Clinical Utility of Multigene Profiling Assays in Early-Stage Invasive Breast Cancer: An Ontario Health (Cancer Care Ontario) Clinical Practice Guideline


Abstract
:1. Introduction
2. Methods
2.1. The Program in Evidence-Based Care (PEBC)
2.2. Patient and Caregiver-Specific Consultation Group
2.3. Internal Review
2.4. External Review
3. Results
3.1. Patient and Caregiver-Specific Consultation Group
3.2. Internal Review
3.3. External Review
4. Recommendations and Key Evidence
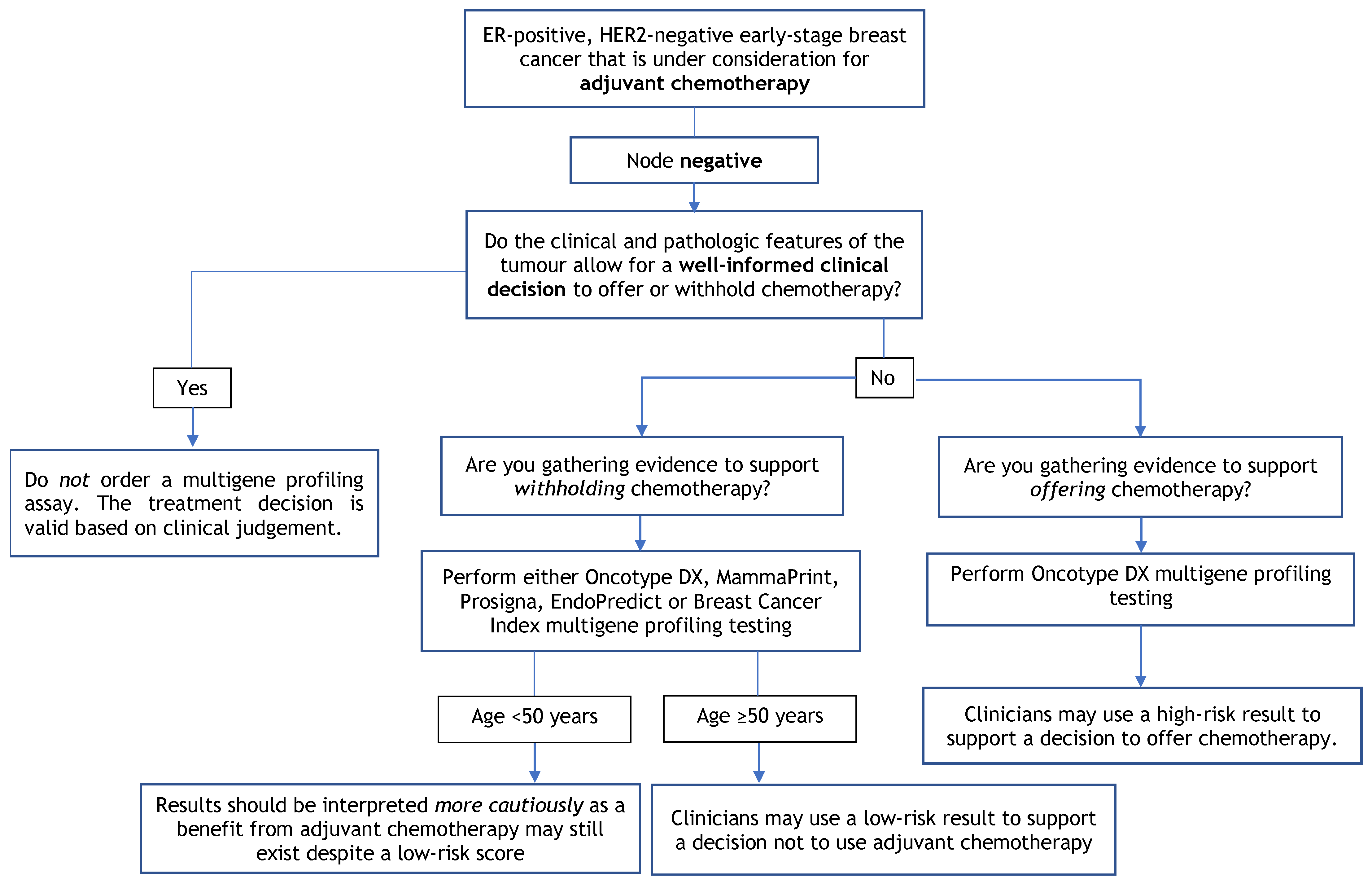
4.1. Recommendation 1
4.1.1. Qualifying Statement for Recommendation 1
- There is currently insufficient evidence to use multigene profiling assays among patients with either HER2-positive or triple-negative breast cancers;
- Multigene profiling assays are recommended for use in patients with lymph node-negative or lymph node-positive (1–3 lymph nodes) disease who are under consideration for adjuvant chemotherapy if the use is supported by other clinical, pathological, or patient-related factors. Clinical and pathological features include patient age, tumour grade, tumour size and nodal status;
- One multigene profiling assay should be requested per patient to guide a specific treatment decision. Requesting multiple tests with different multigene profiling assays on an individual tumour specimen to guide a single treatment decision is discouraged. Additional testing may be considered for patients with either repeat metachronous breast cancer diagnoses or synchronous breast cancer diagnoses where tumour specimens display varying morphologies, grade or hormone receptor status;
- Multigene profiling assays should be interpreted cautiously in pre-menopausal patients where a significant benefit from adjuvant chemotherapy may still exist despite a low-risk score.
