A Portrait of Cord Blood Units Distributed for Transplantation from Canadian Blood Services’ Cord Blood Bank: First Analysis

Abstract
1. Introduction
2. Methods
2.1. Donor, Recipient and CBU Information
2.2. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanate, A.S.; Majhail, N.S.; Savani, B.N.; Bredeson, C.; Champlin, R.E.; Crawford, S.; Giralt, S.A.; LeMaistre, C.F.; Marks, D.I.; Omel, J.L.; et al. Indications for Hematopoietic Cell Transplantation and Immune Effector Cell Therapy: Guidelines from the American Society for Transplantation and Cellular Therapy. Biol. Blood Marrow Transplant. 2020, 26, 1247–1256. [Google Scholar] [CrossRef] [PubMed]
- Allan, D.S.; Takach, S.; Smith, S.; Goldman, M. Impact of declining fertility rates in Canada on donor options in blood and marrow transplantation. Biol. Blood Marrow Transplant. 2009, 15, 1634–1637. [Google Scholar] [CrossRef][Green Version]
- Gragert, L.; Eapen, M.; Williams, E.; Freeman, J.; Spellman, S.; Baitty, R.; Hartzman, R.; Rizzo, J.D.; Horowitz, M.; Confer, D.; et al. HLA Match Likelihoods for Hematopoietic Stem-Cell Grafts in the U.S. Registry. N. Engl. J. Med. 2014, 371, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Allan, D.; Kiernan, J.; Gragert, L.; Dibdin, N.; Bartlett, D.; Campbell, T.; Mostert, K.; Halpenny, M.; Ganz, K.; Maiers, M.; et al. Reducing ethnic disparity in access to high-quality HLA-matched cord blood units for transplantation: Analysis of the Canadian Blood Services’ Cord Blood Bank inventory. Transfusion 2019, 59, 2382–2388. [Google Scholar] [CrossRef] [PubMed]
- Milano, F.; Gooley, T.; Wood, B.; Woolfrey, A.; Flowers, M.E.; Doney, K.; Witherspoon, R.; Mielcarek, M.; Deeg, J.H.; Sorror, M.; et al. Cord-Blood Transplantation in Patients with Minimal Residual Disease. N. Engl. J. Med. 2016, 375, 944–953. [Google Scholar] [CrossRef]
- Niederwieser, D.; Baldomero, H.; Bazuaye, N.; Bupp, C.; Chaudhri, N.; Corbacioglu, S.; Elhaddad, A.; Frutos, C.; Galeano, S.; Hamad, N.; et al. One and a half million hematopoietic stem cell transplants: Continuous and differential improvement in worldwide access with the use of non-identical family donors. Haematologica 2021, 107, 1045–1053. [Google Scholar] [CrossRef]
- Passweg, J.R.; Baldomero, H.; Chabannon, C.; Basak, G.W.; De La Camara, R.; Corbacioglu, S.; Dolstra, H.; Duarte, R.; Glass, B.; Greco, R.; et al. Hematopoietic cell transplantation and cellular therapy survey of the EBMT: Monitoring of activities and trends over 30 years. Bone Marrow Transplant. 2021, 56, 1651–1664. [Google Scholar] [CrossRef]
- Magalon, J.; Maiers, M.; Kurtzberg, J.; Navarrete, C.; Rubinstein, P.; Brown, C.; Schramm, C.; Larghero, J.; Katsahian, S.; Chabannon, C.; et al. Banking or Bankrupting: Strategies for Sustaining the Economic Future of Public Cord Blood Banks. PLoS ONE 2015, 10, e0143440. [Google Scholar] [CrossRef]
- Passweg, J.R.; Baldomero, H.; Chabannon, C.; Corbacioglu, S.; de la Cámara, R.; Dolstra, H.; Glass, B.; Greco, R.; Mohty, M.; Neven, B.; et al. Impact of the SARS-CoV-2 pandemic on hematopoietic cell transplantation and cellular therapies in Europe 2020: A report from the EBMT activity survey. Bone Marrow Transplant. 2022, 57, 742–752. [Google Scholar] [CrossRef]
- Jöris, M.M.; Schmidt, A.H.; Bernas, S.N.; Feinberg, J.; Sacchi, N.; Elmoazzen, H.; Fournier, D.; Oguz, F.; Oliveira, D.; Yang, K.-L.; et al. Impact of COVID-19 pandemic on global unrelated stem cell donations in 2020—Report from World Marrow Donor Association. Bone Marrow Transplant. 2022, 57, 1021–1024. [Google Scholar] [CrossRef]
- Allan, D.S.; Scrivens, N.; Lawless, T.; Mostert, K.; Oppenheimer, L.; Walker, M.; Petraszko, T.; Elmoazzen, H. Delayed clamping of the umbilical cord after delivery and implications for public cord blood banking. Transfusion 2015, 56, 662–665. [Google Scholar] [CrossRef]
- WMDA Global Trends Report. 2021. Available online: https://wmda.info/wp-content/uploads/2022/07/CORRECTED-21042022-GTR-2021-Summary-slides-002.pdf (accessed on 22 November 2022).
