Understanding the Attitudes and Beliefs of Oncologists Regarding the Transitioning and Sharing of Survivorship Care



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design, Setting and Participants
2.2. Survey
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Demographics
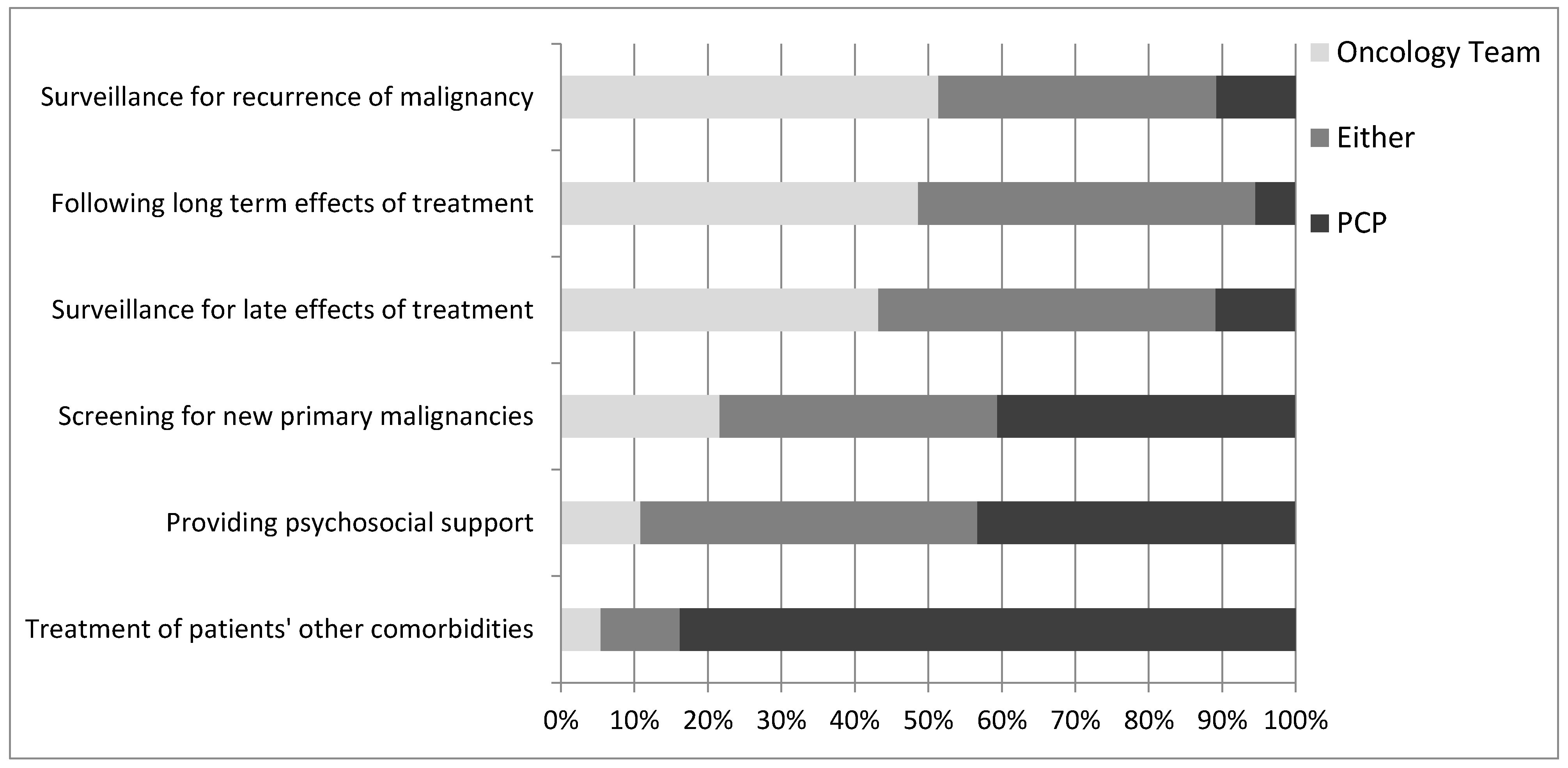
3.2. Current Self-Reported Practice
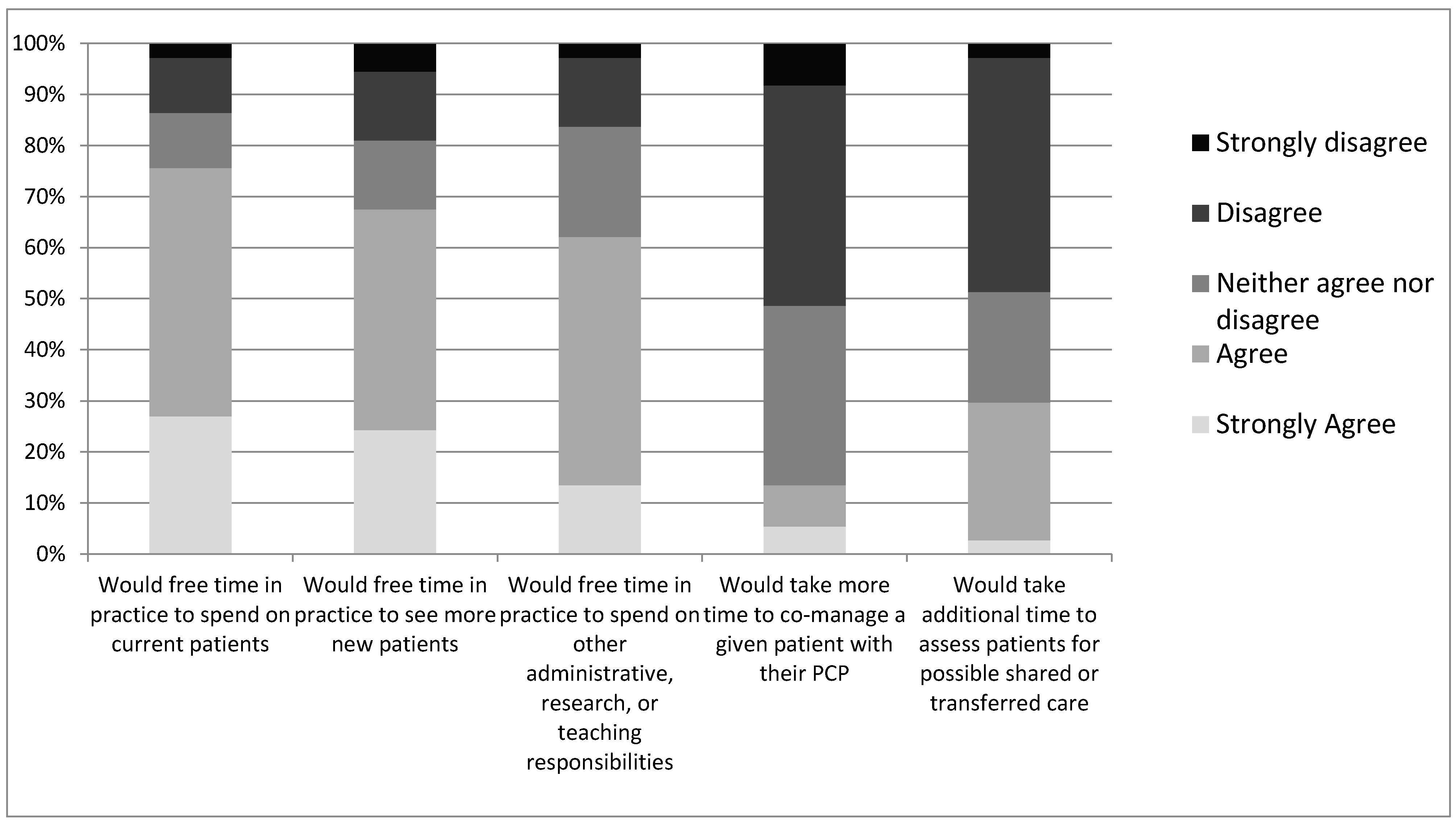
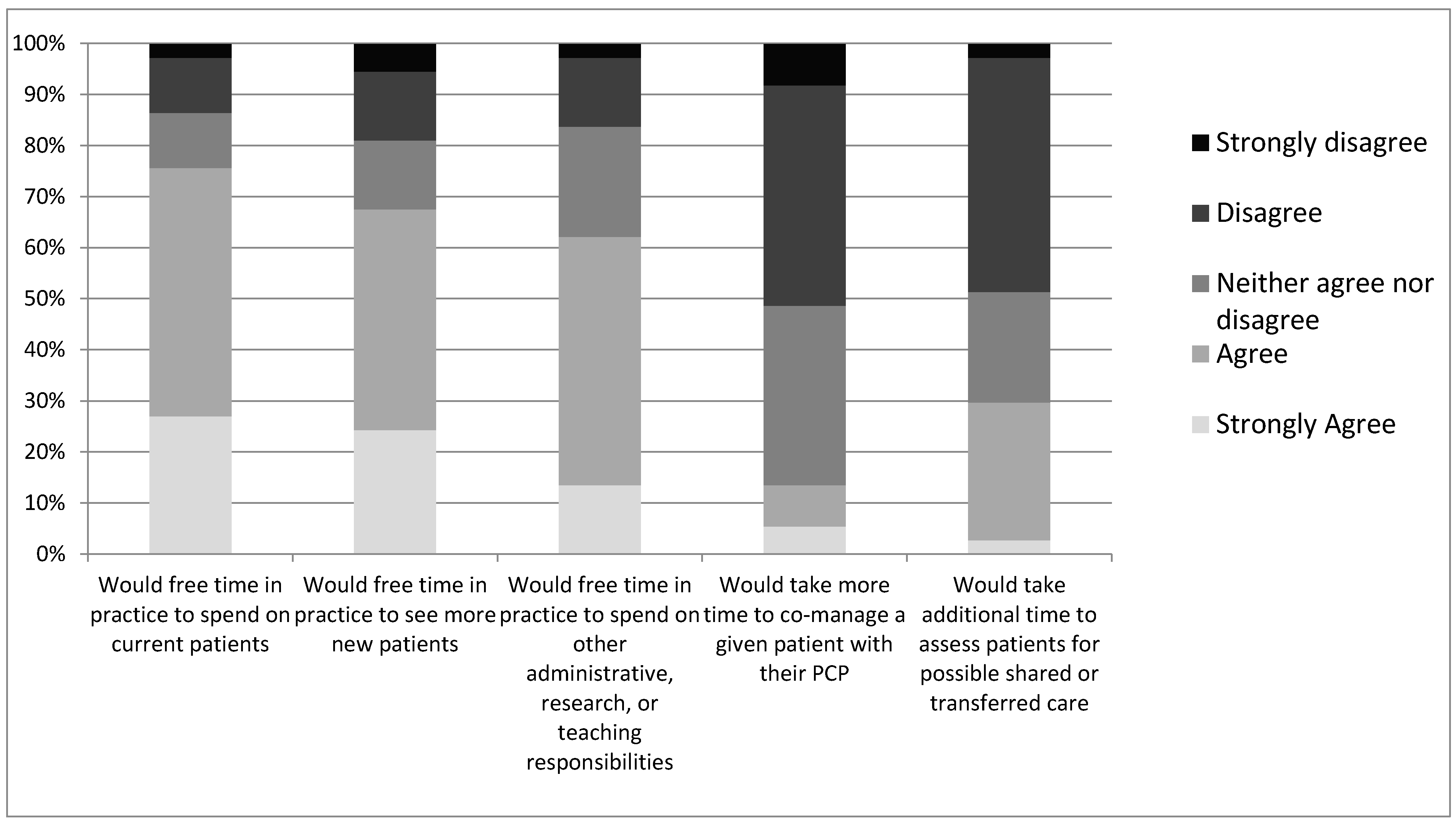
3.3. Attitudes and Beliefs
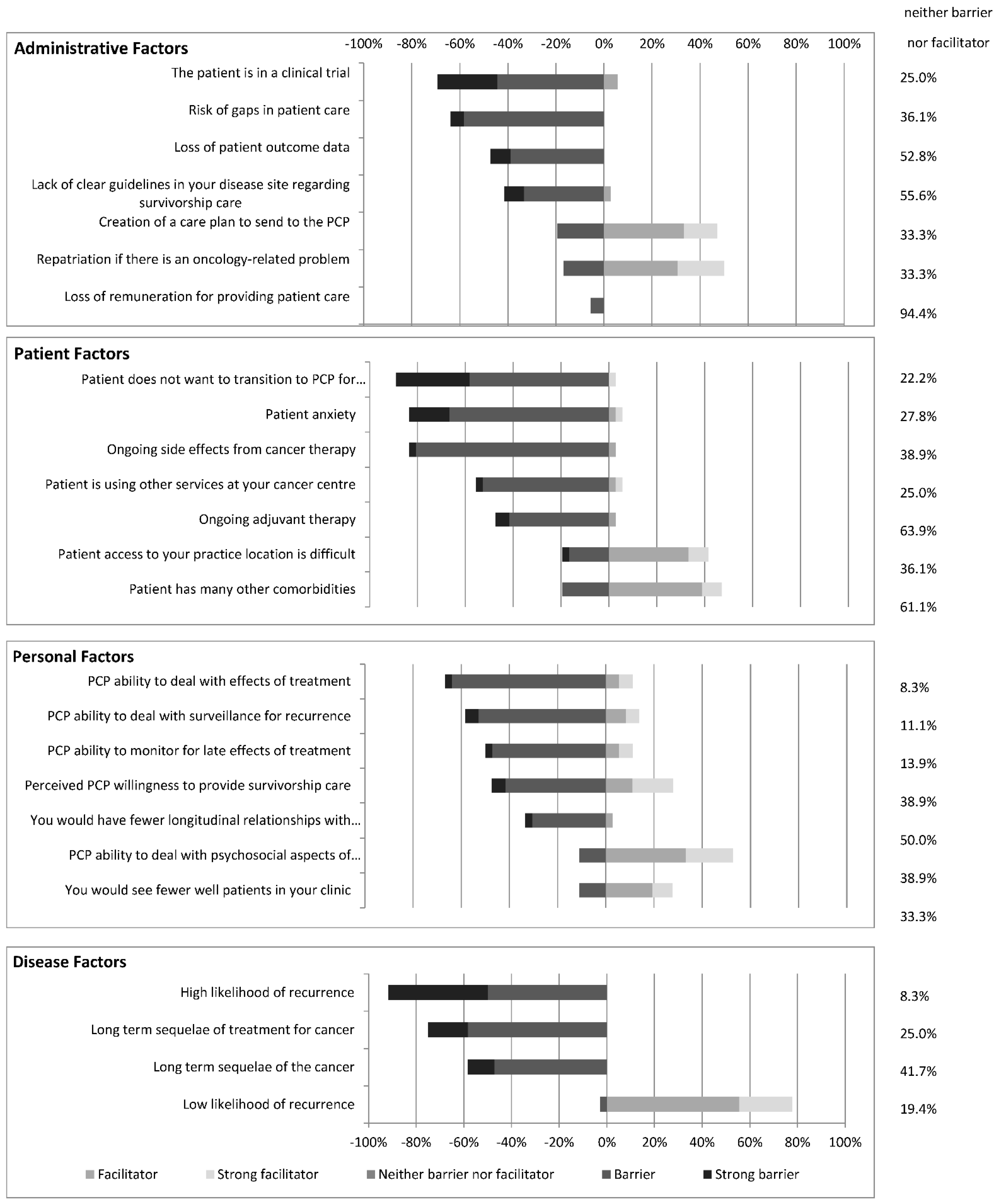
3.4. Barriers and Facilitators
3.4.1. Administrative Factors
3.4.2. Personal Factors
3.4.3. Patient Factors
3.4.4. Disease Factors
3.4.5. Additional Factors
4. Discussion