4.1.2. Key Evidence for Recommendation 1
4.1.3. Justification for Recommendation 1
4.2. Recommendation 2
4.2.1. Qualifying Statement for Recommendation 2
- Patients < 50 years of age may still benefit from chemotherapy despite low-risk scores from multigene assay testing. Risk scores should be interpreted with caution, and decisions should be made while considering other clinical, pathological, or patient-related factors;
- Treatment decisions should be based on all available clinical and pathological information for each patient rather than depending entirely on multigene profiling test results;
- In patients with a low-grade tumour (i.e., grade 1) less than 1 cm in size, the Working Group members do not recommend a multigene assay profiling as this is unlikely to inform a treatment decision to use adjuvant chemotherapy. The Working Group would also not suggest the use of multigene profiling assays in patients who would not be willing or medically able to undergo chemotherapy.
4.2.2. Key Evidence for Recommendation 2
- In the TAILORx trial [12], patients with a recurrence score (RS) ≤ 10 had an invasive disease-free survival (IDFS) rate of 94.0% and an overall survival (OS) rate of 98.0% with adjuvant endocrine therapy alone at five years and an IDFS rate of 84.0% and OS rate of 93.7% at nine years;
- No difference in freedom from distant recurrence (94.5% vs. 95.0%; p = 0.48), IDFS (83.3% vs. 84.3%; p = 0.26) or OS (93.9% vs. 93.8%; p = 0.89) was reported in patients with an RS of 11 to 25 between those who received endocrine therapy and chemoendocrine therapy at nine-year follow-up in the intent-to-treat population [12];
- In a subgroup analysis from the TAILORx trial among women aged ≤50 years [12], there was a significant benefit in those that received chemoendocrine therapy for IDFS with an RS of 16 to 20 (hazard ratio (HR), 1.90, 95% confidence interval (CI), 1.27 to 2.84; p = 0.0016) or 21 to 25 (HR, 1.70; 95% CI, 1.03 to 2.80; p = 0.035). This corresponded to a 1.6% reduction in the rate of distant recurrence among patients with an RS of 16 to 20 and a 6.5% reduction in the rate of distant recurrence among patients with an RS of 21 to 25 at nine-year follow-up;
- In an initial retrospective analysis of NSABP B20 [14], in patients with low (RS < 18) and intermediate scores (RS 18 to 20), there was no significant difference in 10-year freedom from distant recurrence between those that received chemotherapy and those that did not (95.6% vs. 96.8%; p = 0.61) and (89.1% vs. 90.9%; p = 0.39), respectively. There was a statistically significant interaction between chemotherapy treatment and RS score (p = 0.038). In the analysis by Geyer et al. [15], excluding patients with HER2-positive tumours, there was no benefit of chemotherapy in patients with low and intermediate scores. In a multivariable analysis, the test for interaction between chemotherapy and RS was statistically significant (p = 0.023) when controlling for patient age, tumour size, ER and progesterone receptor (PR) status, and tumour grade. Similarly, when the patients were recategorized by RS using TAILORx cut-offs, a statistically significant benefit was shown with the addition of chemotherapy for patients with an RS > 25, but there was no benefit in patients with RS < 11 and RS 11 to 25.
- In a prespecified exploratory subgroup analysis of the MINDACT trial of node-negative, ER-positive, HER2-negative patients, there was no significant difference in distant metastasis-free survival between patients who received chemotherapy and no chemotherapy in the high clinical risk and low genomic risk group (p = NR) or in the low clinical risk and high genomic risk group (p = NR). However, after a median follow-up of 8.7 years, there was a significant difference between the two treatment groups in the high clinical risk and low genomic risk group (HR, 0.60; 95% CI, 0.38 to 0.96; p = NR), but no significant difference in the low clinical risk and high genomic risk group (p = 0.815);
- In a predefined exploratory analysis of hormone receptor (HR)-positive, HER2-negative women at high clinical risk and low genomic risk, a significant chemotherapy benefit was shown (HR, 0.54; 95% CI, 0.30 to 0.98; p = NR) with an absolute difference of 5.0% in the rate of survival without distant metastases between the treatment groups in women 50 years of age or younger. No significant benefit was shown in women older than 50 years (HR, 0.82; 95% CI 0.55 to 1.24; p = NR). However, it is important to note that premenopausal patients were not mandated to receive ovarian suppression prior to treatment.
