Predicting Chemotherapy-Related Adverse Events in Elderly Cancer Patients with Prior Anticancer Therapy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Chemotherapy-Related Adverse Events
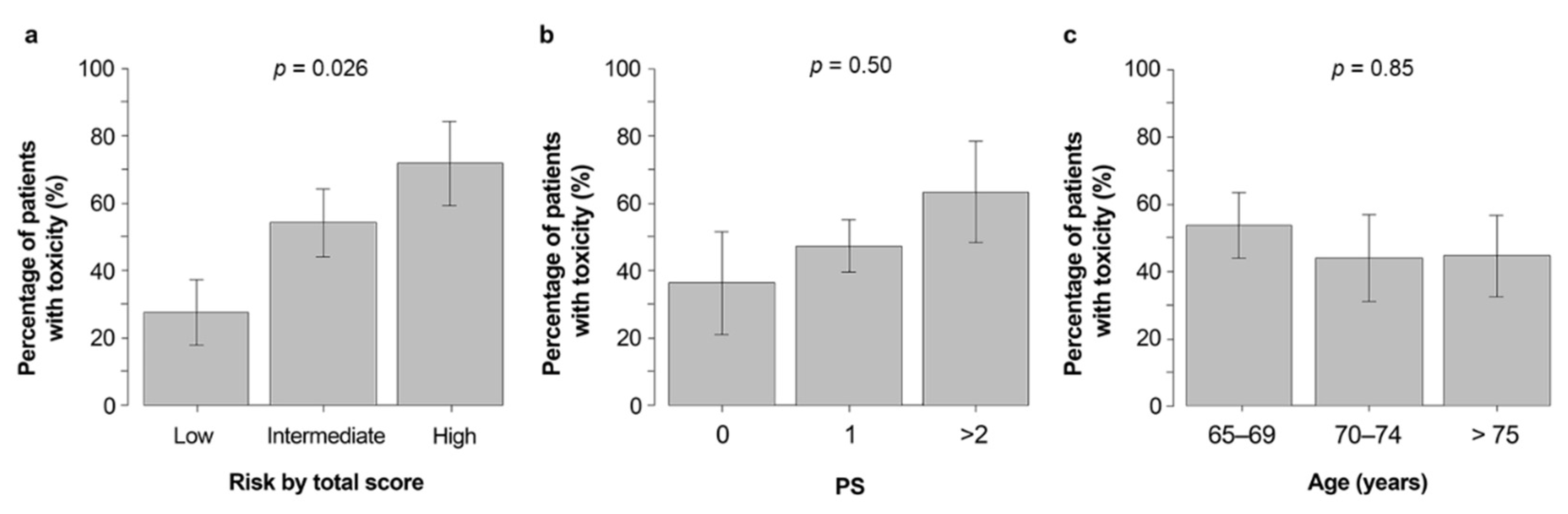
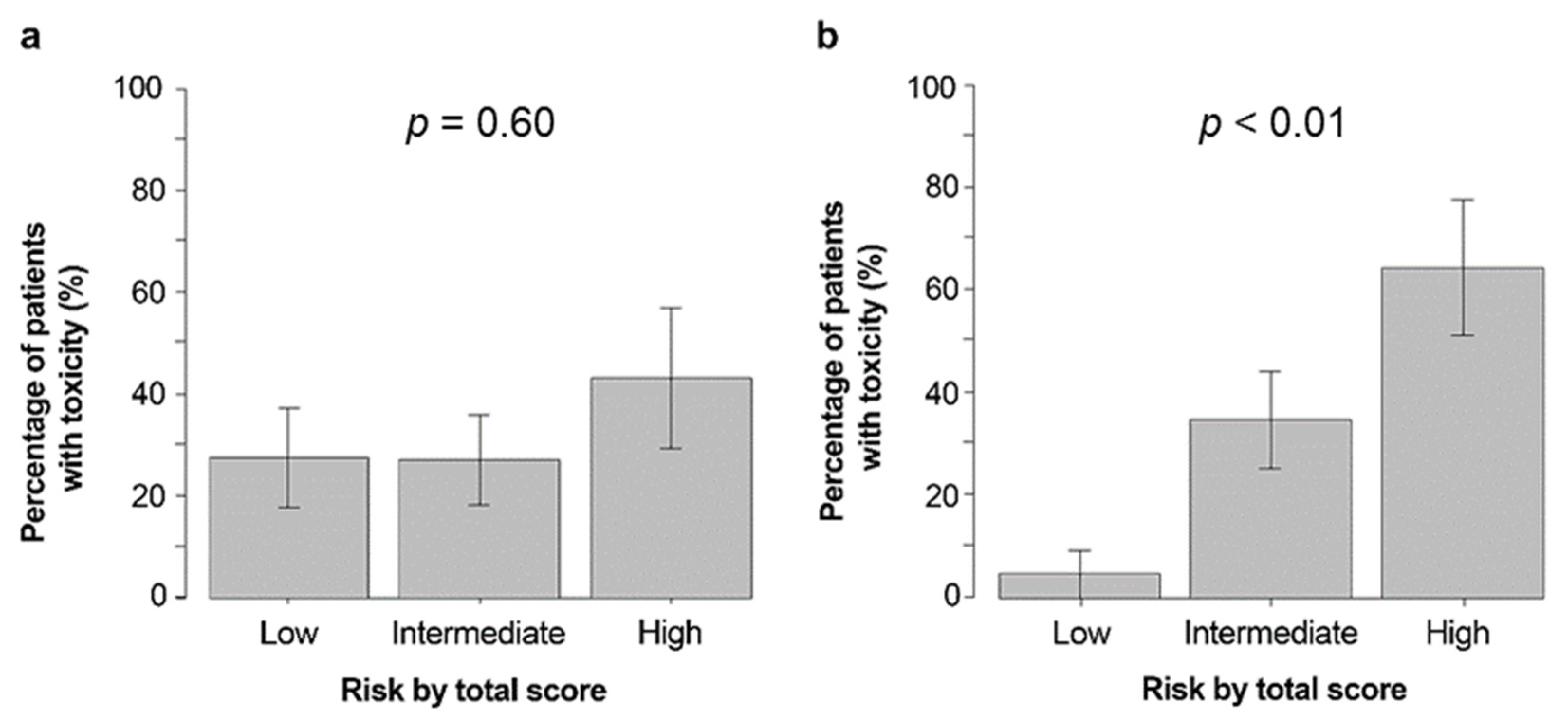
3.3. Comparison of CARG, ECOG PS, and Age for Predicting the Occurrence of Grade 3–5 CRAEs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Hori, M.; Matsuda, T.; Shibata, A.; Katanoda, K.; Sobue, T.; Nishimoto, H. Cancer incidence and incidence rates in Japan in 2009: A study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn. J. Clin. Oncol. 2015, 45, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Hurria, A.; Hurria, A.; Brogan, K.; Panageas, K.S.; Pearce, C.; Norton, L.; Jakubowski, A.; Howard, J.; Hudis, C. Effect of creatinine clearance on patterns of toxicity in older patients receiving adjuvant chemotherapy for breast cancer. Drugs Aging 2005, 22, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Repetto, L. Greater risks of chemotherapy toxicity in elderly patients with cancer. J. Support. Oncol. 2003, 1, 18–24. [Google Scholar] [PubMed]
- Rizzo, A.; Brandi, G. Pitfalls, challenges, and updates in adjuvant systemic treatment for resected biliary tract cancer. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 547–554. [Google Scholar] [CrossRef]
- Rizzo, A.; Ricci, A.D.; Tober, N.; Nigro, M.C.; Mosca, M.; Palloni, A.; Abbati, F.; Frega, G.; De Lorenzo, S.; Tavolari, S.; et al. Second-line Treatment in Advanced Biliary Tract Cancer: Today and Tomorrow. Anticancer Res. 2020, 40, 3013–3030. [Google Scholar] [CrossRef] [PubMed]
- Albain, K.S.; Crowley, J.J.; LeBlanc, M.; Livingston, R.B. Survival determinants in extensive-stage non-small-cell lung cancer: The Southwest Oncology Group experience. