Probiotics Evaluation in Oncological Surgery: A Systematic Review of 36 Randomized Controlled Trials Assessing 21 Diverse Formulations

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
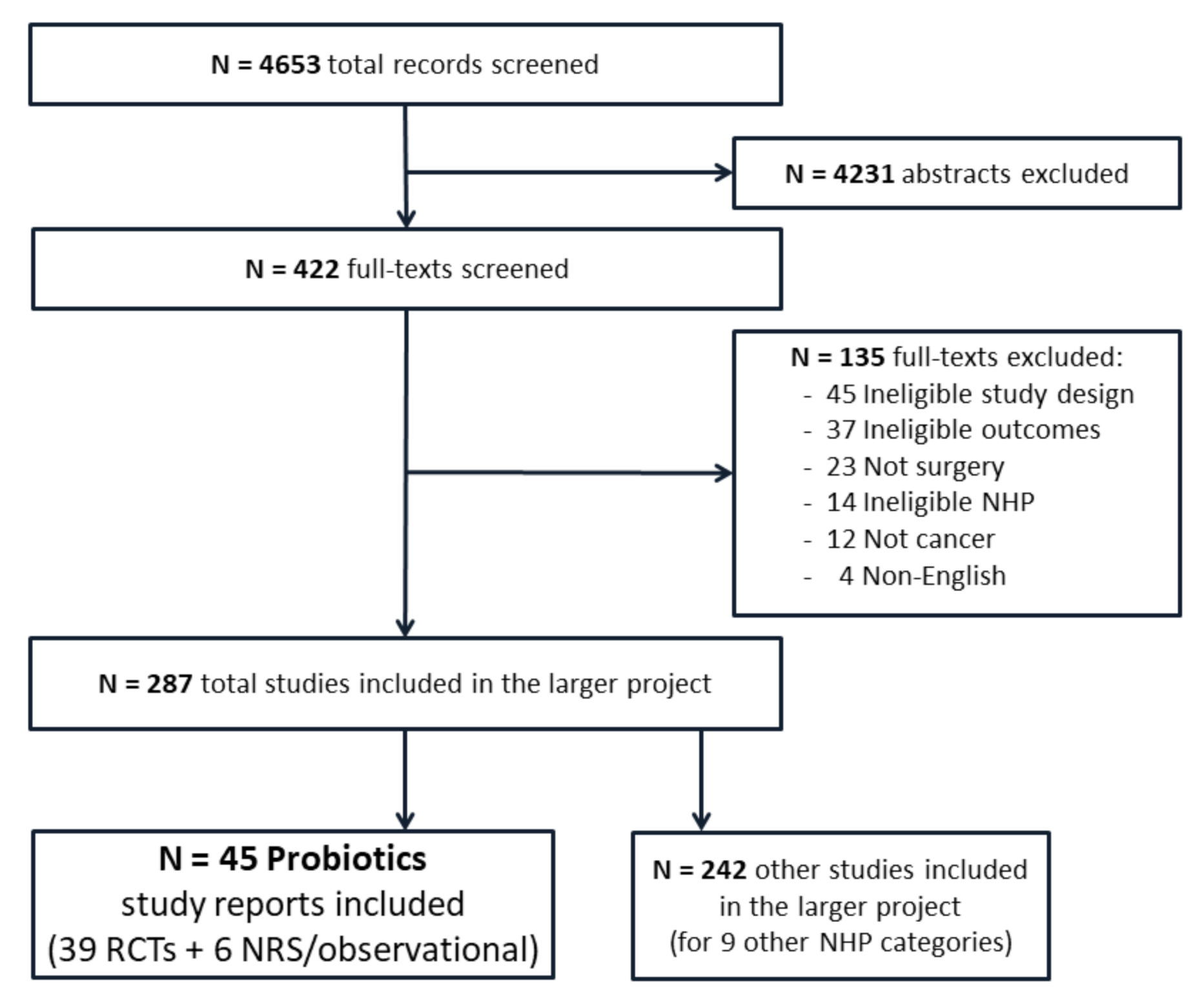
