Extent of Groin Dissection in Melanoma: A Mixed-Methods, Population-Based Study of Practice Patterns and Outcomes


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Surgical Practice Patterns
2.3. Statistical Methods
2.4. Surgeon Preferences and Perceptions
3. Results
3.1. Quantitative Results
3.1.1. Entire Cohort
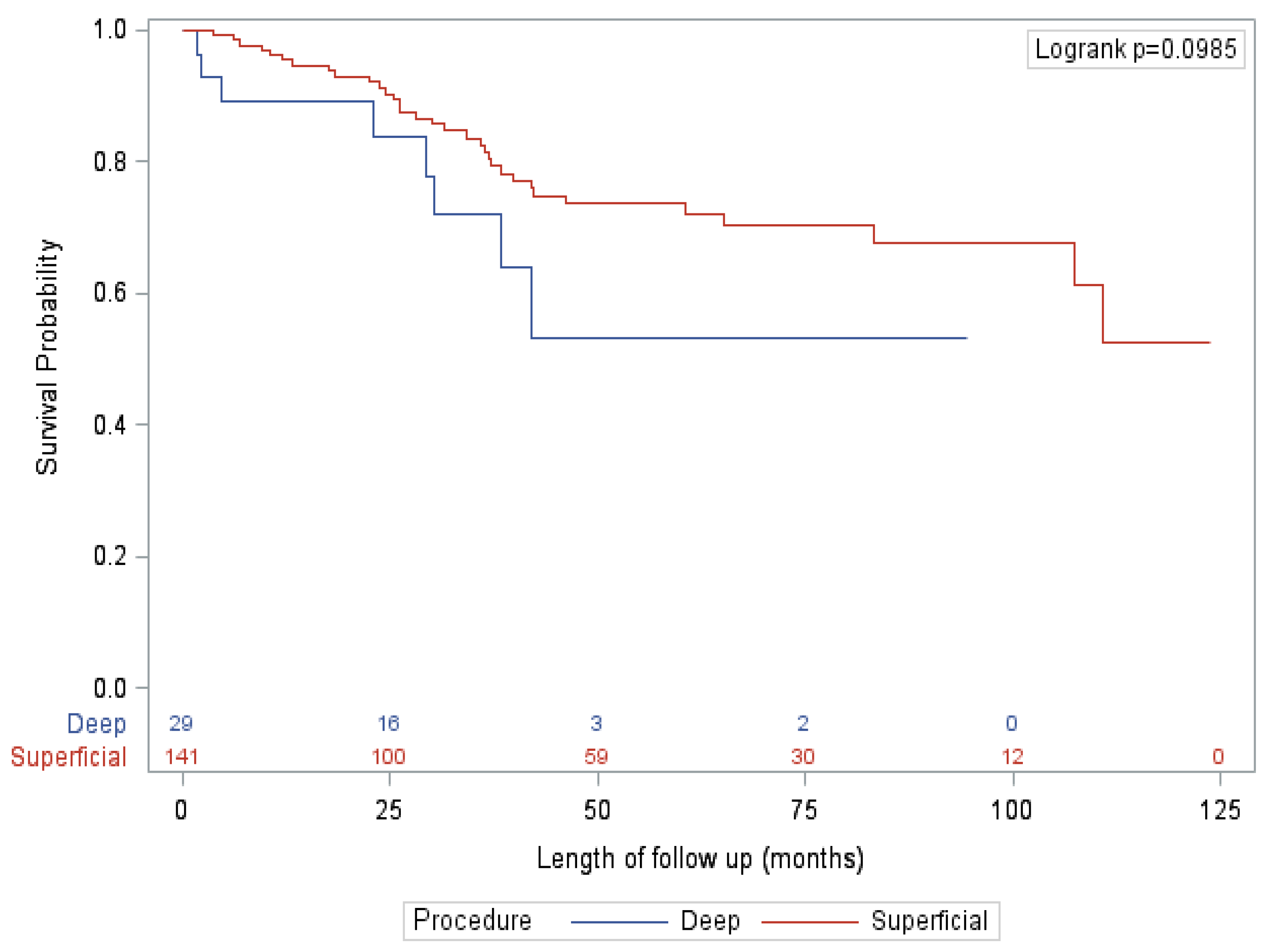
3.1.2. Sentinel Node Positive Cohort
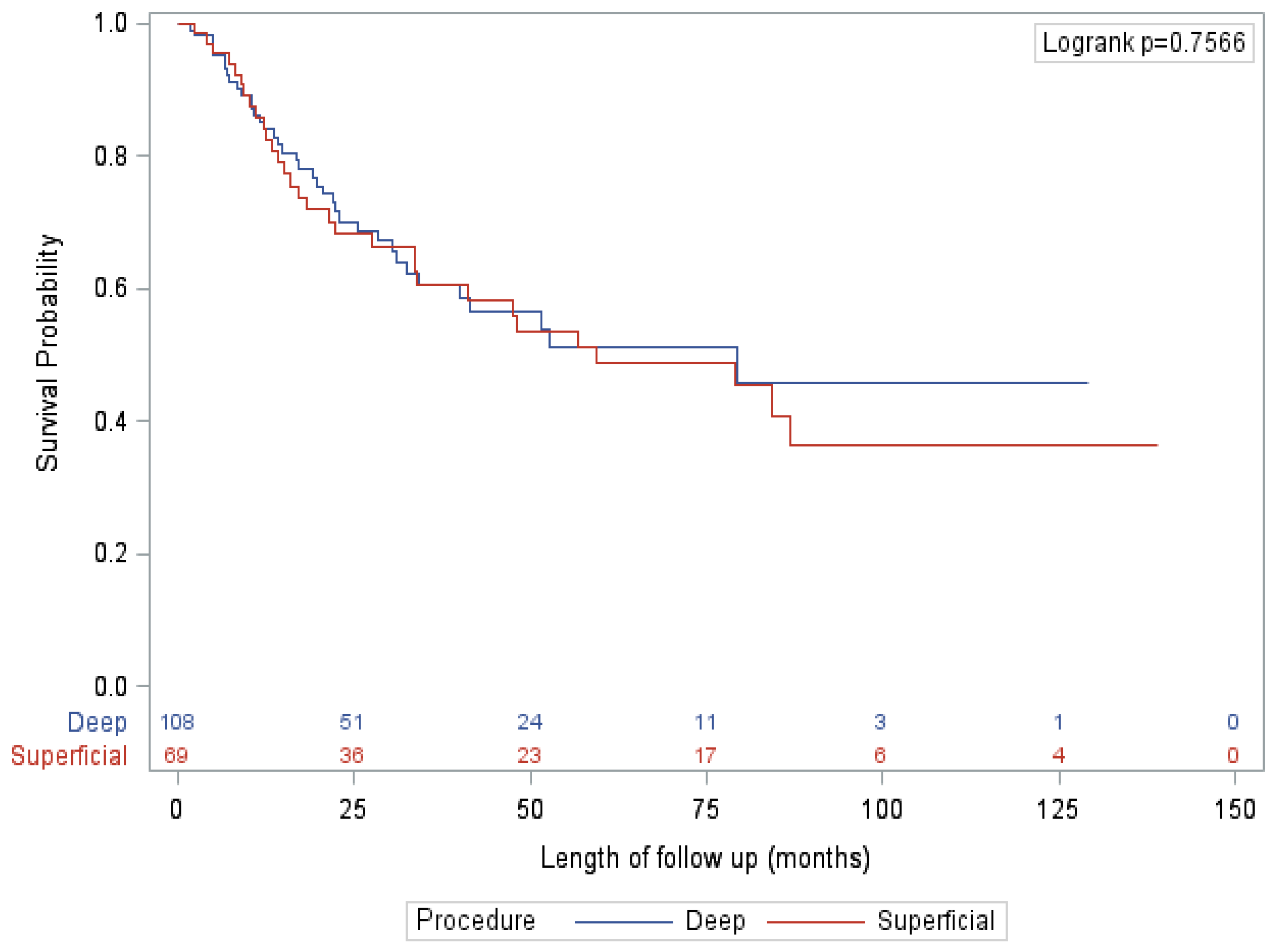
3.1.3. Clinically Positive (Palpable Disease or Imaging Positive) Cohort
3.2. Qualitative Results
3.2.1. Guidelines or Papers Used by the Surgeons
3.2.2. Estimated Percentage of Surgeon’s Dissections That Contain Deep Component
3.2.3. Surgeon-Level Indications for Deep/Pelvic Node Dissection
3.2.4. Perceived Benefits of Deep Dissection
3.2.5. Perceived Risks of Deep Dissection
3.2.6. Type of Incision Used