4.1. Discrepancy between Oncologist Perceptions and PCP Willingness to Provide Survivorship Care
4.2. Facilitators and Barriers of Sharing/Transitioning Survivorship Care
4.3. Synthesis
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canadian Cancer Statistics Advisory Committee. Canadian Cancer Statistics 2019; Canadian Cancer Society: Toronto, ON, Canada, 2019. [Google Scholar]
- Hohmann, N.S.; McDaniel, C.C.; Mason, S.W.; Cheung, W.Y.; Williams, M.S.; Salvador, C.; Graves, E.K.; Camp, C.N.; Chou, C. Healthcare providers’ perspectives on care coordination for adults with cancer and multiple chronic conditions: A systematic review. J. Pharm. Health Serv. Res. 2020, 11, 97–116. [Google Scholar] [CrossRef]
- Hohmann, N.S.; McDaniel, C.C.; Mason, S.W.; Cheung, W.Y.; Williams, M.S.; Salvador, C.; Graves, E.K.; Camp, C.N.; Chou, C. Patient perspectives on primary care and oncology care coordination in the context of multiple chronic conditions: A systematic review. Res. Soc. Adm. Pharm. 2020, 16, 1003–1016. [Google Scholar] [CrossRef]
- De Moor, J.S.; Mariotto, A.B.; Parry, C.; Alfano, C.M.; Padgett, L.; Kent, E.E.; Forsythe, L.; Scoppa, S.; Hachey, M.; Rowland, J.H. Cancer Survivors in the United States: Prevalence across the Survivorship Trajectory and Implications for Care. Cancer Epidemiol. Biomark. Prev. 2013, 22, 561–570. [Google Scholar] [CrossRef] [Green Version]
- Parry, C.; Kent, E.E.; Mariotto, A.B.; Alfano, C.M.; Rowland, J.H. Cancer Survivors: A Booming Population. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1996–2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer in Canada Fact Sheet. 2018. Available online: https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/diseases-conditions/fact-sheet-cancer-canada/fact-sheet-cancer-canada.pdf (accessed on 1 May 2019).
- Lisy, K.; Kent, J.; Piper, A.; Jefford, M. Facilitators and barriers to shared primary and specialist cancer care: A systematic review. Support. Care Cancer 2020, 29, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Canadian Cancer Statistics. 2021. Available online: https://cancer.ca/en/research/cancer-statistics (accessed on 1 May 2019).