- Wynn, L.A.; Horton, R.; Gibson, D. Ethnic diversity and cord blood banking: Satisfying the unmet need. Cytotherapy 2022, 24, 1060–1066. [Google Scholar] [CrossRef] [PubMed]
- Barker, J.N.; Byam, C.E.; Kernan, N.A.; Lee, S.S.; Hawke, R.M.; Doshi, K.A.; Wells, D.S.; Heller, G.; Papadopoulos, E.B.; Scaradavou, A.; et al. Availability of cord blood extends allogeneic hematopoietic stem cell transplant access to racial and ethnic minorities. Biol. Blood Marrow Transplant. 2010, 16, 1541–1548. [Google Scholar] [CrossRef] [PubMed]
- Kosuri, S.; Wolff, T.; Devlin, S.M.; Byam, C.; Mazis, C.M.; Naputo, K.; Davis, E.; Paulson, J.; Nhaissi, M.; Wells, D.S.; et al. Prospective Evaluation of Unrelated Donor Cord Blood and Haploidentical Donor Access Reveals Graft Availability Varies by Patient Ancestry: Practical Implications for Donor Selection. Biol. Blood Marrow Transplant. 2017, 23, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Statistics Canada. Table 98-400-X2016189 Ethnic Origin (101), Age (15A), Sex (3) and Selected Demographic, Cultural, Labour Force, Educational and Income Characteristics (651) for the Population in Private Households of Canada, Provinces and Territories, Census Metropolitan. 2018. Available online: https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/dt-td/Rp-eng.cfm?TABID=2&LANG=E&A=R&APATH=3&DETAIL=0&DIM=0&FL=A&FREE=0&GC=01&GL=- (accessed on 17 June 2022).
