Applications of Artificial Intelligence in Screening, Diagnosis, Treatment, and Prognosis of Colorectal Cancer


Abstract
:1. Introduction
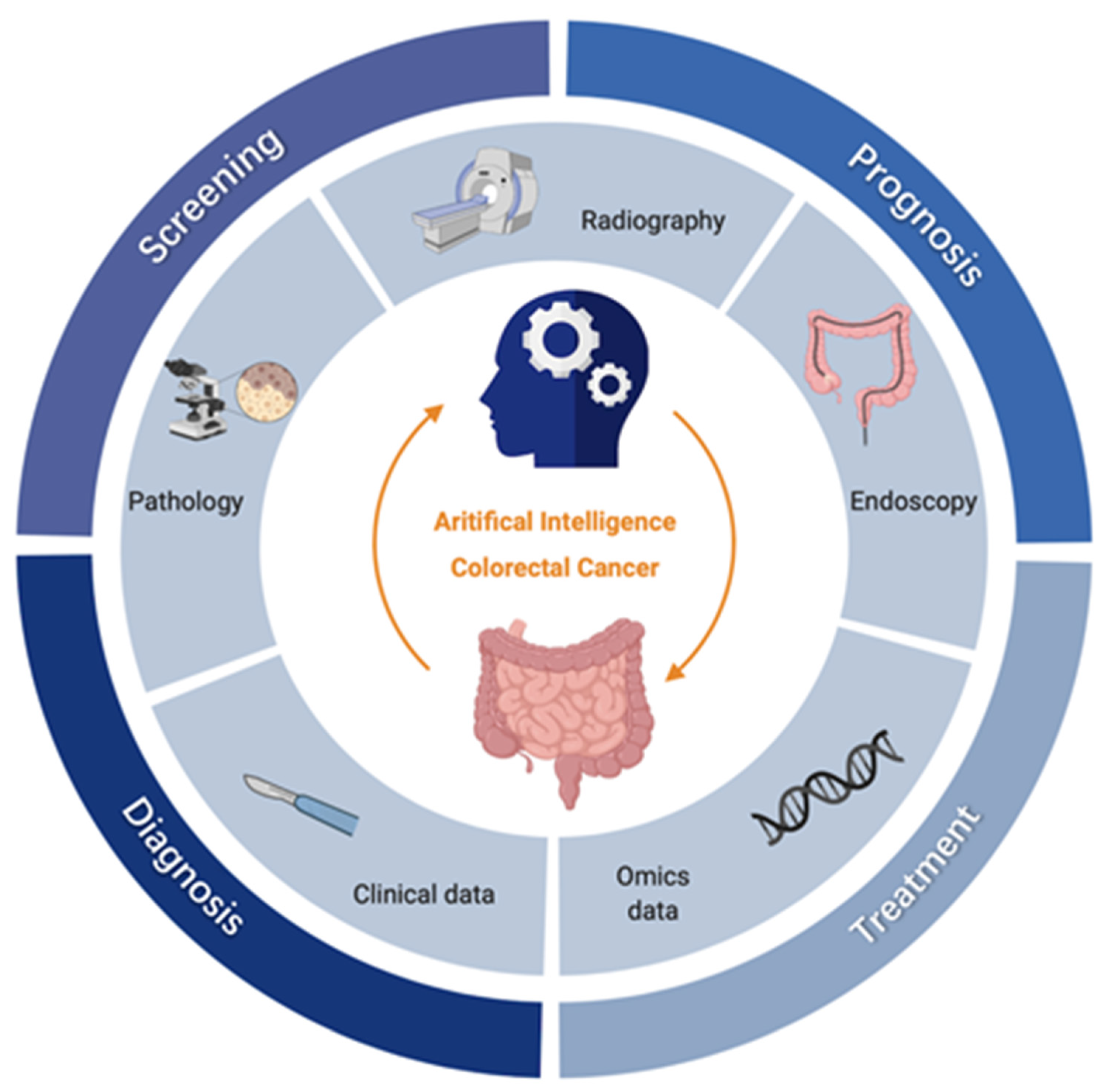
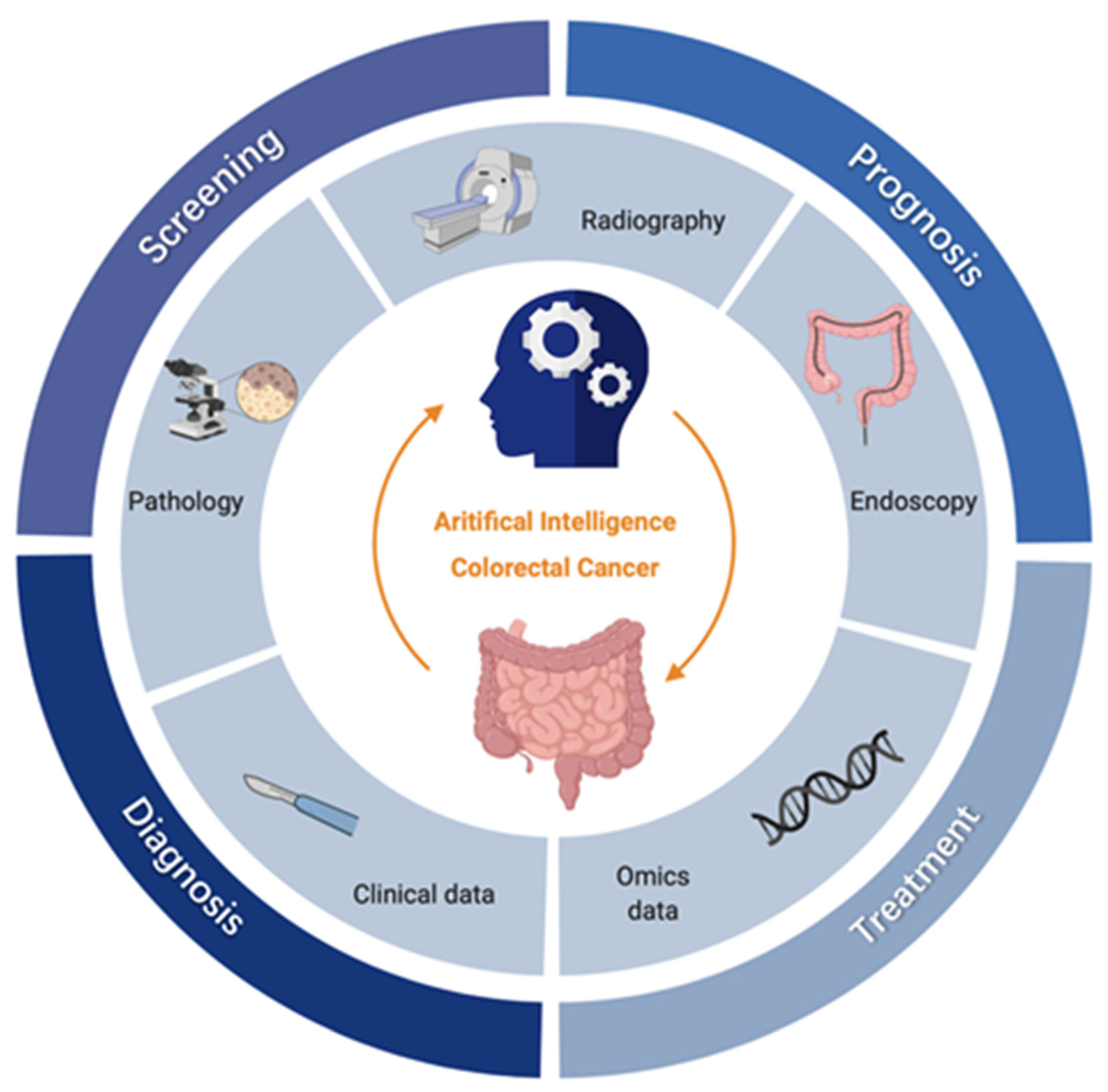
- Screening: Endoscopy is considered the gold standard for CRC screening, supplemented with fecal occult blood test (FOBT), but these methods are relatively dependent on clinical experience and prone to omission and misdiagnosis. The increasing prevalence of endoscopic imaging datasets and electronic medical records (EMRs), AI-assisted endoscopy for polyp detection and characterization, and the use of high-risk prediction models using clinical and omics data, are expected to improve the accuracy and efficiency of CRC screening.
- Diagnosis: The qualitative diagnosis and staging of CRC mainly rely on radiography and pathological examination [5]. Thanks to advanced processing technology in the field of image recognition, DL can significantly improve medical image readability, eliminate differences in experience, and reduce misdiagnosis rates.