- In both exploratory retrospective analyses of patients from the NCIC CTG MA.21 and DBCG 77B trials, the categorical Risk of Relapse (ROR) score was not predictive of response to chemotherapy regimen (p = 0.232) [18] for recurrence-free survival (RFS) or treatment (p = 0.10) for disease-free survival (DFS) [19], respectively;
- In a retrospective analysis of the ATAC trial, Sestak et al. [20] found that the risk of distant recurrence at 5 to 10 years was 1.4% (95% CI, 0.5 to 3.8) for low-risk patients.
- In a retrospective analysis of the ABSCG-8 trial, Filipits et al. [21] found the probability for 15-year distant RFS (DRFS) was 97.6% (95% CI, 94.7 to 98.9) for low-risk patients with a significant difference in late DRFS between patients in the high- vs. low-risk group (HR, 4.74; 95% CI, 1.89 to 11.87; p < 0.001);
- In a study combining both the ATAC trial and ABCSG-8 trial together [22], there was a significant difference in late distant recurrence (i.e., five to 10 years) between patients in the high- vs. low-risk group (HR, 5.49; 95% CI, 2.92 to 10.35; p = NR).
- In a retrospective analysis of the ATAC trial, Sestak et al. [20] found the risk of distant recurrence for EPclin low-risk patients at 5 to 10 years was 4.3% (95% CI, 2.6 to 7.1);
- In an analysis of both the ABCSG-8 and ABCSG-6 trial together [23], there was a significant difference in DRFR from 5 to 15 years in women who were distant recurrence-free at 5 years between those with low and high EPclin scores (HR, 4.52; 95% CI, 2.65 to 7.72; p < 0.001).
- In retrospective analyses of the ATAC trial [25], there was a significant difference between high Breast Cancer Index scores (BCI-high) and BCI-low groups (13.3% vs. 3.5%; HR, 2.97; 95% CI, 1.23 to 7.13; p = NR). In a multivariate analysis for late recurrence, the BCI molecular grade index MGI HOXB13/IL17BR (MGI H/I) was prognostic for risk of distant late recurrence in node-negative (HR, 1.95; 95% CI, 1.22 to 3.14) and node-negative HER2-negative populations (HR, 2.12; 95% CI, 1.30 to 3.47). Sestak et al. [20] found the risk of distant recurrence at 5 to 10 years was 2.6% (95% CI, 1.3 to 5.0) for low-risk patients and 15.9% (95% CI, 8.9 to 27.6) for high-risk patients;
- Zhang et al. [24] found there was a significant difference in late DRFS between the BCI-low, BCI-intermediate, and BCI-high-risk groups for patients in both the Stockholm cohort and the multi-institutional cohort (p = 0.0152 and p = 0.0002, respectively). In a multivariate Cox regression including clinicopathologic variables, BCI was significant for ER-positive, HER2-negative patients in both the Stockholm cohort (HR, 3.50; 95% CI, 1.09 to 11.21; p = 0.035) and the multi-institutional cohort (HR, 9.24; 95% CI, 2.85 to 30.0; p = 0.0002).
4.2.3. Justification for Recommendation 2
4.3. Recommendation 3
4.3.1. Qualifying Statement for Recommendation 3
4.3.2. Key Evidence for Recommendation 3
- In the TAILORx trial [26], the rate of freedom from recurrence of breast cancer at a distant site for high-risk patients (RS 26–100) treated with endocrine therapy plus adjuvant chemotherapy was 93% at five years and 86.8% at nine years;
- In a retrospective analysis of the NSABP B20 trial [14], patients with high RS (RS ≥ 31) experienced a large chemotherapy benefit (60.5% vs. 88.1%; relative risk (RR), 0.26; 95% CI, 0.13 to 0.53) and a statistically significant interaction between chemotherapy treatment and RS score (p = 0.038). In the second re-analysis by Geyer et al. [15], a benefit of chemotherapy remained for patients with high RS (HR 0.18; 95% CI, 0.07 to 0.47; p < 0.001); however, there was no benefit of chemotherapy in patients with RS < 18 and RS 18 to 30. In a multivariable analysis, the test for interaction between chemotherapy and RS was statistically significant (p = 0.023) when controlling for patient age, tumour size, ER and PR status, and tumour grade. Similarly, when the patients were recategorized by RS using TAILORx cut-offs, a statistically significant benefit was shown with the addition of chemotherapy for patients with an RS > 25. In a multivariable analysis, the test for interaction between chemotherapy and RS was statistically significant (p = 0.014) when controlling for patient age, tumour size, ER and PR status, and tumour grade. It is important to note that the patients included in the tamoxifen-only arm were used in the initial development of the Oncotype DX assay, and as a result, these results may be confounded.
4.3.3. Justification for Recommendation 3
4.4. Recommendation 4
4.4.1. Qualifying Statement for Recommendation 4
- Premenopausal patients < 50 years of age have a significant benefit from chemotherapy despite low-risk scores from multigene assay testing. Risk scores should be interpreted with caution, and decisions should be made while considering other clinical, pathological, or patient-related factors;
- It is uncertain whether at least some of the benefit of chemotherapy among premenopausal patients may be due to chemotherapy-induced amenorrhea versus the cytotoxic effects of treatment;
- The Prosigna, EndoPredict/EPclin, and Breast Cancer Index assays are capable of identifying low-risk node-positive patients whose prognostic outcomes are favorable; however, these assays have not demonstrated predictive evidence to support withholding adjuvant chemotherapy among higher risk, node-positive, ER-positive, HER2-negative breast cancer patients.