3.2.7. A Priori Probability of Deep Nodal Disease That Would Prompt a Deep Dissection
4. Discussion
4.1. Patient Selection and Deep Positivity Rate
4.2. Perioperative Outcomes
4.3. Oncologic Outcomes
4.4. Limitations & Generalisability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuk, D.; Shoushtari, A.N.; Barker, C.A.; Panageas, K.S.; Munhoz, R.R.; Momtaz, P.; Ariyan, C.E.; Brady, M.S.; Coit, D.G.; Bogatch, K.; et al. Melanoma and Cutaneous Malignancies Prognosis of Mucosal, Uveal, Acral, Nonacral Cutaneous, and Unknown Primary Melanoma From the Time of First Metastasis. Oncologist 2016, 21, 848. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada Melanoma Skin Cancer. Available online: https://www.canada.ca/en/public-health/services/chronic-diseases/cancer/melanoma-skin-cancer.html (accessed on 13 March 2020).
- Leiter, U.; Stadler, R.; Mauch, C.; Hohenberger, W.; Brockmeyer, N.; Berking, C.; Sunderkötter, C.; Kaatz, M.; Schulte, K.; Lehmann, P.; et al. Complete lymph node dissection versus no dissection in patients with sentinel lymph node biopsy positive melanoma (DeCOG-SLT): A multicentre, randomised, phase 3 trial. Lancet Oncol. 2016, 17, 757–767. [Google Scholar] [CrossRef]
- Faries, M.B.; Thompson, J.F.; Cochran, A.J.; Andtbacka, R.H.; Mozzillo, N.; Zager, J.S.; Jahkola, T.; Bowles, T.L.; Testori, A.; Beitsch, P.D.; et al. Completion Dissection or Observation for Sentinel-Node Metastasis in Melanoma. N. Engl. J. Med. 2017, 376, 2211–2222. [Google Scholar] [CrossRef] [PubMed]
- Melanoma and Skin Cancer Trials Limited Evaluation of Groin Lymphadenectomy Extent for Metastatic Melanoma (EAGLE FM). Available online: https://clinicaltrials.gov/ct2/show/NCT02166788 (accessed on 13 March 2021).
