A Comparison of Patients’ and Physicians’ Knowledge and Expectations Regarding Precision Oncology Tests


Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Questionnaire
2.2. Physician Questionnaire
2.3. Statistical Analysis
3. Results
- (a)
- Characteristics of patients and physicians:
- (b)
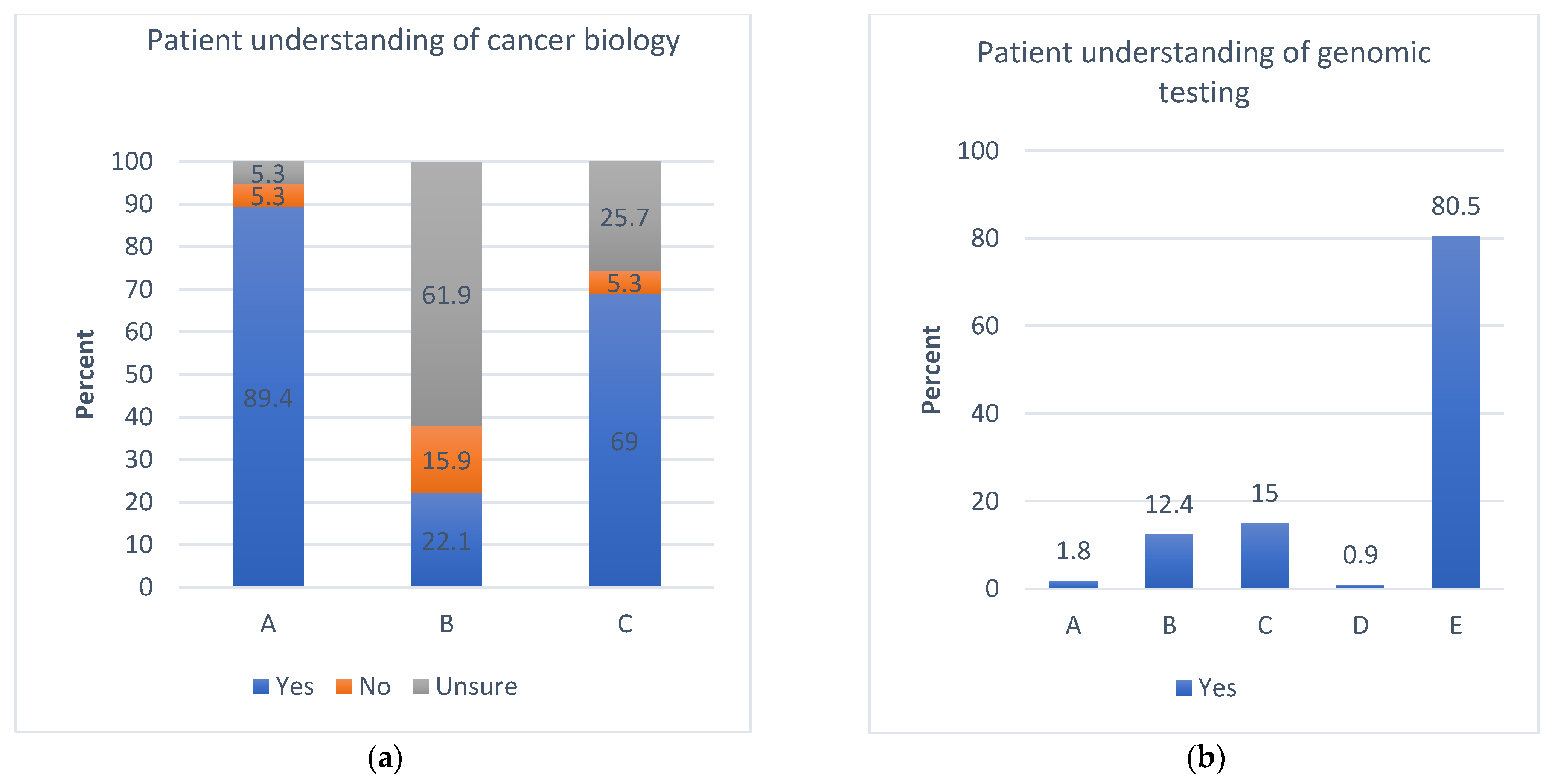
- Patient understanding of cancer biology and awareness of genomic testing:
- (c)
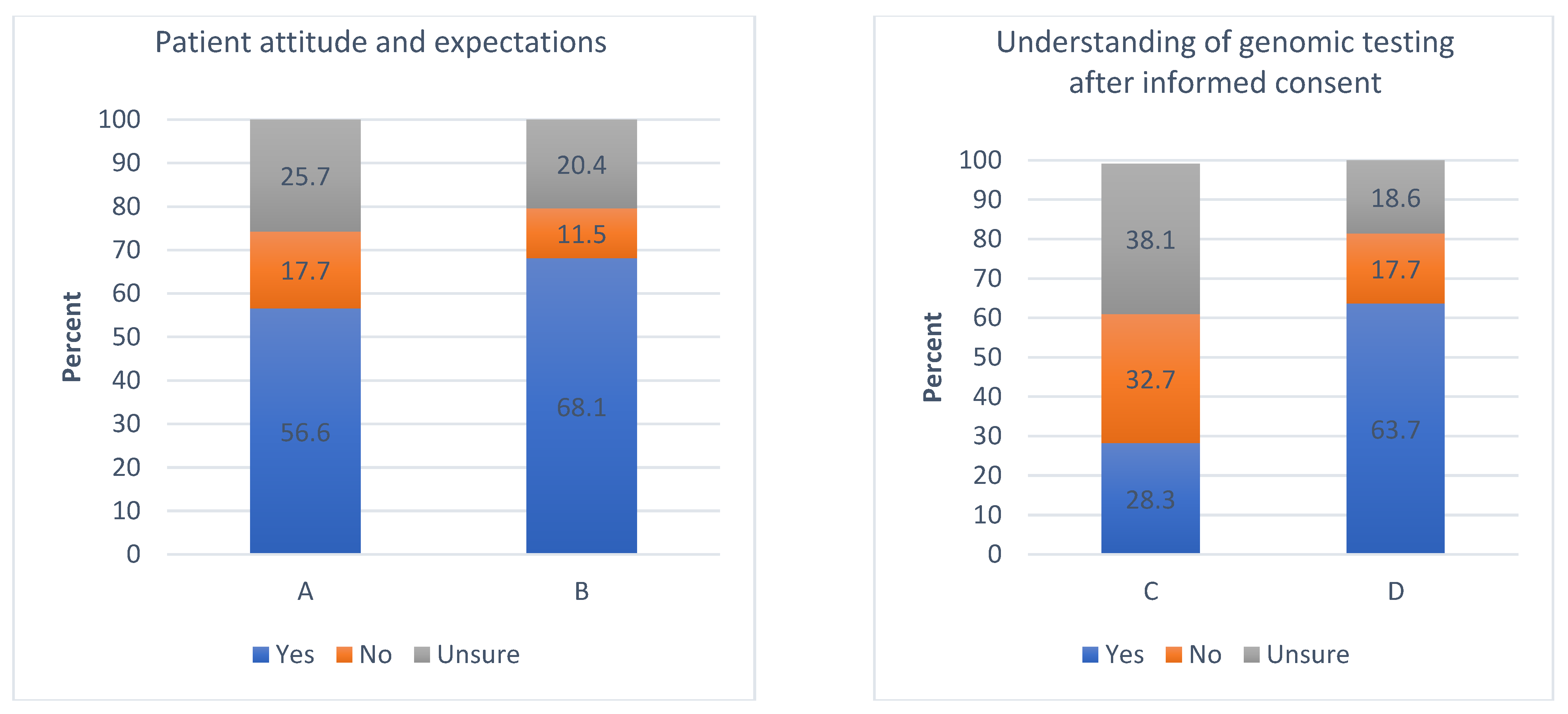
- Attitude and expectations of patients towards genomic testing and research:
- (d)
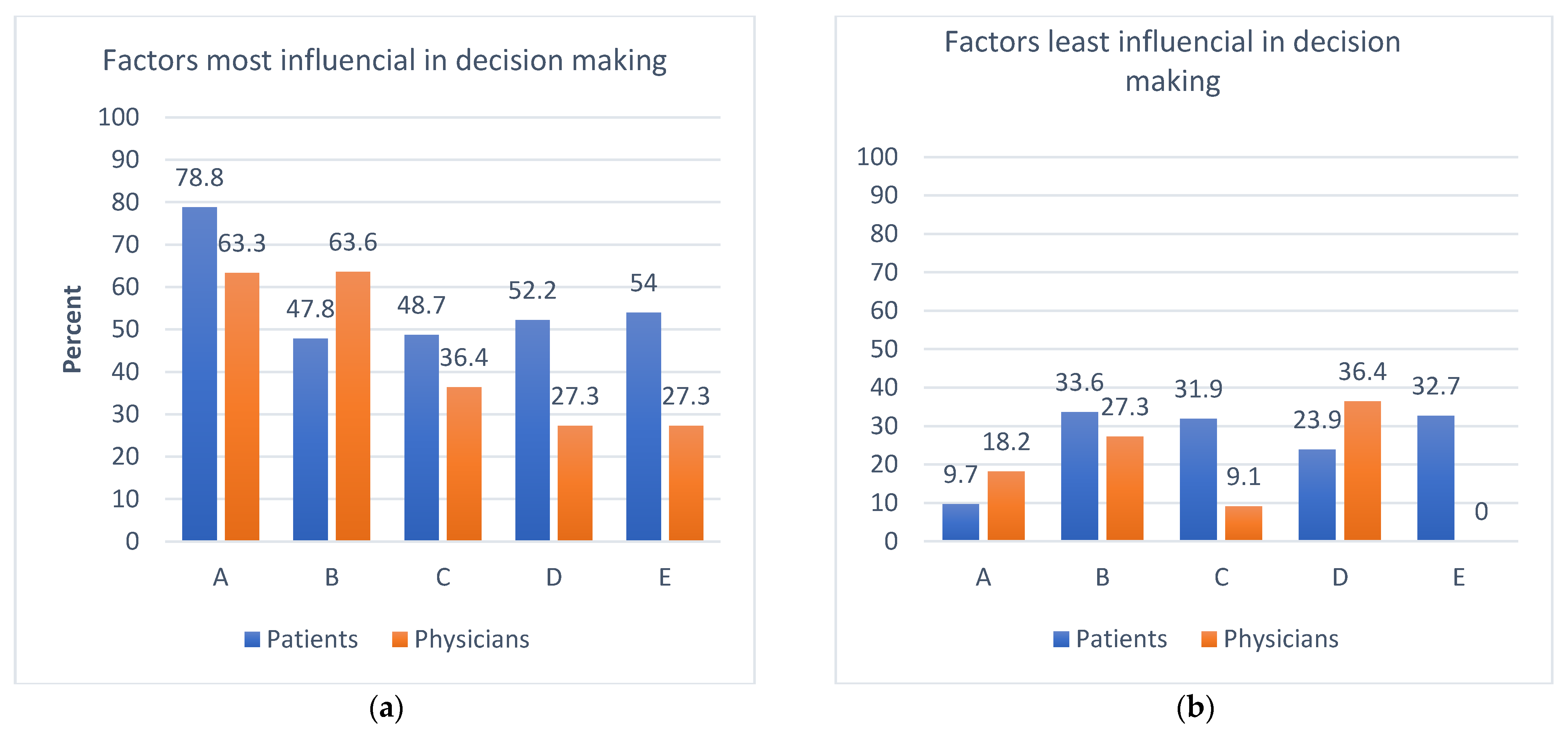
- Attitudes and expectations of patients vs physicians regarding genomic testing:
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDermott, U.; Downing, J.R.; Stratton, M.R. Genomics and the Continuum of Cancer Care. N. Engl. J. Med. 2011, 364, 340–350. [Google Scholar] [CrossRef]
- Bombard, Y.; Bach, P.B.; Offit, K. Translating Genomics in Cancer Care. J. Natl. Compr. Cancer Netw. 2013, 11, 1343–1353. [Google Scholar] [CrossRef] [PubMed]
- Schwartzberg, L.; Kim, E.S.; Liu, D.; Schrag, D. Precision Oncology: Who, How, What, When, and When Not? Am. Soc. Clin. Oncol. Educ. Book 2017, 37, 160–169. [Google Scholar] [CrossRef]
- Seyhan, A.A.; Carini, C. Are innovation and new technologies in precision medicine paving a new era in patient-centric care? J. Transl. Med. 2019, 17, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Chevallier, M.; Borgeaud, M.; Addeo, A.; Friedlaender, A. Oncogenic driver mutations in non-small cell lung cancer: Past, present and future. World J. Clin. Oncol. 2021, 12, 217–237. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. NCCN Guidelines Insights: Non–Small Cell Lung Cancer, Version 2.2021. J. Natl. Compr. Cancer Netw. 2021, 19, 254–266. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.-W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.-Y.; Molina, J.; Kim, J.-H.; Arvis, C.D.; Ahn, M.-J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, T.; Yatabe, Y.; Endoh, H.; Yoshida, K.; Hida, T.; Tsuboi, M.; Tada, H.; Kuwano, H.; Mitsudomi, T. Analysis of Epidermal Growth Factor Receptor Gene Mutation in Patients with Non–Small Cell Lung Cancer and Acquired Resistance to Gefitinib. Clin. Cancer Res. 2006, 12, 5764–5769. [Google Scholar] [CrossRef]