- Politikos, I.; Davis, E.; Nhaissi, M.; Wagner, J.E.; Brunstein, C.G.; Cohen, S.; Shpall, E.J.; Milano, F.; Scaradavou, A.; Barker, J.N. Guidelines for Cord Blood Unit Selection. Biol. Blood Marrow Transplant. 2020, 26, 2190–2196. [Google Scholar] [CrossRef]
- Hough, R.; Danby, R.; Russell, N.; Marks, D.; Veys, P.; Shaw, B.; Wynn, R.; Vora, A.; Mackinnon, S.; Peggs, K.S.; et al. Recommendations for a standard UK approach to incorporating umbilical cord blood into clinical transplantation practice: An update on cord blood unit selection, donor selection algorithms and conditioning protocols. Br. J. Haematol. 2016, 172, 360–370. [Google Scholar] [CrossRef]
- Boelens, J.J.; Aldenhoven, M.; Purtill, D.; Ruggeri, A.; DeFor, T.; Wynn, R.; Wraith, E.; Cavazzana-Calvo, M.; Rovelli, A.; Fischer, A.; et al. Outcomes of transplantation using various hematopoietic cell sources in children with Hurler syndrome after myeloablative conditioning. Blood 2013, 121, 3981–3987. [Google Scholar] [CrossRef]
- Fernandes, J.F.; Rocha, V.; Labopin, M.; Neven, B.; Moshous, D.; Gennery, A.R.; Friedrich, W.; Porta, F.; Diaz de Heredia, C.; Wall, D.; et al. Transplantation in patients with SCID: Mismatched related stem cells or unrelated cord blood? Blood J. Am. Soc. Hematol. 2012, 119, 2949–2955. [Google Scholar] [CrossRef]