- Carvajal, R.D.; Spencer, S.A.; Lydiatt, W. Mucosal Melanoma: A Clinically and Biologically Unique Disease Entity. J. Natl. Compr. Cancer Netw. 2012, 10, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Ploeg, A.; Akkooi, A.; Schmitz, P.; Geel, A.; Wilt, J.; Eggermont, A.; Verhoef, K. Therapeutic Surgical Management of Palpable Melanoma Groin Metastases: Superficial or Combined Superficial and Deep Groin Lymph Node Dissection. Ann. Surg. Oncol. 2011, 18, 3300–3308. [Google Scholar] [CrossRef] [PubMed]
- Verver, D.; Madu, M.F.; Oude Ophuis, C.; Faut, M.; Wilt, J.; Bonenkamp, H.; Grunhagen, D.J.; Akkooi, A.; Verhoef, K.; van Leeuwen, B.L. Optimal extent of completion lymphadenectomy for patients with melanoma and a positive sentinel node in the groin. Br. J. Surg. 2017, 2017, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Strobbe, L.; Jonk, A.; Hart, A.; Nieweg, O.; Kroon, B. Positive Iliac and Obturator Nodes in Melanoma: Survival and Prognostic Factors. Ann. Surg. Oncol. 1999, 6, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Oude Ophuis, C.M.C.; van Akkooi, A.C.J.; Hoekstra, H.J.; Bonenkamp, J.J.; van Wissen, J.; Niebling, M.G.; de Wilt, J.H.W.; van der Hiel, B.; van de Wiel, B.; Koljenovic, S.; et al. Risk Factors for Positive Deep Pelvic Nodal Involvement in Patients with Palpable Groin Melanoma Metastases: Can the Extent of Surgery be Safely Minimized? Ann. Surg. Oncol. 2015, 22, S1172–S1180. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mozzillo, N.; Pasquali, S.; Santinami, M.; Testori, A.; Di Marzo, M.; Crispo, A.; Patuzzo, R.; Verrecchia, F.; Botti, G.; Montella, M.; et al. Factors predictive of pelvic lymph node involvement and outcomes in melanoma patients with metastatic sentinel lymph node of the groin: A multicentre study. Eur. J. Surg. Oncol. 2015, 41, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.E.; Brown, R.E.; Roach, B.A.; Quillo, A.R.; Martin, R.C.G.; Scoggins, C.R.; Stromberg, A.J.; McMasters, K.M. Addition of an Iliac/Obturator Lymph Node Dissection Does Not Improve Nodal Recurrence or Survival in Melanoma. J. Am. Coll. Surg. 2014, 219, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Allan, C.P.; Hayes, A.J.; Thomas, J.M. Ilioinguinal lymph node dissection for palpable metastatic melanoma to the groin. ANZ J. Surg. 2008, 78, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Van Wissen, J.; van der Hiel, B.; van der Hage, J.A.; van de Wiel, B.A.; Wouters, M.W.J.M.; van Akkooi, A.C.J. The diagnostic value of PET/CT imaging in melanoma groin metastases. Ann. Surg. Oncol. 2016, 23, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Henderson, M.A.; Burmeister, B.H.; Ainslie, J.; Fisher, R.; Di Iulio, J.; Smithers, B.M.; Hong, A.; Shannon, K.; Scolyer, R.A.; Carruthers, S.; et al. Adjuvant lymph-node field radiotherapy versus observation only in patients with melanoma at high risk of further lymph-node field relapse after lymphadenectomy (ANZMTG 01.02/TROG 02.01): 6-Year follow-up of a phase 3, randomised controlled trial. Lancet Oncol. 2015, 16, 1049–1060. [Google Scholar] [CrossRef]