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1991, 9, 1618–1626. [Google Scholar] [CrossRef] [PubMed]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting chemotherapy toxicity in older adults with cancer: A prospective multicenter study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurria, A.; Mohile, S.; Gajra, A.; Klepin, H.; Muss, H.; Chapman, A.; Feng, T.; Smith, D.; Sun, C.L.; De Glas, N.; et al. Validation of a Prediction Tool for Chemotherapy Toxicity in Older Adults with Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 2366–2371. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN stimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Nie, X.; Liu, D.; Li, Q.; Bai, C. Predicting chemotherapy toxicity in older adults with lung cancer. J. Geriatr. Oncol. 2013, 4, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Nishijima, T.F.; Deal, A.M.; Williams, G.R.; Sanoff, H.K.; Nyrop, K.A.; Muss, H.B. Chemotherapy Toxicity Risk Score for Treatment Decisions in Older Adults with Advanced Solid Tumors. Oncologist 2018, 23, 573–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohile, S.G.; Mohamed, M.R.; Xu, H.; Culakova, E.; Loh, K.P.; Magnuson, A.; Flannery, M.A.; Obrecht, S.; Gilmore, N.; Ramsdale, E.; et al. Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): A cluster-randomised study. Lancet 2021, 398, 1894–1904. [Google Scholar] [CrossRef]
- Extermann, M.; Boler, I.; Reich, R.R.; Lyman, G.H.; Brown, R.H.; DeFelice, J.; Levine, R.M.; Lubiner, E.T.; Reyes, P.; Schreiber, F.J., 3rd; et al. Predicting the risk of chemotherapy toxicity in older patients: The Chemotherapy Risk Assessment Scale for High-Age Patients (CRASH) score. Cancer 2012, 118, 3377–3386. [Google Scholar] [CrossRef] [PubMed]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhenn, P.S.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef] [PubMed]
- Ando, M.; Ando, Y.; Hasegawa, Y.; Shimokata, K.; Minami, H.; Wakai, K.; Ohno, Y.; Sakai, S. Prognostic value of performance status assessed by patients themselves, nurses, and oncologists in advanced non-small cell lung cancer. Br. J. Cancer 2001, 85, 1634–1639. [Google Scholar] [CrossRef] [PubMed]
