Impact of Nutrition Counseling in Head and Neck Cancer Sufferers Undergoing Antineoplastic Therapy: A Randomized Controlled Pilot Study

Abstract
1. Introduction
2. Materials and Methods
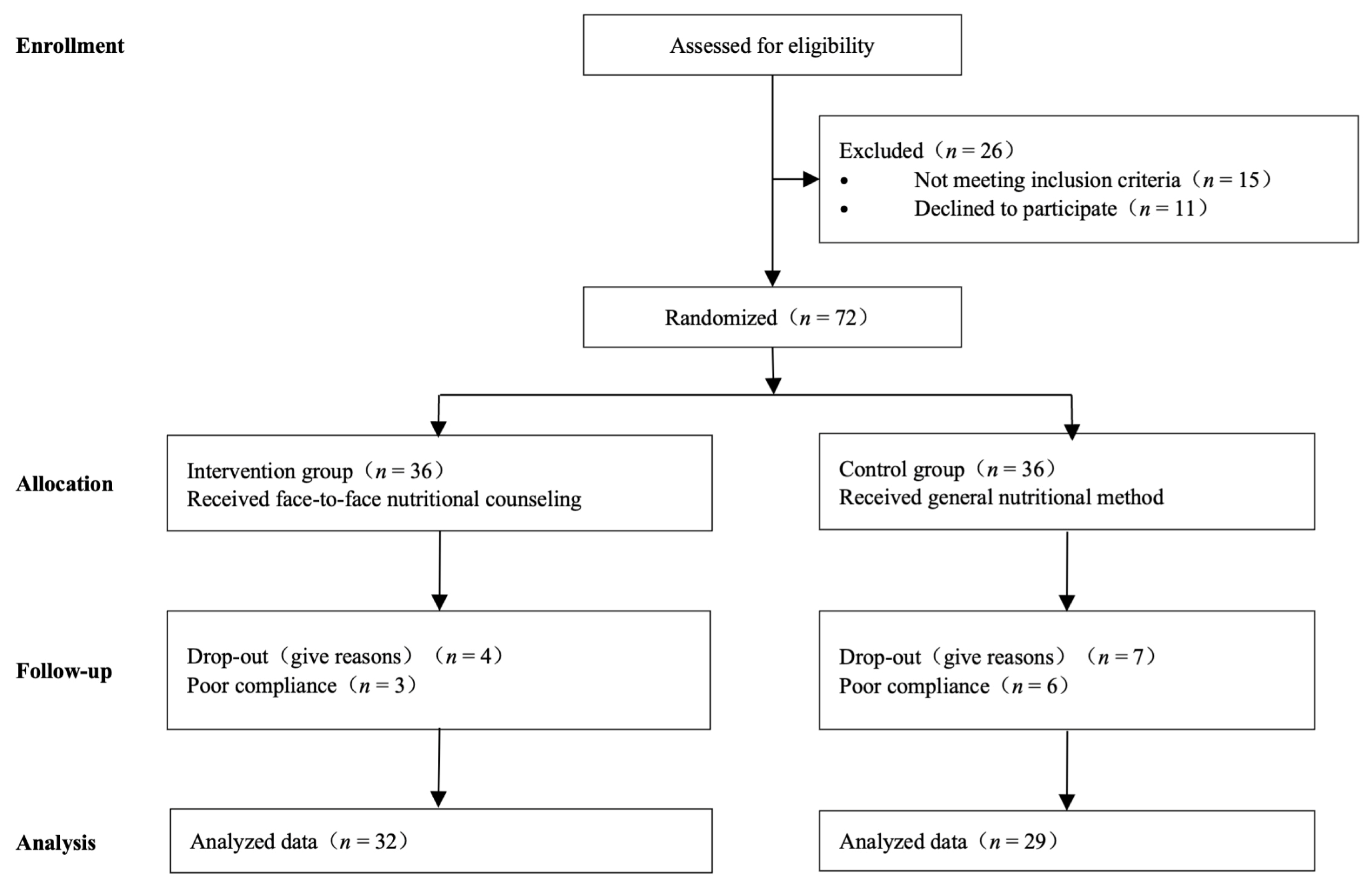
2.1. Patients
2.2. Definitive Concurrent Chemo-Radiotherapy
2.3. Nutrition Counseling
2.4. Follow Up
2.5. Statistical Analyses
3. Results
3.1. Patient Demographics and Clinical Characteristics
3.2. Nutrient Intake
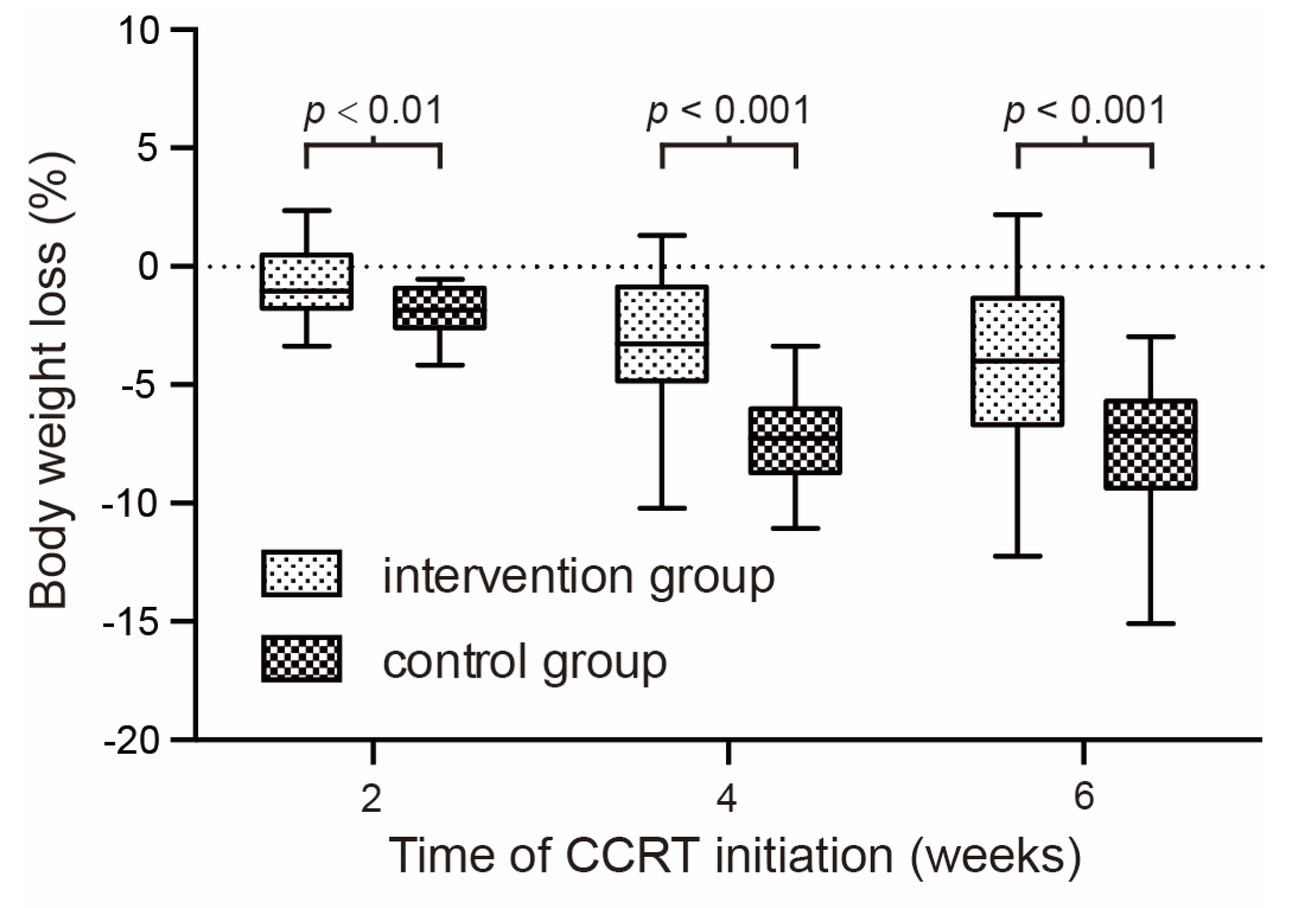
3.3. Physical State Assessment
3.4. Mental State Assessment
3.5. Results of Nutritional Testing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef]
- Demling, R.H. Nutrition, anabolism, and the wound healing process: An overview. Eplasty 2009, 9, e9. [Google Scholar] [PubMed]
- Ho, Y.W.; Yeh, K.Y.; Hsueh, S.W.; Hung, C.Y.; Lu, C.H.; Tsang, N.M.; Wang, H.M.; Hung, Y.S.; Chou, W.C. Impact of early nutrition counseling in head and neck cancer patients with normal nutritional status. Supportive Care Cancer 2021, 29, 2777–2785. [Google Scholar] [CrossRef]
- Kubrak, C.; Martin, L.; Gramlich, L.; Scrimger, R.; Jha, N.; Debenham, B.; Chua, N.; Walker, J.; Baracos, V.E. Prevalence and prognostic significance of malnutrition in patients with cancers of the head and neck. Clin. Nutr. 2020, 39, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.B.; Isenring, E.; Brown, B. Nutrition and swallowing therapy strategies for patients with head and neck cancer. Nutrition 2020, 69, 110548. [Google Scholar] [CrossRef]
- Müller-Richter, U.; Betz, C.; Hartmann, S.; Brands, R.C. Nutrition management for head and neck cancer patients improves clinical outcome and survival. Nutr. Res. 2017, 48, 1–8. [Google Scholar] [CrossRef]
- Neoh, M.K.; Abu Zaid, Z.; Mat Daud, Z.A.; Md Yusop, N.B.; Ibrahim, Z.; Abdul Rahman, Z.; Jamhuri, N. Changes in Nutrition Impact Symptoms, Nutritional and Functional Status during Head and Neck Cancer Treatment. Nutrients 2020, 12, 1225. [Google Scholar] [CrossRef] [PubMed]
- Chindapasirt, J. Sarcopenia in Cancer Patients. Asian Pac. J. Cancer Prev. APJCP 2015, 16, 8075–8077. [Google Scholar] [CrossRef]