- American Society of Clinical Oncology. Status of the medical oncology workforce. The American Society of Clinical Oncology. J. Clin. Oncol. 1996, 14, 2612–2621. [Google Scholar] [CrossRef]
- Whelan, T.; Grunfeld, E.; Sussman, J.; Abelson, J.; William, A.; Sellick, S.; Charles, C.; Fitch, M.; Rand, C.; Tozer, R.; et al. An Evaluation of Continuity of Cancer Care Through Regional Supportive Care Networks; Canadian Health Services Research Foundation: Ottawa, ON, Canada, 2003. [Google Scholar]
- Kendell, C.; Decker, K.; Groome, P.; McBride, M.; Jiang, L.; Krzyzanowska, M.; Porter, G.; Turner, D.; Urquhart, R.; Winget, M.; et al. Use of Physician Services during the Survivorship Phase: A Multi-Province Study of Women Diagnosed with Breast Cancer. Curr. Oncol. 2017, 24, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Schairer, C.; Mink, P.J.; Carroll, L.; Devesa, S.S. Probabilities of Death from Breast Cancer and Other Causes Among Female Breast Cancer Patients. J. Natl. Cancer Inst. 2004, 96, 1311–1321. [Google Scholar] [CrossRef] [Green Version]
- Earle, C.C.; Neville, B.A. Under use of necessary care among cancer survivors. Cancer 2004, 101, 1712–1719. [Google Scholar] [CrossRef]
- Sisler, J.J.; Brown, J.B.; Stewart, M. Family physicians’ roles in cancer care. Survey of patients on a provincial cancer registry. Can. Fam. Physician Med. de Fam. Can. 2004, 50, 889–896. [Google Scholar]
- Snyder, C.F.; Frick, K.D.; Kantsiper, M.E.; Peairs, K.S.; Herbert, R.J.; Blackford, A.L.; Wolff, A.; Earle, C.C. Prevention, Screening, and Surveillance Care for Breast Cancer Survivors Compared with Controls: Changes from 1998 to 2002. J. Clin. Oncol. 2009, 27, 1054–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emery, J.D.; Shaw, K.; Williams, B.; Mazza, D.; Fallon-Ferguson, J.; Varlow, M.; Trevena, L. The role of primary care in early detection and follow-up of cancer. Nat. Rev. Clin. Oncol. 2013, 11, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Grunfeld, E.; Mant, D.; Yudkin, P.; Adewuyi-Dalton, R.; Cole, D.; Stewart, J.; Fitzpatrick, R.; Vessey, M. Routine follow up of breast cancer in primary care: Randomised trial. BMJ 1996, 313, 665–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grunfeld, E.; Levine, M.N.; Julian, J.A.; Coyle, D.; Szechtman, B.; Mirsky, D.; Verma, S.; Dent, S.; Sawka, C.; Pritchard, K.I.; et al. Randomized Trial of Long-Term Follow-Up for Early-Stage Breast Cancer: A Comparison of Family Physician Versus Specialist Care. J. Clin. Oncol. 2006, 24, 848–855. [Google Scholar] [CrossRef]
- Jiwa, M.; Thompson, J.; Coleman, R.; Reed, M. Breast cancer follow-up: Could primary care be the right venue? Curr. Med. Res. Opin. 2006, 22, 625–630. [Google Scholar] [CrossRef]
- Lewis, R.A.; Neal, R.D.; Williams, N.H.; France, B.; Hendry, M.; Russell, D.; Hughes, D.A.; Russell, I.; Stuart, N.S.; Weller, D.; et al. Follow-up of cancer in primary care versus secondary care: Systematic review. Br. J. Gen. Pract. 2009, 59, e234–e247. [Google Scholar] [CrossRef] [Green Version]
- Walsh, G.L.; O’Connor, M.; Willis, K.M.; Milas, M.; Wong, R.S.; Nesbitt, J.C.; Putnam, J.B.; Lee, J.J.; Roth, J.A. Is follow-up of lung cancer patients after resection medically indicated and cost-effective? Ann. Thorac. Surg. 1995, 60, 1563–1572. [Google Scholar] [CrossRef]
- Chubak, J.; Tuzzio, L.; Hsu, C.; Alfano, C.M.; Rabin, B.A.; Hornbrook, M.C.; Spegman, A.; Von Worley, A.; Williams, A.; Nekhlyudov, L. Providing Care for Cancer Survivors in Integrated Health Care Delivery Systems: Practices, Challenges, and Research Opportunities. J. Oncol. Pract. 2012, 8, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Earle, C.C. Cancer Survivorship Research and Guidelines: Maybe the Cart Should Be Beside the Horse. J. Clin. Oncol. 2007, 25, 3800–3801. [Google Scholar] [CrossRef]
- Grunfeld, E.; Earle, C.C. The Interface Between Primary and Oncology Specialty Care: Treatment Through Survivorship. J. Natl. Cancer Inst. Monogr. 2010, 2010, 25–30. [Google Scholar] [CrossRef]
- Institute for Clinical and Evaluative Sciences. Primary Care Atlas: Chapter 10—Physician Care of Cancer Patients; ICES: Toronto, ON, Canada, 2006. [Google Scholar]
- Armes, J.; Crowe, M.; Colbourne, L.; Morgan, H.; Murrells, T.; Oakley, C.; Palmer, N.; Ream, E.; Young, A.; Richardson, A. Patients’ Supportive Care Needs Beyond the End of Cancer Treatment: A Prospective, Longitudinal Survey. J. Clin. Oncol. 2009, 27, 6172–6179. [Google Scholar] [CrossRef] [PubMed]
- Vardy, J.L.; Chan, R.; Koczwara, B.; Lisy, K.; Cohn, R.J.; Joske, D.; Dhillon, H.M.; Jefford, M. Clinical Oncology Society of Australia position statement on cancer survivorship care. Aust. J. Gen. Pract. 2019, 48, 833–836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choosing Wisely Canada, Oncology. 2020. Available online: https://choosingwiselycanada.org/oncology/ (accessed on 1 December 2020).