- Treatment: The most commonly used methods for clinical treatment of CRC are surgery, chemotherapy and radiotherapy [7]. Novel therapies and tools can be evaluated with the help of AI, such as neoadjuvant radiotherapy (nCRT) and chemotherapy, to improve curative effects and provide more precise medical care to patients.
- Prognosis: Prognosis of CRC includes the predicting of recurrence and estimating of the survival period [3]. Statistical methods such as the Cox regression model are traditionally used to predict patient prognosis; however, data-driven ML approaches allow for more effective exploitation of multidimensional data to accurately predict survival and flexibly track disease progression.
2. Overview of Artificial Intelligence
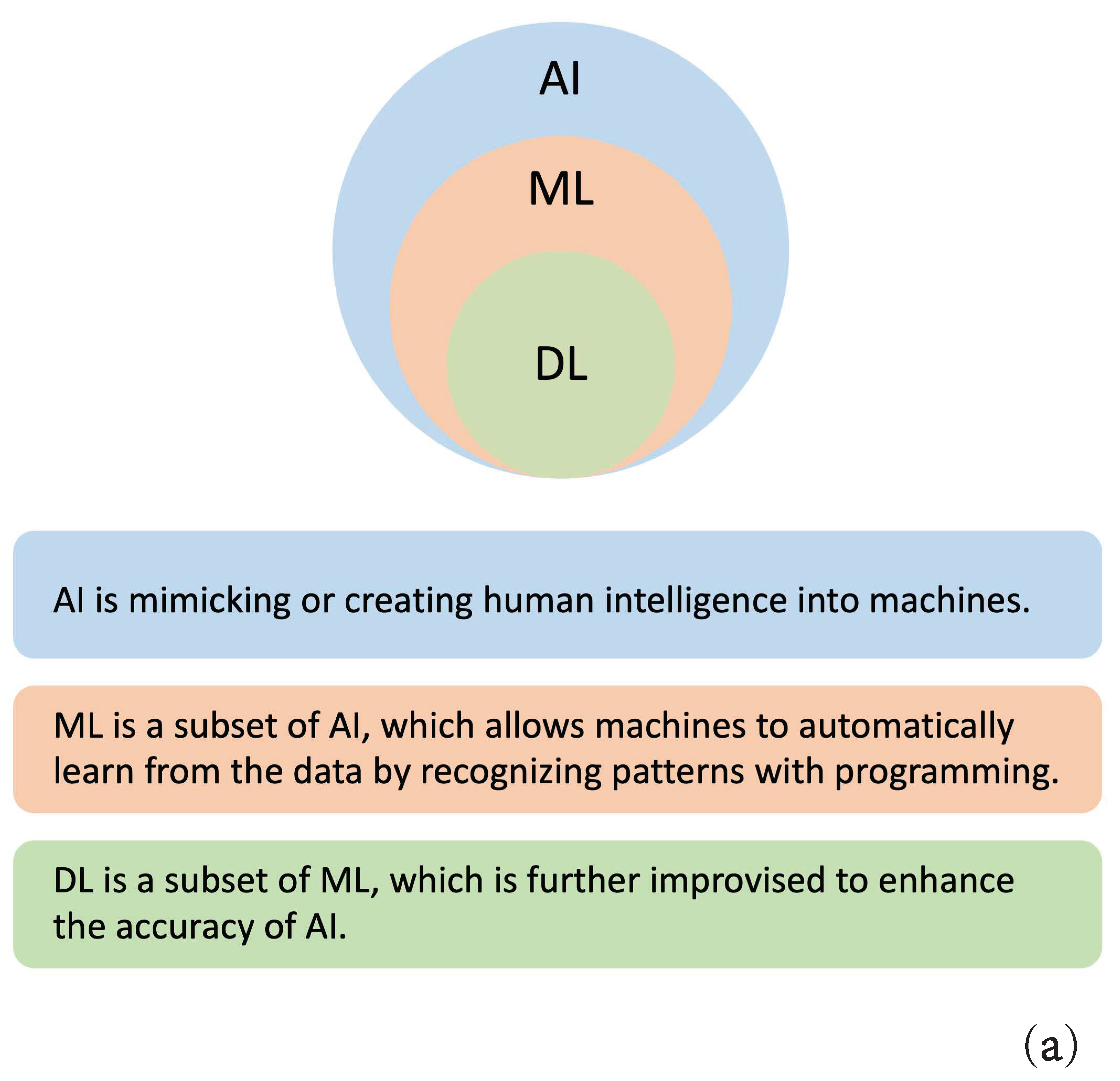
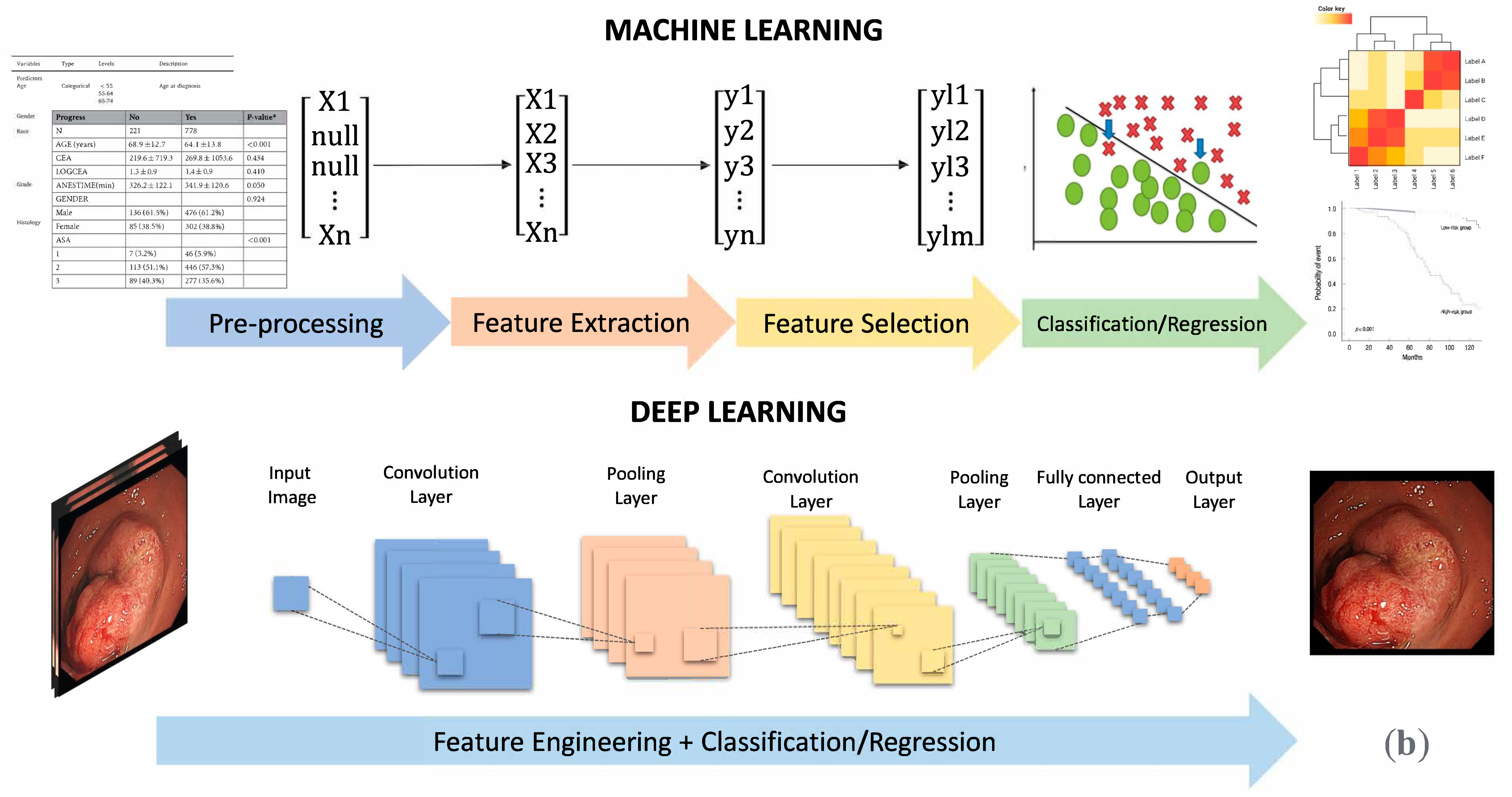
2.1. Basics Concepts of AI
2.2. Data Modality
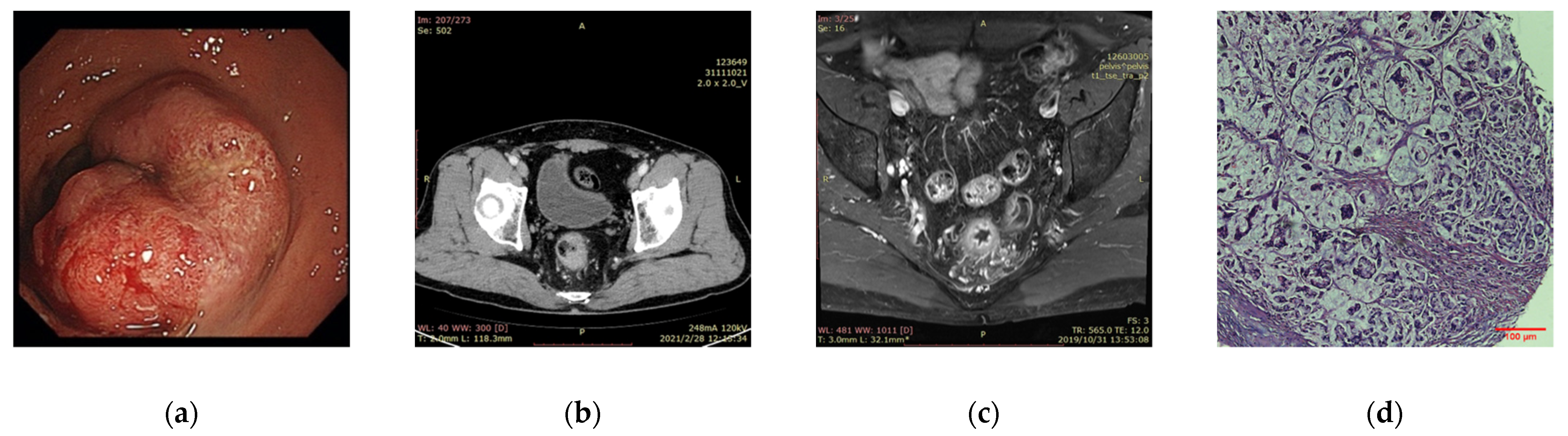
2.2.1. Image Data
2.2.2. Clinical Data
2.2.3. Omics Data
3. Applications in CRC Screening
3.1. Polyp Detection and Characterization
3.2. Population-Based Risk Prediction
3.3. Limitations
4. Applications in CRC Diagnosis and Staging
4.1. Pathological Diagnosis
4.2. Radiological Diagnosis
4.3. Limitations
5. Applications in CRC Treatment
5.1. nCRT Response Prediction
5.2. Adjuvant Chemotherapy Response Prediction
5.3. Limitations
6. Applications in CRC Prognosis
6.1. Recurrence Prediction
6.2. Survival Prediction
6.3. Limitations
7. Current Challenges
8. Future Prospects
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Patterns and Trends in Colorectal Cancer Incidence and Mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, W.; Xie, L.; Han, J.; Guo, X. The Application of Deep Learning in Cancer Prognosis Prediction. Cancers 2020, 12, 603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chahal, D.; Byrne, M.F. A Primer on Artificial Intelligence and Its Application to Endoscopy. Gastrointest. Endosc. 2020, 92, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Goyal, H.; Mann, R.; Gandhi, Z.; Perisetti, A.; Ali, A.; Aman Ali, K.; Sharma, N.; Saligram, S.; Tharian, B.; Inamdar, S. Scope of Artificial Intelligence in Screening and Diagnosis of Colorectal Cancer. J. Clin. Med. 2020, 9, 3313. [Google Scholar] [CrossRef] [PubMed]
- Pacal, I.; Karaboga, D.; Basturk, A.; Akay, B.; Nalbantoglu, U. A Comprehensive Review of Deep Learning in Colon Cancer. Comput. Biol. Med. 2020, 126, 104003. [Google Scholar] [CrossRef]
- Gao, Y.; Zhang, X.X.; Li, S.; Lu, Y. Application of Artificial Intelligence Technology in the Diagnosis and Treatment of Colorectal Cancer. Chin. J. Gastrointest. Surg. 2020, 23, 1155–1158. [Google Scholar] [CrossRef]
- Moor, J. The Dartmouth College Artificial Intelligence Conference: The next Fifty Years. AI Magazine 2006, 27, 87. [Google Scholar]
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial Intelligence in Cancer Diagnosis and Prognosis: Opportunities and Challenges. Cancer Lett. 2020, 471, 61–71. [Google Scholar] [CrossRef]
- Koteluk, O.; Wartecki, A.; Mazurek, S.; Kołodziejczak, I.; Mackiewicz, A. How Do Machines Learn? Artificial Intelligence as a New Era in Medicine. J. Pers. Med. 2021, 11, 32. [Google Scholar] [CrossRef]
- Alizadehsani, R.; Khosravi, A.; Roshanzamir, M.; Abdar, M.; Sarrafzadegan, N.; Shafie, D.; Khozeimeh, F.; Shoeibi, A.; Nahavandi, S.; Panahiazar, M.; et al. Coronary Artery Disease Detection Using Artificial Intelligence Techniques: A Survey of Trends, Geographical Differences and Diagnostic Features 1991–2020. Comput. Biol. Med. 2021, 128, 104095. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.N.; Khoshgoftaar, T.M. A Review of Statistical and Machine Learning Methods for Modeling Cancer Risk Using Structured Clinical Data. Artif. Intell. Med. 2018, 90, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamamoto, R.; Suvarna, K.; Yamada, M.; Kobayashi, K.; Shinkai, N.; Miyake, M.; Takahashi, M.; Jinnai, S.; Shimoyama, R.; Sakai, A.; et al. Application of Artificial Intelligence Technology in Oncology: Towards the Establishment of Precision Medicine. Cancers 2020, 12, 3532. [Google Scholar] [CrossRef] [PubMed]
- Biswas, N.; Chakrabarti, S. Artificial Intelligence (AI)-Based Systems Biology Approaches in Multi-Omics Data Analysis of Cancer. Front. Oncol. 2020, 10, 2224. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA A Cancer J. Clin. 2021, 1, 7–33. [Google Scholar] [CrossRef]
- Nazari, E.; Aghemiri, M.; Avan, A.; Mehrabian, A.; Tabesh, H. Machine Learning Approaches for Classification of Colorectal Cancer with and without Feature Selection Method on Microarray Data. Gene Rep. 2021, 25, 101419. [Google Scholar] [CrossRef]
- Lee, K.-S.; Son, S.-H.; Park, S.-H.; Kim, E.S. Automated Detection of Colorectal Tumors Based on Artificial Intelligence. BMC Med. Inf. Decis. Mak. 2021, 21, 33. [Google Scholar] [CrossRef]
- Pan, Y.; Zhang, L.; Zhang, R.; Han, J.; Qin, W.; Gu, Y.; Sha, J.; Xu, X.; Ren, Z.; Dai, J.; et al. Screening and Diagnosis of Colorectal Cancer and Advanced Adenoma by Bionic Glycome Method and Machine Learning. Am. J. Cancer Res. 2021, 31, 3002–3020. [Google Scholar]
- Ivancic, M.M.; Megna, B.W.; Sverchkov, Y.; Craven, M.; Reichelderfer, M.; Pickhardt, P.J.; Sussman, M.R.; Kennedy, G.D. Noninvasive Detection of Colorectal Carcinomas Using Serum Protein Biomarkers. J. Surg. Res. 2020, 246, 160–169. [Google Scholar] [CrossRef]
- Ozawa, T.; Ishihara, S.; Fujishiro, M.; Kumagai, Y.; Shichijo, S.; Tada, T. Automated Endoscopic Detection and Classification of Colorectal Polyps Using Convolutional Neural Networks. Ther. Adv. Gastroenterol. 2020, 13, 175628482091065. [Google Scholar] [CrossRef] [Green Version]
