Comprehensive Laboratory Diagnostic Workup for Patients with Suspected Intraocular Lymphoma including Flow Cytometry, Molecular Genetics and Cytopathology

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Cytopathology
2.3. Flow Cytometry
2.4. Molecular Genetics
2.5. Imaging
3. Results
3.1. Patient Characteristics
3.2. Diagnostic Power of Cytopathology, Flow Cytometry, and ddPCR/PCR in Vitreous Samples
3.2.1. Patients with Intraocular Lymphoma
Cytopathology
Flow Cytometry
ddPCR/PCR
3.2.2. Patients without Evidence of Intraocular Lymphoma
Cytopathology
Flow Cytometry
Correlation of Cytopathology and Flow Cytometry in Vitreous Samples
Diagnostic Value of Imaging in Patients of the Study
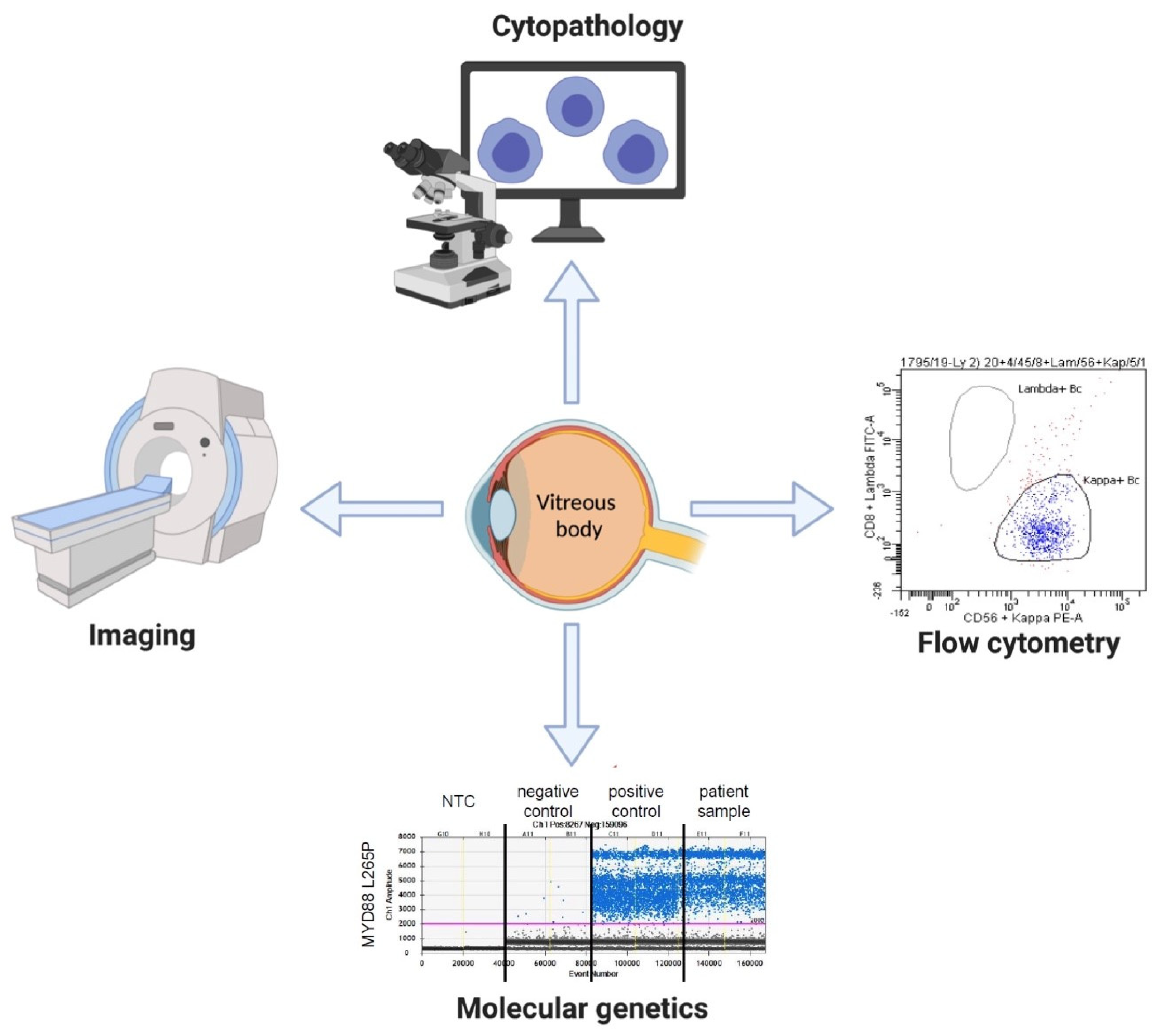
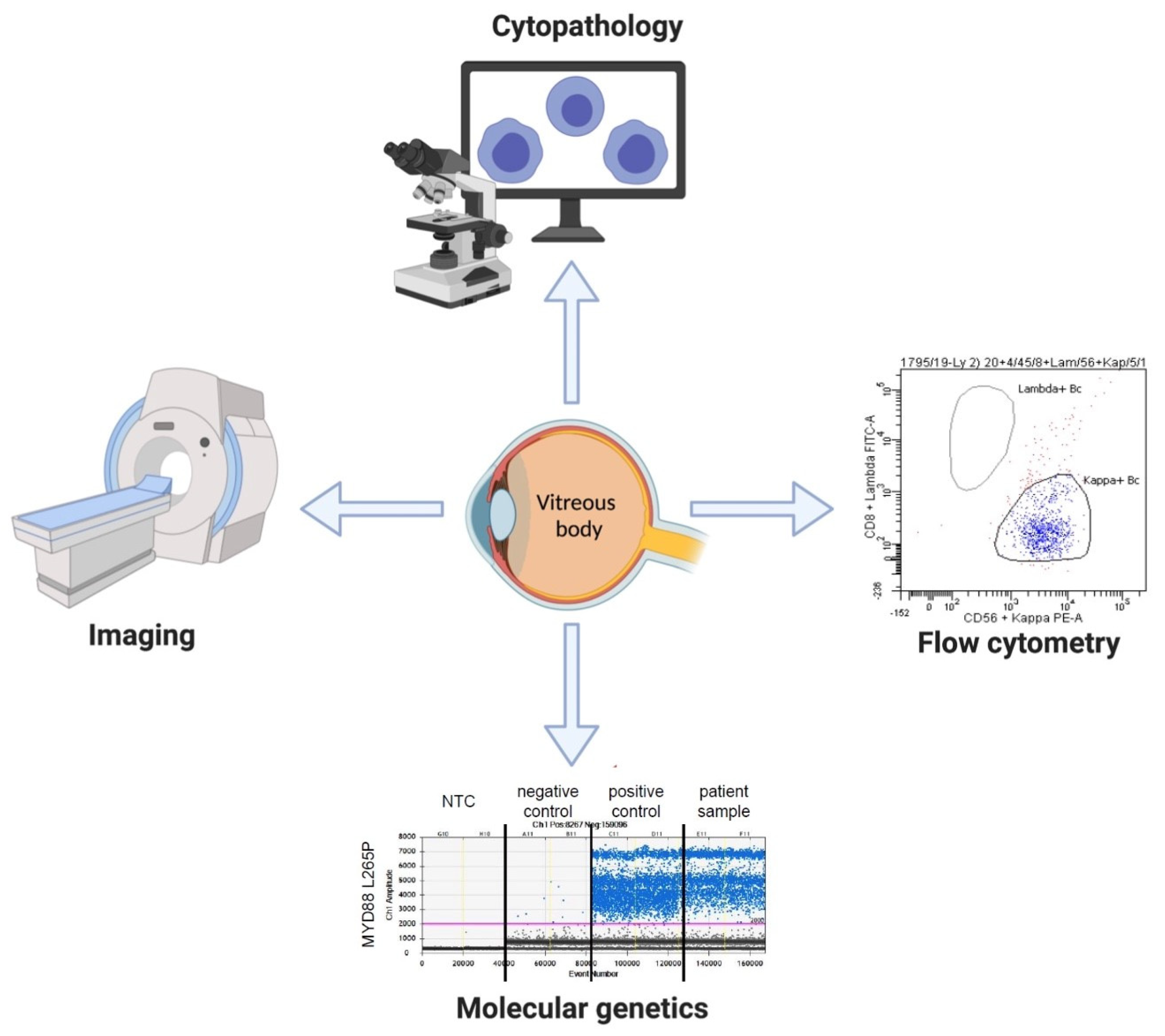
Combination of Cytopathology, Flow Cytometry, Molecular Genetics and Imaging for Diagnostics of IOL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freeman, L.N.; Schachat, A.P.; Knox, D.L.; Michels, R.G.; Green, W.R. Clinical features, laboratory investigations, and survival in ocular reticulum cell sarcoma. Ophthalmology 1987, 94, 1631–1639. [Google Scholar] [CrossRef]
- Reddy, E.K.; Bhatia, P.; Evans, R.G. Primary orbital lymphomas. Int. J. Radiat. Oncol. Biol. Phys. 1988, 15, 1239–1241. [Google Scholar] [CrossRef]
- Hochberg, F.H.; Miller, D.C. Primary central nervous system lymphoma. J. Neurosurg. 1988, 68, 835–853. [Google Scholar] [CrossRef] [PubMed]
- Grimm, S.A.; McCannel, C.A.; Omuro, A.M.P.; Ferreri, A.J.M.; Blay, J.-Y.; Neuwelt, E.A.; Siegal, T.; Batchelor, T.; Jahnke, K.; Shenkier, T.N.; et al. Primary cns lymphoma with intraocular involvement. Int. PCNSL Collab. Group Rep. 2008, 71, 1355–1360. [Google Scholar]
- Farrall, A.L.; Smith, J.R. Eye involvement in primary central nervous system lymphoma. Surv. Ophthalmol. 2020, 65, 548–561. [Google Scholar] [CrossRef] [PubMed]
- Karakawa, A.; Taoka, K.; Kaburaki, T.; Tanaka, R.; Shinozaki-Ushiku, A.; Hayashi, H.; Miyagi-Maeshima, A.; Nishimura, Y.; Uekusa, T.; Kojima, Y.; et al. Clinical features and outcomes of secondary intraocular lymphoma. Br. J. Haematol. 2018, 183, 668–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soussain, C.; Malaise, D. Primary vitreoretinal lymphoma: A diagnostic and management challenge. Blood 2021, 138, 1519–1534. [Google Scholar] [CrossRef]