- Karapetis, C.S.; Khambata-Ford, S.; Jonker, D.J.; O’Callaghan, C.J.; Tu, D.; Tebbutt, N.C.; Simes, R.J.; Chalchal, H.; Shapiro, J.D.; Robitaille, S.; et al. K-rasMutations and Benefit from Cetuximab in Advanced Colorectal Cancer. N. Engl. J. Med. 2008, 359, 1757–1765. [Google Scholar] [CrossRef]
- Bokemeyer, C.; Bondarenko, I.; Hartmann, J.T.; De Braud, F.; Schuch, G.; Zubel, A.; Celik, I.; Schlichting, M.; Koralewski, P. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: The OPUS study. Ann. Oncol. 2011, 22, 1535–1546. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Köhne, C.-H.; Láng, I.; Folprecht, G.; Nowacki, M.P.; Cascinu, S.; Shchepotin, I.; Maurel, J.; Cunningham, D.; Tejpar, S.; et al. Cetuximab Plus Irinotecan, Fluorouracil, and Leucovorin As First-Line Treatment for Metastatic Colorectal Cancer: Updated Analysis of Overall Survival According to Tumor KRAS and BRAF Mutation Status. J. Clin. Oncol. 2011, 29, 2011–2019. [Google Scholar] [CrossRef] [PubMed]
- Ogunwobi, O.O.; Mahmood, F.; Akingboye, A. Biomarkers in Colorectal Cancer: Current Research and Future Prospects. Int. J. Mol. Sci. 2020, 21, 5311. [Google Scholar] [CrossRef] [PubMed]
- Artomov, M. Improving survival prediction for melanoma. eLife 2019, 8, e48145. [Google Scholar] [CrossRef] [PubMed]
- Korngiebel, D.M.; Thummel, K.E.; Burke, W. Implementing Precision Medicine: The Ethical Challenges. Trends Pharmacol. Sci. 2017, 38, 8–14. [Google Scholar] [CrossRef]
- Lerman, C. BRCA1 Testing in Families With Hereditary Breast-Ovarian Cancer. JAMA 1996, 275, 1885. [Google Scholar] [CrossRef]
- Donovan, K.A.; Tucker, D.C. Knowledge about genetic risk for breast cancer and perceptions of genetic testing in a sociodemographically diverse sample. J. Behav. Med. 2000, 23, 15–36. [Google Scholar] [CrossRef]
