Surgical Management for Transposed Ovarian Recurrence of Cervical Cancer: A Systematic Review with Our Experience

 ,
,
Abstract
1. Introduction
2. Detailed Case Description
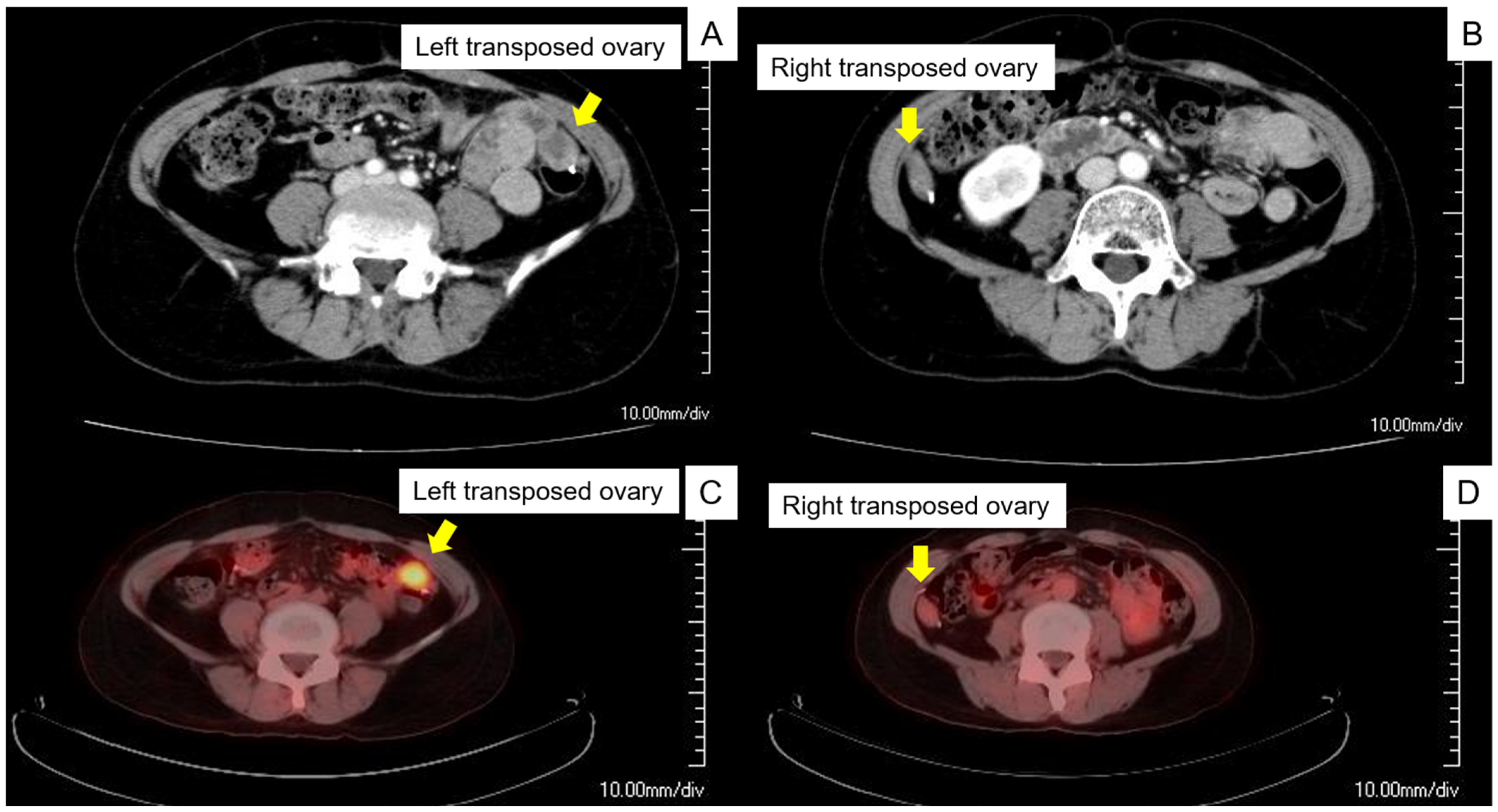
2.1. Preoperative Assessment
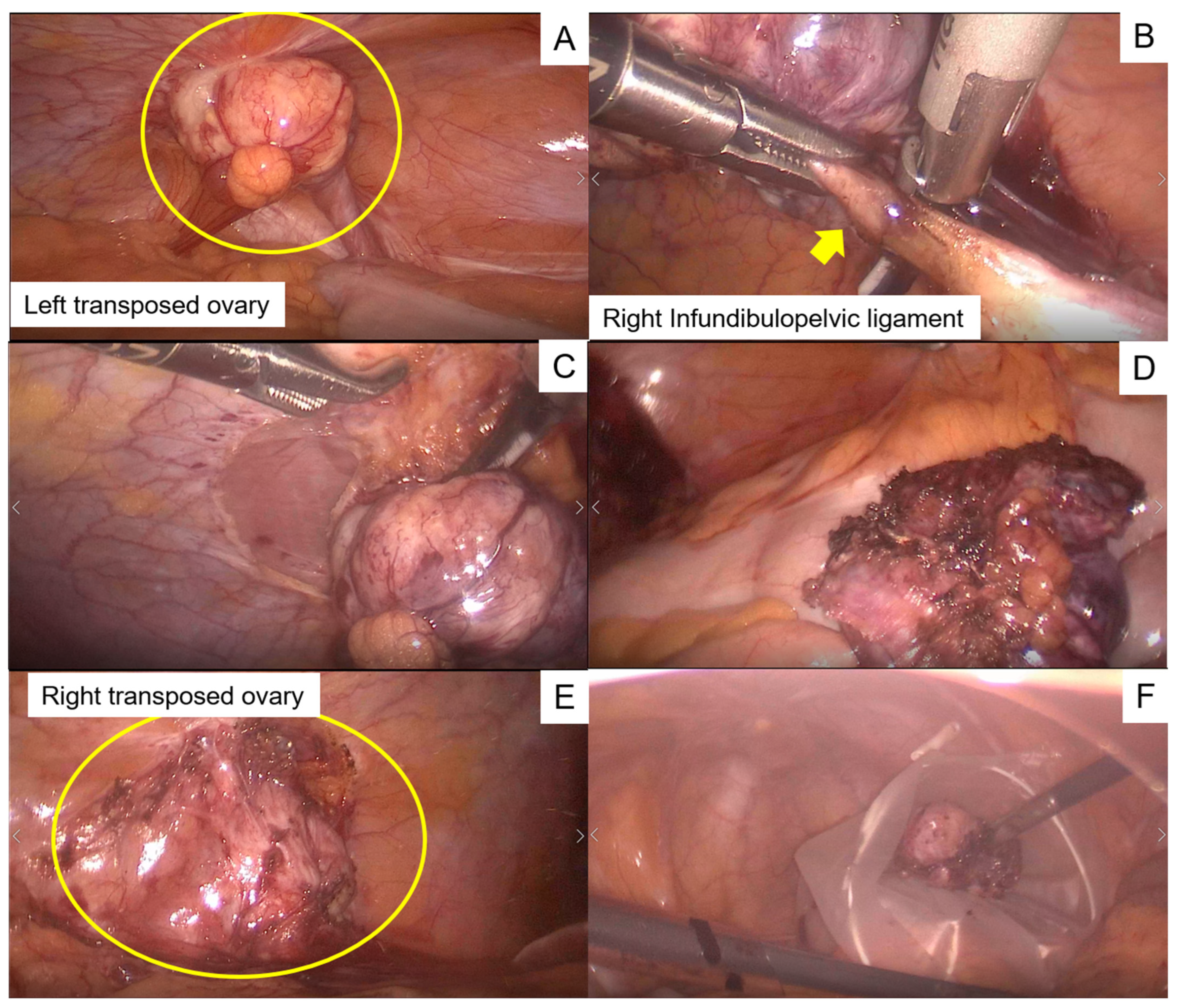
2.2. Intraoperative Findings
2.3. Postoperative Course
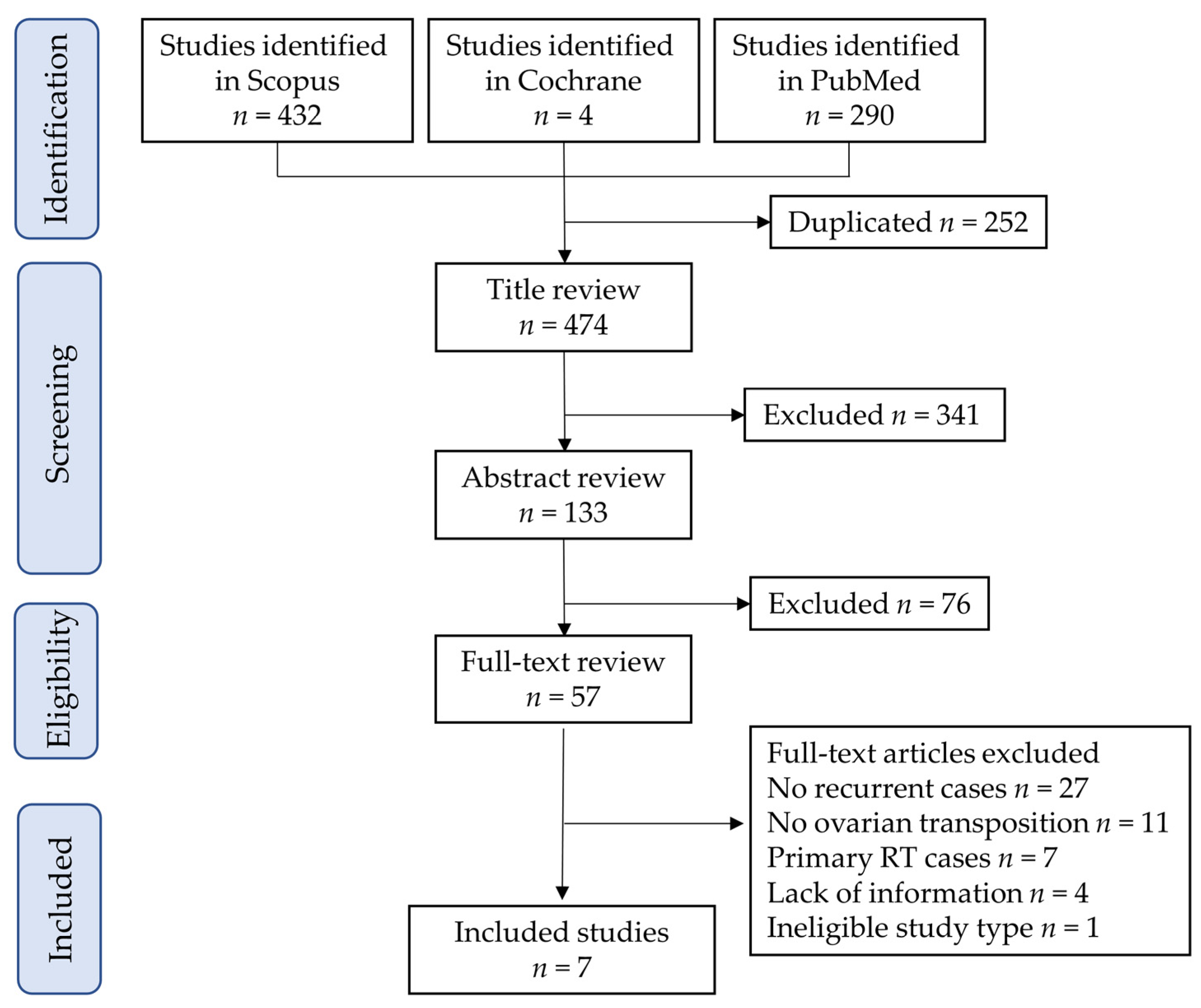
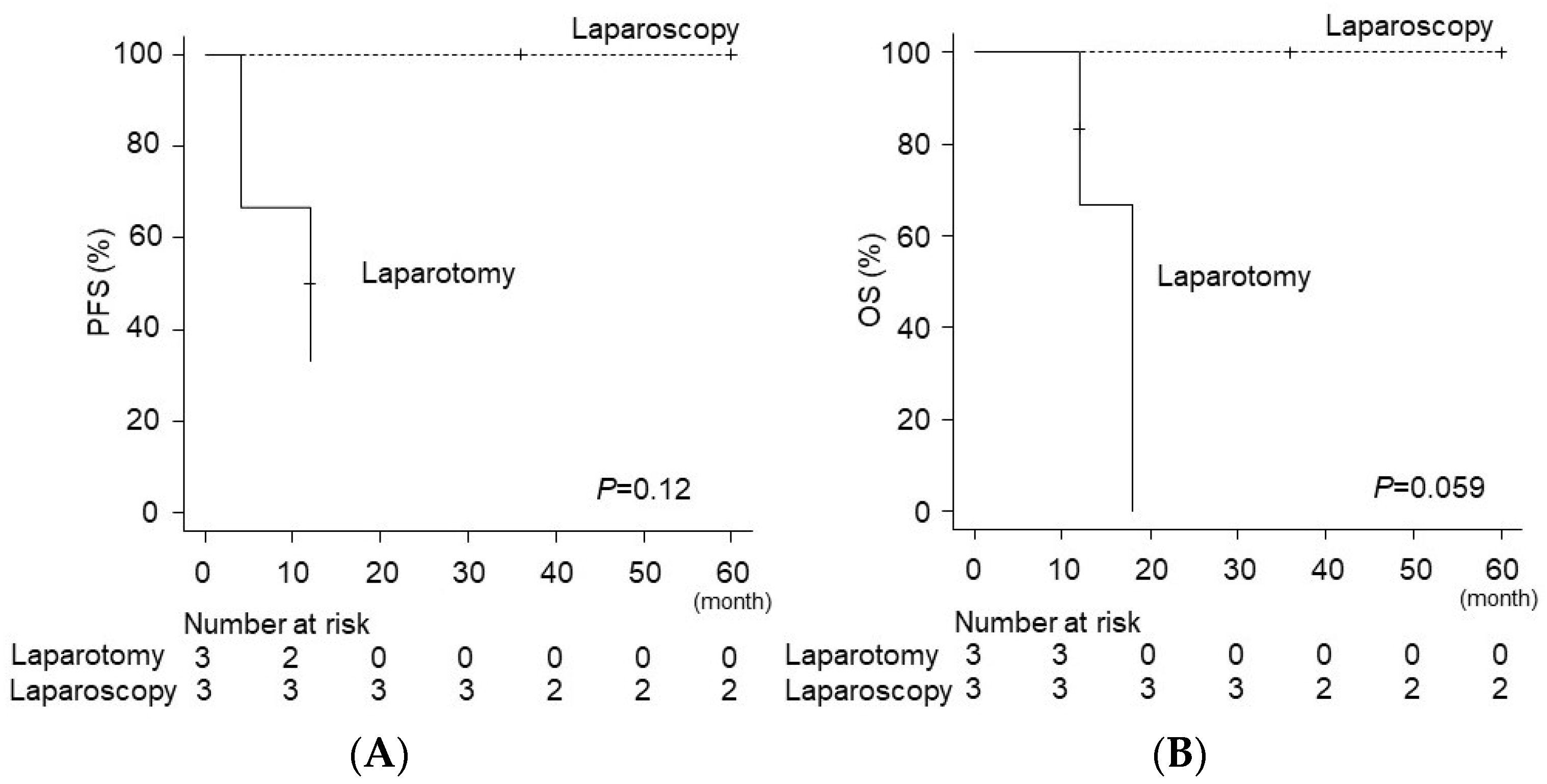
3. Systematic Review
4. Discussion
4.1. Principal Findings
4.2. Effect of Ovarian Metastasis in Cervical Cancer
4.3. Ovarian Transposition for Women with Cervical Cancer
4.4. Ovarian Preservation for Women with Cervical Cancer
4.5. Surgical Treatment for Metastatic Ovarian Tumors
4.6. Identification of Recurrence of Cervical Cancer in Transposed Ovary
4.7. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.A.; Jhingran, A.; Oaknin, A.; Denny, L. Cervical cancer. Lancet 2019, 393, 169–182. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Klar, M.; Mikami, M.; Shimada, M.; Grubbs, B.H.; Fujiwara, K.; Roman, L.D.; Matsuo, K. Management of Stage IIB Cervical Cancer: An Overview of the Current Evidence. Curr. Oncol. Rep. 2020, 22, 28. [Google Scholar] [CrossRef] [PubMed]
- Shimada, M.; Kigawa, J.; Nishimura, R.; Yamaguchi, S.; Kuzuya, K.; Nakanishi, T.; Suzuki, M.; Kita, T.; Iwasaka, T.; Terakawa, N. Ovarian metastasis in carcinoma of the uterine cervix. Gynecol. Oncol. 2006, 101, 234–237. [Google Scholar] [CrossRef]
- Gubbala, K.; Laios, A.; Gallos, I.; Pathiraja, P.; Haldar, K.; Ind, T. Outcomes of ovarian transposition in gynaecological cancers; a systematic review and meta-analysis. J. Ovarian Res. 2014, 7, 69. [Google Scholar] [CrossRef]
- Kjorstad, K.E.; Bond, B. Stage IB adenocarcinoma of the cervix: Metastatic potential and patterns of dissemination. Am. J. Obstet. Gynecol. 1984, 150, 297–299. [Google Scholar] [CrossRef]