- Cunningham, E.T.; Miserocchi, E.; Smith, J.R.; Gonzales, J.A.; Zierhut, M. Intraocular Lymphoma. Ocul. Immunol. Inflamm. 2021, 29, 425–429. [Google Scholar] [CrossRef]
- Tang, L.-J.; Gu, C.-L.; Zhang, P. Intraocular lymphoma. Int. J. Ophthalmol. 2017, 10, 1301–1307. [Google Scholar]
- AlQahtani, A.; Touitou, V.; Cassoux, N.; Aknin, C.; Merle-Beral, H.; Bodaghi, B.; LeHoang, P. More than a masquerade syndrome: Atypical presentations of vitreoretinal lymphomas. Ocul. Immunol. Inflamm. 2014, 22, 189–196. [Google Scholar] [CrossRef]
- Fend, F.; Ferreri, A.J.M.; Coupland, S.E. How we diagnose and treat vitreoretinal lymphoma. Br. J. Haematol. 2016, 173, 680–692. [Google Scholar] [CrossRef] [PubMed]
- Coupland, S.E.; Anastassiou, G.; Bornfeld, N.; Hummel, M.; Stein, H. Primary intraocular lymphoma of t-cell type: Report of a case and review of the literature. Graefe’s Arch. Clin. Exp. Ophthalmol. 2005, 243, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.-C.; Rubenstein, J.L.; Coupland, S.E.; Davis, J.L.; Harbour, J.W.; Johnston, P.B.; Cassoux, N.; Touitou, V.; Smith, J.R.; Batchelor, T.T.; et al. Primary vitreoretinal lymphoma: A report from an international primary central nervous system lymphoma collaborative group symposium. Oncologist 2011, 16, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- Coupland, S.E.; Bechrakis, N.E.; Anastassiou, G.; Foerster, A.M.H.; Heiligenhaus, A.; Pleyer, U.; Hummel, M.; Stein, H. Evaluation of vitrectomy specimens and chorioretinal biopsies in the diagnosis of primary intraocular lymphoma in patients with masquerade syndrome. Graefe’s Arch. Clin. Exp. Ophthalmol. 2003, 241, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Raja, H.; Salomão, D.R.; Viswanatha, D.S.; Pulido, J.S. Prevalence of Myd88 l265p mutation in histologically proven, diffuse large b-cell vitreoretinal lymphoma. Retina 2016, 36, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Bonzheim, I.; Giese, S.; Deuter, C.; Süsskind, D.; Zierhut, M.; Waizel, M.; Szurman, P.; Federmann, B.; Schmidt, J.; Quintanilla-Martinez, L.; et al. High frequency of Myd88 mutations in vitreoretinal b-cell lymphoma: A valuable tool to improve diagnostic yield of vitreous aspirates. Blood 2015, 126, 76–79. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Zhou, X.; Chen, B.; Xiao, J.; Li, Y.; Zhou, X.; Zhou, Q.; Chen, K.; Wang, Q. Clinical relevance of the high prevalence of Myd88 l265p mutated vitreoretinal lymphoma identified by droplet digital polymerase chain reaction. Ocul. Immunol. Inflamm. 2021, 29, 448–455. [Google Scholar] [CrossRef]