4.4.2. Key Evidence for Recommendation 4
- The RxPONDER trial [27] reported there was no significant difference in IDFS at five years between patients (RS ≤ 25) who received chemoendocrine therapy or endocrine therapy (92.2% vs. 91.0%; HR, 0.86; 95% CI, 0.72 to 1.03; p = 0.10). The interaction between chemotherapy benefit and continuous recurrence score was not statistically significant for IDFS when controlling for continuous RS, menopausal status, and treatment group (p = 0.35);
- ○
- In a prespecified analysis, a significant interaction was found between the addition of adjuvant chemotherapy and menopausal status (p = 0.008), allowing for subgroup analysis by menopausal status. In postmenopausal women, there was no significant difference in IDFS between those who received chemoendocrine therapy or endocrine therapy (91.3% vs. 91.9%; HR, 1.02; 95% CI, 0.82 to 1.26; p = 0.89);
- ○
- In premenopausal women, a significant benefit was found in IDFS for women who received chemoendocrine therapy (93.9% vs. 89.0%; HR, 0.60; 95% CI, 0.43 to 0.83; p = 0.002). In premenopausal women who were 50 years old or older, there was no significant chemotherapy benefit (HR, 0.98; 95% CI, 0.54 to 1.78); however, in premenopausal women younger than 50 years old, a significant chemotherapy benefit was observed (HR, 0.48; 95% CI, 0.32 to 0.72; p = NR). The interaction between age and chemotherapy benefit in premenopausal women was not significant (p = 0.06);
- In a retrospective analysis of the SWOG-8814 trial [28], there was no significant benefit for DFS or OS between patients who received either tamoxifen alone or cyclophosphamide, doxorubicin, and 5-fluorouracil (CAF) followed by tamoxifen at 10 years for those with RS < 18 (p = 0.97 and p = 0.68, respectively) or RS between 18 and 30 (p = 0.48 and p = 065, respectively). For DFS, there was no significant interaction between RS and treatment (p = 0.053); however, when assessing the first five years, a significant interaction was seen between RS and treatment for both DFS and OS (p = 0.029 and p = 0.016, respectively) but not after five years (p = 0.58 and p = 0.87, respectively).
4.4.3. Justification for Recommendation 4
4.5. Recommendation 5
4.5.1. Qualifying Statement for Recommendation 5
- While a number of studies have demonstrated the clinical utility of BCI for extending adjuvant endocrine therapy, the preliminary results of the NSABP B42 trial are negative, leading to some uncertainty. Treatment decisions should be based on all available clinical and pathological information for each patient rather than depending only on multigene profiling tests;
- MammaPrint, Oncotype DX, Prosigna, and EndoPredict currently have insufficient evidence to guide the extension of adjuvant endocrine therapy; however, these molecular assays may prognosticate a very low rate of disease recurrence that might not justify an extension of endocrine therapy.
4.5.2. Key Evidence for Recommendation 5
- In a retrospective review of the NSABP B42 trial [32], currently in abstract form, there was no significant difference between receiving an additional five years of letrozole or placebo for recurrence-free interval in those who were BCI (H/I)-low (HR, 0.69; 95% CI, 0.43 to 1.11; p = 0.13) or BCI (H/I)-high (HR, 0.83; 95% CI, 0.55 to 1.26; p = 0.38). There was no significant interaction between BCI (H/I) level and treatment (p = 0.55) for recurrence-free interval, breast cancer-free interval (p = 0.07), DFS (p = 0.62), or distant recurrence (p = 0.14);
- In the translation IDEAL study [31], there was significant benefit in risk of recurrence for BCI (H/I)-high patients who received five years of extended letrozole (HR, 0.42; 95% CI, 0.21 to 0.84; p = 0.011) with an absolute reduction of recurrence risk of 9.8%; however, this benefit was not observed in BCI (H/I)-low patients (HR, 0.95; 95% CI, 0.58 to 1.56; p = 0.835). Similarly, in patients treated with primary adjuvant endocrine therapy with an AI, BCI (H/I)-high patients received a significant benefit from extended letrozole (HR, 0.34; 95% CI, 0.16 to 0.73; p = 0.004), while no benefit was seen in BCI (H/I)-low patients (HR, 0.90; 95% CI, 0.53 to 1.55; p = 0.712). There was a significant interaction between BCI (H/I) level and treatment in both the overall population (p = 0.045) and in the subgroup of patients who received primary adjuvant endocrine therapy with an AI (p = 0.025) after adjusting for age, tumour grade, pT stage, pN stage, prior endocrine therapy and prior chemotherapy;
- In the Trans-aTTom study [30], consisting of node-positive patients only, those classified as BCI (H/I)-high showed a significant benefit from extended tamoxifen (HR, 0.35; 95% CI, 0.15 to 0.86; p = 0.027) with an absolute recurrence risk difference of 10.2%. There was a significant interaction between continuous BCI (H/I) and extended tamoxifen treatment (p = 0.012) after adjusting for age, tumour size, tumour grade, and ER and PR status;
- In the retrospective review of the NCIC CTG MA 17 trial [29], for patients with high H/I, there was a significant difference in the five-year RFS of 73% (95% CI, 56.6 to 84.1) and 89.5% (95% CI, 80.3 to 94.5) for patients receiving placebo and letrozole, respectively, with an absolute risk of reduction of 16.5% (p = 0.007). In an adjusted model, high H/I was significantly associated with patient benefit from letrozole (odds ratio (OR), 0.32; 95% CI, 0.14 to 0.72; p = 0.006). The interaction between H/I and letrozole therapy was significant (p = 0.03).
