients with resectable or borderline resectable pancreatic adenocarcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 270–277. [Google Scholar] [CrossRef] [Green Version]
- De Geus, S.W.L.; Eskander, M.F.; Kasumova, G.G.; Ng, S.C.; Kent, T.S.; Mancias, J.D.; Callery, M.P.; Mahadevan, A.; Tseng, J.F. Stereotactic body radiotherapy for unresected pancreatic cancer: A nationwide review. Cancer 2017, 123, 4158–4167. [Google Scholar] [CrossRef] [Green Version]
- Zhong, J.; Patel, K.; Switchenko, J.; Cassidy, R.J.; Hall, W.A.; Gillespie, T.; Patel, P.R.; Kooby, D.; Landry, J. Outcomes for patients with locally advanced pancreatic adenocarcinoma treated with stereotactic body radiation therapy versus conventionally fractionated radiation. Cancer 2017, 123, 3486–3493. [Google Scholar] [CrossRef]
- Chapman, B.C.; Gleisner, A.; Rigg, D.; Meguid, C.; Goodman, K.; Brauer, B.; Gajdos, C.; Schulick, R.D.; Edil, B.H.; McCarter, M.D. Perioperative outcomes and survival following neoadjuvant stereotactic body radiation therapy (SBRT) versus intensity-modulated radiation therapy (IMRT) in pancreatic adenocarcinoma. J. Surg. Oncol. 2018, 117, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Baine, M.J.; Zhao, N.; Li, S.; Li, X.; Lin, C. Lymphocyte-sparing effect of stereotactic body radiation therapy compared to conventional fractionated radiation therapy in patients with locally advanced pancreatic cancer. BMC Cancer 2019, 19, 977. [Google Scholar] [CrossRef] [Green Version]
- Gourgou-Bourgade, S.; Bascoul-Mollevi, C.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Boige, V.; et al. Impact of FOLFIRINOX compared with gemcitabine on quality of life in patients with metastatic pancreatic cancer: Results from the PRODIGE 4/ACCORD 11 randomized trial. J. Clin. Oncol. 2013, 31, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Meader, N.; King, K.; Llewellyn, A.; Norman, G.; Brown, J.; Rodgers, M.; Moe-Byrne, T.; Higgins, J.P.; Sowden, A.; Stewart, G. A checklist designed to aid consistency and reproducibility of GRADE assessments: Development and pilot validation. Syst. Rev. 2014, 3, 82. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Patients (with Pain) | Pain Evaluation Methods | Pain Response Outcomes | Quality of Evidence (GRADE) |
|---|---|---|---|---|
| Hoyer et al., 2005 [16] | 22 (15) | Scale: WHO; Timing: baseline and after treatment (14 days, 2 and 3 months) | First evaluation after treatment: significant worsening of pain (p = 0.008) and increased (non-significant) use of analgesics (p = 0.08). Evaluation at 3 months: pain reduction in 50% of patients. | Low |
| Seo et al., 2009 [17] | 30 (18) | Pain relief was evaluated by comparing analgesic consumptions before and after SBRT. | Analgesic consumption was reduced in 10 patients (55.6%) after SBRT. | Low |
| Didolkar et al., 2010 [18] | 85 (moderate-severe: 31) | Scale: 0–10 | Analysis performed in patients with pain score > 4: Complete pain relief (for at least 6 months): 48.4%, Partial pain relief: 51.6%. | Very low |
| Shen et al., 2010 [19] | 20 (15) | Scale: visual analog with numeric rating | Some degree of “pain relief” was recorded in 90% of treated patients | Low |
| Polistina et al., 2010 [20] | 23 (NR) | Scale: visual analog with numeric rating; recording of analgesic use. | Mean pretreatment pain score: 3.91 ± 2.41; mean post-treatment score (three months): 3.65 ± 2.81 [p > 0.05]). The authors reported a reduction in the consumption of analgesic drugs, but without showing the data. | Very low |
| Rwigema et al., 2011 [21] | 71 (16) | NR | Complete pain relief: 81.3% | Very low |
