The Impact of Real-World Alternative Dosing Strategies of Palbociclib on Progression-Free Survival in Patients with Metastatic Breast Cancer

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Location, and Ethics
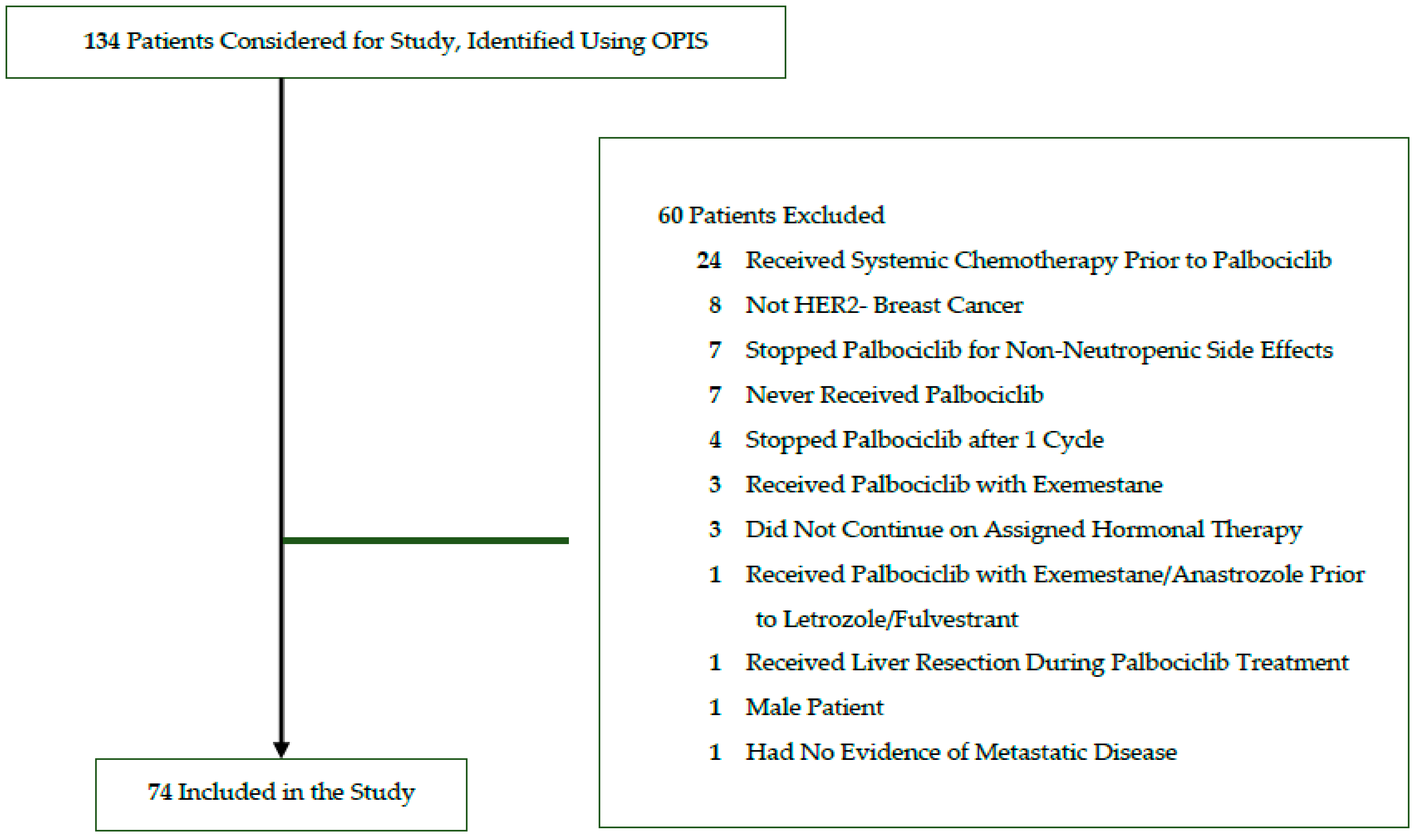
2.2. Study Population
2.3. Study Definitions
2.4. Data Collection and Statistical Analysis
3. Results
3.1. Patient Demographics
3.2. Overall Real-World Outcomes
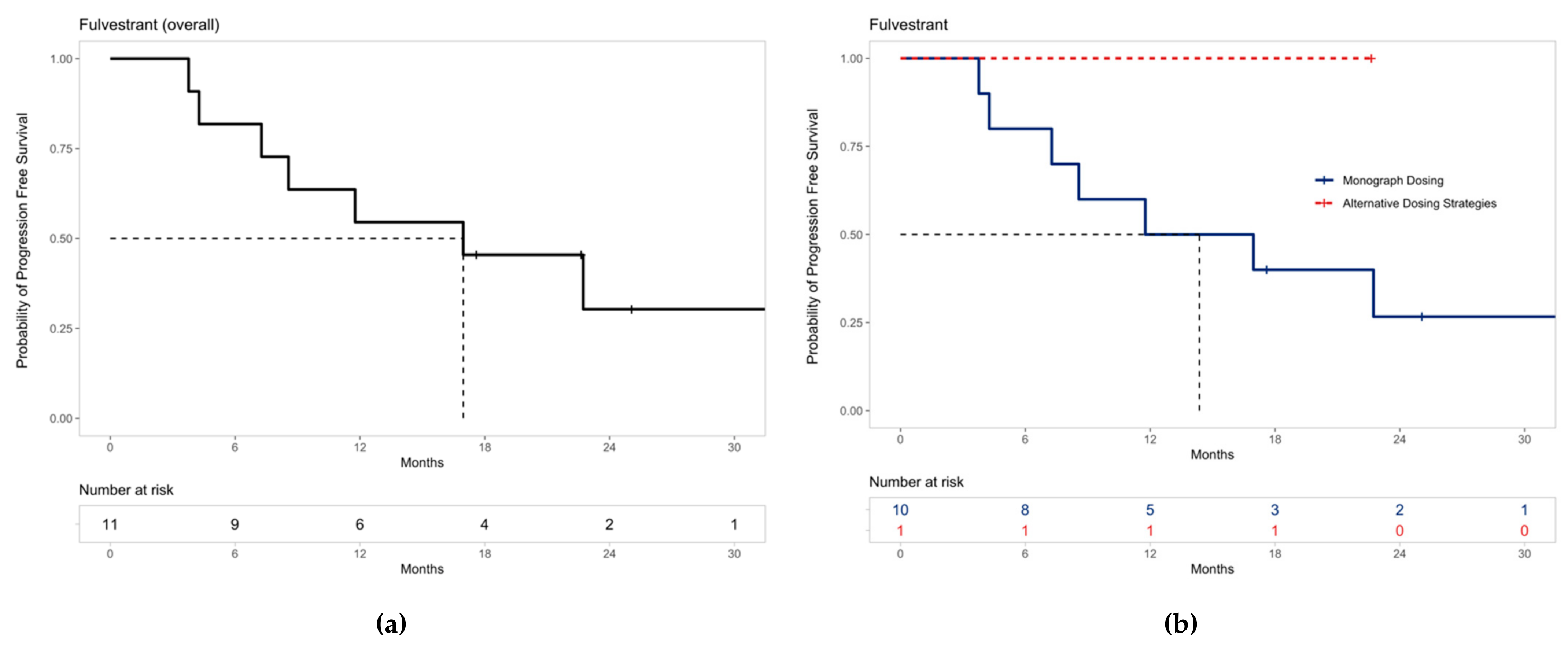
3.3. Alternative Dosing Strategies and Progression-Free Survival
4. Discussion
4.1. Study Results in the Context of Existing Literature
4.2. Implications of Alternative Dosing Strategies on Efficacy and Safety Outcomes
4.3. Limitations of the Study Design
4.4. Ongoing Research Surrounding Alternative Prescribing Schedules
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer Incidence and Mortality Worldwide: Sources, Methods and Major Patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer in Women: Burden and Trends. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2017, 26, 444–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbeck, N.; Gnant, M. Breast Cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular Portraits of Human Breast Tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Sørlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene Expression Patterns of Breast Carcinomas Distinguish Tumor Subclasses with Clinical Implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [Green Version]
- Howlader, N.; Altekruse, S.F.; Li, C.I.; Chen, V.W.; Clarke, C.A.; Ries, L.A.G.; Cronin, K.A. US Incidence of Breast Cancer Subtypes Defined by Joint Hormone Receptor and HER2 Status. JNCI J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rugo, H.S.; Rumble, R.B.; Macrae, E.; Barton, D.L.; Connolly, H.K.; Dickler, M.N.; Fallowfield, L.; Fowble, B.; Ingle, J.N.; Jahanzeb, M.; et al. Endocrine Therapy for Hormone Receptor-Positive Metastatic Breast Cancer: American Society of Clinical Oncology Guideline. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 3069–3103. [Google Scholar] [CrossRef] [PubMed]
- de Groot, A.F.; Kuijpers, C.J.; Kroep, J.R. CDK4/6 Inhibition in Early and Metastatic Breast Cancer: A Review. Cancer Treat. Rev. 2017, 60, 130–138. [Google Scholar] [CrossRef]
- O’Leary, B.; Finn, R.S.; Turner, N.C. Treating Cancer with Selective CDK4/6 Inhibitors. Nat. Rev. Clin. Oncol. 2016, 13, 417–430. [Google Scholar] [CrossRef]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.-A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.-A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus Palbociclib versus Fulvestrant plus Placebo for Treatment of Hormone-Receptor-Positive, HER2-Negative Metastatic Breast Cancer That Progressed on Previous Endocrine Therapy (PALOMA-3): Final Analysis of the Multicentre, Double-Blind, Phase 3 Randomised Controlled Trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gradishar, W.J.; Anderson, B.O.; Balassanian, R.; Blair, S.L.; Burstein, H.J.; Cyr, A.; Elias, A.D.; Farrar, W.B.; Forero, A.; Giordano, S.H.; et al. NCCN Guidelines Insights: Breast Cancer, Version 1.2017. J. Natl. Compr. Cancer Netw. JNCCN 2017, 15, 433–451. [Google Scholar] [CrossRef]
- Giordano, S.H.; Elias, A.D.; Gradishar, W.J. NCCN Guidelines Updates: Breast Cancer. J. Natl. Compr. Cancer Netw. JNCCN 2018, 16, 605–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvestri, M.; Cristaudo, A.; Morrone, A.; Messina, C.; Bennardo, L.; Nisticò, S.P.; Mariano, M.; Cameli, N. Emerging Skin Toxicities in Patients with Breast Cancer Treated with New Cyclin-Dependent Kinase 4/6 Inhibitors: A Systematic Review. Drug Saf. 2021, 44, 725–732. [Google Scholar] [CrossRef] [PubMed]
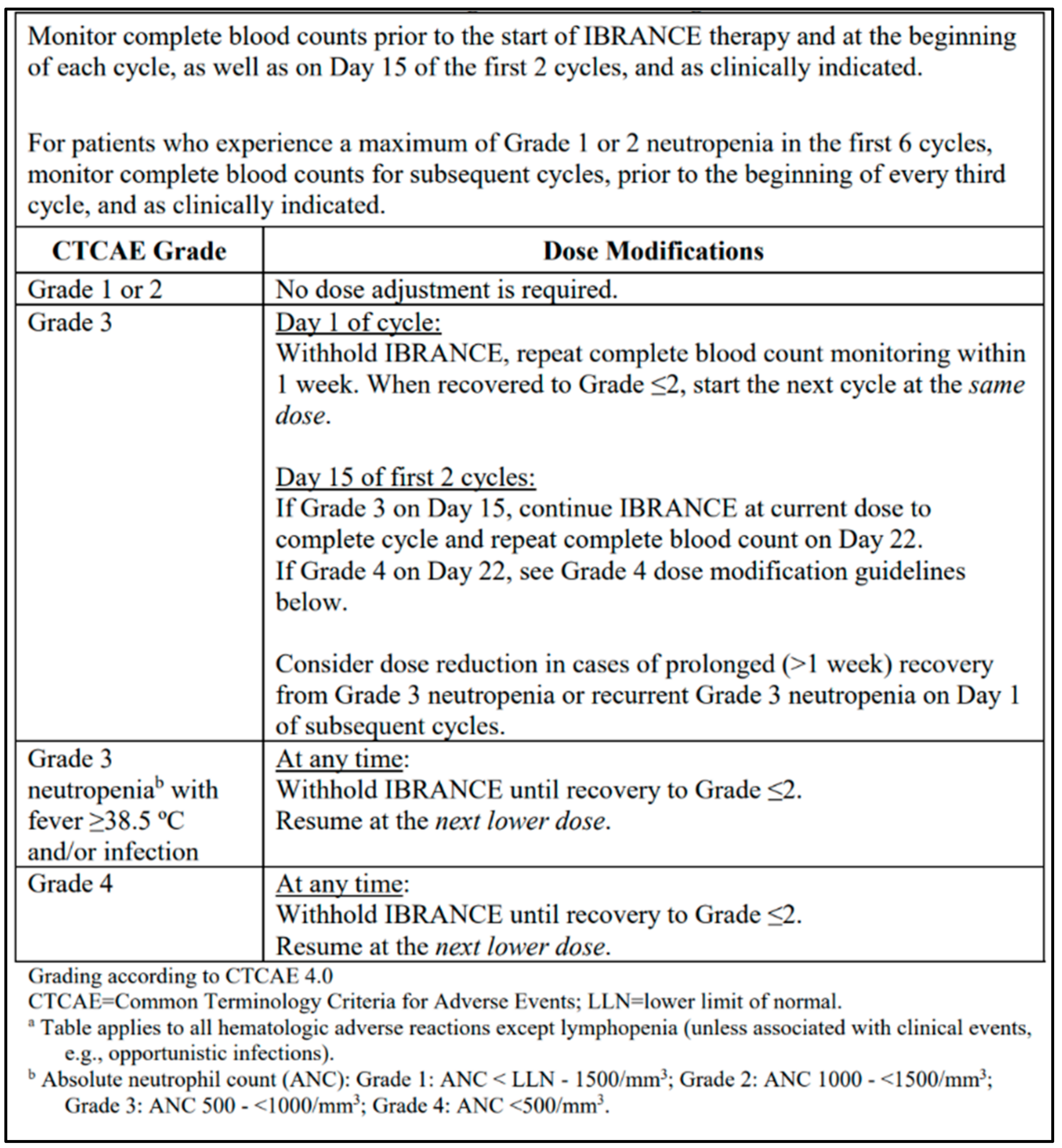
- Pfizer Canada ULC Ibrance Product Monograph. 2020. Available online: https://www.pfizer.ca/sites/default/files/202107/Ibrance_PM_EN_243405_15-Jul-2021.pdf (accessed on 14 February 2022).