- Anvik, T.; Holtedahl, K.A.; Mikalsen, H. “When patients have cancer, they stop seeing me”—The role of the general practitioner in early follow-up of patients with cancer—A qualitative study. BMC Fam. Pract. 2006, 7, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, W.Y.; Aziz, N.M.; Noone, A.-M.; Rowland, J.H.; Potosky, A.L.; Ayanian, J.Z.; Virgo, K.S.; Ganz, P.A.; Stefanek, M.; Earle, C.C. Physician preferences and attitudes regarding different models of cancer survivorship care: A comparison of primary care providers and oncologists. J. Cancer Surviv. 2013, 7, 343–354. [Google Scholar] [CrossRef] [PubMed]
- Schütze, H.; Chin, M.; Weller, D.; Harris, M.F. Patient, general practitioner and oncologist views regarding long-term cancer shared care. Fam. Pract. 2018, 35, 323–329. [Google Scholar] [CrossRef]
- Sussman, J.; Baldwin, L.M. The interface of primary and oncology specialty care: From diagnosis through primary treatment. J. Natl. Cancer Inst. Monogr. 2010, 2010, 18–24. [Google Scholar] [CrossRef]
- Watson, E.K.; Sugden, E.M.; Rose, P.W. Views of primary care physicians and oncologists on cancer follow-up initiatives in primary care: An online survey. J. Cancer Surviv. 2010, 4, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Watson, E.K.; O’Brien, R.; Campbell, C.; Weller, D.; Neal, R.D.; Wilkinson, C.; Rose, P.W.; on behalf of the Prostate Cancer Follow-Up Study Group. Views of health professionals on the role of primary care in the follow-up of men with prostate cancer. Fam. Pract. 2011, 28, 647–654. [Google Scholar] [CrossRef] [Green Version]
- Wood, M.L.; McWilliam, C.L. Cancer in remission. Challenge in collaboration for family physicians and oncologists. Can. Fam. Physician 1996, 42, 899–910. [Google Scholar]
- Cheung, W.Y.; Neville, B.A.; Cameron, D.B.; Cook, E.F.; Earle, C.C. Comparisons of Patient and Physician Expectations for Cancer Survivorship Care. J. Clin. Oncol. 2009, 27, 2489–2495. [Google Scholar] [CrossRef]
- Del Giudice, M.E.; Grunfeld, E.; Harvey, B.J.; Piliotis, E.; Verma, S. Primary Care Physicians’ Views of Routine Follow-Up Care of Cancer Survivors. J. Clin. Oncol. 2009, 27, 3338–3345. [Google Scholar] [CrossRef] [PubMed]
- Sussman, J.; Bainbridge, D.; Evans, W.K. Towards integrating primary care with cancer care: A regional study of current gaps and opportunities in Canada. Healthc. Policy 2017, 12, 50–65. [Google Scholar] [CrossRef] [Green Version]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef] [Green Version]
- Atkins, L.; Francis, J.; Islam, R.; O’Connor, D.; Patey, A.; Ivers, N.; Foy, R.; Duncan, E.; Colquhoun, H.; Grimshaw, J.M.; et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement. Sci. 2017, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Aubin, M.; Giguère, A.; Martin, M.; Verreault, R.; Fitch, M.I.; Kazanjian, A.; Carmichael, P.-H. Interventions to improve continuity of care in the follow-up of patients with cancer. Cochrane Database Syst. Rev. 2012, 7, CD007672. [Google Scholar] [CrossRef] [PubMed]
- Sada, Y.H.; Street, R.L., Jr.; Singh, H.; Shada, R.E.; Naik, A.D. Primary care and communication in shared cancer care: A qualitative study. Am. J. Manag. Care 2011, 17, 259–265. [Google Scholar]
- Virgo, K.S.; Lerro, C.C.; Klabunde, C.N.; Earle, C.; Ganz, P.A. Barriers to Breast and Colorectal Cancer Survivorship Care: Perceptions of Primary Care Physicians and Medical Oncologists in the United States. J. Clin. Oncol. 2013, 31, 2322–2336. [Google Scholar] [CrossRef] [Green Version]
- MacCallum, R.C.; Zhang, S.; Preacher, K.J.; Rucker, D.D. On the practice of dichotomization of quantitative variables. Psychol. Methods 2002, 7, 19–40. [Google Scholar] [CrossRef]
- Creswell, J.W. Research Design: Qualitative and Quantitative Approaches, 2nd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2002. [Google Scholar]
- Kline, R.M.; Arora, N.K.; Bradley, C.J.; Brauer, E.R.; Graves, D.L.; Lunsford, N.B.; McCabe, M.S.; Nasso, S.F.; Nekhlyudov, L.; Rowland, J.H.; et al. Long-Term Survivorship Care After Cancer Treatment—Summary of a 2017 National Cancer Policy Forum Workshop. J. Natl. Cancer Inst. 2018, 110, 1300–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, M.; De Rossi, S.; Sussman, J. Supporting Models to Transition Breast Cancer Survivors to Primary Care: Formative Evaluation of a Cancer Care Ontario Initiative. J. Oncol. Pract. 2015, 11, e288–e295. [Google Scholar] [CrossRef]
- Clinical Oncology Society of Australia. Model of Survivorship Care: Appendix 1. 2016. Available online: https://www.cosa.org.au/media/332340/cosa-model-of-survivorship-care-full-version-final-20161107.pdf (accessed on 1 December 2020).