- Corre, R.; Greillier, L.; Le Caër, H.; Audigier-Valette, C.; Baize, N.; Bérard, H.; Falchero, L.; Monnet, I.; Dansin, E.; Vergnenègre, A.; et al. Use of a Comprehensive Geriatric Assessment for the Management of Elderly Patients with Advanced Non-Small-Cell Lung Cancer: The Phase III Randomized ESOGIA-GFPC-GECP 08-02 Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 1476–1483. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Value/Response | Score |
|---|---|---|
| Age | ≥72 years <72 years | 2 0 |
| Cancer type | GI or GU cancer Other cancer types | 2 0 |
| Planned chemotherapy dose | Standard dose Dose reduced upfront | 2 0 |
| Planned number of chemotherapy drugs | Polychemotherapy Monochemotherapy | 2 0 |
| Hemoglobin level | <11 g/dL (male) <10 g/dL (female) ≥11 g/dL (male) ≥10 g/dL (female) | 3 0 |
| Creatinine clearance | <34 mL/min ≥34 mL/min | 3 0 |
| How is your hearing (with a hearing aid if needed)? | Fair, poor, or totally deaf Excellent or good | 2 0 |
| Number of falls in the past 6 months | ≥1 None | 3 0 |
| Can you take your own medicine? | Able with some help/unable Able without help | 1 0 |
| Does your health limit your ability to walk 100 m? | Somewhat limited/limited a lot Not limited at all | 2 0 |
| During the past 4 weeks, how much of the time have your physical health or emotional problems interfered with social activities (like visiting with friends, relatives, etc.)? | Limited some of the time, most of the time, or all of the time Limited none of the time or a little of the time | 1 0 |
| Patient Characteristic | Number | % |
|---|---|---|
| Age (years) 65–69 70–74 75–79 ≥80 | 28 16 14 4 | 45 26 23 6 |
| Sex Male Female | 33 29 | 53 47 |
| ECOG PS 0 1 ≥2 | 11 40 11 | 18 64 18 |
| Cancer type Breast Lung GI GYN GU Other | 9 4 36 2 0 11 | 15 6 58 3 0 18 |
| Treatment Standard dose Yes No Number of chemotherapy drugs Monochemotherapy Polychemotherapy Line of chemotherapy Second ≥Third Growth factor use Yes No | 43 19 44 18 39 23 7 55 | 69 31 71 29 63 37 11 89 |
| Hemoglobin <10 g/dL (female) ≥10 g/dL (female) <11 g/dL (male) ≥11 g/dL (male) | 16 13 17 16 | 26 21 27 26 |