- Tabata, M.; Ichinoe, K.; Sakuragi, N.; Shiina, Y.; Yamaguchi, T.; Mabuchi, Y. Incidence of ovarian metastasis in patients with cancer of the uterine cervix. Gynecol. Oncol. 1987, 28, 255–261. [Google Scholar] [CrossRef]
- Toki, N.; Tsukamoto, N.; Kaku, T.; Toh, N.; Saito, T.; Kamura, T.; Matsukuma, K.; Nakano, H. Microscopic ovarian metastasis of the uterine cervical cancer. Gynecol. Oncol. 1991, 41, 46–51. [Google Scholar] [CrossRef]
- Wu, H.S.; Yen, M.S.; Lai, C.R.; Ng, H.T. Ovarian metastasis from cervical carcinoma. Int. J. Gynaecol. Obstet. 1997, 57, 173–178. [Google Scholar] [CrossRef]
- Yamamoto, R.; Okamoto, K.; Yukiharu, T.; Kaneuchi, M.; Negishi, H.; Sakuragi, N.; Fujimoto, S. A study of risk factors for ovarian metastases in stage Ib-IIIb cervical carcinoma and analysis of ovarian function after a transposition. Gynecol. Oncol. 2001, 82, 312–316. [Google Scholar] [CrossRef]
- Nakanishi, T.; Wakai, K.; Ishikawa, H.; Nawa, A.; Suzuki, Y.; Nakamura, S.; Kuzuya, K. A comparison of ovarian metastasis between squamous cell carcinoma and adenocarcinoma of the uterine cervix. Gynecol. Oncol. 2001, 82, 504–509. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Wu, L.; Xing, H.; Yang, R.; Li, X.; Huang, K.; Jia, Y.; Zhang, Q.; Chen, Z.; Wang, S.; et al. Development of criteria for ovarian preservation in cervical cancer patients treated with radical surgery with or without neoadjuvant chemotherapy: A multicenter retrospective study and meta-analysis. Ann. Surg. Oncol. 2013, 20, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Shimada, M.; Yamaguchi, S.; Kanao, H.; Nakanishi, T.; Saito, T.; Kamiura, S.; Iwata, T.; Mikami, M.; Sugiyama, T. Identifying a candidate population for ovarian conservation in young women with clinical stage IB-IIB cervical cancer. Int. J. Cancer 2018, 142, 1022–1032. [Google Scholar] [CrossRef] [PubMed]
