Epithelioid Trophoblastic Tumour: A Case with Genetic Linkage to a Child Born over Seventeen Years Prior, Successfully Treated with Surgery and Pembrolizumab

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
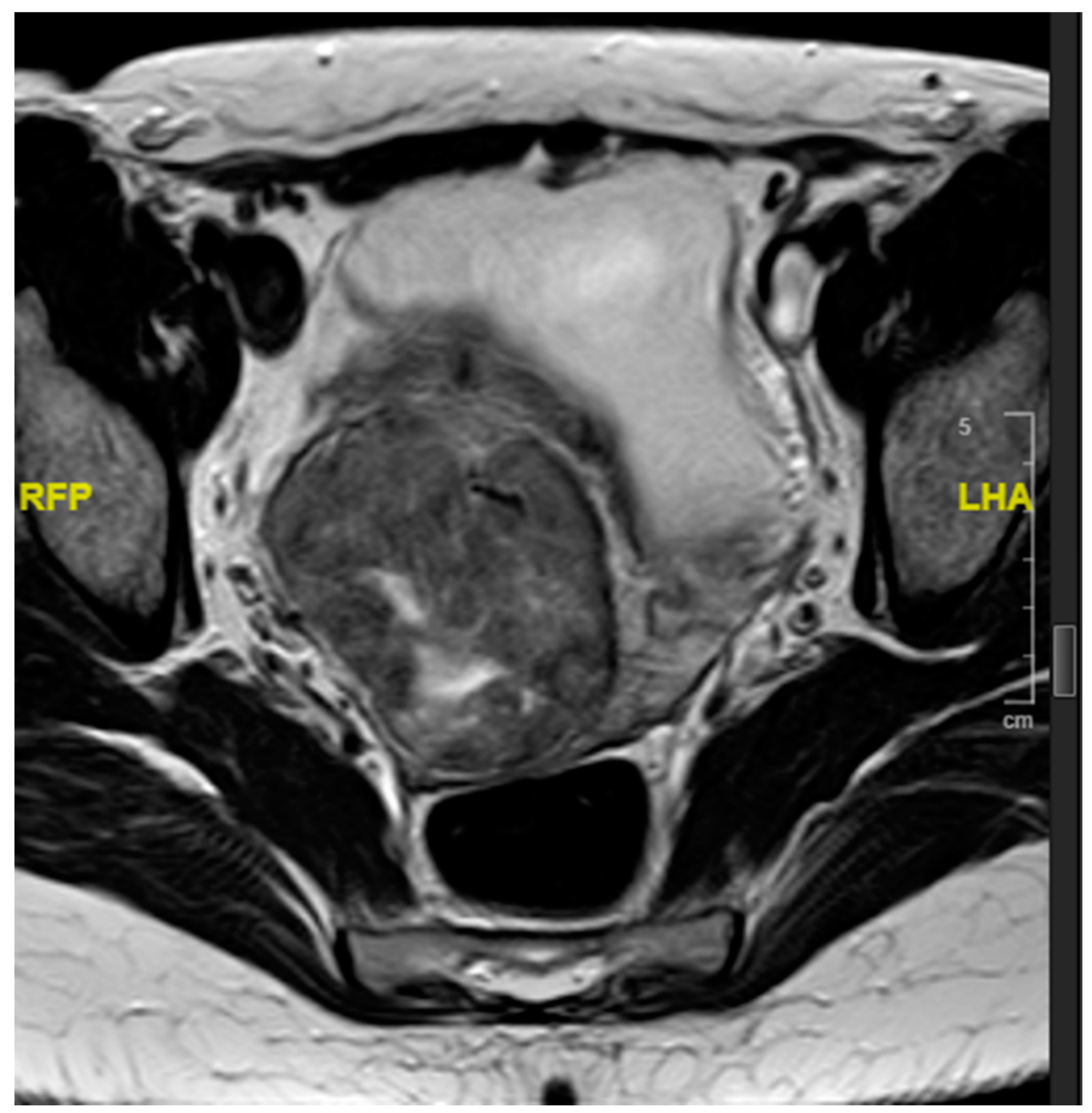
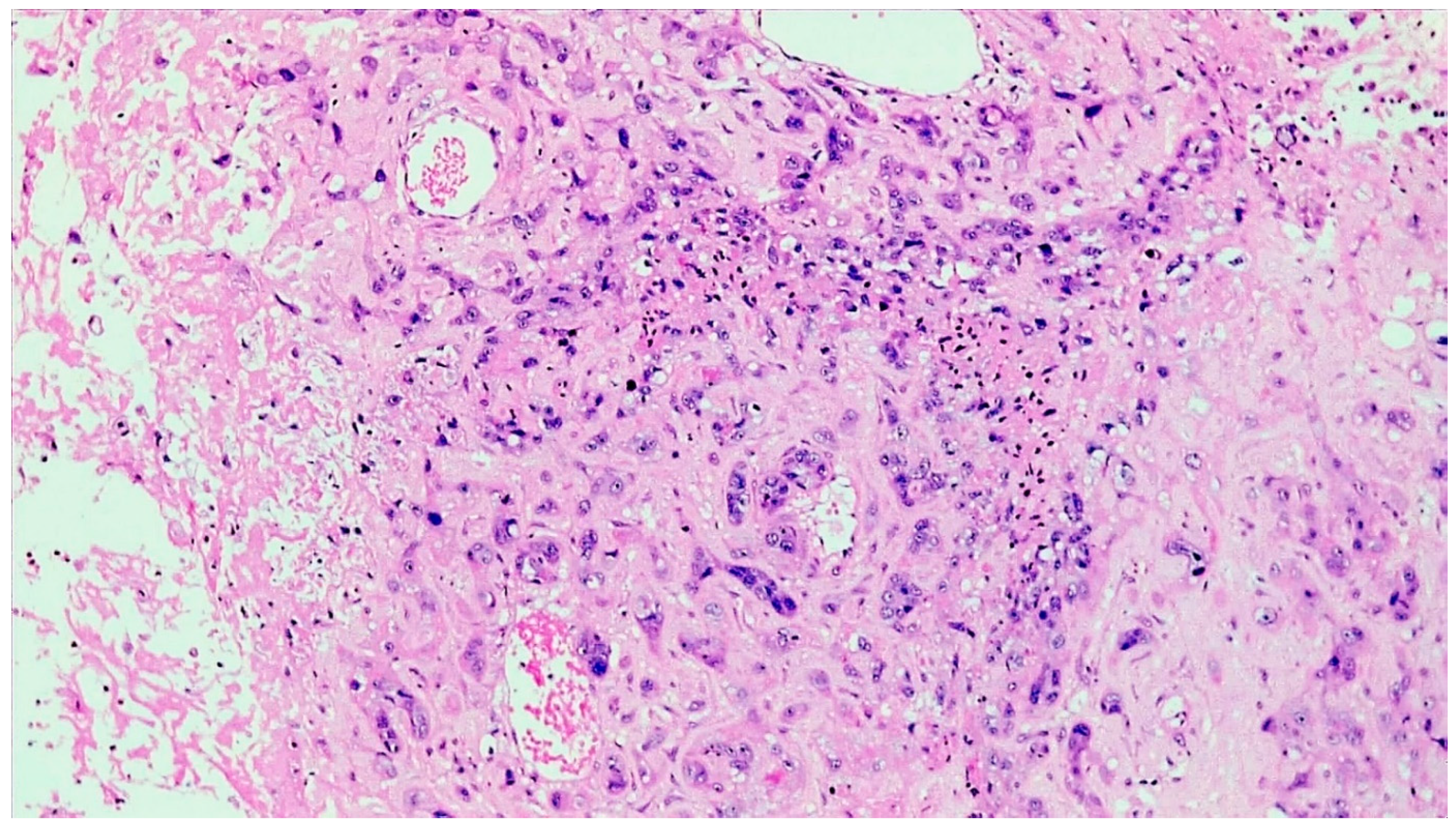
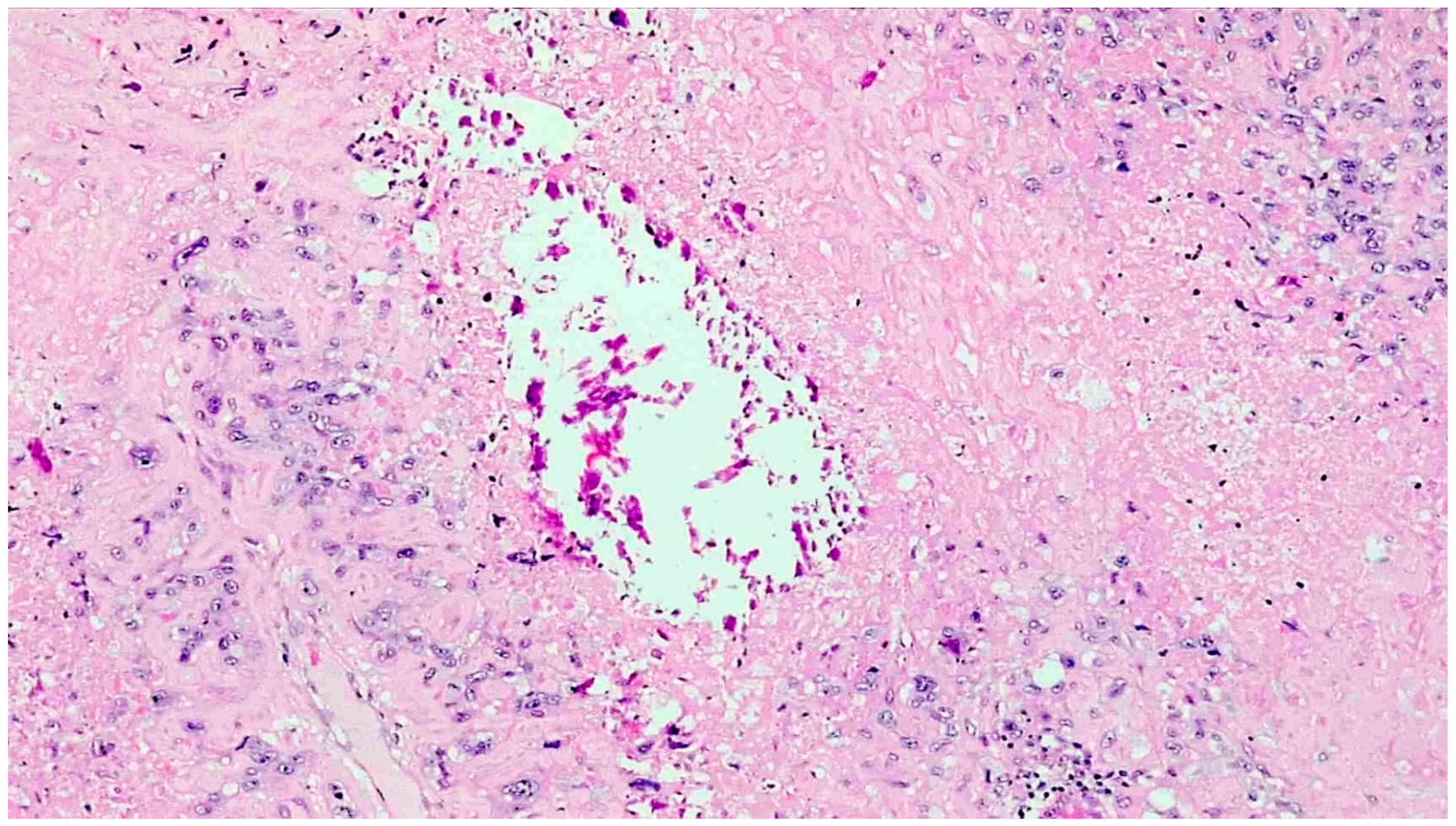
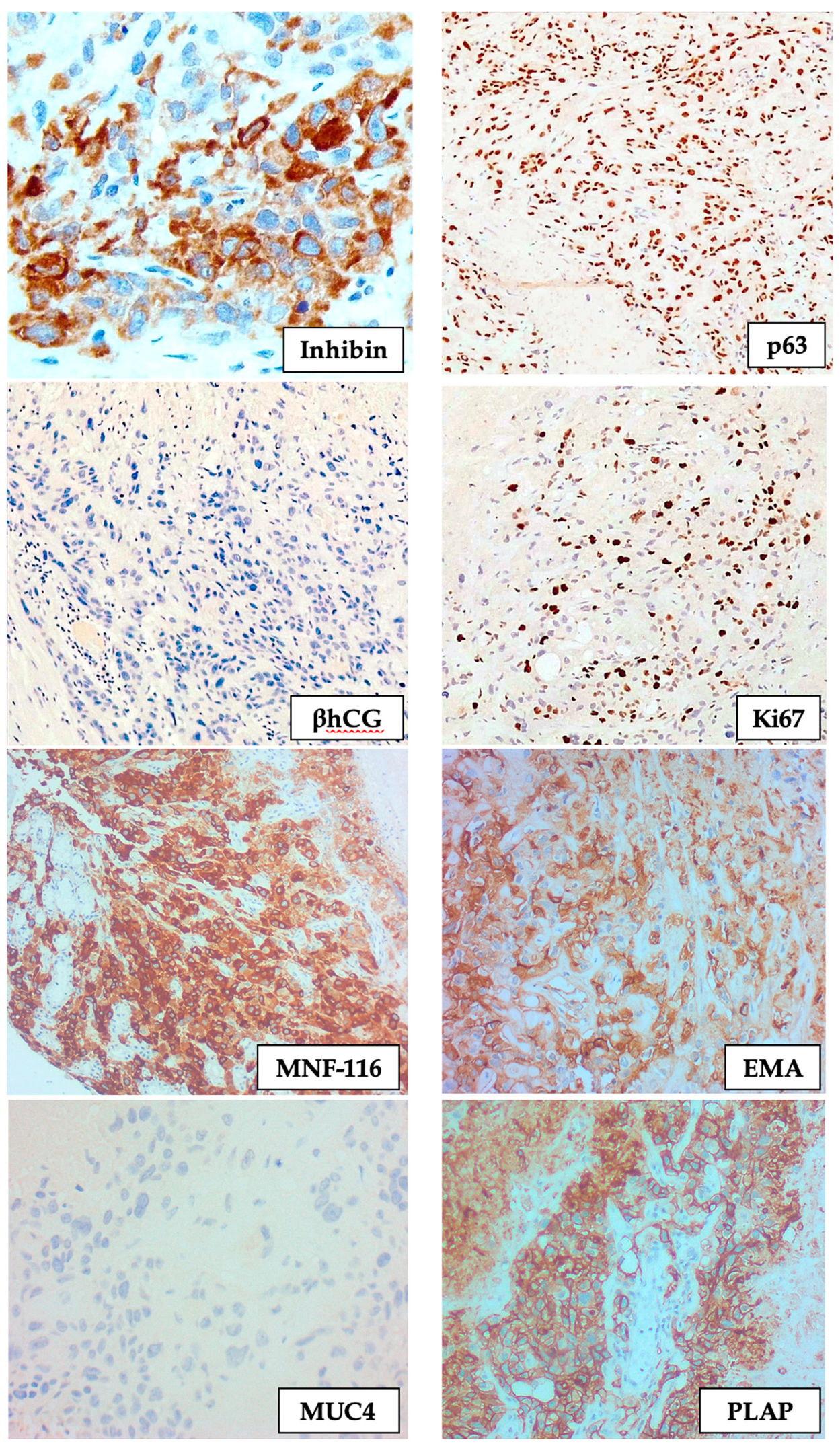
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shih, I.M. Gestational trophoblastic neoplasia-pathogenesis and potential therapeutic targets. Lancet Oncol. 2007, 8, 642–650. [Google Scholar] [CrossRef]
- Knöfler, M.; Haider, S.; Saleh, L.; Pollheimer, J.; Gamage, T.K.; James, J. Human placenta and trophoblast development: Key molecular mechanisms and model systems. Cell Mol. Life Sci. 2019, 76, 3479–3496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cierna, Z.; Varga, I.; Danihel, L.; Kuracinova, K.; Janegova, A. Intermediate trophoblast—A distinctive, unique and often unrecognized population