- Davis, J.L.; Viciana, A.L.; Ruiz, P. Diagnosis of intraocular lymphoma by flow cytometry. Am. J. Ophthalmol. 1997, 124, 362–372. [Google Scholar] [CrossRef]
- Kase, S.; Namba, K.; Iwata, D.; Mizuuchi, K.; Kitaichi, N.; Tagawa, Y.; Okada-Kanno, H.; Matsuno, Y.; Ishida, S. Diagnostic efficacy of cell block method for vitreoretinal lymphoma. Diagn. Pathol. 2016, 11, 29. [Google Scholar] [CrossRef] [Green Version]
- Flores-Montero, J.; Grigore, G.; Fluxá, R.; Hernández, J.; Fernandez, P.; Almeida, J.; Muñoz, N.; Böttcher, S.; Sedek, L.; van der Velden, V.; et al. Euroflow lymphoid screening tube (lst) data base for automated identification of blood lymphocyte subsets. J. Immunol. Methods 2019, 475, 112662. [Google Scholar] [CrossRef]
- Tanaka, R.; Kaburaki, T.; Taoka, K.; Karakawa, A.; Tsuji, H.; Nishikawa, M.; Yatomi, Y.; Shinozaki-Ushiku, A.; Ushiku, T.; Araki, F. More accurate diagnosis of vitreoretinal lymphoma using a combination of diagnostic test results: A prospective observational study. Ocul. Immunol. Inflamm. 2021, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cantu, C.A.; Green, C.L.; Cummings, T.J.; Liu, B.; Dash, R.C. Flow cytometry immunophenotyping of vitreous specimens does not contribute to diagnosis of lymphoma without supporting morphologic features. Diagn. Cytopathol. 2019, 47, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Raparia, K.; Chang, C.C.; Chévez-Barrios, P. Intraocular lymphoma: Diagnostic approach and immunophenotypic findings in vitrectomy specimens. Arch. Pathol. Lab. Med. 2009, 133, 1233–1237. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patient No | Age/ Gender | History of Lymphoma/Other Conditions | Clinical, Instrumental and Histopathology Findings Accompanying Vitrectomy | Investigation of Vitreous Body | Final Diagnosis | Treatment/Clinical Course |
|---|---|---|---|---|---|---|
| Lymphoma patients | ||||||