- Mann, G.; Coit, D. Does the Extent of Operation Influence the Prognosis in Patients with Melanoma Metastatic to Inguinal Nodes? Ann. Surg. Oncol. 1999, 6, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Badgwell, B.; Xing, Y.; Gershenwald, J.; Lee, J.; Mansfield, P.; Ross, M.; Cormier, J. Pelvic Lymph Node Dissection Is Beneficial in Subsets of Patients with Node-positive Melanoma. Ann. Surg. Oncol. 2007, 14, 2867–2875. [Google Scholar] [CrossRef] [PubMed]
- Rauwerdink, D.J.W.; Molina, G.; Frederick, D.T.; Sharova, T.; Carmichael, H.; Boland, G.M. Adjuvant Therapy Failure Patterns in the Modern Era of Melanoma Management. Ann. Surg. Oncol. 2020, 27, 5128. [Google Scholar] [CrossRef] [PubMed]
- Pasquali, S.; Sommariva, A.; Spillane, A.J.; Bilimoria, K.Y.; Rossi, C.R. Measuring the quality of melanoma surgery–highlighting issues with standardization and quality assurance of care in surgical oncology. Eur. J. Surg. Oncol. 2016, 43, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Huo, J.; Lairson, D.R.; Du, X.L.; Chan, W.; Jiang, J.; Buchholz, T.A.; Guadagnolo, B.A. Hospital Case Volume Is Associated with Improved Survival for Patients With Metastatic Melanoma. Am. J. Clin. Oncol. 2016, 39, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Cheraghlou, S.; Agogo, G.O.; Girardi, M. Treatment of primary nonmetastatic melanoma at high-volume academic facilities is associated with improved long-term patient survival. J. Am. Acad. Dermatol. 2019, 80, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Kretschmer, L.; Neumann, C.; Preußer, K.-P.; Marsch, W.C. Superficial Inguinal and Radical Ilioinguinal Lymph Node Dissection in Patients with Palpable Melanoma Metastases to the Groin—An Analysis of Survival and Local Recurrence. Acta Oncol. 2001, 40, 72–78. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Category | Total (N = 347) |
|---|---|---|
| Age | Median (IQR) | 57.1 (47.3–68.4) |
| Sex | F | 197 (56.8%) |
| M | 150 (43.2%) | |
| BMI | Median (IQR) | 26.2 (23.4–30.1) |
| Comorbidities—CHF | Yes | 23 (6.6%) |
| Comorbidities—COPD | Yes | 7 (2%) |
| Comorbidities—CRF | Yes | 5 (1.4%) |
| Comorbidities—CVA | Yes | 5 (1.4%) |
| Comorbidities—DM | Yes | 29 (8.4%) |
| Known primary | No | 26 (7.5%) |
| Yes | 320 (92.2%) | |
| Thickness | Thin (≤1 mm) | 25 (7.2%) |
| Intermediate (1.01–4 mm) | 173 (49.9%) | |
| Thick (>4 mm) | 113 (32.6%) | |
| Unknown | 36 (10.4%) | |
| Clark level | ≤III | 108 (31.1%) |
| IV/V | 239 (68.9%) | |
| Ulceration | No | 148 (42.7%) |
| Yes | 143 (41.2%) | |
| Unknown | 56 (16.1%) | |
| Mitoses | No | 95 (27.4%) |