- Kayser, M.; Soberanis-Mukul, R.D.; Zvereva, A.-M.; Klare, P.; Navab, N.; Albarqouni, S. Understanding the Effects of Artifacts on Automated Polyp Detection and Incorporating That Knowledge via Learning without Forgetting. arXiv 2020. [Google Scholar] [CrossRef]
- Qadir, H.A.; Balasingham, I.; Solhusvik, J.; Bergsland, J.; Aabakken, L.; Shin, Y. Improving Automatic Polyp Detection Using CNN by Exploiting Temporal Dependency in Colonoscopy Video. IEEE J. Biomed. Health Inform. 2020, 24, 180–193. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Pu, L.Z.C.T.; Singh, R.; Burt, A.D.; Carneiro, G. One-Stage Five-Class Polyp Detection and Classification. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 70–73. [Google Scholar]
- Urban, G.; Tripathi, P.; Alkayali, T.; Mittal, M.; Jalali, F.; Karnes, W.; Baldi, P. Deep Learning Localizes and Identifies Polyps in Real Time With 96% Accuracy in Screening Colonoscopy. Gastroenterology 2018, 155, 1069–1078. [Google Scholar] [CrossRef]
- Akbari, M.; Mohrekesh, M.; Nasr-Esfahani, E.; Soroushmehr, S.M.R.; Karimi, N.; Samavi, S.; Najarian, K. Polyp Segmentation in Colonoscopy Images Using Fully Convolutional Network. IEEE 2018, 69–72. [Google Scholar] [CrossRef] [Green Version]
- Hilsden, R.J.; Heitman, S.J.; Mizrahi, B.; Narod, S.A.; Goshen, R. Prediction of Findings at Screening Colonoscopy Using a Machine Learning Algorithm Based on Complete Blood Counts (ColonFlag). PLoS ONE 2018, 13, e0207848. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zheng, Y.; Mak, T.W.C.; Yu, R.; Wong, S.H.; Lau, J.Y.W.; Poon, C.C.Y. Automatic Detection and Classification of Colorectal Polyps by Transferring Low-Level CNN Features from Nonmedical Domain. IEEE J. Biomed. Health Inform. 2017, 21, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Hornbrook, M.C.; Goshen, R.; Choman, E.; O’Keeffe-Rosetti, M.; Kinar, Y.; Liles, E.G.; Rust, K.C. Early Colorectal Cancer Detected by Machine Learning Model Using Gender, Age, and Complete Blood Count Data. Dig. Dis. Sci. 2017, 62, 2719–2727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinar, Y.; Akiva, P.; Choman, E.; Kariv, R.; Shalev, V.; Levin, B.; Narod, S.A.; Goshen, R. Performance Analysis of a Machine Learning Flagging System Used to Identify a Group of Individuals at a High Risk for Colorectal Cancer. PLoS ONE 2017, 12, e0171759. [Google Scholar] [CrossRef]
- Fernández-Esparrach, G.; Bernal, J.; López-Cerón, M.; Córdova, H.; Sánchez-Montes, C.; Rodríguez De Miguel, C.; Sánchez, F.J. Exploring the Clinical Potential of an Automatic Colonic Polyp Detection Method Based on the Creation of Energy Maps. Endoscopy 2016, 48, 837–842. [Google Scholar] [CrossRef]
- Kinar, Y.; Kalkstein, N.; Akiva, P.; Levin, B.; Half, E.E.; Goldshtein, I.; Chodick, G.; Shalev, V. Development and Validation of a Predictive Model for Detection of Colorectal Cancer in Primary Care by Analysis of Complete Blood Counts: A Binational Retrospective Study. J. Am. Med. Inform. Assoc. 2016, 23, 879–890. [Google Scholar] [CrossRef] [Green Version]
- Takemura, Y.; Yoshida, S.; Tanaka, S.; Kawase, R.; Onji, K.; Oka, S.; Tamaki, T.; Raytchev, B.; Kaneda, K.; Yoshihara, M.; et al. Computer-Aided System for Predicting the Histology of Colorectal Tumors by Using Narrow-Band Imaging Magnifying Colonoscopy (with Video). Gastrointest. Endosc. 2012, 75, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Issa, I.A.; NouredDine, M. Colorectal Cancer Screening: An Updated Review of the Available Options. World J. Gastroenterol. 2017, 23, 5086–5096. [Google Scholar] [CrossRef] [PubMed]
- Van Rijn, J.C.; Reitsma, J.B.; Stoker, J.; Bossuyt, P.M.; Van Deventer, S.J.; Dekker, E. Polyp Miss Rate Determined by Tandem Colonoscopy: A Systematic Review. Am. J. Gastroenterol. 2006, 101, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.J.; Lin, M.C.; Lai, M.J.; Lin, J.C.; Lu, H.H.S.; Tseng, V.S. Accurate Classification of Diminutive Colorectal Polyps Using Computer-Aided Analysis. Gastroenterology 2018, 154, 568–575. [Google Scholar] [CrossRef]
- Yamada, M.; Saito, Y.; Imaoka, H.; Saiko, M.; Yamada, S.; Kondo, H.; Takamaru, H.; Sakamoto, T.; Sese, J.; Kuchiba, A.; et al. Development of a Real-Time Endoscopic Image Diagnosis Support System Using Deep Learning Technology in Colonoscopy. Sci. Rep. 2019, 9, 14465. [Google Scholar] [CrossRef] [Green Version]
- Wan, N.; Weinberg, D.; Liu, T.Y.; Niehaus, K.; Delubac, D.; Kannan, A.; White, B.; Ariazi, E.A.; Bailey, M.; Bertin, M.; et al. Machine Learning Enables Detection of Early-Stage Colorectal Cancer by Whole-Genome Sequencing of Plasma Cell-Free DNA. bioRxiv 2018, 19, 832. [Google Scholar] [CrossRef] [Green Version]
- Kyrochristos, I.D.; Roukos, D.H. Comprehensive Intra-Individual Genomic and Transcriptional Heterogeneity: Evidence-Based Colorectal Cancer Precision Medicine. Cancer Treat. Rev. 2019, 80, 101894. [Google Scholar] [CrossRef]
- Mori, Y.; Bretthauer, M.; Kalager, M. Hopes and Hypes for Artificial Intelligence in Colorectal Cancer Screening. Gastroenterology 2021, 161, 774–777. [Google Scholar] [CrossRef]
- Song, C.L.; Vardaki, M.Z.; Goldin, R.D.; Kazarian, S.G. Fourier Transform Infrared Spectroscopic Imaging of Colon Tissues: Evaluating the Significance of Amide I and C–H Stretching Bands in Diagnostic Applications with Machine Learning. Anal. Bioanal. Chem. 2019, 411, 6969–6981. [Google Scholar] [CrossRef] [Green Version]
- Shimada, Y.; Okuda, S.; Watanabe, Y.; Tajima, Y.; Nagahashi, M.; Ichikawa, H.; Nakano, M.; Sakata, J.; Takii, Y.; Kawasaki, T.; et al. Histopathological Characteristics and Artificial Intelligence for Predicting Tumor Mutational Burden-High Colorectal Cancer. J Gastroenterol 2021, 56, 547–559. [Google Scholar] [CrossRef]