- Fattouh, M.; Chang, G.Y.; Ow, T.J.; Shifteh, K.; Rosenblatt, G.; Patel, V.M.; Smith, R.V.; Prystowsky, M.B.; Schlecht, N.F. Association between pretreatment obesity, sarcopenia, and survival in patients with head and neck cancer. Head Neck 2019, 41, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Gama, R.R.; Song, Y.; Zhang, Q.; Brown, M.C.; Wang, J.; Habbous, S.; Tong, L.; Huang, S.H.; O’sullivan, B.; Waldron, J.; et al. Body mass index and prognosis in patients with head and neck cancer. Head Neck 2017, 39, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, D.; Laszlo, M.; Provisor, A.; Yu, A. Nutrition Management for the Head and Neck Cancer Patient. Cancer Treat. Res. 2018, 174, 187–208. [Google Scholar] [PubMed]
- Do Nascimento Santos Lima, E.; Ferreira, I.B.; Lajolo, P.P.; Paiva, C.E.; De Paiva Maia, Y.C.; Das Graças Pena, G. Health-related quality of life became worse in short-term during treatment in head and neck cancer patients: A prospective study. Health Qual. Life Outcomes 2020, 18, 307. [Google Scholar] [CrossRef] [PubMed]
- Gosak, M.; Gradišar, K.; Rotovnik Kozjek, N.; Strojan, P. Psychological distress and nutritional status in head and neck cancer patients: A pilot study. Eur Arch Otorhinolaryngol. 2020, 277, 1211–1217. [Google Scholar] [CrossRef] [PubMed]
- Duc, S.; Rainfray, M.; Soubeyran, P.; Fonck, M.; Blanc, J.F.; Ceccaldi, J.; Cany, L.; Brouste, V.; Mathoulin-Pélissier, S. Predictive factors of depressive symptoms of elderly patients with cancer receiving first-line chemotherapy. Psycho-Oncol. 2017, 26, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Kam, D.; Salib, A.; Gorgy, G.; Patel, T.D.; Carniol, E.T.; Eloy, J.A.; Baredes, S.; Park, R.C. Incidence of Suicide in Patients with Head and Neck Cancer. JAMA Otolaryngol.—Head Neck Surg. 2015, 141, 1075–1081. [Google Scholar] [CrossRef] [PubMed]