| #1 | 88 yrs, female | Behçet’s disease | granulomatous uveitis; MRI: no signs of intracerebral tumor; CT: no lymphadenopathy; pathology (BM): no lymphoma; | flow cytometry: CD5 neg. monoclonal B-cell population (92% of all cells); cytopathology: no evidence of lymphoma cells; ddPCR: mutated MYD88 (p.L265P) (50.5%) | isolated intraocular B-cell lymphoma | corticosteroid pulse therapy; last FU (1 mo): death from sepsis |
| #2 | 67 yrs, male | No | bilateral visual impairment; MRI: perivascular lesions periventricular; CT: no lymphadenopathy; pathology (BM): no lymphoma | flow cytometry: CD5/CD10 neg. monoclonal B-cell population (51% of all cells); cytopathology: infiltrates of CD5/CD10 neg. B-cell neoplasm; PCR: clonal IGH-gene rearrangement ddPCR: mutated MYD88 (p.L265P) (49%) | primary B-cell CNS lymphoma with intra-ocular lymphoma | MATRIX x2 with PR; last FU (5 mo): death from sepsis in aplasia |
| #3 | 63 yrs, female | No | intermediate uveitis bilaterally; MRI: no signs of intracerebral tumor; PET/CT: no lymphadenopathy; CSF: inconspicuous | flow cytometry: CD5/CD10 neg. monoclonal B-cell population (33% of all cells); cytopathology: single atypical blastic lymphoid cells; laboratory chemistry: increased IL-10/IL ratio (34.2) | isolated B-cell intraocular lymphoma | radiotherapy of both eyes; last FU (7 mo): alive (in remission) |
| #4 | 53 yrs, male | epilepsy for years | progressive bilateral loss of vision; MRI: confluent bilateral medullary lesions; CT: no lymphadenopathy; CSF: inconspicuous | flow cytometry: CD5 neg. monoclonal B-cell population (45% of all cells); cytopathology: no evidence of lymphoma cells; ddPCR: mutated MYD88 (p.L265P) pathology (brain): DLBCL, mutated MYD88 (p.L265P) | primary CNS lymphoma (DLBCL) with intraocular lymphoma | MATRIX x4 followed by front-line HDCT/ASCT; last FU (13 mo): alive (in remission) |
| #5 | 80 yrs, male | DLBCL, IVb followed by R-CHOP x6 with PR | progressive loss of vision, nystagmus, headache, ataxia, oculomotor palsy both-sided; ophthalmological consultation: suspected intraocular lymphoma;
| flow cytometry: acellular punctate cytopathology: numerous macrophages and reactive T lymphocytes, no lymphoma cells | secondary CNS lymphoma following progress of DLBCL; no evidence of intraocular lymphoma | MTX x2 with stable disease; last FU (4 mo): death, non-cancer cause |
| Non-lymphoma patients | ||||||