4.5.3. Justification for Recommendation 5
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019; Canadian Cancer Society: Toronto, ON, Canada, 2019. [Google Scholar]
- Lagace, F.; Ghazawi, F.M.; Le, M.; Rahme, E.; Savin, E.; Zubarev, A.; Alakel, A.; Sasseville, D.; Moreau, L.; Meterissian, S.; et al. Analysis of incidence, mortality trends, and geographic distribution of breast cancer patients in Canada. Breast Cancer Res. Treat. 2019, 178, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Curigliano, G.; Loibl, S.; Dubsky, P.; Gnant, M.; Poortmans, P.; Colleoni, M.; Denkert, C.; Piccart-Gebhart, M.; Regan, M.; et al. Estimating the benefits of therapy for early-stage breast cancer: The St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann. Oncol. 2019, 30, 1541–1557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 365, 1687–1717. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group. Comparisons between different polychemotherapy regimens for early breast cancer: Meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 2012, 379, 432–444. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.J.; Jagsi, R.; Morrow, M. Reducing Overtreatment of Cancer With Precision Medicine: Just What the Doctor Ordered. JAMA 2018, 319, 1091–1092. [Google Scholar] [CrossRef] [PubMed]
- Kittaneh, M.; Badve, S.; Caldera, H.; Coleman, R.; Goetz, M.P.; Mahtani, R.; Mamounas, E.; Kalinsky, K.; Lower, E.; Pegram, M.; et al. Case-Based Review and Clinical Guidance on the Use of Genomic Assays for Early-Stage Breast Cancer: Breast Cancer Therapy Expert Group (BCTEG). Clin. Breast Cancer 2020, 20, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Cuzick, J.; Dowsett, M.; Pineda, S.; Wale, C.; Salter, J.; Quinn, E.; Zabaglo, L.; Mallon, E.; Green, A.R.; Ellis, I.O.; et al. Prognostic value of a combined estrogen receptor, progesterone receptor, Ki-67, and human epidermal growth factor receptor 2 immunohistochemical score and comparison with the genomic health recurrence score in early breast cancer. J. Clin. Oncol. 2011, 29, 4273–4278. [Google Scholar] [CrossRef] [Green Version]
- Browman, G.P.; Newman, T.E.; Mohide, E.A.; Graham, I.D.; Levine, M.N.; Pritchard, K.I.; Evans, W.K.; Maroun, J.A.; Hodson, D.I.; Carey, M.S.; et al. Progress of clinical oncology guidelines development using the Practice Guidelines Development Cycle: The role of practitioner feedback. J. Clin. Oncol. 1998, 16, 1226–1231. [Google Scholar] [CrossRef]
- Browman, G.P.; Levine, M.N.; Mohide, E.A.; Hayward, R.S.; Pritchard, K.I.; Gafni, A.; Laupacis, A. The practice guidelines development cycle: A conceptual tool for practice guidelines development and implementation. J. Clin. Oncol. 1995, 13, 502–512. [Google Scholar] [CrossRef]
- Blanchette, P.; Sivajohanathan, D.; Bartlett, J.; Eisen, A.; Feilotter, H.; Pezo, R.; the Clinical Utility of Multigene Profiling Assays in Early-Stage Invasive Breast Cancer Expert Panel. Clinical Utility of Multigene Profiling Assays in Early-Stage Invasive Breast Cancer; Ontario Health (Cancer Care Ontario): Toronto, ON, Canada, 2022; Program in Evidence-Based Care Guideline No.: MOTAC-4 Version 2. [Google Scholar]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; Olson, J.A., Jr.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Sparano, J.A.; Gray, R.J.; Ravdin, P.M.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; et al. Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer. N. Engl. J. Med. 2019, 380, 2395–2405. [Google Scholar] [CrossRef] [PubMed]
- Paik, S.; Tang, G.; Shak, S.; Kim, C.; Baker, J.; Kim, W.; Cronin, M.; Baehner, F.L.; Watson, D.; Bryant, J.; et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J. Clin. Oncol. 2006, 24, 3726–3734. [Google Scholar] [CrossRef] [PubMed]