- Kiss, N.; Gilliland, S.; Quinn, P.; Atkins, L.; Black, J.; Frowen, J. Evaluating the effectiveness of a nutrition assistant role in a head and neck cancer clinic. Nutr. Diet. J. Dietit. Assoc. Aust. 2019, 76, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Vangelov, B.; Venchiarutti, R.L.; Smee, R.I. Critical weight loss in patients with oropharynx cancer during radiotherapy (± chemotherapy). Nutr. Cancer 2017, 69, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Wang, T.J.; Chu, P.Y. Predictors of weight loss during and after radiotherapy in patients with head and neck cancer: A longitudinal study. Eur. J. Oncol. Nurs. 2019, 39, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Mulasi, U.; Vock, D.M.; Jager-Wittenaar, H.; Teigen, L.; Kuchnia, A.J.; Jha, G.; Fujioka, N.; Rudrapatna, V.; Patel, M.R.; Earthman, C.P. Nutrition Status and Health-Related Quality of Life Among Outpatients with Advanced Head and Neck Cancer. Nutr. Clin. Pract. 2020, 35, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.R.; Pilz, W.; Hoebers, F.J.P.; Leeters, I.P.M.; Schols, A.; Willemsen, A.C.H.; Winkens, B.; Baijens, L.W.J. Malnutrition screening in head and neck cancer patients with oropharyngeal dysphagia. Clin. Nutr. ESPEN 2021, 44, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Momoki, C.; Okada, G.; Matsumoto, Y.; Yasui, Y.; Habu, D.; Matsuda, Y.; Lee, S.; Osugi, H. Preoperative Depressive Mood of Patients with Esophageal Cancer Might Delay Recovery From Operation-Related Malnutrition. J. Clin. Med. Res. 2019, 11, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Westin, T.; Jansson, A.; Zenckert, C.; Hällström, T.; Edström, S. Mental depression is associated with malnutrition in patients with head and neck cancer. Arch. Otolaryngol.—Head Neck Surg. 1988, 114, 1449–1453. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Category | Intervention Group (n = 32) | Control Group (n = 29) | p Value |
|---|---|---|---|
| Age | 51.7 ± 12.9 | 56.0 ± 8.3 | 0.12 |
| Sex | |||
| Male | 27 | 23 | 0.74 |
| Female | 5 | 6 | |
| Height (m) | |||
| Male | 1.68 ± 0.07 | 1.66 ± 0.07 | 0.49 |
| Female | 1.59 ± 0.07 | 1.55 ± 0.05 | 0.19 |
| Weight (kg) | |||
| Male | 69.6 ± 11.6 | 66.8 ± 9.8 | 0.45 |
| Female | 65.1 ± 10.3 | 58.3 ± 6.4 | 0.22 |
| Calorie intake (kcal/d) | 1642.1 ± 183.0 | 1614.1 ± 201.5 | 0.57 |
| Protein intake (g/d) | 54.3 ± 6.9 | 52.8 ± 6.8 | 0.40 |
| Energy nitrogen ratio | 190.2 ± 16.9 | 191.4 ± 8.3 | 0.73 |