- Spring, L.M.; Zangardi, M.L.; Moy, B.; Bardia, A. Clinical Management of Potential Toxicities and Drug Interactions Related to Cyclin-Dependent Kinase 4/6 Inhibitors in Breast Cancer: Practical Considerations and Recommendations. Oncologist 2017, 22, 1039–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mycock, K.; Zhan, L.; Taylor-Stokes, G.; Milligan, G.; Mitra, D. Real-World Palbociclib Use in HR+/HER2- Advanced Breast Cancer in Canada: The IRIS Study. Curr. Oncol. Tor. Ont 2021, 28, 66. [Google Scholar] [CrossRef] [PubMed]
- Amaro, C.P.; Batra, A.; Lupichuk, S. First-Line Treatment with a Cyclin-Dependent Kinase 4/6 Inhibitor Plus an Aromatase Inhibitor for Metastatic Breast Cancer in Alberta. Curr. Oncol. 2021, 28, 209. [Google Scholar] [CrossRef]
- Bui, T.B.V.; Burgers, D.M.; Agterof, M.J.; van de Garde, E.M. Real-World Effectiveness of Palbociclib Versus Clinical Trial Results in Patients with Advanced/Metastatic Breast Cancer That Progressed on Previous Endocrine Therapy. Breast Cancer Basic Clin. Res. 2019, 13, 1178223418823238. [Google Scholar] [CrossRef]
- Wilkie, J.; Schickli, M.A.; Berger, M.J.; Lustberg, M.; Reinbolt, R.; Noonan, A.; Ramaswamy, B.; Sardesai, S.; VanDeusen, J.; Wesolowski, R.; et al. Progression-Free Survival for Real-World Use of Palbociclib in Hormone Receptor-Positive Metastatic Breast Cancer. Clin. Breast Cancer 2020, 20, 33–40. [Google Scholar] [CrossRef]
- Taylor-Stokes, G.; Mitra, D.; Waller, J.; Gibson, K.; Milligan, G.; Iyer, S. Treatment Patterns and Clinical Outcomes among Patients Receiving Palbociclib in Combination with an Aromatase Inhibitor or Fulvestrant for HR+/HER2-Negative Advanced/Metastatic Breast Cancer in Real-World Settings in the US: Results from the IRIS Study. Breast Edinb. Scotl. 2019, 43, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Varella, L.; Eziokwu, A.S.; Jia, X.; Kruse, M.; Moore, H.C.F.; Budd, G.T.; Abraham, J.; Montero, A.J. Real-World Clinical Outcomes and Toxicity in Metastatic Breast Cancer Patients Treated with Palbociclib and Endocrine Therapy. Breast Cancer Res. Treat. 2019, 176, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Watson, G.A.; Deac, O.; Aslam, R.; O’Dwyer, R.; Tierney, A.; Sukor, S.; Kennedy, J. Real-World Experience of Palbociclib-Induced Adverse Events and Compliance With Complete Blood Count Monitoring in Women With Hormone Receptor-Positive/HER2-Negative Metastatic Breast Cancer. Clin. Breast Cancer 2019, 19, e186–e194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Park, H.S.; Won, H.S.; Yang, J.H.; Lee, H.Y.; Woo, I.S.; Shin, K.; Hong, J.H.; Yang, Y.J.; Chun, S.H.; et al. Real-World Clinical Data of Palbociclib in Asian Metastatic Breast Cancer Patients: Experiences from Eight Institutions. Cancer Res. Treat. 2021, 53, 409–423. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Bartlett, M.; Spurden, D.; Hooper, B.; Zhan, L.; Rosta, E.; Cameron, C.; Mitra, D.; Zhou, A. CDK4/6 Inhibitors in HR+/HER2- Advanced/Metastatic Breast Cancer: A Systematic Literature Review of Real-World Evidence Studies. Future Oncol. 2021, 17, 2107–2122. [Google Scholar] [CrossRef] [PubMed]
- DeMichele, A.; Cristofanilli, M.; Brufsky, A.; Liu, X.; Mardekian, J.; McRoy, L.; Layman, R.M.; Emir, B.; Torres, M.A.; Rugo, H.S.; et al. Comparative Effectiveness of First-Line Palbociclib plus Letrozole versus Letrozole Alone for HR+/HER2- Metastatic Breast Cancer in US Real-World Clinical Practice. Breast Cancer Res. BCR 2021, 23, 37. [Google Scholar] [CrossRef]
- Fernández-Cuerva, C.; Valencia, J.C.D.R.; Bermejo, R.T. Effectiveness and Safety of Palbociclib plus Endocrine Therapy in Hormone Receptor-Positive, HER2-Negative Metastatic Breast Cancer: Real-World Results. Can. J. Hosp. Pharm. 2022, 75, 26–33. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Litière, S.; de Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1-Update and Clarification: From the RECIST Committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Common Terminology Criteria for Adverse Events (CTCAE). 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_8.5x11.pdf (accessed on 14 February 2022).
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 24 January 2022).