- Cyrus-David, M.S. Knowledge and Accuracy of Perceived Personal Risk in Underserved Women Who are at Increased Risk of Breast Cancer. J. Cancer Educ. 2010, 25, 617–623. [Google Scholar] [CrossRef]
- Caruso, A.; Vigna, C.; Maggi, G.; Sega, F.M.; Cognetti, F.; Savarese, A. The withdrawal from oncogenetic counselling and testing for hereditary and familial breast and ovarian cancer. A descriptive study of an Italian sample. J. Exp. Clin. Cancer Res. 2008, 27, 75. [Google Scholar] [CrossRef]
- Bluman, L.G.; Rimer, B.; Berry, D.A.; Borstelmann, N.A.; Iglehart, J.D.; Regan, K.; Schildkraut, J.M.; Winer, E.P. Attitudes, knowledge, and risk perceptions of women with breast and/or ovarian cancer considering testing for BRCA1 and BRCA2. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1999, 17, 1040–1046. [Google Scholar] [CrossRef]
- Gray, S.W.; Hicks-Courant, K.; Lathan, C.S.; Garraway, L.; Park, E.R.; Weeks, J.C. Attitudes of Patients With Cancer About Personalized Medicine and Somatic Genetic Testing. J. Oncol. Pract. 2012, 8, 329–335. [Google Scholar] [CrossRef]
- Cheung, W.Y.; Neville, B.A.; Cameron, D.B.; Cook, E.F.; Earle, C.C. Comparisons of Patient and Physician Expectations for Cancer Survivorship Care. J. Clin. Oncol. 2009, 27, 2489–2495. [Google Scholar] [CrossRef] [PubMed]
- Cheung, W.Y.; Neville, B.A.; Earle, C.C. Associations Among Cancer Survivorship Discussions, Patient and Physician Expectations, and Receipt of Follow-Up Care. J. Clin. Oncol. 2010, 28, 2577–2583. [Google Scholar] [CrossRef] [PubMed]
- Ciardiello, F.; Adams, R.; Tabernero, J.; Seufferlein, T.; Taieb, J.; Moiseyenko, V.; Ma, B.; Lopez, G.; Vansteenkiste, J.F.; Esser, R.; et al. Awareness, Understanding, and Adoption of Precision Medicine to Deliver Personalized Treatment for Patients With Cancer: A Multinational Survey Comparison of Physicians and Patients. Oncologist 2016, 21, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.-H.; Kang, H.-Y.; Suh, H.S.; Lee, S.; Oh, E.S.; Jeong, H. Awareness and attitude of the public toward personalized medicine in Korea. PLoS ONE 2018, 13, e0192856. [Google Scholar] [CrossRef]