of trophoblastic cells. Ann. Anat. Anat. Anz. 2016, 204, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Shih, I.M.; Kurman, R.J. Epithelioid trophoblastic tumor: A neoplasm distinct from choriocarcinoma and placental site tropho-blastic tumor simulating carcinoma. Am. J. Surg. Pathol. 1998, 22, 1393–1403. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Carinelli, S.; Guerrieri, M.E.; Aletti, G.D. Placental site trophoblastic tumor and epithelioid trophoblastic tumor: Clinical and pathological features, prognostic variables and treatment strategy. Gynecol. Oncol. 2019, 153, 684–693. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, N.S.; Goldstein, D.P.; Berkowitz, R.S. Placental site trophoblastic tumors and epithelioid trophoblastic tumors: Biology, natural history, and treatment modalities. Gynecol. Oncol. 2017, 144, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lü, W.; Lü, B. Epithelioid Trophoblastic Tumor: An Outcome-Based Literature Review of 78 Reported Cases. Int. J. Gynecol. Cancer 2013, 23, 1334–1338. [Google Scholar] [CrossRef] [PubMed]
- Seckl, M.J.; Sebire, N.J.; Fisher, R.A.; Golfier, F.; Massuger, L.; Sessa, C.; ESMO Guidelines Working Group. Gestational trophoblastic disease: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013, 24 (Suppl. 6), vi39–vi50. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Xiang, Y.; Guo, L.-N. Laparoscopic diagnosis and treatment of an isolated epithelioid trophoblastic tumor in recto-uterine pouch. J. Obstet. Gynaecol. Res. 2018, 44, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Trujillo, A.; Martínez-Serrano, M.J.; Saco, A.; Torné, A. Two cases of epithelioid trophoblastic tumors in postmenopausal women. Menopause 2017, 24, 1304–1308. [Google Scholar] [CrossRef] [PubMed]
- Coulson, L.E.; Kong, C.S.; Zaloudek, C. Epithelioid trophoblastic tumor of the uterus in a postmenopausal woman: A case report and review of the literature. Am. J. Surg. Pathol. 2000, 24, 1558–1562. [Google Scholar] [CrossRef]