- de Latour, R.P.; Purtill, D.; Ruggeri, A.; Sanz, G.; Michel, G.; Gandemer, V.; Maury, S.; Kurtzberg, J.; Bonfim, C.; Aljurf, M.; et al. Influence of nucleated cell dose on overall survival of unrelated cord blood transplantation for patients with severe acquired aplastic anemia: A study by eurocord and the aplastic anemia working party of the European group for blood and marrow transplantation. Biol. Blood Marrow Transplant. 2011, 17, 78–85. [Google Scholar]
- O’Donnell, P.V.; Brunstein, C.G.; Fuchs, E.J.; Zhang, M.J.; Allbee-Johnson, M.; Antin, J.H.; Leifer, E.S.; Elmariah, H.; Grunwald, M.R.; Hashmi, H.; et al. Umbilical cord blood or HLA-haploidentical transplantation: Real-world outcomes versus randomized trial outcomes. Transplant. Cell. Ther. 2022, 28, 109-e1. [Google Scholar] [CrossRef]
- Fuchs, E.J.; O’Donnell, P.V.; Eapen, M.; Logan, B.; Antin, J.H.; Dawson, P.; Devine, S.; Horowitz, M.M.; Horwitz, M.E.; Karanes, C.; et al. Double unrelated umbilical cord blood vs HLA-haploidentical bone marrow transplantation: The BMT CTN 1101 trial. Blood 2021, 137, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Saiyin, T.; Kirkham, A.M.; Bailey, A.J.; Shorr, R.; Pineault, N.; Maganti, H.B.; Allan, D.S. Clinical outcomes of umbilical cord blood transplantation utilizing ex vivo expansion: A systematic review and meta-analysis of controlled studies. Transplant. Cell. Ther. 2022. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
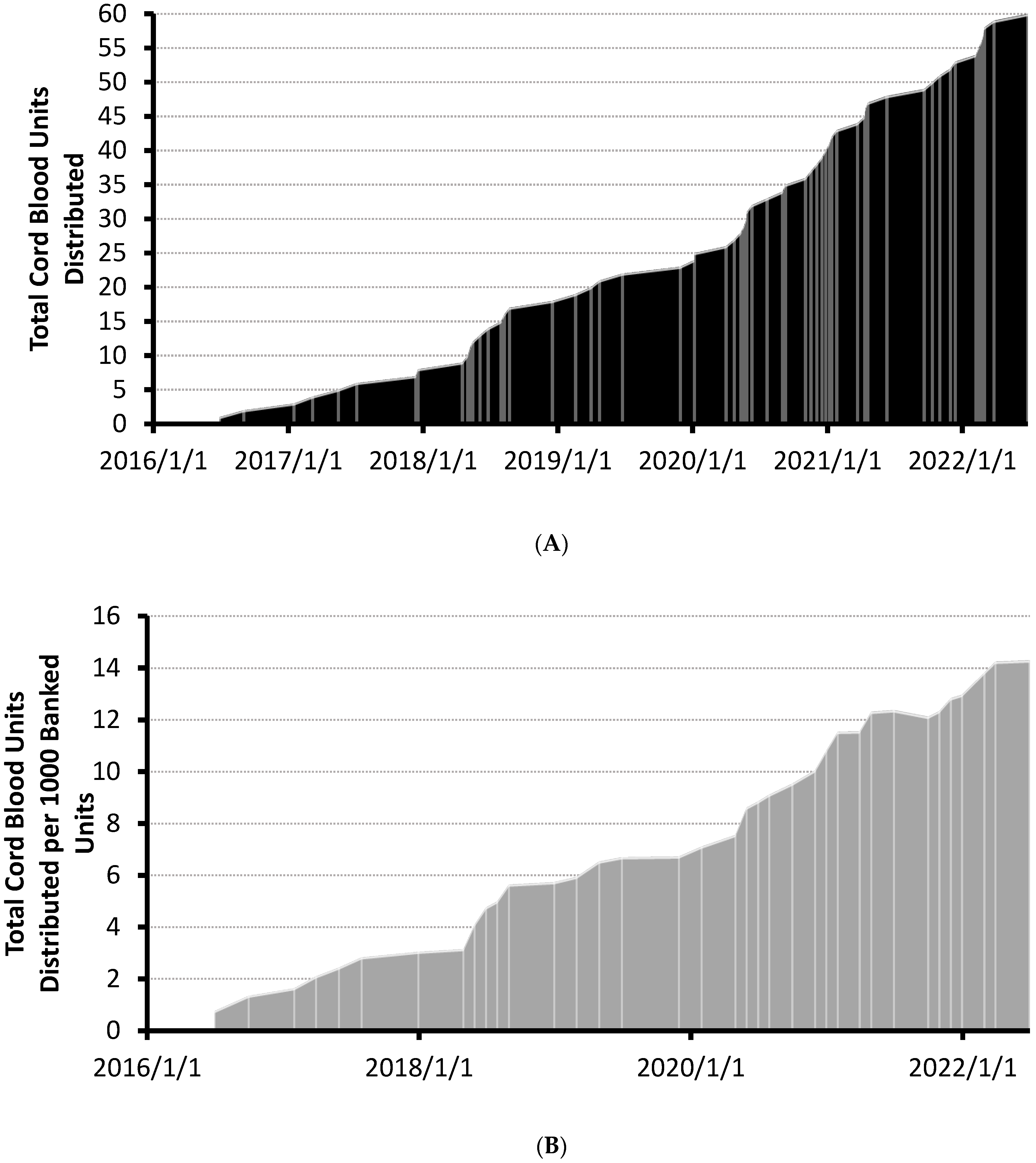