- Bizzarri, N.; Pedone Anchora, L.; Kucukmetin, A.; Ratnavelu, N.; Korompelis, P.; Fedele, C.; Bruno, M.; Di Fiore, G.L.M.; Fagotti, A.; Fanfani, F.; et al. Risk of ovarian recurrence after ovarian conservation in early-stage cervical cancer treated with radical surgery: A propensity match analysis. Eur. J. Surg. Oncol. 2021, 47, 2158–2165. [Google Scholar] [CrossRef] [PubMed]
- Touhami, O.; Plante, M. Should ovaries be removed or not in (early-stage) adenocarcinoma of the uterine cervix: A review. Gynecol. Oncol. 2015, 136, 384–388. [Google Scholar] [CrossRef]
- Wo, J.Y.; Viswanathan, A.N. Impact of radiotherapy on fertility, pregnancy, and neonatal outcomes in female cancer patients. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1304–1312. [Google Scholar] [CrossRef]
- Lushbaugh, C.C.; Casarett, G.W. The effects of gonadal irradiation in clinical radiation therapy: A review. Cancer 1976, 37, 1111–1125. [Google Scholar] [CrossRef]
- Buonomo, B.; Multinu, F.; Casarin, J.; Betella, I.; Zanagnolo, V.; Aletti, G.; Peccatori, F. Ovarian transposition in patients with cervical cancer prior to pelvic radiotherapy: A systematic review. Int. J. Gynecol. Cancer 2021, 31, 360–370. [Google Scholar] [CrossRef]
- Morice, P.; Juncker, L.; Rey, A.; El-Hassan, J.; Haie-Meder, C.; Castaigne, D. Ovarian transposition for patients with cervical carcinoma treated by radiosurgical combination. Fertil. Steril. 2000, 74, 743–748. [Google Scholar] [CrossRef]
- Wright, J.D. Minimal risk for minimally invasive hysterectomy for stage IA cervical cancer? Int. J. Gynecol. Cancer 2021, 31, 1104–1105. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Klar, M.; Chang, E.J.; Matsuzaki, S.; Maeda, M.; Zhang, R.H.; Roman, L.D.; Matsuo, K. Minimally Invasive Surgery and Surgical Volume-Specific Survival and Perioperative Outcome: Unmet Need for Evidence in Gynecologic Malignancy. J. Clin. Med. 2021, 10, 4787. [Google Scholar] [CrossRef] [PubMed]