| Creatinine clearance <34 mL/min ≥34 mL/min | 4 58 | 6 94 |
| Hearing Fair, poor, or totally deaf Excellent or good | 3 59 | 5 95 |
| No. of falls in the past 6 months ≥1 None | 2 60 | 3 97 |
| Taking medications With some help/unable Without help | 5 57 | 8 92 |
| Limited in walking 100 m Somewhat limited/limited a lot Not limited | 18 44 | 29 71 |
| Decrease in social activity due to health/emotional problems Some, most, all of the time A little, or none of the time | 21 41 | 34 66 |
| CARG 0–5 (low) 6–9 (intermediate) ≥10 (high) | 22 26 14 | 35 42 23 |
| Adverse Event | Grade 3–5 CRAE No. % | Grade 3 CRAE No. % | Grade 4 CRAE No. % |
|---|---|---|---|
| Hematologic Leukopenia Neutropenia Anemia Thrombocytopenia Febrile neutropenia | 9 15 13 21 5 8 4 6 1 2 | 8 13 8 13 5 8 3 5 1 2 | 1 2 5 8 0 0 1 2 0 0 |
| Nonhematologic Fatigue Nausea Mucositis oral Diarrhea Hypertension Proteinuria Edema Hyponatremia Hyperkalemia Hypomagnesemia | 8 13 11 18 4 6 1 2 1 2 1 2 1 2 1 2 2 3 1 2 | 8 13 11 18 4 6 1 2 1 2 1 2 1 2 0 0 2 3 0 0 | 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 2 0 0 1 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suto, H.; Inui, Y.; Okamura, A. Predicting Chemotherapy-Related Adverse Events in Elderly Cancer Patients with Prior Anticancer Therapy. Curr. Oncol. 2022, 29, 2185-2192. https://doi.org/10.3390/curroncol29040177
Suto H, Inui Y, Okamura A. Predicting Chemotherapy-Related Adverse Events in Elderly Cancer Patients with Prior Anticancer Therapy. Current Oncology. 2022; 29(4):2185-2192. https://doi.org/10.3390/curroncol29040177
Chicago/Turabian StyleSuto, Hirotaka, Yumiko Inui, and Atsuo Okamura. 2022. "Predicting Chemotherapy-Related Adverse Events in Elderly Cancer Patients with Prior Anticancer Therapy" Current Oncology 29, no. 4: 2185-2192. https://doi.org/10.3390/curroncol29040177
APA StyleSuto, H., Inui, Y., & Okamura, A. (2022). Predicting Chemotherapy-Related Adverse Events in Elderly Cancer Patients with Prior Anticancer Therapy. Current Oncology, 29(4), 2185-2192. https://doi.org/10.3390/curroncol29040177