| Year | Total Cords Distributed (Cumulative) | Total Cords in Inventory | Usage (%) |
|---|---|---|---|
| 2015 | 0 | 664 | 0 |
| 2016 | 2 | 1684 | 0.12 |
| 2017 | 10 | 2626 | 0.30 |
| 2018 | 18 | 3137 | 0.57 |
| 2019 | 23 | 3437 | 0.67 |
| 2020 | 40 | 3701 | 1.1 |
| 2021 | 53 | 4085 | 1.3 |
| June 2022 | 60 | 4197 | 1.4 |
| Recipient Age, n (%), and Weight, kg (Range) | |
|---|---|
| 0–4 years | 25 (41.7), 10.6 (4–19) |
| 5–17 years | 7 (11.7), 42.7 (13–108) |
| 18+ years | 28 (46.7), 84.2 (54–157) |
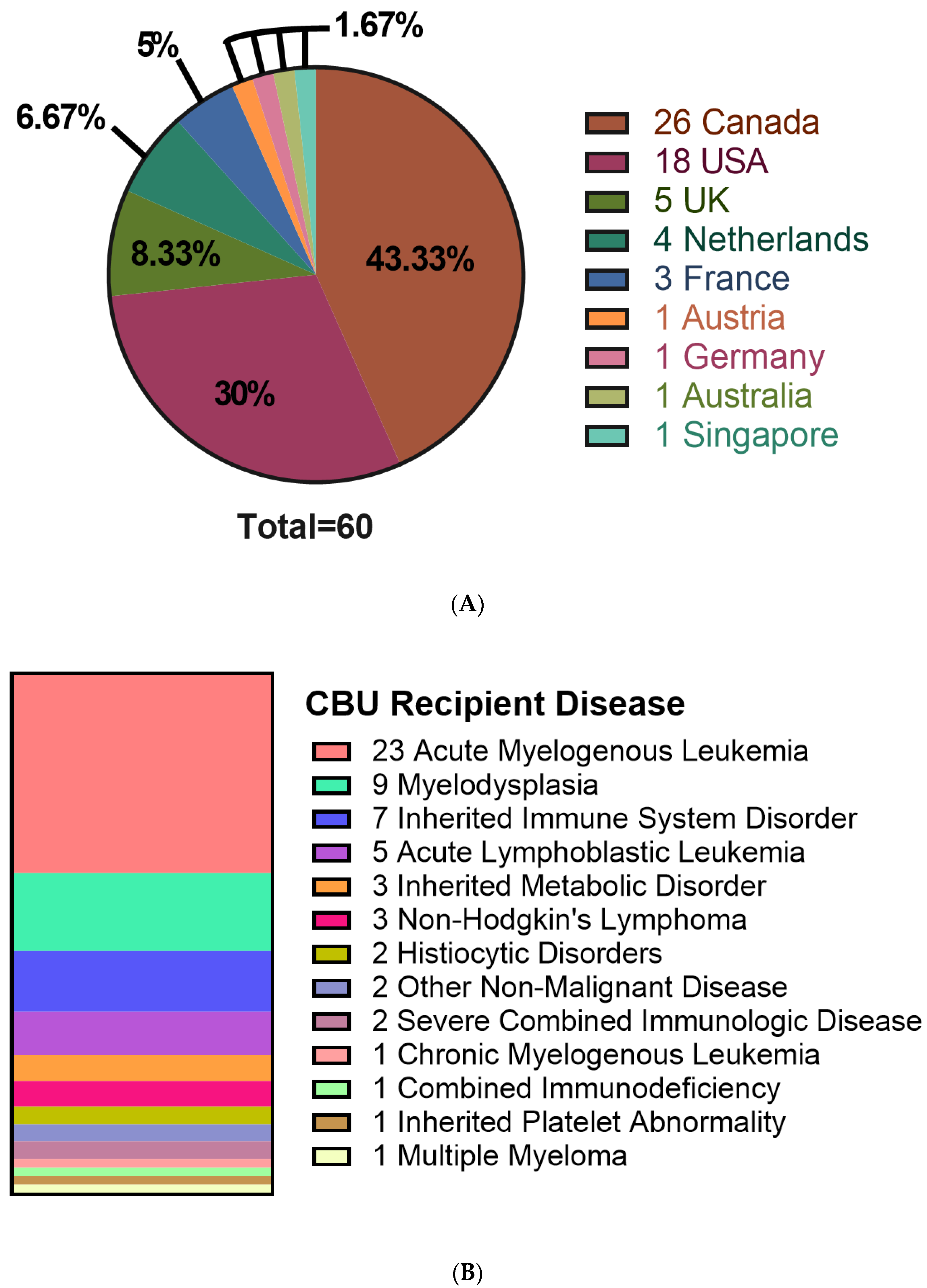
| Recipient Location (N, (%)) | |
| Canada | 26 (43.3) |
| USA | 18 (30) |
| Other | 16 (26.7) |
| Recipient Disease (N, (%)) | |
| Hematologic Cancer | 42 (70) |
| Inherited Disorder | 14 (23.3) |
| Other | 4 (6.7) |
| Donor-Recipient Match Level (N, (%)) | |
| 6/6 Match | 9 (15) |
| 5/6 Match | 28 (46.7) |
| 4/6 Match | 23 (38.3) |
| Double cord blood recipients (N, (%)) * | 10 (16.7) |
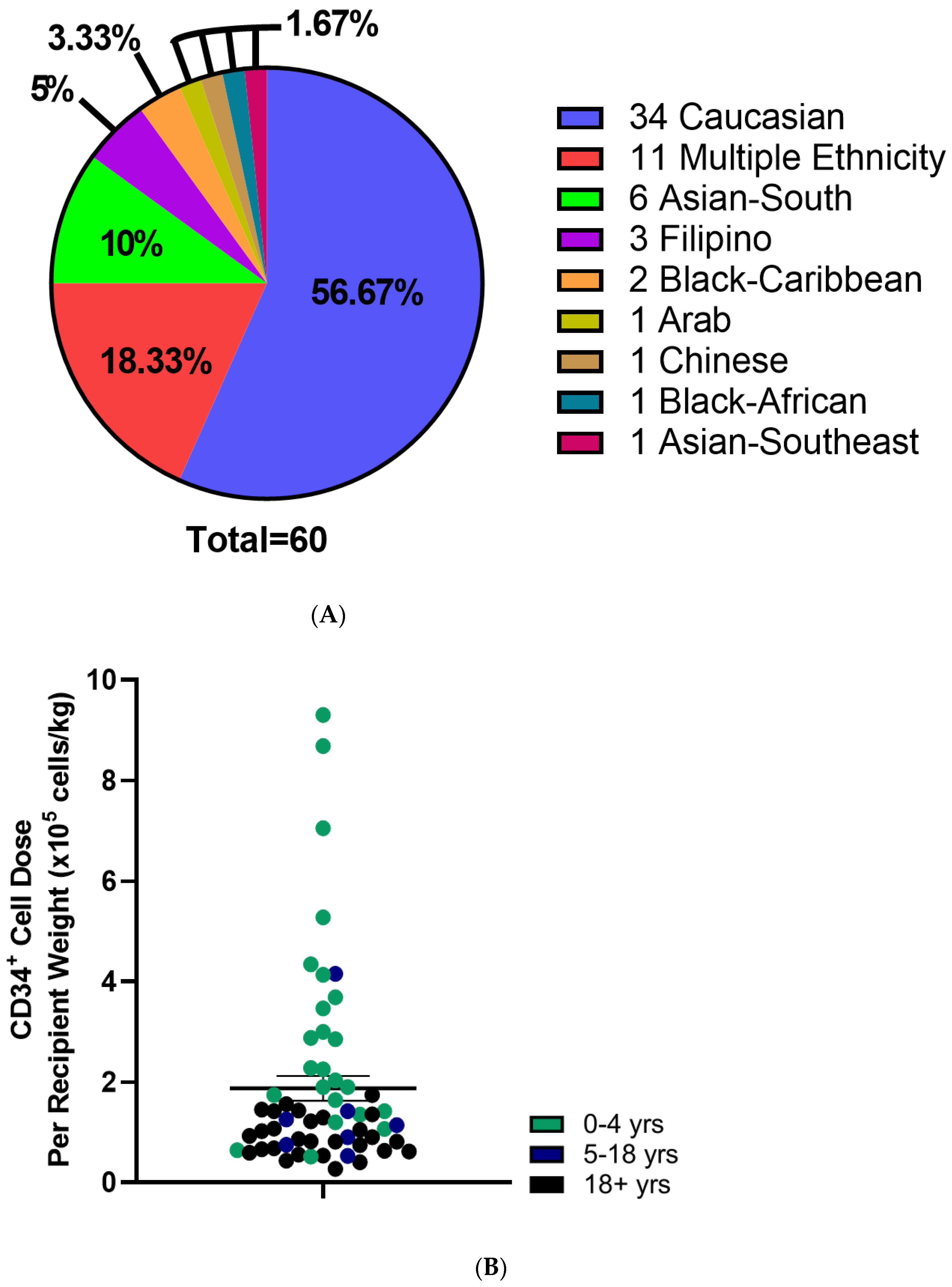
| CBU Ethnicity (N, (%)) | |
|---|---|
| Caucasian | 34 (56.7) |
| Multiple Ethnicity | 11 (18.3) |
| Other | 15 (25) |
| Total Nucleated Cell Count (×109 cells) | 1.9 ± 0.1 |
| Total CD34+ Cell Count (×106 cells) | 5.3 ± 0.5 |
| Utilization Score | |
| Below 0.1 (N, (%)) | 44 (73.3) |
| Above 0.1 (N, (%)) | 16 (26.7) |
| CD34+ Cell Dose (×105 cells/kg recipient weight) | 1.9 ± 0.2 |
| 0–4 years | 3.1 ± 0.5 |
| 5–17 years | 1.4 ± 0.5 |