- Geyer, C.E., Jr.; Tang, G.; Mamounas, E.P.; Rastogi, P.; Paik, S.; Shak, S.; Baehner, F.L.; Crager, M.; Wickerham, D.L.; Costantino, J.P.; et al. 21-Gene assay as predictor of chemotherapy benefit in HER2-negative breast cancer. NPJ Breast Cancer 2018, 4, 37. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; van’t Veer, L.J.; Bogaerts, J.; Slaets, L.; Viale, G.; Delaloge, S.; Pierga, J.Y.; Brain, E.; Causeret, S.; DeLorenzi, M.; et al. 70-Gene Signature as an Aid to Treatment Decisions in Early-Stage Breast Cancer. N. Engl. J. Med. 2016, 375, 717–729. [Google Scholar] [CrossRef] [Green Version]
- Piccart, M.; van’t Veer, L.J.; Poncet, C.; Lopes Cardozo, J.M.N.; Delaloge, S.; Pierga, J.Y.; Vuylsteke, P.; Brain, E.; Vrijaldenhoven, S.; Neijenhuis, P.A.; et al. 70-gene signature as an aid for treatment decisions in early breast cancer: Updated results of the phase 3 randomised MINDACT trial with an exploratory analysis by age. Lancet Oncol. 2021, 22, 476–488. [Google Scholar] [CrossRef]
- Liu, S.; Chapman, J.A.; Burnell, M.J.; Levine, M.N.; Pritchard, K.I.; Whelan, T.J.; Rugo, H.S.; Albain, K.S.; Perez, E.A.; Virk, S.; et al. Prognostic and predictive investigation of PAM50 intrinsic subtypes in the NCIC CTG MA.21 phase III chemotherapy trial. Breast Cancer Res. Treat. 2015, 149, 439–448. [Google Scholar] [CrossRef]
- Jensen, M.B.; Laenkholm, A.V.; Nielsen, T.O.; Eriksen, J.O.; Wehn, P.; Hood, T.; Ram, N.; Buckingham, W.; Ferree, S.; Ejlertsen, B. The Prosigna gene expression assay and responsiveness to adjuvant cyclophosphamide-based chemotherapy in premenopausal high-risk patients with breast cancer. Breast Cancer Res. 2018, 20, 79. [Google Scholar] [CrossRef] [Green Version]
- Sestak, I.; Buus, R.; Cuzick, J.; Dubsky, P.; Kronenwett, R.; Denkert, C.; Ferree, S.; Sgroi, D.; Schnabel, C.; Baehner, F.L.; et al. Comparison of the Performance of 6 Prognostic Signatures for Estrogen Receptor-Positive Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2018, 4, 545–553. [Google Scholar] [CrossRef]
- Filipits, M.; Nielsen, T.O.; Rudas, M.; Greil, R.; Stoger, H.; Jakesz, R.; Bago-Horvath, Z.; Dietze, O.; Regitnig, P.; Gruber-Rossipal, C.; et al. The PAM50 risk-of-recurrence score predicts risk for late distant recurrence after endocrine therapy in postmenopausal women with endocrine-responsive early breast cancer. Clin. Cancer Res. 2014, 20, 1298–1305. [Google Scholar] [CrossRef] [Green Version]
- Sestak, I.; Cuzick, J.; Dowsett, M.; Lopez-Knowles, E.; Filipits, M.; Dubsky, P.; Cowens, J.W.; Ferree, S.; Schaper, C.; Fesl, C.; et al. Prediction of late distant recurrence after 5 years of endocrine treatment: A combined analysis of patients from the Austrian breast and colorectal cancer study group 8 and arimidex, tamoxifen alone or in combination randomized trials using the PAM50 risk of recurrence score. J. Clin. Oncol. 2015, 33, 916–922. [Google Scholar] [CrossRef]
- Filipits, M.; Dubsky, P.; Rudas, M.; Greil, R.; Balic, M.; Bago-Horvath, Z.; Singer, C.F.; Hlauschek, D.; Brown, K.; Bernhisel, R.; et al. Prediction of Distant Recurrence Using EndoPredict Among Women with ER+, HER2− Node-Positive and Node-Negative Breast Cancer Treated with Endocrine Therapy Only. Clin. Cancer Res. 2019, 25, 3865–3872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Schnabel, C.A.; Schroeder, B.E.; Jerevall, P.L.; Jankowitz, R.C.; Fornander, T.; Stal, O.; Brufsky, A.M.; Sgroi, D.; Erlander, M.G. Breast cancer index identifies early-stage estrogen receptor-positive breast cancer patients at risk for early- and late-distant recurrence. Clin. Cancer Res. 2013, 19, 4196–4205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sgroi, D.C.; Sestak, I.; Cuzick, J.; Zhang, Y.; Schnabel, C.A.; Schroeder, B.; Erlander, M.G.; Dunbier, A.; Sidhu, K.; Lopez-Knowles, E.; et al. Prediction of late distant recurrence in patients with oestrogen-receptor-positive breast cancer: A prospective comparison of the breast-cancer index (BCI) assay, 21-gene recurrence score, and IHC4 in the TransATAC study population. Lancet Oncol. 2013, 14, 1067–1076. [Google Scholar] [CrossRef] [Green Version]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Albain, K.S.; Saphner, T.J.; Badve, S.S.; Wagner, L.I.; Kaklamani, V.G.; Keane, M.M.; Gomez, H.L.; et al. Clinical Outcomes in Early Breast Cancer With a High 21-Gene Recurrence Score of 26 to 100 Assigned to Adjuvant Chemotherapy Plus Endocrine Therapy: A Secondary Analysis of the TAILORx Randomized Clinical Trial. JAMA Oncol. 2020, 6, 367–374. [Google Scholar] [CrossRef] [Green Version]