- Fadare, O.; Parkash, V.; Carcangiu, M.-L.; Hui, P. Epithelioid trophoblastic tumor: Clinicopathological features with an emphasis on uterine cervical involvement. Mod. Pathol. 2006, 19, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Sung, W.J.; Shin, H.C.; Kim, M.-K.; Kim, M.J. Epithelioid Trophoblastic Tumor: Clinicopathologic and Immunohistochemical Analysis of Three Cases. Korean J. Pathol. 2013, 47, 67–73. [Google Scholar] [CrossRef]
- Sobecki-Rausch, J.; Winder, A.; Maniar, K.P.; Hoekstra, A.V.; Berry, E.; Novak, K.; Lurain, J.R. Surgery and Platinum/Etoposide-Based Chemotherapy for the Treatment of Epithelioid Trophoblastic Tumor. Int. J. Gynecol. Cancer 2018, 28, 1117–1122. [Google Scholar] [CrossRef]
- Lei, W.; Zhang, F.; Zheng, C.; Zhao, C.; Tu, S.; Bao, Y. Metastatic epithelioid trophoblastic tumor of the lung: A case report. Medicine 2018, 97, e0306. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Lee, S.K.; Hwang, S.H.; Kim, J.-S.; Yoon, G.; Lee, Y.-Y.; Kim, T.-J.; Choi, C.H.; Kim, B.-G.; Bae, D.-S.; et al. Extrauterine epithelioid trophoblastic tumor in hysterectomized woman. Obstet. Gynecol. Sci. 2017, 60, 124–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Zong, L.; Wang, J.; Wan, X.; Feng, F.; Xiang, Y. Epithelioid Trophoblastic Tumors: Treatments, Outcomes, and Potential Therapeutic Targets. J. Cancer 2019, 10, 11–19. [Google Scholar] [CrossRef] [PubMed]
- NCCN Guideline Gestational Trophoblastic Neoplasia Version 2.2021; 31 Mar 21. Available online: https://www.nccn.org/professionals/physician_gls/pdf/gtn.pdf (accessed on 25 October 2021).
- NHS Urgent Clinical Commissioning Policy Statement: Pembrolizumab for Drug-Resistant Gestational Trophoblastic Neo-plasia. NHS England Reference: 170027P. Available online: https://www.england.nhs.uk/wp-content/uploads/2018/12/Pembrolizumab-for-drug-resistant-gestational-trophoblastic-neoplasia.pdf (accessed on 24 October 2021).