- Theodosi, A.; Ouzounis, S.; Kostopoulos, S.; Glotsos, D.; Kalatzis, I.; Tzelepi, V.; Ravazoula, P.; Asvestas, P.; Cavouras, D.; Sakellaropoulos, G. Design of a Hybrid Deep Learning System for Discriminating between Low- and High-Grade Colorectal Cancer Lesions, Using Microscopy Images of IHC Stained for AIB1 Expression Biopsy Material. Mach. Vis. Appl. 2021, 32, 58. [Google Scholar] [CrossRef]
- Iizuka, O.; Kanavati, F.; Kato, K.; Rambeau, M.; Arihiro, K.; Tsuneki, M. Deep Learning Models for Histopathological Classification of Gastric and Colonic Epithelial Tumours. Sci. Rep. 2020, 10, 1504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, P.; Wang, W.; Li, L.; Zhang, G.; Gao, Z.; Tang, Z.; Dang, X.; Wu, Y. Profiles of Immune Cell Infiltration and Immune-Related Genes in the Tumor Microenvironment of Colorectal Cancer. Biomed. Pharmacother. 2019, 118, 109228. [Google Scholar] [CrossRef] [PubMed]
- Kather, J.N.; Pearson, A.T.; Halama, N.; Jäger, D.; Krause, J.; Loosen, S.H.; Marx, A.; Boor, P.; Tacke, F.; Neumann, U.P.; et al. Deep Learning Can Predict Microsatellite Instability Directly from Histology in Gastrointestinal Cancer. Nat. Med. 2019, 25, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Sena, P.; Fioresi, R.; Faglioni, F.; Losi, L.; Faglioni, G.; Roncucci, L. Deep Learning Techniques for Detecting Preneoplastic and Neoplastic Lesions in Human Colorectal Histological Images. Oncol. Lett. 2019, 18, 6101–6107. [Google Scholar] [CrossRef] [Green Version]
- Yoon, H.; Lee, J.; Oh, J.E.; Kim, H.R.; Lee, S.; Chang, H.J.; Sohn, D.K. Tumor Identification in Colorectal Histology Images Using a Convolutional Neural Network. 2019; 32, pp. 131–140. [Google Scholar] [CrossRef]
- Ponzio, F.; Macii, E.; Ficarra, E.; Di Cataldo, S. Colorectal Cancer Classification Using Deep Convolutional Networks. Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies 2, 58–66. [CrossRef]
- Haj-Hassan, H.; Chaddad, A.; Harkouss, Y.; Desrosiers, C.; Toews, M.; Tanougast, C. Classifications of Multispectral Colorectal Cancer Tissues Using Convolution Neural Network. J. Pathol. Inform. 2017, 8, 1. [Google Scholar] [CrossRef]
- Xu, Y.; Jia, Z.; Wang, L.B.; Ai, Y.; Zhang, F.; Lai, M.; Chang, E.I.C. Large Scale Tissue Histopathology Image Classification, Segmentation, and Visualization via Deep Convolutional Activation Features. BMC Bioinform. 2017, 18, 281. [Google Scholar] [CrossRef] [Green Version]
- Korbar, B.; Olofson, A.; Miraflor, A.; Nicka, C.; Suriawinata, M.; Torresani, L.; Suriawinata, A.; Hassanpour, S. Deep Learning for Classification of Colorectal Polyps on Whole-Slide Images. J. Pathol. Inform. 2017, 8, 30. [Google Scholar] [CrossRef]
- Daye, D.; Tabari, A.; Kim, H.; Chang, K.; Kamran, S.C.; Hong, T.S.; Kalpathy-Cramer, J.; Gee, M.S. Quantitative Tumor Heterogeneity MRI Profiling Improves Machine Learning–Based Prognostication in Patients with Metastatic Colon Cancer. Eur. Radiol. 2021, 31, 5759–5767. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Wang, Q.; Zhang, Y.; Wu, H.; Zhou, Y.; Zhao, S. Preoperative Prediction of Regional Lymph Node Metastasis of Colorectal Cancer Based on 18F-FDG PET/CT and Machine Learning. Ann. Nucl. Med. 2021, 35, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Kiritani, S.; Yoshimura, K.; Arita, J.; Kokudo, T.; Hakoda, H.; Tanimoto, M.; Ishizawa, T.; Akamatsu, N.; Kaneko, J.; Takeda, S.; et al. A New Rapid Diagnostic System with Ambient Mass Spectrometry and Machine Learning for Colorectal Liver Metastasis. BMC Cancer 2021, 21, 262. [Google Scholar] [CrossRef] [PubMed]
- Taghavi, M.; Trebeschi, S.; Simões, R.; Meek, D.B.; Beckers, R.C.J.; Lambregts, D.M.J.; Verhoef, C.; Houwers, J.B.; van der Heide, U.A.; Beets-Tan, R.G.H.; et al. Machine Learning-Based Analysis of CT Radiomics Model for Prediction of Colorectal Metachronous Liver Metastases. Abdom. Radiol. 2021, 46, 249–256. [Google Scholar] [CrossRef]
- González-Castro, V.; Cernadas, E.; Huelga, E.; Fernández-Delgado, M.; Porto, J.; Antunez, J.R.; Souto-Bayarri, M. CT Radiomics in Colorectal Cancer: Detection of KRAS Mutation Using Texture Analysis and Machine Learning. Appl. Sci. 2020, 10, 6214. [Google Scholar] [CrossRef]
- Kim, J.; Oh, J.E.; Lee, J.; Kim, M.J.; Hur, B.Y.; Sohn, D.K.; Lee, B. Rectal Cancer: Toward Fully Automatic Discrimination of T2 and T3 Rectal Cancers Using Deep Convolutional Neural Network. Int. J. Imaging Syst. Technol. 2019, 29, 247–259. [Google Scholar] [CrossRef]
- Ding, L.; Liu, G.W.; Zhao, B.C.; Zhou, Y.P.; Li, S.; Zhang, Z.D.; Guo, Y.T.; Li, A.Q.; Lu, Y.; Yao, H.W.; et al. Artificial Intelligence System of Faster Region-Based Convolutional Neural Network Surpassing Senior Radiologists in Evaluation of Metastatic Lymph Nodes of Rectal Cancer. Chin. Med. J. 2019, 132, 379–387. [Google Scholar] [CrossRef]
- Godkhindi, A.M.; Gowda, R.M. Automated Detection of Polyps in CT Colonography Images Using Deep Learning Algorithms in Colon Cancer Diagnosis. In Proceedings of the 2017 International Conference on Energy, Communication, Data Analytics and Soft Computing, ICECDS, Chennai, India, 1–2 August 2017; pp. 1722–1728. [Google Scholar] [CrossRef]
- Umehara, K.; Näppi, J.J.; Hironaka, T.; Regge, D.; Ishida, T.; Yoshida, H. Deep Ensemble Learning of Virtual Endoluminal Views for Polyp Detection in CT Colonography. Med. Imaging Comput.-Aided Diagn. 2017, 10134, 101340G. [Google Scholar] [CrossRef]
- Ştefănescu, D.; Streba, C.; Cârţână, E.T.; Săftoiu, A.; Gruionu, G.; Gruionu, L.G. Computer Aided Diagnosis for Confocal Laser Endomicroscopy in Advanced Colorectal Adenocarcinoma. PLoS ONE 2016, 11, e0154863. [Google Scholar] [CrossRef] [Green Version]
- Song, B.; Zhang, G.; Lu, H.; Wang, H.; Zhu, W.; Pickhardt, P.J.; Liang, Z. Volumetric Texture Features from Higher-Order Images for Diagnosis of Colon Lesions via CT Colonography. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 1021–1031. [Google Scholar] [CrossRef]