- Kichko, K.; Marschall, P.; Flessa, S. Personalized Medicine in the U.S. and Germany: Awareness, Acceptance, Use and Preconditions for the Wide Implementation into the Medical Standard. J. Pers. Med. 2016, 6, 15. [Google Scholar] [CrossRef]
- Marchiano, E.J.; Birkeland, A.C.; Swiecicki, P.L.; Spector-Bagdady, K.; Shuman, A.G. Revisiting Expectations in an Era of Precision Oncology. Oncologist 2018, 23, 386–388. [Google Scholar] [CrossRef]
- Bedard, P.L.; Oza, A.M.; Tsao, M.-S.; Leighl, N.B.; Shepherd, F.A.; Chen, E.X.; Tannock, I.; Krzyzanowska, M.K.; Dhani, N.C.; Clarke, B.; et al. Princess Margaret Cancer Centre (PMCC) Integrated Molecular Profiling in Advanced Cancers Trial (IMPACT) using genotyping and targeted next-generation sequencing (NGS). J. Clin. Oncol. 2013, 31, 11002. [Google Scholar] [CrossRef]
- Dancey, J.E.; Bedard, P.L.; Onetto, N.; Hudson, T.J. The Genetic Basis for Cancer Treatment Decisions. Cell 2012, 148, 409–420. [Google Scholar] [CrossRef]
- Miller, F.A.; Hayeems, R.Z.; Bytautas, J.P.; Bedard, P.L.; Ernst, S.; Hirte, H.; Hotte, S.; Oza, A.; Razak, A.; Welch, S.; et al. Testing personalized medicine: Patient and physician expectations of next-generation genomic sequencing in late-stage cancer care. Eur. J. Hum. Genet. 2014, 22, 391–395. [Google Scholar] [CrossRef]
- Blanchette, P.S.; Spreafico, A.; Miller, F.A.; Chan, K.; Bytautas, J.; Kang, S.; Bedard, P.L.; Eisen, A.; Potanina, L.; Holland, J.; et al. Genomic testing in cancer: Patient knowledge, attitudes, and expectations. Cancer 2014, 120, 3066–3073. [Google Scholar] [CrossRef]