- Eiriksson, L.; Dean, E.; Sebastianelli, A.; Salvador, S.; Comeau, R.; Jang, J.-H.; Bouchard-Fortier, G.; Osborne, R.; Sauthier, P. Guideline No. 408: Management of Gestational Trophoblastic Diseases. J. Obstet. Gynaecol. Can. 2021, 43, 91–105.e1. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Locus | Chromosome Location | Tumour | Patient (Mother) | Biological Father | Child-2003 | Child-2006 | Comments |
|---|---|---|---|---|---|---|---|
| D3S1358 | 3p21.31 | 15/17 | 15/15 | 17/17 | 15/17 | 15/17 | Non-maternal allele |
| vWA | 12p13.31 | 14/17 | 17/17 | 14/16 | 14/17 | 16/17 | Non-maternal allele (2003) |
| D16S539 | 16q24.1 | 11/11 | 11/11 | 9/11 | 11 | 9/11 | Non informative |
| CSF1PO | 5q33.3-34 | 10/11/14 | 11/14 | 10/12 | 10/11 | 12/14 | Non-maternal allele (2003) |
| TPOX | 2p23-2per | 8/10 | 8/8 | 8/10 | 8/10 | 8/10 | NMA |
| Y | Yq11.221 | – | – | 2 | – | 2 | Non informative |
| Amelogenin | X:p22.1-22.3 Y:p11.2 | XX | XX | XY | XX | XY | - |
| D8S1179 | 8q24.13 | 10/13 | 10/13 | 13/14 | 13/13 | 10/13 | Not informative |
| D21S11 | 21q11.2-q21 | 29/30/32.2 | 29/32.2 | 29/30 | 30/32.2 | 29/30 | Non-maternal allele |
| D18S51 | 18q21.33 | 12/13/17 | 12/17 | 12/13 | 12/13 | 12/13 | Non-maternal allele |
| DYS391 | Yq11.21 | – | – | 10 | – | 10 | - |
| D2S441 | 2p14 | 11/11.3/12 | 11/11.3 | 12/14.3 | 11/12 | 11/14.3 | Non-maternal allele (2003) |
| D19S433 | 19q12 | 13/14.2 | 13/13 | 14/14.2 | 13/14.2 | 13/14 | Non-maternal allele (2003) |
| TH01 | 11p15.5 | 9/9.3/10 | 9.3/10 | 9/9 | 9/10 | 9/10 | Non-maternal allele |
| FGA | 4q28 | 19/22/24 | 19/24 | 20/22 | 22/24 | 20/24 | Non-maternal allele (2003) |
| D22S1045 | 22q12.3 | 11/16/18 | 16/18 | 11/16 | 11/16 | 16/18 | Non-maternal allele (2003) |
| D5S818 | 5q21-31 | 8/11 | 11/11 | 8/11 | 8/11 | 8/11 | Non-maternal allele |
| D13S317 | 13q22-31 | 12/12 | 12/12 | 11/12 | 12/12 | 12/12 | Not informative |
| D7S820 | 7q11.21-22 | 11/11 | 11/11 | 10/11 | 11/11 | 11/11 | Not informative |
| SE33 | 6q14 | 16/24.2/26.2 | 16/24.2 | 26.2/31 | 24.2/26.2 | 16/31 | Non-maternal allele (2003) |
| D10S1248 | 10q26.3 | 12/13 | 12/13 | 12/15 | 12/13 | 12/15 | Not informative |
| D1S1656 | 1q42.2 | 11/13/14 | 13/14 | 11/19.3 | 11/13 | 11/13 | Non-maternal allele |
| D12S391 | 12p13.2 | 19/20/24 | 20/24 | 19/20 | 19/20 | 19/20 | Non-maternal allele |
| D2S1338 | 2q35 | 17/23 | 17/23 | 22/23 | 17/23 | 22/23 | Not informative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisani, D.; Calleja-Agius, J.; Di Fiore, R.; O’Leary, J.J.; Beirne, J.P.; O’Toole, S.A.; Felix, A.; Said-Huntingford, I. Epithelioid Trophoblastic Tumour: A Case with Genetic Linkage to a Child Born over Seventeen Years Prior, Successfully Treated with Surgery and Pembrolizumab. Curr. Oncol. 2021, 28, 5346-5355. https://doi.org/10.3390/curroncol28060446
Pisani D, Calleja-Agius J, Di Fiore R, O’Leary JJ, Beirne JP, O’Toole SA, Felix A, Said-Huntingford I. Epithelioid Trophoblastic Tumour: A Case with Genetic Linkage to a Child Born over Seventeen Years Prior, Successfully Treated with Surgery and Pembrolizumab. Current Oncology. 2021; 28(6):5346-5355. https://doi.org/10.3390/curroncol28060446
Chicago/Turabian StylePisani, David, Jean Calleja-Agius, Riccardo Di Fiore, John J. O’Leary, James P. Beirne, Sharon A. O’Toole, Ana Felix, and Ian Said-Huntingford. 2021. "Epithelioid Trophoblastic Tumour: A Case with Genetic Linkage to a Child Born over Seventeen Years Prior, Successfully Treated with Surgery and Pembrolizumab" Current Oncology 28, no. 6: 5346-5355. https://doi.org/10.3390/curroncol28060446
APA StylePisani, D., Calleja-Agius, J., Di Fiore, R., O’Leary, J. J., Beirne, J. P., O’Toole, S. A., Felix, A., & Said-Huntingford, I. (2021). Epithelioid Trophoblastic Tumour: A Case with Genetic Linkage to a Child Born over Seventeen Years Prior, Successfully Treated with Surgery and Pembrolizumab. Current Oncology, 28(6), 5346-5355. https://doi.org/10.3390/curroncol28060446