| Yes | 252 (72.6%) | |
| LVI | No | 221 (63.7%) |
| Yes | 45 (13%) | |
| Satellites | No | 230 (66.3%) |
| Yes | 37 (10.7%) | |
| Mode of diagnosis | Imaging | 26 (7.5%) |
| Palpable | 151 (43.5%) | |
| SLNB | 170 (49%) | |
| Timing of diagnosis | Initial presentation | 224 (64.6%) |
| Recurrence | 122 (35.2%) | |
| Systemic Metastases | No | 336 (96.8%) |
| Yes | 9 (2.6%) | |
| Extent of dissection | Superficial only | 210 (60.5%) |
| Combined | 137 (39.5%) | |
| LOS—Initial | Median (IQR) | 2 (1–3) |
| LOS—Total * | Median (IQR) | 2 (1–4) |
| Complications | No | 185 (53.3%) |
| Yes | 162 (46.7%) | |
| Complications—Grade † | <III | 282 (81.3%) |
| III/IV | 65 (18.7%) | |
| Lymphedema | No | 198 (57.1%) |
| Yes | 149 (42.9%) | |
| Adjuvant therapy (any) | No | 160 (46.1%) |
| Yes | 185 (53.3%) | |
| Adjuvant therapy—type of therapy | None | 161 (46.4%) |
| Radiation | 57 (16.4%) | |
| Interferon | 76 (21.9%) | |
| Immunotherapy | 18 (5.2%) | |
| Combination | 23 (6.6%) | |
| Clinical trial | 12 (3.5%) | |
| Adjuvant radiation | No | 290 (83.6%) |
| Yes | 57 (16.4%) |
| Variables | Category | Palpable/Imaging (n = 177) | SLNB (n = 170) | ||||
|---|---|---|---|---|---|---|---|
| Deep (N = 108) | Superficial (N = 69) | p-Value | Deep (N = 29) | Superficial (N = 141) | p-Value | ||
| Age | Median (IQR) | 59.4 (48.5–70) | 63 (48.6–75.2) | 0.2987 | 62 (53–73.4) | 54 (45–62) | 0.007 |
| Sex | F | 68 (63%) | 37 (53.6%) | 0.2173 | 13 (44.8%) | 79 (56%) | 0.2703 |
| M | 40 (37%) | 32 (46.4%) | 16 (55.2%) | 62 (44%) | |||
| BMI | Median (IQR) | 26.2 (23.3–29.7) | 27.6 (24.4–31.6) | 0.2165 | 28.3 (24–30.8) | 25.6 (22.6–29.4) | 0.1277 |
| Comorbidities—CHF | 1 | 7 (6.5%) | 11 (15.9%) | 0.0423 | 3 (10.3%) | 2 (1.4%) | 0.0355 |
| Comorbidities—COPD | 1 | 3 (2.8%) | 2 (2.9%) | 1 | 1 (3.4%) | 1 (0.7%) | 0.3129 |
| Comorbidities—CRF | 1 | 1 (0.9%) | 4 (5.8%) | 0.0765 | 0.1594 | ||
| Comorbidities—CVA | 1 | 2 (1.9%) | 1 (1.4%) | 1 | 0 (0%) | 2 (1.4%) | 1 |
| Comorbidities—DM | 1 | 10 (9.3%) | 7 (10.1%) | 0.8454 | 3 (10.3%) | 9 (6.4%) | 0.4325 |
| Known primary | No | 17 (15.7%) | 9 (13%) | 0.621 | 1 | ||
| Yes | 91 (84.3%) | 60 (87%) | 29 (100%) | 140 (99.3%) | |||
| Thickness | Thin (≤1 mm) | 13 (12%) | 7 (10.1%) | 0.9449 | 1 (3.4%) | 4 (2.8%) | 0.081 |
| Intermediate (1.01–4 mm) | 40 (37%) | 27 (39.1%) | 13 (44.8%) | 93 (66%) | |||
| Thick (>4 mm) | 32 (29.6%) | 22 (31.9%) | 15 (51.7%) | 44 (31.2%) | |||
| Clark level | ≤III | 44 (40.7%) | 26 (37.7%) | 0.6847 | 6 (20.7%) | 32 (22.7%) | 0.8134 |
| IV/V | 64 (59.3%) | 43 (62.3%) | 23 (79.3%) | 109 (77.3%) | |||
| Ulceration | No | 42 (38.9%) | 22 (31.9%) | 0.5012 | 7 (24.1%) | 77 (54.6%) | 0.0061 |
| Yes | 35 (32.4%) | 28 (40.6%) | 21 (72.4%) | 59 (41.8%) | |||
| Mitoses | No | 38 (35.2%) | 34 (49.3%) | 0.0627 | 2 (6.9%) | 21 (14.9%) | 0.374 |