| HADS-A score | 5.8 ± 1.3 | 5.3 ± 1.8 | 0.31 |
| HADS-D score | 4.3 ± 1.7 | 4.3 ± 1.2 | 0.94 |
| KPS score | 91.6 ± 7.7 | 91.0 ± 6.7 | 0.78 |
| Educational level | |||
| High school graduate | 9 | 6 | 0.56 |
| Less than high school | 23 | 23 | |
| Tumor site | |||
| Nasopharynx | 27 | 24 | 1.00 |
| Hypo-pharynx | 1 | 2 | |
| Tonsil | 1 | 0 | |
| Cervical lymph node | 0 | 1 | |
| Tongue | 0 | 1 | |
| Larynx | 2 | 1 | |
| Oropharynx | 1 | 0 | |
| Nutrition support method | |||
| Dietary | 9 | 7 | 0.732 |
| ONS | 21 | 20 | |
| Tube feeding | 2 | 2 |
| Category | Second Week | Fourth Week | Sixth Week | F | p Value |
|---|---|---|---|---|---|
| Calorie difference | |||||
| Intervention group (n = 32) | −136.2 ± 108.5 | −308.2 ± 130.1 | −72.0 ± 122.1 | 21.32 | 0.00 |
| Control group (n = 29) | −150.7 ± 77.6 | −466.8 ± 126.0 | −251.0 ± 113.0 | ||
| Protein difference | |||||
| Intervention group (n = 32) | 9.1 ± 4.4 | 2.3 ± 3.9 | 12.6 ± 4.7 | 223.71 | 0.00 |
| Control group (n = 29) | −5.9 ± 4.5 | −15.0 ± 5.1 | −6.2 ± 6.7 | ||
| Energy nitrogen ratio | |||||
| Intervention group (n = 32) | 149.3 ± 13.3 | 147.7 ± 10.6 | 147.5 ± 11.8 | 190.56 | 0.00 |
| Control group (n = 29) | 195.9 ± 12.6 | 190.4 ± 19.0 | 184.0 ± 25.0 |
| Category | Second Week | Fourth Week | Sixth Week | F | p Value |
|---|---|---|---|---|---|
| Weight | |||||
| Intervention group (n = 32) | 68.3 ± 10.8 | 66.7 ± 10.3 | 66.1 ± 10.3 | 4.86 | 0.03 |
| Control group (n = 29) | 63.9 ± 9.8 | 60.2 ± 9.5 | 60.0 ± 9.0 |
| Category | Second Week | Fourth Week | Sixth Week | F | p Value |
|---|---|---|---|---|---|
| KPS score | |||||
| Intervention group (n = 32) | 81.3 ± 6.6 | 70.6 ± 6.7 | 65.6 ± 5.0 | 8.16 | 0.01 |
| Control group (n = 29) | 78.6 ± 7.9 | 66.6 ± 6.7 | 62.1 ± 4.9 |
| Category | Second Week | Fourth Week | Sixth Week | F | p Value |
|---|---|---|---|---|---|
| HADS-A score | |||||
| Intervention group (n = 32) | 4.6 ± 1.5 | 5.5 ± 1.8 | 3.6 ± 1.0 | 8.77 | 0.00 |
| Control group (n = 29) | 5.2 ± 1.5 | 6.3 ± 1.1 | 4.5 ± 1.0 | ||
| HADS-D score | |||||
| Intervention group (n = 32) | 3.7 ± 0.8 | 4.8 ± 1.2 | 3.8 ± 1.2 | 6.97 | 0.01 |