- Maher, J.; Petchey, L.; Greenfield, D.; Levitt, G.; Fraser, M. Implementation of nationwide cancer survivorship plans: Experience from the UK. J. Cancer Policy 2018, 15, 76–81. [Google Scholar] [CrossRef]
- Vanhuyse, M.; Bedard, P.; Sheiner, J.; Fitzgerald, B.; Clemons, M. Transfer of Follow-up Care to Family Physicians for Early-stage Breast Cancer. Clin. Oncol. 2007, 19, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Cardella, J.; Coburn, N.G.; Gagliardi, A.; Maier, B.-A.; Greco, E.; Last, L.; Smith, A.J.; Law, C.; Wright, F. Compliance, attitudes and barriers to post-operative colorectal cancer follow-up. J. Eval. Clin. Pract. 2008, 14, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Earle, C.C.; Grunfeld, E.; Coyle, D.; Cripps, M.C.; Stern, H.S. Cancer physicians’ attitudes toward colorectal cancer follow-up. Ann. Oncol. 2003, 14, 400–405. [Google Scholar] [CrossRef]
- Hwang, S.S.; Chang, V.T.; Cogswell, J.; Alejandro, Y.; Osenenko, P.; Morales, E.; Srinivas, S.; Kasimis, B. Study of unmet needs in symptomatic veterans with advanced cancer: Incidence, independent predictors and unmet needs outcome model. J. Pain Symptom Manag. 2004, 28, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, M.; Greenfield, S.; Stovall, E. From Cancer Patient to Cancer Survivor: Lost in Transition; The National Academies Press: Washington, DC, USA, 2005; Available online: http://www.nap.edu/catalog/11468.html (accessed on 1 May 2019).
- Salz, T.; Oeffinger, K.C.; McCabe, M.S.; Layne, T.M.; Bach, P.B. Survivorship care plans in research and practice. CA Cancer J. Clin. 2012, 62, 101–117. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, P.; DeRosa, A.P.; Henderson, T.O.; Mayer, D.K.; Moskowitz, C.S.; Paskett, E.D.; Rowland, J.H. Systematic Review of the Impact of Cancer Survivorship Care Plans on Health Outcomes and Health Care Delivery. J. Clin. Oncol. 2018, 36, 2088–2100. [Google Scholar] [CrossRef]
- Salz, T.; McCabe, M.S.; Onstad, E.E.; Baxi, S.S.; Deming, R.L.; Franco, R.A.; Glenn, L.A.; Harper, G.R.; Jumonville, A.J.; Payne, R.M.; et al. Survivorship care plans: Is there buy-in from community oncology providers? Cancer 2013, 120, 722–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grunfeld, E.; Mant, D.; Vessey, M.P.; Fitzpatrick, R. Specialist and general practice views on routine follow-up of breast cancer patients in general practice. Fam. Pract. 1995, 12, 60–65. [Google Scholar] [CrossRef]
- Jefford, M.; Baravelli, C.; Dudgeon, P.; Dabscheck, A.; Evans, M.; Moloney, M.; Schofield, P. Tailored Chemotherapy Information Faxed to General Practitioners Improves Confidence in Managing Adverse Effects and Satisfaction with Shared Care: Results from a Randomized Controlled Trial. J. Clin. Oncol. 2008, 26, 2272–2277. [Google Scholar] [CrossRef] [PubMed]
- Mansell, G.; Shapley, M.; Jordan, J.L.; Jordan, K. Interventions to reduce primary care delay in cancer referral: A systematic review. Br. J. Gen. Pract. 2011, 61, e821–e835. [Google Scholar] [CrossRef] [PubMed]
- Papagrigoriadis, S.; Koreli, A. The needs of general practitioners in the follow-up of patients with colorectal cancer. Eur. J. Surg. Oncol. 2001, 27, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Potosky, A.L.; Han, P.; Rowland, J.; Klabunde, C.N.; Smith, T.; Aziz, N.; Earle, C.; Ayanian, J.Z.; Ganz, P.A.; Stefanek, M. Differences Between Primary Care Physicians’ and Oncologists’ Knowledge, Attitudes and Practices Regarding the Care of Cancer Survivors. J. Gen. Intern. Med. 2011, 26, 1403–1410. [Google Scholar] [CrossRef] [Green Version]