- Kanao, H.; Aoki, Y.; Omi, M.; Nomura, H.; Tanigawa, T.; Okamoto, S.; Chang, E.J.; Kurita, T.; Netsu, S.; Matoda, M.; et al. Laparoscopic pelvic exenteration and laterally extended endopelvic resection for postradiation recurrent cervical carcinoma: Technical feasibility and short-term oncologic outcome. Gynecol. Oncol. 2021, 161, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Jochum, F.; Vermel, M.; Faller, E.; Boisrame, T.; Lecointre, L.; Akladios, C. Three and Five-Year Mortality in Ovarian Cancer after Minimally Invasive Compared to Open Surgery: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2507. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Nagase, Y.; Ueda, Y.; Kakuda, M.; Maeda, M.; Matsuzaki, S.; Kamiura, S. Placenta Previa Complicated with Endometriosis: Contemporary Clinical Management, Molecular Mechanisms, and Future Research Opportunities. Biomedicines 2021, 9, 1536. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Ueda, Y.; Nagase, Y.; Matsuzaki, S.; Kakuda, M.; Kakuda, S.; Sakaguchi, H.; Hisa, T.; Kamiura, S. Placenta Accreta Spectrum Disorder Complicated with Endometriosis: Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 390. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Nagase, Y.; Ueda, Y.; Lee, M.; Matsuzaki, S.; Maeda, M.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Endo, M.; et al. The association of endometriosis with placenta previa and postpartum hemorrhage: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2021, 3, 100417. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Nagase, Y.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Lee, M.; Matsuzaki, S.; Ueda, Y.; Tomimatsu, T.; Endo, M.; et al. Antenatal diagnosis of placenta accreta spectrum after in vitro fertilization-embryo transfer: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 9205. [Google Scholar] [CrossRef]