- Prince, A.E.R.; Berkman, B.E. Reconceptualizing harms and benefits in the genomic age. Per. Med. 2018, 15, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Mcfarland, D.C.; Blackler, E.; Banerjee, S.; Holland, J. Communicating About Precision Oncology. JCO Precis. Oncol. 2017, 1, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Arora, N.K. Interacting with cancer patients: The significance of physicians’ communication behavior. Soc. Sci. Med. 2003, 57, 791–806. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, I.; Rapti, M.; Extra, J.M.; Petri-Cal, A.; Apostolidis, T.; Ferrero, J.-M.; Bachelot, T.; Viens, P.; JuliaŽ Reynier, C.; Bertucci, F. Tailored chemotherapy based on tumour gene expression analysis: Breast cancer patients’ misinterpretations and positive attitudes. Eur. J. Cancer Care 2012, 21, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Lillie, S.E.; Brewer, N.T.; O’Neill, S.C.; Morrill, E.F.; Dees, E.C.; Carey, L.A.; Rimer, B. Retention and Use of Breast Cancer Recurrence Risk Information from Genomic Tests: The Role of Health Literacy. Cancer Epidemiol. Biomark. Prev. 2007, 16, 249–255. [Google Scholar] [CrossRef]
- McClement, S.E.; Chochinov, H.M. Hope in advanced cancer patients. Eur. J. Cancer 2008, 44, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Sulmasy, D.P.; Astrow, A.B.; He, M.K.; Seils, D.M.; Meropol, N.J.; Micco, E.; Weinfurt, K.P. The culture of faith and hope. Cancer 2010, 116, 3702–3711. [Google Scholar] [CrossRef]
- Weeks, J.C.; Catalano, P.J.; Cronin, A.; Finkelman, M.D.; Mack, J.W.; Keating, N.L.; Schrag, D. Patients’ Expectations about Effects of Chemotherapy for Advanced Cancer. N. Engl. J. Med. 2012, 367, 1616–1625. [Google Scholar] [CrossRef]
- Kalia, S.S.; Adelman, K.; Bale, S.J.; Chung, W.K.; Eng, C.; Evans, J.P.; Herman, G.E.; Hufnagel, S.B.; Klein, T.E.; Korf, B.R.; et al. Recommendations for reporting secondary findings in clinical exome and genome sequencing, 2016 update (ACMG SF 2.0): A policy statement of American College of Genetics and Genomics. Genet. Med. 2017, 19, 249–255. [Google Scholar] [CrossRef]