- Ray, S.; Archbold, R.A.; Preston, S.; Ranjadayalan, K.; Suliman, A.; Timmis, A.D. Computer-generated correspondence for patients attending an open-access chest pain clinic. J. R. Coll. Physicians Lond. 1998, 32, 420–421. [Google Scholar] [PubMed]
- Grunfeld, E.; Julian, J.A.; Pond, G.; Maunsell, E.; Coyle, D.; Folkes, A.; Joy, A.A.; Provencher, L.; Rayson, D.; Rheaume, D.E.; et al. Evaluating Survivorship Care Plans: Results of a Randomized, Clinical Trial of Patients With Breast Cancer. J. Clin. Oncol. 2011, 29, 4755–4762. [Google Scholar] [CrossRef]
- Mayer, E.L.; Gropper, A.B.; Neville, B.A.; Partridge, A.H.; Cameron, D.B.; Winer, E.P.; Earle, C.C. Breast Cancer Survivors’ Perceptions of Survivorship Care Options. J. Clin. Oncol. 2012, 30, 158–163. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Characteristic | No. | % | ||
|---|---|---|---|---|
| New patients/week | Median = 5, range = 2–24 | |||
| Funding Model | Blended | 17 | 43.6 | |
| Salary | 15 | 38.5 | ||
| Fee for service | 2 | 5.1 | ||
| No response | 5 | 12.8 | ||
| Years in practice | ≤5 | 5 | 12.8 | |
| 6–10 | 8 | 20.5 | ||
| 11+ | 26 | 66.7 | ||
| Main area of clinical practice | ||||
| Radiation oncology | 18 | 46.2 | ||
| Medical oncology | 12 | 30.8 | ||
| Hematology/oncology | 4 | 10.3 | ||
| Gynecologic | 1 | 2.6 | ||
| General medicine | 4 | 10.3 | ||
| Type(s) of cancer treated on regular basis a | ||||
| Breast | 19 | 48.7 | ||
| Other gastrointestinal | 17 | 43.6 | ||
| Colorectal | 10 | 25.6 | ||
| Lung | 8 | 20.5 | ||
| Prostate | 5 | 12.8 | ||
| Hematologic | 5 | 12.8 | ||
| Sarcoma | 5 | 12.8 | ||
| Central nervous system | 5 | 12.8 | ||
| Skin | 4 | 10.3 | ||
| Head and Neck | 4 | 10.3 | ||
| Non-prostate genitourinary | 4 | 10.3 | ||
| Gynecologic | 2 | 5.1 | ||
| Other | 10 | 25.6 | ||
| Considered primary cancer site b | ||||
| Breast | 10 | 25.6 | ||
| Hematologic | 5 | 12.8 | ||
| Lung | 5 | 12.8 | ||
| Other gastrointestinal | 4 | 10.3 | ||
| Central nervous system | 3 | 7.7 | ||
| Prostate | 3 | 7.7 | ||
| Colorectal | 2 | 5.1 | ||
| Gynecologic | 2 | 5.1 | ||
| Skin | 2 | 5.1 | ||
| Head and neck | 1 | 2.6 | ||
| Sarcoma | 1 | 2.6 | ||
| Other | 1 | 2.6 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coschi, C.H.; Bainbridge, D.; Sussman, J. Understanding the Attitudes and Beliefs of Oncologists Regarding the Transitioning and Sharing of Survivorship Care. Curr. Oncol. 2021, 28, 5452-5465. https://doi.org/10.3390/curroncol28060454
Coschi CH, Bainbridge D, Sussman J. Understanding the Attitudes and Beliefs of Oncologists Regarding the Transitioning and Sharing of Survivorship Care. Current Oncology. 2021; 28(6):5452-5465. https://doi.org/10.3390/curroncol28060454
Chicago/Turabian StyleCoschi, Courtney H., Daryl Bainbridge, and Jonathan Sussman. 2021. "Understanding the Attitudes and Beliefs of Oncologists Regarding the Transitioning and Sharing of Survivorship Care" Current Oncology 28, no. 6: 5452-5465. https://doi.org/10.3390/curroncol28060454
APA StyleCoschi, C. H., Bainbridge, D., & Sussman, J. (2021). Understanding the Attitudes and Beliefs of Oncologists Regarding the Transitioning and Sharing of Survivorship Care. Current Oncology, 28(6), 5452-5465. https://doi.org/10.3390/curroncol28060454