- Delotte, J.; Ferron, G.; Kuei, T.L.; Mery, E.; Gladieff, L.; Querleu, D. Laparoscopic management of an isolated ovarian metastasis on a transposed ovary in a patient treated for stage IB1 adenocarcinoma of the cervix. J. Minim. Invasive Gynecol. 2009, 16, 106–108. [Google Scholar] [CrossRef]
- Janse, J.A.; Sie-Go, D.M.; Schreuder, H.W. Ovarian metastasis in a transposed ovary 10 years after primary cervical cancer: The importance of histologic examination and review of literature. BMJ Case Rep. 2011, 2011, bcr0420114155. [Google Scholar] [CrossRef]
- Nguyen, L.; Brewer, C.A.; DiSaia, P.J. Ovarian metastasis of stage IB1 squamous cell cancer of the cervix after radical parametrectomy and oophoropexy. Gynecol. Oncol. 1998, 68, 198–200. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, T.; Ohishi, Y.; Fujita, T.; Higashihara, J.; Irie, T.; Hayashi, T. Metastatic carcinoma in a transposed ovary after radical hysterectomy for a stage 1B cervical adenosquamous cell carcinoma. Case report. Eur. J. Gynaecol. Oncol. 2000, 21, 383–386. [Google Scholar] [PubMed]
- Reisinger, S.A.; Palazzo, J.P.; Talerman, A.; Carlson, J.; Jahshan, A. Stage IB glassy cell carcinoma of the cervix diagnosed during pregnancy and recurring in a transposed ovary. Gynecol. Oncol. 1991, 42, 86–90. [Google Scholar] [CrossRef]
- Morice, P.; Haie-Meder, C.; Pautier, P.; Lhomme, C.; Castaigne, D. Ovarian metastasis on transposed ovary in patients treated for squamous cell carcinoma of the uterine cervix: Report of two cases and surgical implications. Gynecol. Oncol. 2001, 83, 605–607. [Google Scholar] [CrossRef] [PubMed]