- Hoerger, M.; Epstein, R.M.; Winters, P.C.; Fiscella, K.; Duberstein, P.R.; Gramling, R.; Butow, P.N.; Mohile, S.G.; Kaesberg, P.R.; Tang, W.; et al. Values and options in cancer care (VOICE): Study design and rationale for patient-centred communication and decision-making intervention for physicians, patients with advanced cancer, and their caregivers. BMC Cancer 2013, 13, 188. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | N (%) |
|---|---|
| Gender | |
| Male | 61 (53.9%) |
| Female | 52 (46%) |
| Tumour sites | |
| Breast | 48 (44%) |
| Colon | 30 (26.5%) |
| Pancreas | 5 (4.4%) |
| Renal | 4 (3.5%) |
| Melanoma | 11 (9.7%) |
| Lung | 10 (8.8%) |
| Prostate | 5 (4.4%) |
| Marital status | |
| Single | 16 (14.2%) |
| Married | 74 (65.5%) |
| Common-law/live-in partner | 8 (7.1%) |
| Separated/divorced | 6 (5.3%) |
| Widowed | 7 (6.2%) |
| Other | 1 (0.9%) |
| Prefer not to say | 1 (0.9%) |
| Highest level of education | |
| Less than high school | 1 (0.9%) |
| High school certificate or equivalent | 26 (23%) |
| Community college, technical college, or CEGEP | 41 (36.3%) |
| University—undergraduate degree | 22 (19.5%) |
| University—graduate or professional degree | 20 (17.7%) |
| Prefer not to say | 3 (2.6%) |
| Work experience/educational experience in healthcare | |
| Yes | 21 (18.6%) |
| No | 92 (81.4%) |
| A family member works in healthcare | |
| Yes | 39 (34.5%) |
| No | 74 (65.4%) |
| A family member diagnosed with cancer | |
| Yes | 62 (54.9%) |
| No | 51 (45.1%) |
| Personal annual income | |
| Less than CAD 50,000 | 33 (29.2%) |
| CAD 50,000–99,999 | 34 (31.1%) |
| CAD 100,000–149,999 | 10 (8.8%) |
| CAD 150,000 or greater | 6 (5.3%) |
| I prefer not to say | 30 (26.5%) |
| Questions about Patients’ and Physicians’ Interests, Attitudes, and Expectations about Genomics Testing in Cancer Care | Concordance (%) |
|---|---|
| Would most of your patients be willing to undergo a minor procedure—a needle biopsy under a local anesthetic, if required—to obtain a tissue sample for genomics testing? | 68.75 |
| Would most of your patients be willing to undergo a more significant procedure—a surgical biopsy under a general anesthetic—to obtain a tissue sample for genomics testing? | 33.04 |