- Tripathy, D.; Blum, J.L.; Rocque, G.B.; Bardia, A.; Karuturi, M.S.; Cappelleri, J.C.; Liu, Y.; Zhang, Z.; Davis, K.L.; Wang, Y. POLARIS: A Prospective, Multicenter, Noninterventional Study Assessing Palbociclib in Hormone Receptor-Positive Advanced Breast Cancer. Future Oncol. 2020, 16, 2475–2485. [Google Scholar] [CrossRef]
- Parulekar, W.R.; Joy, A.A.; Gelmon, K.; Mates, M.; Desbiens, C.; Clemons, M.; Taylor, S.; Lemieux, J.; Bartlett, J.; Whelan, T.; et al. Abstract PD1-10: Randomized Phase II Study Comparing Two Different Schedules of Palbociclib plus Second Line Endocrine Therapy in Women with Estrogen Receptor Positive, HER2 Negative Advanced/Metastatic Breast Cancer: CCTG MA38 (NCT02630693). Cancer Res. 2019, 79, PD1-10. [Google Scholar] [CrossRef]
- Krishnamurthy, J.; Luo, J.; Ademuyiwa, F.; Suresh, R.; Rigden, C.; Reardon, T.; Weilbaecher, K.; Frith, A.; Roshal, A.; Tandra, P.; et al. Abstract P1-19-13: A Phase II Trial Assessing the Safety of an Alternative Dosing Schedule of Palbociclib (Palbo) in Hormone Receptor Positive (HR+), HER2 Negative (HER2-) Metastatic Breast Cancer (MBC): Alt Dose Palbo. Cancer Res. 2020, 80, P1-19-13. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (n = 74) | Palbociclib with Letrozole (n = 63) | Palbociclib with Fulvestrant (n = 11) |
|---|---|---|---|
| Treatment Site—n (%) | |||
| Credit Valley Hospital | 54 (73.0%) | 46 (73.0%) | 8 (72.7%) |
| Queensway Health Centre | 20 (27.0%) | 17 (27.0%) | 3 (27.3%) |
| Age | |||
| Mean (SD) | 57.4 (12.6) | 57.2 (12.5) | 59.1 (14.0) |
| Median (range) | 57.5 (33–85) | 55 (34–85) | 60 (33–77) |
| <65—n (%) | 52 (70.3%) | 44 (69.8%) | 8 (72.7%) |
| ≥65—n (%) | 22 (29.7%) | 19 (30.2%) | 3 (27.3%) |
| ECOG Performance Status—n (%) | |||
| 0 | 19 (25.7%) | 17 (27.0%) | 2 (18.2%) |
| 1 | 49 (66.2%) | 41 (65.1%) | 8 (72.7%) |
| 2 | 5 (6.8%) | 5 (7.9%) | 0 (0%) |
| 3 | 1 (1.4%) | 0 (0%) | 1 (9.1%) |
| Disease Site | |||
| Bone | 63 (85.1%) | 56 (88.9%) | 7 (63.6%) |
| Bone only | 27 (36.5%) | 25 (39.7%) | 2 (18.2%) |
| Lung | 18 (24.3%) | 14 (22.2%) | 4 (36.4%) |
| Pleura | 13 (17.6%) | 11 (17.4%) | 2 (18.2%) |
| Liver | 14 (18.9%) | 8 (12.7%) | 6 (54.5%) |
| CNS | 2 (2.7%) | 1 (1.6%) | 1 (9.1%) |
| Other | 16 (21.6%) | 14 (22.2%) | 2 (18.2%) |
| Received prior adjuvant or neoadjuvant endocrine therapy | 13 (17.6%) | 7 (11.1%) | 6 (54.5%) |
| Received prior endocrine therapy in the metastatic setting | |||
| Anastrozole | 1 (1.4%) | 0 (0%) | 1 (9.1%) |
| Exemestane | 5 (6.8%) | 3 (4.8%) | 2 (18.2%) |
| Letrozole | 5 (6.8%) | 0 (0%) | 5 (45.5%) |
| Tamoxifen | 6 (8.1%) | 5 (7.9%) | 1 (9.1%) |
| Received prior adjuvant therapy | |||
| Anastrozole | 9 (12.2%) | 7 (11.1%) | 2 (18.2%) |
| Exemestane | 5 (6.8%) | 4 (6.3%) | 1 (9.1%) |
| Letrozole | 2 (2.7%) | 1 (1.6%) | 1 (9.1%) |