- Parham, G.; Heppard, M.C.; DiSaia, P.J. Metastasis from a stage IB cervical adenocarcinoma in a transposed ovary: A case report and review of the literature. Gynecol. Oncol. 1994, 55, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Matsuzaki, S.; Chang, E.J.; Yasukawa, M.; Roman, L.D.; Matsuo, K. Surgical and oncologic outcomes of hyperthermic intraperitoneal chemotherapy for uterine leiomyosarcoma: A systematic review of literature. Gynecol. Oncol. 2021, 161, 70–77. [Google Scholar] [CrossRef]
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri: 2021 update. Int. J. Gynaecol. Obstet. 2021, 155 (Suppl. S1), 28–44. [Google Scholar] [CrossRef]
- Salvo, G.; Odetto, D.; Pareja, R.; Frumovitz, M.; Ramirez, P.T. Revised 2018 International Federation of Gynecology and Obstetrics (FIGO) cervical cancer staging: A review of gaps and questions that remain. Int. J. Gynecol. Cancer 2020, 30, 873–878. [Google Scholar] [CrossRef]
- Thomas, P.R.; Winstanly, D.; Peckham, M.J.; Austin, D.E.; Murray, M.A.; Jacobs, H.S. Reproductive and endocrine function in patients with Hodgkin’s disease: Effects of oophoropexy and irradiation. Br. J. Cancer 1976, 33, 226–231. [Google Scholar] [CrossRef][Green Version]
- Nahhas, W.A.; Nisce, L.Z.; D’Angio, G.J.; Lewis, J.L., Jr. Lateral ovarian transposition. Ovarian relocation in patients with Hodgkin’s disease. Obstet. Gynecol. 1971, 38, 785–788. [Google Scholar]
- Moawad, N.S.; Santamaria, E.; Rhoton-Vlasak, A.; Lightsey, J.L. Laparoscopic Ovarian Transposition Before Pelvic Cancer Treatment: Ovarian Function and Fertility Preservation. J. Minim. Invasive Gynecol. 2017, 24, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Cervical Cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Available online: http://www.nccn.org (accessed on 22 September 2022).