| Control group (n = 29) | 3.8 ± 1.0 | 5.5 ± 1.2 | 4.8 ± 1.2 |
| Category | Intervention Group (n = 32) | Control Group (n = 29) | t | p Value | |
|---|---|---|---|---|---|
| TP (g/L) | Baseline level | 70.4 ± 11.7 | 73.6 ± 5.9 | −1.32 | 0.19 |
| Deltas against the baseline | 0.7 ± 13.0 | −5.5 ± 6.9 | 2.31 | 0.02 | |
| ALB (g/L) | Baseline level | 42.8 ± 3.1 | 42.0 ± 2.9 | 1.03 | 0.31 |
| Deltas against the baseline | −1.4 ± 3.4 | −3.1 ± 2.9 | 2.06 | 0.04 | |
| TF (g/L) | Baseline level | 2.0 ± 0.4 | 2.1 ± 0.3 | −0.44 | 0.67 |
| Deltas against the baseline | −0.1 ± 0.5 | −0.3 ± 0.4 | 2.19 | 0.03 | |
| PA (mg/L) | Baseline level | 251.8 ± 59.2 | 232.0 ± 68.3 | 1.20 | 0.24 |
| Deltas against the baseline | −26.4 ± 71.3 | −56.7 ± 62.5 | 1.75 | 0.08 | |
| TSF (mm) | Baseline level | 136.3 ± 15.7 | 133.1 ± 18.8 | −0.90 | 0.38 |
| Deltas against the baseline | −6.0 ± 10.5 | −9.8 ± 12.4 | 2.01 | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dai, W.; Wang, S.-A.; Wang, K.; Chen, C.; Wang, J.; Chen, X.; Yan, J. Impact of Nutrition Counseling in Head and Neck Cancer Sufferers Undergoing Antineoplastic Therapy: A Randomized Controlled Pilot Study. Curr. Oncol. 2022, 29, 6947-6955. https://doi.org/10.3390/curroncol29100546
Dai W, Wang S-A, Wang K, Chen C, Wang J, Chen X, Yan J. Impact of Nutrition Counseling in Head and Neck Cancer Sufferers Undergoing Antineoplastic Therapy: A Randomized Controlled Pilot Study. Current Oncology. 2022; 29(10):6947-6955. https://doi.org/10.3390/curroncol29100546
Chicago/Turabian StyleDai, Wangshu, Shu-An Wang, Kongcheng Wang, Chen Chen, Juan Wang, Xiaotian Chen, and Jing Yan. 2022. "Impact of Nutrition Counseling in Head and Neck Cancer Sufferers Undergoing Antineoplastic Therapy: A Randomized Controlled Pilot Study" Current Oncology 29, no. 10: 6947-6955. https://doi.org/10.3390/curroncol29100546
APA StyleDai, W., Wang, S.-A., Wang, K., Chen, C., Wang, J., Chen, X., & Yan, J. (2022). Impact of Nutrition Counseling in Head and Neck Cancer Sufferers Undergoing Antineoplastic Therapy: A Randomized Controlled Pilot Study. Current Oncology, 29(10), 6947-6955. https://doi.org/10.3390/curroncol29100546