| 18+ years | 0.9 ± 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parmar, G.; Green, M.; Mostert, K.; Lawless, T.; Dibdin, N.; Weiss, J.; Ganz, K.; Petraszko, T.; Seftel, M.D.; Allan, D.S. A Portrait of Cord Blood Units Distributed for Transplantation from Canadian Blood Services’ Cord Blood Bank: First Analysis. Curr. Oncol. 2022, 29, 9572-9581. https://doi.org/10.3390/curroncol29120752
Parmar G, Green M, Mostert K, Lawless T, Dibdin N, Weiss J, Ganz K, Petraszko T, Seftel MD, Allan DS. A Portrait of Cord Blood Units Distributed for Transplantation from Canadian Blood Services’ Cord Blood Bank: First Analysis. Current Oncology. 2022; 29(12):9572-9581. https://doi.org/10.3390/curroncol29120752
Chicago/Turabian StyleParmar, Gaganvir, Meagan Green, Karen Mostert, Tiffany Lawless, Nicholas Dibdin, Jason Weiss, Kathy Ganz, Tanya Petraszko, Matthew D. Seftel, and David S. Allan. 2022. "A Portrait of Cord Blood Units Distributed for Transplantation from Canadian Blood Services’ Cord Blood Bank: First Analysis" Current Oncology 29, no. 12: 9572-9581. https://doi.org/10.3390/curroncol29120752
APA StyleParmar, G., Green, M., Mostert, K., Lawless, T., Dibdin, N., Weiss, J., Ganz, K., Petraszko, T., Seftel, M. D., & Allan, D. S. (2022). A Portrait of Cord Blood Units Distributed for Transplantation from Canadian Blood Services’ Cord Blood Bank: First Analysis. Current Oncology, 29(12), 9572-9581. https://doi.org/10.3390/curroncol29120752