- Kalinsky, K.; Barlow, W.E.; Gralow, J.R.; Meric-Bernstam, F.; Albain, K.S.; Hayes, D.F.; Lin, N.U.; Perez, E.A.; Goldstein, L.J.; Chia, S.K.L.; et al. 21-Gene Assay to Inform Chemotherapy Benefit in Node-Positive Breast Cancer. N. Engl. J. Med. 2021, 385, 2336–2347. [Google Scholar] [CrossRef]
- Albain, K.S.; Barlow, W.E.; Shak, S.; Hortobagyi, G.N.; Livingston, R.B.; Yeh, I.T.; Ravdin, P.; Bugarini, R.; Baehner, F.L.; Davidson, N.E.; et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: A retrospective analysis of a randomised trial. Lancet Oncol. 2010, 11, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Sgroi, D.C.; Carney, E.; Zarrella, E.; Steffel, L.; Binns, S.N.; Finkelstein, D.M.; Szymonifka, J.; Bhan, A.K.; Shepherd, L.E.; Zhang, Y.; et al. Prediction of late disease recurrence and extended adjuvant letrozole benefit by the HOXB13/IL17BR biomarker. J. Natl. Cancer Inst. 2013, 105, 1036–1042. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, J.M.S.; Sgroi, D.C.; Treuner, K.; Zhang, Y.; Ahmed, I.; Piper, T.; Salunga, R.; Brachtel, E.F.; Pirrie, S.J.; Schnabel, C.A.; et al. Breast Cancer Index and prediction of benefit from extended endocrine therapy in breast cancer patients treated in the Adjuvant Tamoxifen-To Offer More? (aTTom) trial. Ann. Oncol. 2019, 30, 1776–1783. [Google Scholar] [CrossRef] [Green Version]
- Noordhoek, I.; Treuner, K.; Putter, H.; Zhang, Y.; Wong, J.; Kranenbarg, E.M.K.; Carpentier, M.D.D.; van de Velde, C.J.H.; Schnabel, C.A.; Liefers, G.J. Breast cancer index predicts extended endocrine benefit to individualize selection of patients with HR+ early-stage breast cancer for 10 years of endocrine therapy. Clin. Cancer Res. 2021, 27, 311–319. [Google Scholar] [CrossRef]
- Mamounas, E.P.; Bandos, H.; Rastogi, P.; Zhang, Y.; Treuner, K.; Lucas, P.C.; Geyer, C.E.; Fehrenbacher, L.; Graham, M.; Chia, S.K.L.; et al. Breast Cancer Index (BCI) and prediction of benefit from extended aromatase inhibitor (AI) therapy (tx) in HR+ breast cancer: NRG oncology/NSABP B-42. J. Clin. Oncol. 2021, 39, 501. [Google Scholar] [CrossRef]
- Rastogi, P.; Bandos, H.; Lucas, P.C.; van’t Veer, L.; Wei, J.J.; Geyer, C.E.; Fehrenbacher, L.; Graham, M.; Chia, S.K.L.; Brufsky, A.; et al. Utility of the 70-gene MammaPrint assay for prediction of benefit from extended letrozole therapy (ELT) in the NRG Oncology/NSABP B-42 trial. J. Clin. Oncol. 2021, 39 (Suppl. S15), 502. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Question | Reviewer Ratings (n = 1) | ||||
|---|---|---|---|---|---|
| Lowest Quality | Highest Quality | ||||
| (1) | (2) | (3) | (4) | (5) | |
| Rate the guideline development methods. | 0 | 0 | 0 | 0 | 1 |
| Rate the guideline presentation. | 0 | 0 | 0 | 0 | 1 |
| Rate the guideline recommendations. | 0 | 0 | 0 | 1 | 0 |
| Rate the completeness of reporting. | 0 | 0 | 0 | 0 | 1 |
| Does this document provide sufficient information to inform your decisions? If not, what areas are missing? | 0 | 0 | 0 | 0 | 1 |
| Rate the overall quality of the guideline report. | 0 | 0 | 0 | 0 | 1 |
| Strongly disagree | Neutral | Strongly agree | |||
| (1) | (2) | (3) | (4) | (5) | |
| I would make use of this guideline in my professional decisions. | 0 | 0 | 0 | 0 | 1 |
| I would recommend this guideline for use in practice. | 0 | 0 | 0 | 0 | 1 |
What are the barriers or enablers to the implementation of this guideline report?