| Tamoxifen | 32 (43.2%) | 24 (38.1%) | 8 (72.7%) |
| Average cycles of palbociclib received | |||
| Mean (SD) | 17.9 (8.9) | 18.3 (8.7) | 15.4 (9.9) |
| Median (range) | 17 (2–48) | 17 (2–48) | 15 (3–34) |
| Any dose modifications received (monograph or unique) | 33 (44.6%) | 30 (47.6%) | 3 (27.3%) |
| Monograph dose reductions | 4 (5.4%) | 2 (3.2%) | 2 (18.2%) |
| Alternative dosing strategies | 29 (39.2%) | 28 (44.4%) | 1 (9.1%) |
| Treatment Group | Grade 3 n (%) | Grade 4 n (%) | Grade 3 and 4 n (%) |
|---|---|---|---|
| Letrozole (n = 63) | 42 (66.7%) | 4 (6.3%) | 46 (73%) |
| Fulvestrant (n = 11) | 5 (45.5%) | 1 (9.1%) | 6 (54.5%) |
| Palbociclib Dosing Strategy | Patients (n) | 6 Months (n) | 12 Months (n) | 15 Months (n) | 18 Months (n) |
|---|---|---|---|---|---|
| Letrozole (Overall) | 63 | 59 | 53 | 49 | 35 |
| Monograph dosing | 35 | 31 | 26 | 24 | 18 |
| Alternative Dosing Strategies | |||||
| Palbociclib prescribed 3 weeks on, 2 weeks off | 8 | 8 | 7 | 6 | 4 |
| Palbociclib dose decreased for only one episode of ANC < 1.0 × 109/L | 6 | 6 | 6 | 5 | 4 |
| Lowered palbociclib dose despite ANC > 1.0 × 109/L | 5 | 5 | 5 | 5 | 4 |
| Remained on palbociclib 75 mg despite recurrent grade 3 neutropenia | 5 | 5 | 5 | 5 | 2 |
| Decreased palbociclib from 125 mg to 75 mg for grade 3 neutropenia | 2 | 2 | 2 | 2 | 2 |
| Palbociclib initiated at 100 mg daily | 1 | 1 | 1 | 1 | 0 |
| Palbociclib prescribed 2 weeks on, 2 weeks off | 1 | 1 | 1 | 1 | 1 |
| Fulvestrant (Overall) | 11 | 9 | 6 | 6 | 4 |
| Monograph dosing | 10 | 8 | 5 | 5 | 3 |
| Alternative Dosing Strategies | |||||
| Palbociclib dose decreased for only one episode of ANC < 1.0 × 109/L | 1 | 1 | 1 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, F.; Kano, J.; Ma, J.; Guindy, M. The Impact of Real-World Alternative Dosing Strategies of Palbociclib on Progression-Free Survival in Patients with Metastatic Breast Cancer. Curr. Oncol. 2022, 29, 1761-1772. https://doi.org/10.3390/curroncol29030145
Fu F, Kano J, Ma J, Guindy M. The Impact of Real-World Alternative Dosing Strategies of Palbociclib on Progression-Free Survival in Patients with Metastatic Breast Cancer. Current Oncology. 2022; 29(3):1761-1772. https://doi.org/10.3390/curroncol29030145
Chicago/Turabian StyleFu, Fulbert, Jessica Kano, Julia Ma, and Mera Guindy. 2022. "The Impact of Real-World Alternative Dosing Strategies of Palbociclib on Progression-Free Survival in Patients with Metastatic Breast Cancer" Current Oncology 29, no. 3: 1761-1772. https://doi.org/10.3390/curroncol29030145
APA StyleFu, F., Kano, J., Ma, J., & Guindy, M. (2022). The Impact of Real-World Alternative Dosing Strategies of Palbociclib on Progression-Free Survival in Patients with Metastatic Breast Cancer. Current Oncology, 29(3), 1761-1772. https://doi.org/10.3390/curroncol29030145