- Shuster, L.T.; Gostout, B.S.; Grossardt, B.R.; Rocca, W.A. Prophylactic oophorectomy in premenopausal women and long-term health. Menopause Int. 2008, 14, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Rocca, W.A.; Lohse, C.M.; Smith, C.Y.; Fields, J.A.; Machulda, M.M.; Mielke, M.M. Association of Premenopausal Bilateral Oophorectomy With Cognitive Performance and Risk of Mild Cognitive Impairment. JAMA Netw. Open 2021, 4, e2131448. [Google Scholar] [CrossRef] [PubMed]
- Thong, E.P.; Hart, R.J.; Teede, H.J.; Vincent, A.J.; Enticott, J.C. Increased mortality and non-cancer morbidity risk may be associated with early menopause and varies with aetiology: An exploratory population-based study using data-linkage. Maturitas 2022, 164, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Tuesley, K.M.; Protani, M.M.; Webb, P.M.; Dixon-Suen, S.C.; Wilson, L.F.; Stewart, L.M.; Jordan, S.J. Hysterectomy with and without oophorectomy and all-cause and cause-specific mortality. Am. J. Obstet. Gynecol. 2020, 223, 723.e1–723.e16. [Google Scholar] [CrossRef]
- Atsma, F.; Bartelink, M.L.; Grobbee, D.E.; van der Schouw, Y.T. Postmenopausal status and early menopause as independent risk factors for cardiovascular disease: A meta-analysis. Menopause 2006, 13, 265–279. [Google Scholar] [CrossRef]
- Parker, W.H.; Broder, M.S.; Chang, E.; Feskanich, D.; Farquhar, C.; Liu, Z.; Shoupe, D.; Berek, J.S.; Hankinson, S.; Manson, J.E. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the nurses’ health study. Obstet. Gynecol. 2009, 113, 1027–1037. [Google Scholar] [CrossRef]
- Honigberg, M.C.; Zekavat, S.M.; Aragam, K.; Finneran, P.; Klarin, D.; Bhatt, D.L.; Januzzi, J.L., Jr.; Scott, N.S.; Natarajan, P. Association of Premature Natural and Surgical Menopause With Incident Cardiovascular Disease. JAMA 2019, 322, 2411–2421. [Google Scholar] [CrossRef]
- Ryan, N.A.; McMahon, R.F.; Ramchander, N.C.; Seif, M.W.; Evans, D.G.; Crosbie, E.J. Lynch syndrome for the gynaecologist. Obstet. Gynaecol. J. Contin. Prof. Dev. R. Coll. Obstet. Gynaecol. 2021, 23, 9–20. [Google Scholar] [CrossRef]
- Shulman, L.P. Hereditary breast and ovarian cancer (HBOC): Clinical features and counseling for BRCA1 and BRCA2, Lynch syndrome, Cowden syndrome, and Li-Fraumeni syndrome. Obstet. Gynecol. Clin. N. Am. 2010, 37, 109–133. [Google Scholar] [CrossRef]
- Konstantinopoulos, P.A.; Norquist, B.; Lacchetti, C.; Armstrong, D.; Grisham, R.N.; Goodfellow, P.J.; Kohn, E.C.; Levine, D.A.; Liu, J.F.; Lu, K.H.; et al. Germline and Somatic Tumor Testing in Epithelial Ovarian Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, 1222–1245. [Google Scholar] [CrossRef] [PubMed]
- Mandelbaum, R.S.; Matsuzaki, S.; Sangara, R.N.; Klar, M.; Matsushima, K.; Roman, L.D.; Paulson, R.J.; Wright, J.D.; Matsuo, K. Paradigm shift from tubal ligation to opportunistic salpingectomy at cesarean delivery in the United States. Am. J. Obstet. Gynecol. 2021, 225, 399.e1–399.e32. [Google Scholar] [CrossRef]
- Banerjee, S.; Moore, K.N.; Colombo, N.; Scambia, G.; Kim, B.G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; et al. Maintenance olaparib for patients with newly diagnosed advanced ovarian cancer and a BRCA mutation (SOLO1/GOG 3004): 5-year follow-up of a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2021, 22, 1721–1731. [Google Scholar] [CrossRef]
- Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W., Jr.; Kubik, M.; Landefeld, C.S.; et al. Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2019, 322, 652–665. [Google Scholar] [CrossRef]
- de Waal, Y.R.; Thomas, C.M.; Oei, A.L.; Sweep, F.C.; Massuger, L.F. Secondary ovarian malignancies: Frequency, origin, and characteristics. Int. J. Gynecol. Cancer 2009, 19, 1160–1165. [Google Scholar] [CrossRef]
- Uccella, S.; Franchi, M.P.; Cianci, S.; Zorzato, P.C.; Bertoli, F.; Alletti, S.G.; Ghezzi, F.; Scambia, G. Laparotomy vs. minimally invasive surgery for ovarian cancer recurrence: A systematic review. Gland Surg. 2020, 9, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Berek, J.S.; Renz, M.; Kehoe, S.; Kumar, L.; Friedlander, M. Cancer of the ovary, fallopian tube, and peritoneum: 2021 update. Int. J. Gynaecol. Obstet. 2021, 155 (Suppl. S1), 61–85. [Google Scholar] [CrossRef]