| #6 | 58 yrs, female | sarcoidosis-like disease with chronic alveolitis, arthritis and keratouveitis | dyspnea, decreased visual acuity in right eye; PET/CT: inflammatory bilateral pulmonary changes, no lymphadenopathy; histopathology (lung): unclassifiable interstitial pneumonia | flow cytometry: relative increase in NK cells, lack of B cells, T-cells 2% of all cells | no findings of intraocular lymphoma | long-term steroids; last FU (24 mo): alive, progressive pulmonary hypertension |
| #7 | 65 yrs, female | prurigo subacute; unspecific medullary lesions in MRI | recurrent bilateral uveitis with no response on MTX/steroids; CT: no lymphadenopathy | flow cytometry: relative increase in T-cells with increased CD4/CD8 ratio, no B-cells | no findings of intraocular lymphoma | last FU (4 mo): alive |
| Patient No | Flow Cytometry (FC) | Cytopathology (CP) | Interpretation of Results | Final Diagnosis |
|---|---|---|---|---|
| Lymphoma patients | ||||
| #1 | lymphocytes 92%, B-cells 84%, T-cells 3%, NK-cells 1% (of all evaluable cell events); B-cells: CD19+, CD20+, CD5-, CD10-, CD38+, CD79b+, CD81+, CD95+, CD200+, FMC7+, HLA-DR-, skappa+ | macroscopic: colorless, clear liquid; microscopic: few normal lymphocytes and macrophages | discordance: lymphoma evidence by FC; lack of lymphoma evidence by CP | isolated intraocular B-cell lymphoma |
| #2 | lymphocytes 87%, B-cells 51%, T-cells 12%, NK-cells 12%; B-cells: CD19+, CD20+, CD5-, CD10-, CD11c+, CD23+, CD25+, CD38+, CD79b+, CD81+, CD95+, CD200+, FMC7+, HLA-DR+, slambda+ | macroscopic: colorless clear liquid; microscopic: small to medium-sized lymphoid infiltrate | concordance: lymphoma evidence by FC and CP | primary B-cell CNS lymphoma with intraocular lymphoma |
| #3 | lymphocytes 66%, B-cells 35%, T-cells 14%, NK-cells 17%; B-cells: CD19+, CD20+, CD5-, CD10-, CD38-, CD200+, HLA-DR+, skappa+ | macroscopic: colorless clear liquid; microscopic: atypical blast-like lymphoid cells | concordance: lymphoma evidence by FC and CP | isolated B-cell intraocular lymphoma |
| #4 | lymphocytes 36%, B-cells 30%, T-cells 1%, NK-cells 5%; B-cells: CD19+, CD20+, CD5-, CD38+, ckappa+ | macroscopic: colorless clear liquid; microscopic: no conspicuous lymphocytes | discordance: lymphoma evidence by FC; lack of lymphoma evidence by CP | primary CNS lymphoma (DLBCL) with intraocular lymphoma |