| |||||
| General Questions | Overall Guideline Assessment (n = 25) | ||||
|---|---|---|---|---|---|
| Lowest Quality | Highest Quality | ||||
| (1) | (2) | (3) | (4) | (5) | |
| Rate the overall quality of the guideline report. | 0 | 0 | 1 | 14 | 10 |
| Strongly disagree | Strongly agree | ||||
| (1) | (2) | (3) | (4) | (5) | |
| I would make use of this guideline in my professional decisions. | 0 | 0 | 4 | 9 | 12 |
| I would recommend this guideline for use in practice. | 0 | 0 | 2 | 9 | 14 |
What are the barriers or enablers to the implementation of this guideline report?
| |||||
| Characteristics/Assay Name | Oncotype DX | Prosigna | MammaPrint | EndoPredict | Breast Cancer Index |
|---|---|---|---|---|---|
| Tissue Required | FFPE | FFPE | FFPE or fresh tissue | FFPE | FFPE |
| Technique | qRT-PCR | qRT-PCR and nCounter DX Analysis System | Microarray | qRT-PCR | qRT-PCR |
| Assay Output | RS (0–100) | Intrinsic subtype and ROR score (0–100) | MammaPrint Index Risk of distant recurrence at 5 years | EPclin score (1–6) Molecular score (1–15) | BCI score (0–10) and BCI (H/I) low and BCI (H/I) high (ratio HoxB13 and interleukin-17B receptor) |
| Categories for Risk Measurement | TAILORx categories Low: ≤15 Intermediate: 16–25 High: 26–100 Pre-TAILORx categories Low: <18 Intermediate: 18–30 High: ≥31 | LN-negative Low: 0–40 Intermediate: 41–60 High: 61–100 LN-positive (1–3 nodes) Low: 0–40 High: 41–100 | Low: 0 to 1 High: −1 to 0 | EPclin score Low: < 3.3 High: ≥ 3.3 Molecular score Low: < 5 High: ≥ 5 | BCI predictive H/I Low: <0.06 High: ≥0.06 BCI prognostic node-negative Low: <5.0825 Intermediate: 5.0825–6.5025 High: ≥6.5025 BCI prognostic node-positive Low: <6.93 High: ≥6.93 |
| Regulatory Approval or Endorsement | Assay conducted in centralized Exact Science’s CLIA-certified lab | FDA cleared for decentralized testing (2014) | FDA cleared for Agendia centralized lab testing in FFPE (2015) | CE Mark for decentralized testing (2012) | Assay conducted in centralized CAP/CLIA-certified lab |
| Manufacturer | Exact Sciences Corp. | Veracyte | Agendia | Myriad Genetics, Inc. | Biotheranostics, Inc. |
| Testing Location | Central (1 laboratory in US) | Various labs across US, UK | Central (1 laboratory in the Netherlands, 1 in US) | Central laboratory in the US | Central (1 laboratory in US) |
| Genes, n | 21-gene assay | 50-gene assay | 70-gene assay | 12-gene assay EPclin score: 12-gene assay plus tumour size and nodal status | HOXB13:IL17BR expression ratio (H/I) and Molecular Grade Index |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanchette, P.; Sivajohanathan, D.; Bartlett, J.; Eisen, A.; Feilotter, H.; Pezo, R.; Turashvili, G.; Williams, P. Clinical Utility of Multigene Profiling Assays in Early-Stage Invasive Breast Cancer: An Ontario Health (Cancer Care Ontario) Clinical Practice Guideline. Curr. Oncol. 2022, 29, 2599-2615. https://doi.org/10.3390/curroncol29040213
Blanchette P, Sivajohanathan D, Bartlett J, Eisen A, Feilotter H, Pezo R, Turashvili G, Williams P. Clinical Utility of Multigene Profiling Assays in Early-Stage Invasive Breast Cancer: An Ontario Health (Cancer Care Ontario) Clinical Practice Guideline. Current Oncology. 2022; 29(4):2599-2615. https://doi.org/10.3390/curroncol29040213
Chicago/Turabian StyleBlanchette, Phillip, Duvaraga Sivajohanathan, John Bartlett, Andrea Eisen, Harriet Feilotter, Rossanna Pezo, Gulisa Turashvili, and Phillip Williams. 2022. "Clinical Utility of Multigene Profiling Assays in Early-Stage Invasive Breast Cancer: An Ontario Health (Cancer Care Ontario) Clinical Practice Guideline" Current Oncology 29, no. 4: 2599-2615. https://doi.org/10.3390/curroncol29040213
APA StyleBlanchette, P., Sivajohanathan, D., Bartlett, J., Eisen, A., Feilotter, H., Pezo, R., Turashvili, G., & Williams, P. (2022). Clinical Utility of Multigene Profiling Assays in Early-Stage Invasive Breast Cancer: An Ontario Health (Cancer Care Ontario) Clinical Practice Guideline. Current Oncology, 29(4), 2599-2615. https://doi.org/10.3390/curroncol29040213