- Taylor, S.A.; Iinuma, G.; Saito, Y.; Zhang, J.; Halligan, S. CT Colonography: Computer-Aided Detection of Morphologically Flat T1 Colonic Carcinoma. Eur. Radiol. 2008, 18, 1666–1673. [Google Scholar] [CrossRef] [PubMed]
- Acs, B.; Rantalainen, M.; Hartman, J. Artificial Intelligence as the next Step towards Precision Pathology. J. Intern. Med. 2020, 288, 62–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, H.; Pan, Z.; Cen, Q.; Li, Y.; Chen, S. Multi-Scale Fully Convolutional Network for Gland Segmentation Using Three-Class Classification. Neurocomputing 2020, 380, 150–161. [Google Scholar] [CrossRef]
- Rathore, S.; Hussain, M.; Aksam Iftikhar, M.; Jalil, A. Novel Structural Descriptors for Automated Colon Cancer Detection and Grading. Comput. Methods Programs Biomed. 2015, 121, 92–108. [Google Scholar] [CrossRef]
- Takamatsu, M.; Yamamoto, N.; Kawachi, H.; Chino, A.; Saito, S.; Ueno, M.; Ishikawa, Y.; Takazawa, Y.; Takeuchi, K. Prediction of Early Colorectal Cancer Metastasis by Machine Learning Using Digital Slide Images. Comput. Methods Programs Biomed. 2019, 178, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Yun, L.; Guangwei, L. Application, Problems and Countermeasures of Artificial Intelligence in Colorectal Cancer. Chin. J. Pract. Surg. 2020, 40, 271–274. [Google Scholar] [CrossRef]
- Kim, D.H.; Pickhardt, P.J.; Taylor, A.J.; Leung, W.K.; Winter, T.C.; Hinshaw, J.L.; Gopal, D.V.; Reichelderfer, M.; Hsu, R.H.; Pfau, P.R. CT Colonography versus Colonoscopy for the Detection of Advanced Neoplasia. N. Engl. J. Med. 2007, 357, 1403–1412. [Google Scholar] [CrossRef] [Green Version]
- Khalili, K.; Lawlor, R.L.; Pourafkari, M.; Lu, H.; Tyrrell, P.; Kim, T.K.; Jang, H.J.; Johnson, S.A.; Martel, A.L. Convolutional Neural Networks versus Radiologists in Characterization of Small Hypoattenuating Hepatic Nodules on CT: A Critical Diagnostic Challenge in Staging of Colorectal Carcinoma. Sci. Rep. 2020, 10, 15248. [Google Scholar] [CrossRef]
- Lu, Y.; Yu, Q.; Gao, Y.; Zhou, Y.; Liu, G.; Dong, Q.; Ma, J.; Ding, L.; Yao, H.; Zhang, Z.; et al. Identification of Metastatic Lymph Nodes in MR Imaging with Faster Region-Based Convolutional Neural Networks. Cancer Res. 2018, 78, 5135–5143. [Google Scholar] [CrossRef] [Green Version]
- Wáng, Y.X.J.; Idée, J.M. A Comprehensive Literatures Update of Clinical Researches of Superparamagnetic Resonance Iron Oxide Nanoparticles for Magnetic Resonance Imaging. Quant. Imaging Med. Surg. 2017, 7, 88–122. [Google Scholar] [CrossRef] [Green Version]
- Badic, B.; Tixier, F.; Rest, C.C.L.; Hatt, M.; Visvikis, D. Radiogenomics in Colorectal Cancer. Cancers 2021, 13, 973. [Google Scholar] [CrossRef] [PubMed]
- Wei, B. Application of Artificial Intelligence Technology in Whole Course Management of Colorectal Cancer. J. Adv. Oxid. Technol. 2018, 21, 2017–2020. [Google Scholar] [CrossRef]
- Thakur, N.; Yoon, H.; Chong, Y. Current Trends of Artificial Intelligence for Colorectal Cancer Pathology Image Analysis: A Systematic Review. Cancers 2020, 12, 1884. [Google Scholar] [CrossRef]
- Yu, C.; Helwig, E.J. The Role of AI Technology in Prediction, Diagnosis and Treatment of Colorectal Cancer. Artif. Intell. Rev. 2021, 55, 323–343. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Hastie, T. Causal Interpretations of Black-Box Models. J. Bus. Econ. Stat. 2021, 39, 272–281. [Google Scholar] [CrossRef]
- Bondeven, P.; Laurberg, S.; Hagemann-Madsen, R.H.; Ginnerup Pedersen, B. Suboptimal Surgery and Omission of Neoadjuvant Therapy for Upper Rectal Cancer Is Associated with a High Risk of Local Recurrence. Colorectal Dis. 2015, 17, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.M.; Huang, M.Y.; Huang, C.W.; Tsai, H.L.; Su, W.C.; Chang, W.C.; Wang, J.Y.; Shi, H.Y. Machine Learning for Predicting Pathological Complete Response in Patients with Locally Advanced Rectal Cancer after Neoadjuvant Chemoradiotherapy. Sci. Rep. 2020, 10, 12555. [Google Scholar] [CrossRef]
- Tan, Y.; Fu, D.; Li, D.; Kong, X.; Jiang, K.; Chen, L.; Yuan, Y.; Ding, K. Predictors and Risk Factors of Pathologic Complete Response Following Neoadjuvant Chemoradiotherapy for Rectal Cancer: A Population-Based Analysis. Front. Oncol. 2019, 9, 497. [Google Scholar] [CrossRef]
- Shayesteh, S.P.; Alikhassi, A.; Fard Esfahani, A.; Miraie, M.; Geramifar, P.; Bitarafan-rajabi, A.; Haddad, P. Neo-Adjuvant Chemoradiotherapy Response Prediction Using MRI Based Ensemble Learning Method in Rectal Cancer Patients. Phys. Med. 2019, 62, 111–119. [Google Scholar] [CrossRef]
- Ferrari, R.; Mancini-Terracciano, C.; Voena, C.; Rengo, M.; Zerunian, M.; Ciardiello, A.; Grasso, S.; Mare, V.; Paramatti, R.; Russomando, A.; et al. MR-Based Artificial Intelligence Model to Assess Response to Therapy in Locally Advanced Rectal Cancer. Eur. J. Radiol. 2019, 118, 1–9. [Google Scholar] [CrossRef]
- Oyaga-Iriarte, E.; Insausti, A.; Sayar, O.; Aldaz, A. Prediction of Irinotecan Toxicity in Metastatic Colorectal Cancer Patients Based on Machine Learning Models with Pharmacokinetic Parameters. J. Pharmacol. Sci. 2019, 140, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Cruz, S.; Gomes, S.E.; Borralho, P.M.; Rodrigues, C.M.P.; Gaudêncio, S.P.; Pereira, F. In Silico HCT116 Human Colon Cancer Cell-Based Models En Route to the Discovery of Lead-like Anticancer Drugs. Biomolecules 2018, 8, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Ding, Z.; Qian, Y.; Shi, X.; Castranova, V.; Harner, E.J.; Guo, L. Predicting Cancer Drug Response by Proteomic Profiling. Clin. Cancer Res. 2006, 12, 4583–4589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elfiky, A.A.; Pany, M.J.; Parikh, R.B.; Obermeyer, Z. Development and Application of a Machine Learning Approach to Assess Short-Term Mortality Risk Among Patients With Cancer Starting Chemotherapy. JAMA Netw. Open 2018, 1, e180926. [Google Scholar] [CrossRef] [Green Version]