| How much do you agree or disagree with the following statement about genomics testing in your cancer patients: | |
| 26.13 |
| 29.73 |
| 36.04 |
| 25.23 |
| Of the following listed factors, which would most influence you to pursue genomics testing in the care of your cancer patients? | |
| 65.18 |
| 38.39 |
| 23.21 |
| 12.5 |
| None |
| Of the following listed factors, which would least influence you to pursue genomics testing in the care of your cancer patients? | |
| None |
| 3.57 |
| 5.36 |
| 8.04 |
| 13.39 |
| Of the following listed factors, which would most influence you in a decision not to pursue genomics testing in the care of your cancer patients? | |
| 56.25 |
| 19.64 |
| 8.04 |
| None |
| 26.79 |
| Of the following listed factors, which would least influence you in a decision not to pursue DNA testing in the care of your cancer patients? | |
| 6.25 |
| 8.93 |
| 5.36 |
| 24.11 |
| 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dehar, N.; Abedin, T.; Tang, P.; Bebb, G.; Cheung, W.Y. A Comparison of Patients’ and Physicians’ Knowledge and Expectations Regarding Precision Oncology Tests. Curr. Oncol. 2022, 29, 9916-9927. https://doi.org/10.3390/curroncol29120780
Dehar N, Abedin T, Tang P, Bebb G, Cheung WY. A Comparison of Patients’ and Physicians’ Knowledge and Expectations Regarding Precision Oncology Tests. Current Oncology. 2022; 29(12):9916-9927. https://doi.org/10.3390/curroncol29120780
Chicago/Turabian StyleDehar, Navdeep, Tasnima Abedin, Patricia Tang, Gwyn Bebb, and Winson Y. Cheung. 2022. "A Comparison of Patients’ and Physicians’ Knowledge and Expectations Regarding Precision Oncology Tests" Current Oncology 29, no. 12: 9916-9927. https://doi.org/10.3390/curroncol29120780
APA StyleDehar, N., Abedin, T., Tang, P., Bebb, G., & Cheung, W. Y. (2022). A Comparison of Patients’ and Physicians’ Knowledge and Expectations Regarding Precision Oncology Tests. Current Oncology, 29(12), 9916-9927. https://doi.org/10.3390/curroncol29120780