| Yes | 70 (64.8%) | 35 (50.7%) | 27 (93.1%) | 120 (85.1%) | |||
| LVI | No | 61 (56.5%) | 35 (50.7%) | 0.4383 | 20 (69%) | 105 (74.5%) | 0.4656 |
| Yes | 8 (7.4%) | 9 (13%) | 7 (24.1%) | 21 (14.9%) | |||
| Satellites | No | 57 (52.8%) | 40 (58%) | 0.7529 | 17 (58.6%) | 116 (82.3%) | 0.0019 |
| Yes | 9 (8.3%) | 6 (8.7%) | 10 (34.5%) | 12 (8.5%) | |||
| Mode of diagnosis | Imaging | 23 (21.3%) | 3 (4.3%) | 0.0019 | |||
| Palpable | 85 (78.7%) | 66 (95.7%) | |||||
| SLNB | 29 (100%) | 141 (100%) | 0.0433 | ||||
| Timing of diagnosis | Initial presentation | 38 (35.2%) | 22 (31.9%) | 0.8439 | 28 (96.6%) | 136 (96.5%) | 1 |
| Recurrence | 69 (63.9%) | 47 (68.1%) | 1 (3.4%) | 5 (3.5%) | |||
| Unknown | 1 (0.9%) | 0 (0%) | |||||
| Systemic Metastases | No | 104 (96.3%) | 64 (92.8%) | 0.2645 | 27 (93.1%) | 141 (100%) | 0.0283 |
| Yes | 3 (2.8%) | 5 (7.2%) | 1 (3.4%) | 0 (0%) | |||
| Unknown | 1 (0.9%) | 0 (0%) | 1 (3.4%) | 0 (0%) | |||
| LOS—Initial | Median (IQR) | 2 (1–4) | 2 (1–3) | 0.7634 | 3 (1–4) | 2 (1–3) | 0.1342 |
| LOS—Total | Median (IQR) | 2 (1–4) | 2 (1–4) | 0.8466 | 3 (1–4) | 2 (1–3) | 0.0679 |
| Complications | No | 48 (44.4%) | 38 (55.1%) | 0.1677 | 12 (41.4%) | 87 (61.7%) | 0.0433 |
| Yes | 60 (55.6%) | 31 (44.9%) | 17 (58.6%) | 54 (38.3%) | |||
| Complications—Grade | <III | 86 (79.6%) | 53 (76.8%) | 0.6561 | 24 (82.8%) | 119 (84.4%) | 0.7847 |
| III/IV | 22 (20.4%) | 16 (23.2%) | 5 (17.2%) | 22 (15.6%) | |||
| Lymphedema | No | 54 (50%) | 40 (58%) | 0.3 | 17 (58.6%) | 87 (61.7%) | 0.7565 |
| Yes | 54 (50%) | 29 (42%) | 12 (41.4%) | 54 (38.3%) | |||
| Total nodes harvested | Median (IQR) | 16 (12–21) | 9 (7–13) | <0.0001 | 16 (13–19) | 8 (6–11) | <0.0001 |
| Positive nodes | No | 5 (4.6%) | 10 (14.5%) | 0.0216 | 13 (44.8%) | 116 (82.3%) | <0.0001 |
| Yes | 103 (95.4%) | 59 (85.5%) | 16 (55.2%) | 25 (17.7%) | |||
| Positive deep nodes | No | 62 (57.4%) | 69 (100%) | <0.0001 | 19 (65.5%) | 141 (100%) | <0.0001 |
| Yes | 46 (42.6%) | 0 (0%) | 10 (34.5%) | 0 (0%) | |||
| Extra-nodal extension | No | 53 (49.1%) | 32 (46.4%) | 0.7079 | 17 (58.6%) | 101 (71.6%) | 0.0143 |
| Yes | 46 (42.6%) | 33 (47.8%) | 8 (27.6%) | 12 (8.5%) | |||
| Adjuvant therapy (any) | No | 45 (41.7%) | 27 (39.1%) | 0.7376 | 12 (41.4%) | 76 (53.9%) | 0.1594 |
| Yes | 63 (58.3%) | 42 (60.9%) | 16 (55.2%) | 64 (45.4%) | |||
| Adjuvant therapy—type of therapy | No | 44 (40.7%) | 27 (39.1%) | 0.8154 | 13 (44.8%) | 77 (54.6%) | 0.0008 |
| Radiation | 31 (28.7%) | 16 (23.2%) | 5 (17.2%) | 5 (3.5%) | |||
| Interferon | 11 (10.2%) | 11 (15.9%) | 4 (13.8%) | 50 (35.5%) | |||
| Immunotherapy | 7 (6.5%) | 5 (7.2%) | 3 (10.3%) | 3 (2.1%) | |||
| Combination | 11 (10.2%) | 6 (8.7%) | 3 (10.3%) | 3 (2.1%) | |||
| Clinical trial | 4 (3.7%) | 4 (5.8%) | 1 (3.4%) | 3 (2.1%) | |||
| Adjuvant radiation | No | 77 (71.3%) | 53 (76.8%) | 0.4177 | 24 (82.8%) | 136 (96.5%) | 0.014 |