- Shi, L.; Zhang, Y.; Nie, K.; Sun, X.; Niu, T.; Yue, N.; Kwong, T.; Chang, P.; Chow, D.; Chen, J.H.; et al. Machine Learning for Prediction of Chemoradiation Therapy Response in Rectal Cancer Using Pre-Treatment and Mid-Radiation Multi-Parametric MRI. Magnetic Resonance Imaging 2019, 61, 33–40. [Google Scholar] [CrossRef]
- Takenaka, Y.; Miyoshi, N.; Fujino, S.; Takahashi, Y.; Nishimura, J.; Yasui, M.; Ide, Y.; Hirose, H.; Tokuoka, M.; Ohue, M. Development of a Novel Prediction Model for Recurrent Stage II Colon Cancer. Surg. Today 2020, 50, 389–395. [Google Scholar] [CrossRef]
- Xu, Y.; Ju, L.; Tong, J.; Zhou, C.M.; Yang, J.J. Machine Learning Algorithms for Predicting the Recurrence of Stage IV Colorectal Cancer After Tumor Resection. Sci. Rep. 2020, 10, 2519. [Google Scholar] [CrossRef]
- Li, H.; Boimel, P.; Janopaul-Naylor, J.; Zhong, H.; Xiao, Y.; Ben-Josef, E.; Fan, Y. Deep Convolutional Neural Networks for Imaging Data Based Survival Analysis of Rectal Cancer. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019; pp. 846–849. [Google Scholar]
- Joensuu, H.; Vehtari, A.; Riihimäki, J.; Nishida, T.; Steigen, S.E.; Brabec, P.; Plank, L.; Nilsson, B.; Cirilli, C.; Braconi, C.; et al. Risk of Recurrence of Gastrointestinal Stromal Tumour after Surgery: An Analysis of Pooled Population-Based Cohorts. Lancet Oncol. 2012, 13, 265–274. [Google Scholar] [CrossRef]
- Weiser, M.R.; Landmann, R.G.; Kattan, M.W.; Gonen, M.; Shia, J.; Chou, J.; Paty, P.B.; Guillem, J.G.; Temple, L.K.; Schrag, D.; et al. Individualized Prediction of Colon Cancer Recurrence Using a Nomogram. J. Clin. Oncol. 2008, 26, 380–385. [Google Scholar] [CrossRef]
- Hossain, M.J.; Chowdhury, U.N.; Islam, M.B.; Uddin, S.; Ahmed, M.B.; Quinn, J.M.W.; Moni, M.A. Machine Learning and Network-Based Models to Identify Genetic Risk Factors to the Progression and Survival of Colorectal Cancer. Comput. Biol. Med. 2021, 135, 104539. [Google Scholar] [CrossRef]
- Jiang, D.; Liao, J.; Duan, H.; Wu, Q.; Owen, G.; Shu, C.; Chen, L.; He, Y.; Wu, Z.; He, D.; et al. A Machine Learning-Based Prognostic Predictor for Stage III Colon Cancer. Sci. Rep. 2020, 10, 10333. [Google Scholar] [CrossRef] [PubMed]
- Skrede, O.J.; De Raedt, S.; Kleppe, A.; Hveem, T.S.; Liestøl, K.; Maddison, J.; Askautrud, H.A.; Pradhan, M.; Nesheim, J.A.; Albregtsen, F.; et al. Deep Learning for Prediction of Colorectal Cancer Outcome: A Discovery and Validation Study. Lancet 2020, 395, 350–360. [Google Scholar] [CrossRef]
- Kather, J.N.; Krisam, J.; Charoentong, P.; Luedde, T.; Herpel, E.; Weis, C.A.; Gaiser, T.; Marx, A.; Valous, N.A.; Ferber, D.; et al. Predicting Survival from Colorectal Cancer Histology Slides Using Deep Learning: A Retrospective Multicenter Study. PLoS Med. 2019, 16, e1002730. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, D.; Ye, X.; Wang, Y.; Yin, Y.; Jin, Y. A Tree Ensemble-Based Two-Stage Model for Advanced-Stage Colorectal Cancer Survival Prediction. Inf. Sci. 2019, 474, 106–124. [Google Scholar] [CrossRef]
- Yue, X.; Dimitriou, N.; Caie, P.D.; Harrison, D.J.; Arandjelović, O. Colorectal Cancer Outcome Prediction from H&E Whole Slide Images Using Machine Learning and Automatically Inferred Phenotype Profiles. In Proceedings of the Proceedings of 11th International Conference on Bioinformatics and Computational Biology, Honolulu, HI, USA, 18–20 March 2019. [Google Scholar]
- Wang, Y.H.; Nguyen, P.A.; Mohaimenul Islam, M.; Li, Y.C.; Yang, H.C. Development of Deep Learning Algorithm for Detection of Colorectal Cancer in EHR Data. Stud. Health Technol. Inform. 2019, 264, 438–441. [Google Scholar] [CrossRef]
- Gupta, P.; Chiang, S.; Sahoo, P.K.; Mohapatra, S.K.; You, J.-F.; Onthoni, D.D.; Hung, H.-Y.; Chiang, J.-M.; Huang, Y.; Tsai, W.-S. Prediction of Colon Cancer Stages and Survival Period with Machine Learning Approach. Cancers 2019, 11, 2007. [Google Scholar] [CrossRef] [Green Version]
- Al-Bahrani, R.; Agrawal, A.; Choudhary, A. Survivability Prediction of Colon Cancer Patients Using Neural Networks. Health Inform. J. 2019, 25, 878–891. [Google Scholar] [CrossRef]
- Bychkov, D.; Linder, N.; Turkki, R.; Nordling, S.; Kovanen, P.E.; Verrill, C.; Walliander, M.; Lundin, M.; Haglund, C.; Lundin, J. Deep Learning Based Tissue Analysis Predicts Outcome in Colorectal Cancer. Sci. Rep. 2018, 8, 3395. [Google Scholar] [CrossRef]
- Pourhoseingholi, M.A.; Kheirian, S.; Zali, M.R. Comparison of Basic and Ensemble Data Mining Methods in Predicting 5-Year Survival of Colorectal Cancer Patients. Acta Inform. Med. 2017, 25, 254–258. [Google Scholar] [CrossRef] [Green Version]
- Sailer, F.; Pobiruchin, M.; Bochum, S.; Martens, U.M.; Schramm, W. Prediction of 5-Year Survival with Data Mining Algorithms. Stud. Health Technol. Inform. 2015, 213, 75–78. [Google Scholar] [CrossRef]
- Tai, Y.H.; Chang, W.K.; Wu, H.L.; Chan, M.Y.; Chen, H.H.; Chang, K.Y. The Effect of Epidural Analgesia on Cancer Progression in Patients with Stage IV Colorectal Cancer after Primary Tumor Resection: A Retrospective Cohort Study. PLoS ONE 2018, 13, e0200893. [Google Scholar] [CrossRef] [Green Version]
- Keyang, C.; Ning, W.; Wenxi, S.; Yongzhao, Z. Research Advances in the Interpretability of Deep Learning. J. Comput. Res. Dev. 2020, 57, 1208–1217. [Google Scholar] [CrossRef]
- Li, J.; Tian, Y.; Zhu, Y.; Zhou, T.; Li, J.; Ding, K.; Li, J. A Multicenter Random Forest Model for Effective Prognosis Prediction in Collaborative Clinical Research Network. Artif. Intell. Med. 2020, 103, 101814. [Google Scholar] [CrossRef] [PubMed]