- Matsuo, K.; Huang, Y.; Matsuzaki, S.; Klar, M.; Roman, L.D.; Sood, A.K.; Wright, J.D. Minimally Invasive Surgery and Risk of Capsule Rupture for Women With Early-Stage Ovarian Cancer. JAMA Oncol. 2020, 6, 1110–1113. [Google Scholar] [CrossRef]
- Ataseven, B.; Grimm, C.; Harter, P.; Heikaus, S.; Heitz, F.; Traut, A.; Prader, S.; Kahl, A.; Schneider, S.; Kurzeder, C.; et al. Prognostic Impact of Port-Site Metastasis After Diagnostic Laparoscopy for Epithelial Ovarian Cancer. Ann. Surg. Oncol. 2016, 23, 834–840. [Google Scholar] [CrossRef]
- Yada-Hashimoto, N.; Yamamoto, T.; Kamiura, S.; Seino, H.; Ohira, H.; Sawai, K.; Kimura, T.; Saji, F. Metastatic ovarian tumors: A review of 64 cases. Gynecol. Oncol. 2003, 89, 314–317. [Google Scholar] [CrossRef]
- Jo, K.H.; Kim, S.; Hwang, S.H.; Jeong, Y.H.; Nam, E.J.; Kang, W.J. Characteristics of surgically transposed ovaries on (18)F-FDG PET/CT among patients with cancer. Ann. Nucl. Med. 2021, 35, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Davidson, T.; Komisar, O.; Korach, J.; Felder, S.; Apter, S.; Ben-Haim, S.; Perri, T. Physiologic uptake of 18F-FDG in transposed ovaries may mimic metastasis on 18F-FDG PET/CT imaging. Nucl. Med. Commun. 2018, 39, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Laios, A.; Otify, M.; Papadopoulou, A.; Gallos, I.D.; Ind, T. Outcomes of ovarian transposition in cervical cancer; an updated meta-analysis. BMC Womens Health 2022, 22, 305. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Age | Stage † | Hist | Rec | CC | Diagnosis | Surgery | Size | Adj | Rec | PFS | OS | Status |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Present study | 2022 | 45 | IIB | SCC | 36M | None | PET-CT | LSC | 3 cm | CT | No | 60M | 60M | NED |
| Janse [30] | 2011 | 53 | IB | ASC | 120M | Abd pain | US | LSC | 6 cm | No | No | 36M | 36M | NED |
| Delotte [29] | 2009 | 36 | IB2 | ADC | 13M | Abd pain | MRI | LSC | 4.5 cm | No | No | 60M | 60M | NED |
| Morice [34] | 2001 | 34 | IB | SCC | 36M | Abd pain | Palp | - | 10 cm | - | Yes | - | 15M | DOD |
| Morice [34] | 2001 | 34 | IB | SCC | 36M | None | Palp | - | 10 cm | CCRT | - | - | - | - |
| Shigematsu [32] | 2000 | 41 | IB3 | ASC | 24M | None | CT | Open | 7 cm | CT | No | 12M | 12M | NED |
| Nguyen [31] | 1998 | 43 | IB | SCC | 98M | Abd pain | CT | Open | 7 cm | RT | Yes | 4M | 18M | DOD |
| Parham [35] | 1994 | 33 | IB2 | ADC | 7M | Abd pain | CT | Open | 6 cm | RT | Yes | 12M | 12M | DOD |
| Reisinger [33] | 1991 | 31 | IB3 | Glassy | 1M | Abd pain | CT | - | 5 cm | RT | Yes | 0 M | 5M | DOD |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maeda, M.; Hisa, T.; Kurahashi, H.; Hayashida, H.; Lee, M.; Kakubari, R.; Matsuzaki, S.; Mabuchi, S.; Kamiura, S. Surgical Management for Transposed Ovarian Recurrence of Cervical Cancer: A Systematic Review with Our Experience. Curr. Oncol. 2022, 29, 7158-7170. https://doi.org/10.3390/curroncol29100563
Maeda M, Hisa T, Kurahashi H, Hayashida H, Lee M, Kakubari R, Matsuzaki S, Mabuchi S, Kamiura S. Surgical Management for Transposed Ovarian Recurrence of Cervical Cancer: A Systematic Review with Our Experience. Current Oncology. 2022; 29(10):7158-7170. https://doi.org/10.3390/curroncol29100563
Chicago/Turabian StyleMaeda, Michihide, Tsuyoshi Hisa, Hiroki Kurahashi, Harue Hayashida, Misooja Lee, Reisa Kakubari, Shinya Matsuzaki, Seiji Mabuchi, and Shoji Kamiura. 2022. "Surgical Management for Transposed Ovarian Recurrence of Cervical Cancer: A Systematic Review with Our Experience" Current Oncology 29, no. 10: 7158-7170. https://doi.org/10.3390/curroncol29100563
APA StyleMaeda, M., Hisa, T., Kurahashi, H., Hayashida, H., Lee, M., Kakubari, R., Matsuzaki, S., Mabuchi, S., & Kamiura, S. (2022). Surgical Management for Transposed Ovarian Recurrence of Cervical Cancer: A Systematic Review with Our Experience. Current Oncology, 29(10), 7158-7170. https://doi.org/10.3390/curroncol29100563