| #5 | acellular punctate | macroscopic: slightly yellow and turbid liquid microscopic: some inconspicuous lymphocytes, a few hyalocytes and erythrocytes | concordance: acellular vitrous body, i.e. no lymphocytes, according to FC; no evidence of ocular manifestation of DLBCL with CNS involvement according to CP | secondary CNS lymphoma following progress of DLBCL; no findings of intraocular lymphoma according to CP and FC |
| Exclusion of intraocular lymphoma | ||||
| #6 | lymphocytes 5%, B-cells <1%, T-cells 2%, NK-cells 2%; no aberrant immunophenotype | NA | no evidence of intraocular lymphoma by FC; CP not performed | no findings of intraocular lymphoma |
| #7 | lymphocytes 71%, B-cells <1%, T-cells 49%, NK-cells 20%; no aberrant immunophenotype | NA | no evidence of intraocular lymphoma by FC; CP not performed | no findings of intraocular lymphoma |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shumilov, E.; Mazzeo, P.; Zinkernagel, M.S.; Legros, M.; Porret, N.; Romagna, L.; Haase, D.; Lenz, G.; Novak, U.; Banz, Y.; et al. Comprehensive Laboratory Diagnostic Workup for Patients with Suspected Intraocular Lymphoma including Flow Cytometry, Molecular Genetics and Cytopathology. Curr. Oncol. 2022, 29, 766-776. https://doi.org/10.3390/curroncol29020065
Shumilov E, Mazzeo P, Zinkernagel MS, Legros M, Porret N, Romagna L, Haase D, Lenz G, Novak U, Banz Y, et al. Comprehensive Laboratory Diagnostic Workup for Patients with Suspected Intraocular Lymphoma including Flow Cytometry, Molecular Genetics and Cytopathology. Current Oncology. 2022; 29(2):766-776. https://doi.org/10.3390/curroncol29020065
Chicago/Turabian StyleShumilov, Evgenii, Paolo Mazzeo, Martin S. Zinkernagel, Myriam Legros, Naomi Porret, Lorenz Romagna, Detlef Haase, Georg Lenz, Urban Novak, Yara Banz, and et al. 2022. "Comprehensive Laboratory Diagnostic Workup for Patients with Suspected Intraocular Lymphoma including Flow Cytometry, Molecular Genetics and Cytopathology" Current Oncology 29, no. 2: 766-776. https://doi.org/10.3390/curroncol29020065
APA StyleShumilov, E., Mazzeo, P., Zinkernagel, M. S., Legros, M., Porret, N., Romagna, L., Haase, D., Lenz, G., Novak, U., Banz, Y., Pabst, T., & Bacher, U. (2022). Comprehensive Laboratory Diagnostic Workup for Patients with Suspected Intraocular Lymphoma including Flow Cytometry, Molecular Genetics and Cytopathology. Current Oncology, 29(2), 766-776. https://doi.org/10.3390/curroncol29020065