- Hueman, M.; Wang, H.; Henson, D.; Chen, D. Expanding the TNM for Cancers of the Colon and Rectum Using Machine Learning: A Demonstration. ESMO Open 2019, 4, e000518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spanheimer, P.M.; Armstrong, J.G.; Fu, S.; Liao, J.; Regenbogen, S.E.; Byrn, J.C. Robotic Proctectomy for Rectal Cancer: Analysis of 71 Patients from a Single Institution. Int. J. Med. Robot. Comput. Assist. Surg. 2017, 13, e1841. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Topic | Task | Dataset | Model | Performance | Year | Ref. |
|---|---|---|---|---|---|---|
| CRC Screening | High-risk patient detection | 111 patients’ microarray data including 22,278 features | LightGBM, DNN | Accuracy: 100% | 2021 | [16] |
| Polyp classification | 47,555 endoscopy images for 24 patients | SSD | Accuracy: 0.9067, precision: 0.9744, recall: 0.9067, F1: 0.9393 | 2021 | [17] | |
| Serum biomarker detection | 186 blood serum samples (39 advanced adenomas, 90 CRC and 57 healthy controls) | RF, Random Tree, LMT, SVM | Accuracy: 75% | 2021 | [18] | |
| Serum biomarker detection | 263 blood serum protein samples (213 individuals undergoing screening endoscopy and 50 non-metastatic CRC) | LR, SVM, Gaussian NB, DT, RF, and extremely randomized trees | AUC: 0.75, Sensitivity: 70%, Specificity: 89% | 2020 | [19] | |
| Polyp detection and classification | 27,508 endoscopy images | CNN | Detection: Sensitivity—0.92, PPV—0.86; Classification: Sensitivity—0.83, PPV—0.81 | 2020 | [20] | |
| Polyp localization | EAD2019, CVC-ClinicDB, ETIS-Larib, in-house dataset, Kvasir-SEG | RetinaNet | Precision: 0.537 | 2020 | [21] | |
| Polyp detection | CVC-CLINIC, ASU-Mayo Clinic, CVC-ClinicVideoDB | Faster R-CNN, SSD | Sensitivity: 0.9086, precision: 0.8154, F1: 0.8595 | 2020 | [22] | |
| Polyp detection and classification | 871 endoscopy images from218 patients | ResNet50, RetinaNet | F1: 0.6872, F2: 0.6607 | 2019 | [23] | |
| Polyp detection | 8641 endoscopy images | CNN | Sensitivity: 90.0%, Specificity: 63.3, Accuracy: 76.5% | 2018 | [24] | |
| Polyp segmentation | CVC-ColonDB | CNN | Specificity: 74.8%, Sensitivity: 99.3%, Accuracy: 97.7% | 2018 | [25] | |
| High-risk patient prediction | Colon cancer screening center data (EMRs) | Colonflag | The odds of Colonflag and normal colonoscopies: 2.0 | 2018 | [26] | |
| Polyp classification | 1930 NBI images | CNN | Accuracy: 85.9%, Precision: 87.3%, Recall rate: 87.6% | 2017 | [27] | |
| High-risk patient detection | 112,584,133 US community-based insured data | Colonflag | AUC: 0.80 ± 0.01 | 2017 | [28] | |
| High-risk patient detection | 17,095 patients from KPNW (EMRs) | Mescore | Top 3% score > 97.02 Top 1% score > 99.38 | 2017 | [29] | |
| Polyp detection | 24 endoscopy videos | Energy map | AUC: 0.79, Sensitivity: 70.4%, Specificity: 72.4% | 2016 | [30] | |
| High-risk patient detection | 606,403 Israelis and 25,613 UK dataset (EMRs) | Mescore | AUC: 0.82 ± 0.01 and 0.81 for validation sets | 2016 | [31] | |
| Polyp classification | 1890 NBI endoscopic images | HuPAS version 3.1 | Accuracy: 98.7% | 2012 | [32] |
| Topic | Task | Dataset | Model | Performance | Year | Ref. |
|---|---|---|---|---|---|---|
| Pathological diagnosis | Tumor mutational burden-high prediction | 278 HE slides | CNN | AUC: 0.934 | 2021 | [41] |
| Low/high-grade classification | Immunohistochemically stained biopsy of 67 patients | hDL-system (VGG16, SVM) | hDL-system accuracy: 99.1%; sML-system accuracy: 92.5% | 2021 | [42] | |
| NL/AD/ADC classification | 4036 WSI | CNN, RNN | AUC: 0.96 for ADC; 0.99 for AD | 2020 | [43] | |
| Tumor immune microenvironment analysis | 404 CRC and 20 adjacent non-tumorous tissues | CIBERSORT | C-index: stage I-II 0.69; stage III-IV 0.71; AUC: 0.67 | 2019 | [44] | |
| NL/Tumor classification | 94 WSI, 370 TCGA-KR, 378 TCGA-DX | ResNet18 | AUC > 0.99 | 2019 | [45] | |
| NL/HP/AD/ADC classification | 393 WSI (12,565 patches) | CNN | Accuracy: 80% | 2019 | [46] | |
| NL/Tumor classification | 57 WSI (10,280 patches) | VGG | Accuracy: 93.5%, Sensitivity: 95.1% | 2018 | [47] | |
| NL/AD/ADC classification | 27 WSI (13,500 patches) | VGG16 | Accuracy: 96%, Specificity: 92.8% | 2018 | [48] | |
| NL/AD/ADC classification | 30 multispectral image patches | CNN | Accuracy: 99.2% | 2017 | [49] | |
| Cancer subtypes classification | 717 patches | AlexNet | Accuracy: 97.5% | 2017 | [50] | |
| Polyp subtypes classification | 2074 patches 936 WSI | ResNet | Accuracy: 93.0% | 2017 | [51] | |
| Radiological diagnosis | Metastatic CRC prediction | MRI from 55 stage VI patients with known hepatic metastasis | RF | AUC: 0.94 (Add imaging-based heterogeneity features) | 2021 | [52] |
| Metastatic lymph node prediction | PET-CT scan images from 199 CRC patients | LR, SVM, RF, NN, and XGBoost | AUC of LR: 0.866; AUC of XGBoost: 0.903 | 2021 | [53] | |
| Colorectal liver metastasis prediction | 103 metastasis samples and 80 non-cancer tissues | Probe electrospray ionization-mass spectrometry, and LR | Accuracy: 99.5%, AUC: 0.9999 | 2021 | [54] | |
| Colorectal liver metastasis prediction | CT scan images from 91 patients | Bayesian-optimized RF with wrapper feature selection | AUC of radiomics features model: 86%; AUC of clinical features model: 71%; AUC of combination: 86% | 2021 | [55] | |
| KRAS mutations detection | CT scan images from 47 patients | Haralick texture analysis, SVM, LightGBM, NN, and RF | Accuracy: 83%, kappa: 64.7% | 2020 | [56] | |
| Classification of T2 and T3 | 290 MRI images from 133 patients | CNN | Accuracy: 0.94 | 2019 | [57] | |