| Macchia et al., 2012 [22] | 16 (9) | Scales: visual analog with numerical rating; Pain score (symptom severity × frequency); Drug score (class of analgesics × frequency of intake) | Complete or partial pain relief: 44.4% Pain worsening: 6.2% Reduction in analgesic consumption: 40.0% | Moderate |
| Wild et al., 2013 [23] | 18 (7) | NR | Pain relief: 57.1% (4–8 weeks after SBRT) | Very low |
| Tozzi et al., 2013 [24] | 30 (11) | Scale: numerical rating score | Discontinuation of analgesic consumption: 63.6% Reduction in analgesic consumption: 36.4% | Very low |
| Herman et al., 2015 [25] | 49 (NR) | Scale: QLQ-PAN26 | Pain reduction from score 25 to score 17 (median values), statistically significant (p = 0.001), recorded 4 weeks after treatment. | High |
| Su et al., 2015 [26] | 25 (20) | Scale: numerical rating score | Discontinuation of analgesic consumption: 50.0% Reduction in analgesic consumption: 15.0% | Low |
| Kim et al., 2013 [27] | 26 (14) | NR | Abdominal pain relief: 80.0% Back pain relief: 75.0% Discontinuation of opioid consumption: 35.7% | |
| Comito et al., 2017 [28] | 31 (22) | Scale: numerical rating score | Discontinuation of analgesic consumption: 59.1% Reduction in analgesic consumption: 40.9% | Low |
| Koong et al., 2017 [29] | 23 (14) | NR | Complete pain relief: 57.1% Pain worsening: 7.1% | Low |
| Zeng et al., 2016 [30] | 24 (13) | Scale: visual analog with numeric rating | Both short-term (1 week after SBRT: 2.7 ± 1.3) and long-term (6 months after SBRT: 1.2 ± 1.4) mean pain scores were significantly reduced compared to pre-treatment values (7.2 ± 2.5) (p < 0.05) | Low |
| Ryan et al., 2018 [31] | 29 (11) | Scale: National Cancer Institute Common Terminology Criteria for Adverse Events | Pain relief: 72.7% (3 months after SBRT) | Very low |
| Tian et al., 2018 [32] | 31 (28) | Scale: Brief Pain Inventory questionnaires (before treatment and one and three months after treatment) | Pain relief: 57.0% (1 month after SBRT) | Low |
| Ji et al., 2018 [33] | 35 (35) | Scale: numerical rating score | Both mean and worst pain scores were significantly improved after SBRT (p < 0.05), in all assessments over time. Pain relief was further improved in a subset of patients undergoing both SBRT and celiac plexus block in the 2–4 weeks post-treatment interval. | Moderate |
| Koong et al., 2020 [34] | 27 (17) | Scale: Stanford Pain Score | Complete pain relief: 30.0% Partial pain relief: 70.0% | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buwenge, M.; Arcelli, A.; Cellini, F.; Deodato, F.; Macchia, G.; Cilla, S.; Galietta, E.; Strigari, L.; Malizia, C.; Cammelli, S.; et al. Pain Relief after Stereotactic Radiotherapy of Pancreatic Adenocarcinoma: An Updated Systematic Review. Curr. Oncol. 2022, 29, 2616-2629. https://doi.org/10.3390/curroncol29040214
Buwenge M, Arcelli A, Cellini F, Deodato F, Macchia G, Cilla S, Galietta E, Strigari L, Malizia C, Cammelli S, et al. Pain Relief after Stereotactic Radiotherapy of Pancreatic Adenocarcinoma: An Updated Systematic Review. Current Oncology. 2022; 29(4):2616-2629. https://doi.org/10.3390/curroncol29040214
Chicago/Turabian StyleBuwenge, Milly, Alessandra Arcelli, Francesco Cellini, Francesco Deodato, Gabriella Macchia, Savino Cilla, Erika Galietta, Lidia Strigari, Claudio Malizia, Silvia Cammelli, and et al. 2022. "Pain Relief after Stereotactic Radiotherapy of Pancreatic Adenocarcinoma: An Updated Systematic Review" Current Oncology 29, no. 4: 2616-2629. https://doi.org/10.3390/curroncol29040214
APA StyleBuwenge, M., Arcelli, A., Cellini, F., Deodato, F., Macchia, G., Cilla, S., Galietta, E., Strigari, L., Malizia, C., Cammelli, S., & Morganti, A. G. (2022). Pain Relief after Stereotactic Radiotherapy of Pancreatic Adenocarcinoma: An Updated Systematic Review. Current Oncology, 29(4), 2616-2629. https://doi.org/10.3390/curroncol29040214