| Yes | 31 (28.7%) | 16 (23.2%) | 5 (17.2%) | 5 (3.5%) | |||
| Recurrence | No | 41 (38%) | 28 (40.6%) | 0.1636 | 14 (48.3%) | 84 (59.6%) | 0.503 |
| Combined | 13 (12%) | 6 (8.7%) | 5 (17.2%) | 12 (8.5%) | |||
| Distant | 39 (36.1%) | 17 (24.6%) | 4 (13.8%) | 15 (10.6%) | |||
| Local | 0 (0%) | 1 (1.4%) | 0 (0%) | 3 (2.1%) | |||
| Regional | 15 (13.9%) | 17 (24.6%) | 6 (20.7%) | 27 (19.1%) | |||
| Isolated deep node recurrence | No | 63 (58.3%) | 34 (49.3%) | 0.1725 | 15 (51.7%) | 46 (32.6%) | 0.0728 |
| Yes | 4 (3.7%) | 7 (10.1%) | 0 (0%) | 11 (7.8%) | |||
| Unknown | 41 (38%) | 28 (40.6%) | 14 (48.3%) | 84 (59.6%) | |||
| Time to recurrence | Median (IQR) | 6.2 (3.6–13.7) | 7 (3.4–18.7) | 0.5512 | 18.4 (4.2–24.4) | 15.5 (8.8–25.3) | 0.6031 |
| Follow up | Median (IQR) | 22.2 (11.1–41.7) | 32.4 (11–74) | 0.1721 | 27.4 (8.2–38.6) | 38.3 (22.4–70.2) | 0.0034 |
| Status at follow-up | Alive, disease | 27 (25%) | 11 (15.9%) | 0.2171 | 11 (37.9%) | 20 (14.2%) | 0.0094 |
| Alive, no disease | 46 (42.6%) | 28 (40.6%) | 12 (41.4%) | 88 (62.4%) | |||
| Dead | 35 (32.4%) | 30 (43.5%) | 6 (20.7%) | 33 (23.4%) | |||
| Mortality | No | 70 (64.8%) | 38 (55.1%) | 0.1949 | 21 (72.4%) | 108 (76.6%) | 0.6316 |
| Yes | 38 (35.2%) | 31 (44.9%) | 8 (27.6%) | 33 (23.4%) | |||
| Cancer specific | No | 74 (68.5%) | 43 (62.3%) | 0.3954 | 23 (79.3%) | 110 (78%) | 0.8776 |
| Yes | 34 (31.5%) | 26 (37.7%) | 6 (20.7%) | 31 (22%) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Küpper, S.; Austin, J.L.; Dingley, B.; Xu, Y.; Kong, K.; Brar, M.; Wright, F.C.; Nessim, C.; Bouchard-Fortier, A.; Quan, M.L. Extent of Groin Dissection in Melanoma: A Mixed-Methods, Population-Based Study of Practice Patterns and Outcomes. Curr. Oncol. 2021, 28, 5422-5433. https://doi.org/10.3390/curroncol28060452
Küpper S, Austin JL, Dingley B, Xu Y, Kong K, Brar M, Wright FC, Nessim C, Bouchard-Fortier A, Quan ML. Extent of Groin Dissection in Melanoma: A Mixed-Methods, Population-Based Study of Practice Patterns and Outcomes. Current Oncology. 2021; 28(6):5422-5433. https://doi.org/10.3390/curroncol28060452
Chicago/Turabian StyleKüpper, Suzana, Janice L. Austin, Brittany Dingley, Yuan Xu, Kristine Kong, Mantaj Brar, Frances C. Wright, Carolyn Nessim, Antoine Bouchard-Fortier, and May Lynn Quan. 2021. "Extent of Groin Dissection in Melanoma: A Mixed-Methods, Population-Based Study of Practice Patterns and Outcomes" Current Oncology 28, no. 6: 5422-5433. https://doi.org/10.3390/curroncol28060452
APA StyleKüpper, S., Austin, J. L., Dingley, B., Xu, Y., Kong, K., Brar, M., Wright, F. C., Nessim, C., Bouchard-Fortier, A., & Quan, M. L. (2021). Extent of Groin Dissection in Melanoma: A Mixed-Methods, Population-Based Study of Practice Patterns and Outcomes. Current Oncology, 28(6), 5422-5433. https://doi.org/10.3390/curroncol28060452