| Metastatic lymph node prediction | MRI images from 414 patients | Faster R-CNN | r-radiologist-Faster R-CNN 0.912 | 2019 | [58] | |
| Polyp detection | 825 CT scan images | CNN | Accuracy: 0.87, Sensitivity: 0.8877, Specificity: 0.8735 | 2017 | [59] | |
| Polyp detection | 154 CT scan images | CNN | Accuracy: 0.971 | 2017 | [60] | |
| Polyp classification | 1035 endomicroscopy images | Mathworks “NAVICAD” system | Accuracy: 84.5% | 2016 | [61] | |
| Polyp detection and classification | 148 CT scan images | Haralick texture analysis, SVM | ROC: 0.85 | 2014 | [62] | |
| CAD system for polyp detection | 24 T1 stage patients’ CT scan images | Coloncad API 4.0, Medicsight plc | True positives rate >96.1% | 2008 | [63] |
| Topic | Task | Dataset | Model | Performance | Year | Ref. |
|---|---|---|---|---|---|---|
| nCRT | nCRT response prediction | Medical records from 282 patients (248 training and 34 validation) | ANN, KNN, SVM, NBC, MLR | ANN model outperformed others: Accuracy: 0.88, AUC: 0.84, Sensitivity: 0.94 | 2020 | [79] |
| nCRT response prediction | 6555 patients’ records from the SEER | LR | 3-year OS rate: 92.4% with pCR; 88.2% without pCR | 2019 | [80] | |
| nCRT response prediction | 98 patients MRI (53 training set and 45 validation set) | SVM, NN, BN, KNN | Test: AUC: 97.8%, Accuracy: 92.8%, Validation: AUC: 95%, Accuracy: 90% | 2019 | [81] | |
| nCRT response prediction | 55 patients MRI | RF | Mean AUC: 0.83 | 2019 | [82] | |
| Chemotherapy | The toxicity of CPT-11 prediction | Demographic data, liver function bloody tests and tumor markers from 20 advanced CRC patients | SVM | Accuracy: 91% for diarrhea, 76% for leukopenia, and 75% for neutropenia | 2019 | [83] |
| Drug IC50 detection | 18,850 organic compounds | KNN, RF, SVM | Accuracy: over 63% | 2018 | [84] |
| Topic | Task | Dataset | Model | Performance | Year | Ref. |
|---|---|---|---|---|---|---|
| Recurrence | Recurrence perdition of stage II CRC | Clinicopathological data of 350 patients after curative resection for stage II CRC | Nomogram | C-index: 0.585 in the validation set | 2020 | [88] |
| Recurrence prediction of Stage IV CRC after tumor resection | EHR data from 999 patients of stage IV CRC | LR, DT, GB and LightGBM | LightGBM: AUC: 0.761 | 2020 | [89] | |
| Recurrence prediction of local tumor | PET-CT images from 84 patients | CNN, Proportional hazards model | C-index: 0.64 | 2019 | [90] | |
| Risk prediction of recurrence of gastrointestinal stromal tumor | Clinical data of 2560 patients | Proportional hazards, Non-linear model | AUC: 0.88 | 2012 | [91] | |
| Recurrence perdition after surgery | Clinicopathological data of 1320 nonmetastatic CRC patients | NomogramCOX regression | C-index: 0.77 | 2008 | [92] | |
| Survival | Genetic risk factors Identification | National Center for Biotechnology Information Gene Expression Omnibus | GSEA, PPI network, Cox Proportional Hazard regression | 4 sub-networks and 8 hub genes as potential therapeutic targets | 2021 | [93] |
| Prognostic prediction for stage III CRC | Clinicopathological data of 215 patients | CNN, GB | HR: 8.976 and 10.273 | 2020 | [94] | |
| Outcome prediction | 12,000,000 HE images | CNN | HR: 3.84 and 3.04 with established prognostic markers | 2020 | [95] | |
| Survival prediction | 7180 HE images of 25 patients | CNN | Nine-class accuracy: >94% | 2019 | [96] | |
| Survival prediction | PET-CT images of 84 patients | CNN, proportional hazards model | C-index: 0.64 | 2019 | [90] | |
| Outcome prediction, and remaining lifespan prediction | SEER | tree-based ensemble model | Accuracy: 0.7069, Sensitivity: 0.8452, Specificity: 0.66 | 2019 | [97] | |
| Outcome prediction | 75 WSIs from stage I and II CRC patients with surgical resection | CNN | F1: 0.67 | 2019 | [98] | |
| Outcome prediction | EHR data of 58,152 patients | CNN | AUC: 0.922, Sensitivity: 0.837, specificity: 0.867, PPV: 0.532 | 2019 | [99] | |
| Prediction of Stages and Survival Period | Clinicopathological data of 4021 patients | RF, SVM, LR, MLP, KNN, and AdaBoost | RF: F-measure: 0.89, Accuracy: 84%, AUC: 0.82 ± 0.10 | 2019 | [100] | |
| 1/2/5 years Survival prediction | SEER data | DNN | AUC: 0.87 | 2019 | [101] | |
| Outcome prediction | Digitized HE tumor tissue microarray samples of 420 patients | CNN, LSTM | LSTM: AUC: 0.69, histological grade AUC: 0.57, the visual risk score AUC: 0.58 | 2018 | [102] | |
| 5-year survival prediction | EHR data of 1127 CRC patients | Ensemble (bagging and voting) classifier | Ensemble voting model AUC: 0.96 | 2017 | [103] | |
| 5-year survival prediction | EHR data of 334,583 cases from Robert Koch Institute | SVM, LR, NB, DT, KNN, LR, NN, RF | Average accuracy of the clinicians: 59%, ML: 67.7% | 2015 | [104] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, H.; Ding, S.; Liu, J.; Wang, L.; Wang, X. Applications of Artificial Intelligence in Screening, Diagnosis, Treatment, and Prognosis of Colorectal Cancer. Curr. Oncol. 2022, 29, 1773-1795. https://doi.org/10.3390/curroncol29030146
Qiu H, Ding S, Liu J, Wang L, Wang X. Applications of Artificial Intelligence in Screening, Diagnosis, Treatment, and Prognosis of Colorectal Cancer. Current Oncology. 2022; 29(3):1773-1795. https://doi.org/10.3390/curroncol29030146
Chicago/Turabian StyleQiu, Hang, Shuhan Ding, Jianbo Liu, Liya Wang, and Xiaodong Wang. 2022. "Applications of Artificial Intelligence in Screening, Diagnosis, Treatment, and Prognosis of Colorectal Cancer" Current Oncology 29, no. 3: 1773-1795. https://doi.org/10.3390/curroncol29030146
APA StyleQiu, H., Ding, S., Liu, J., Wang, L., & Wang, X. (2022). Applications of Artificial Intelligence in Screening, Diagnosis, Treatment, and Prognosis of Colorectal Cancer. Current Oncology, 29(3), 1773-1795. https://doi.org/10.3390/curroncol29030146