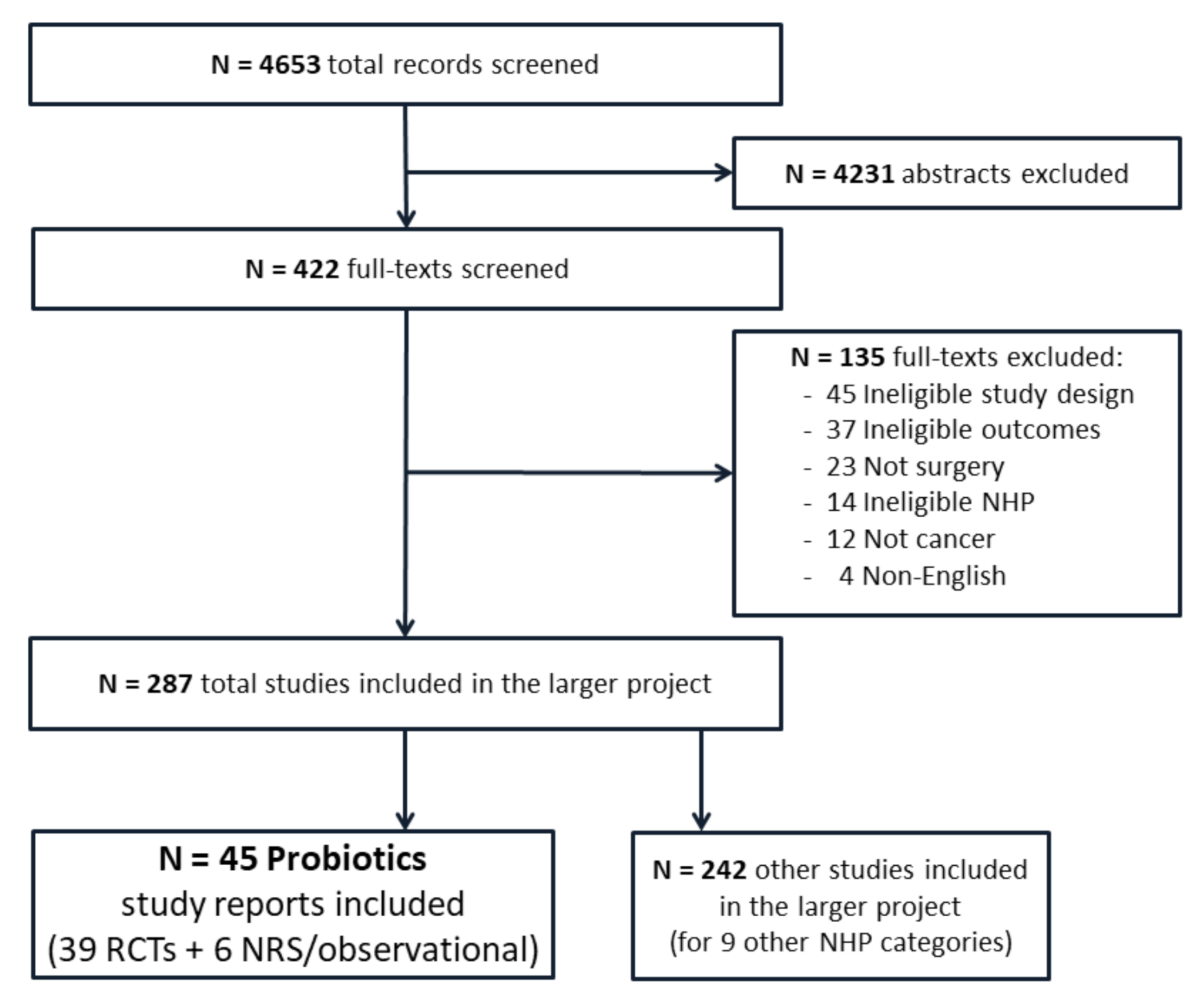
3.1. Included Studies
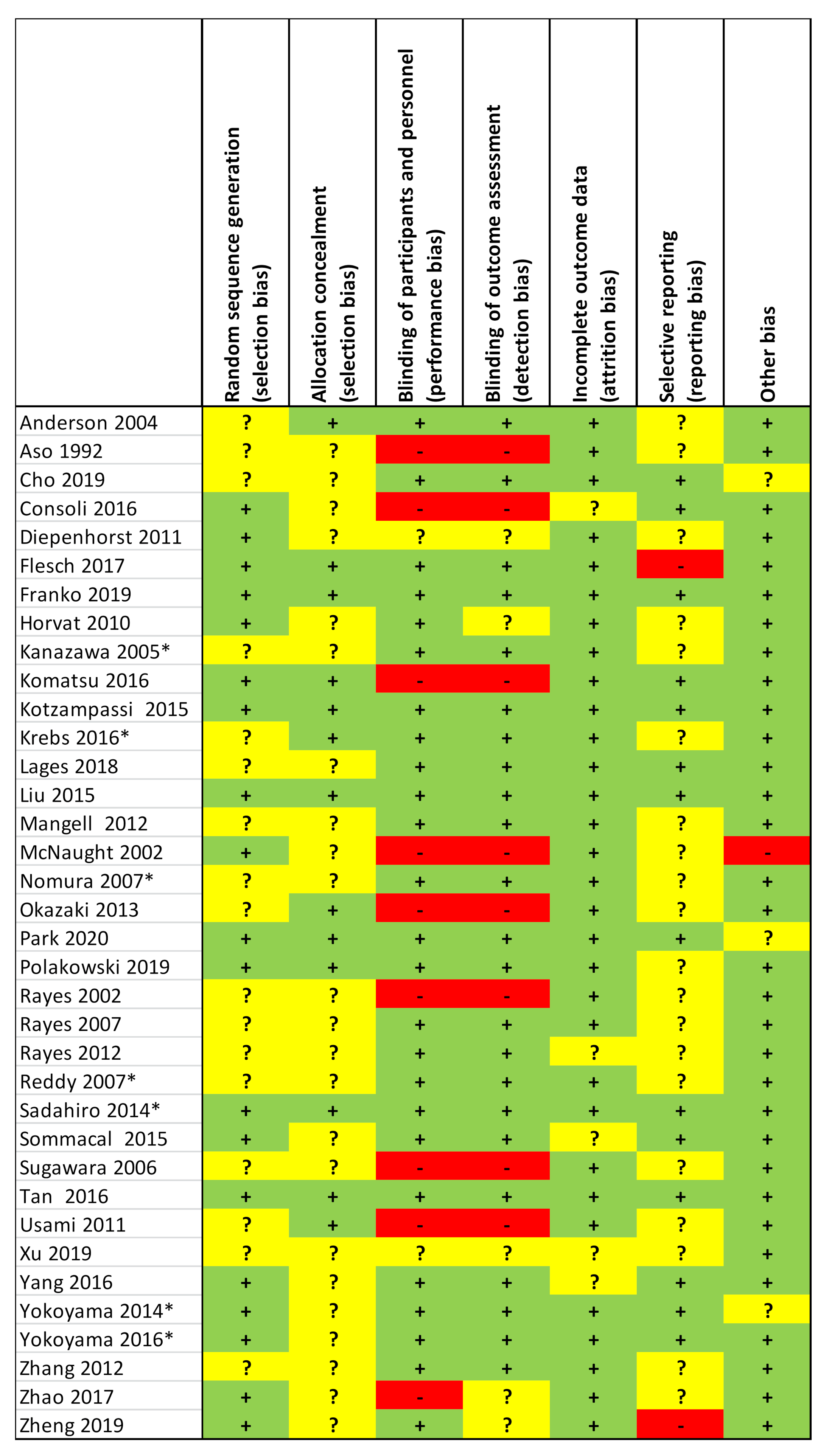
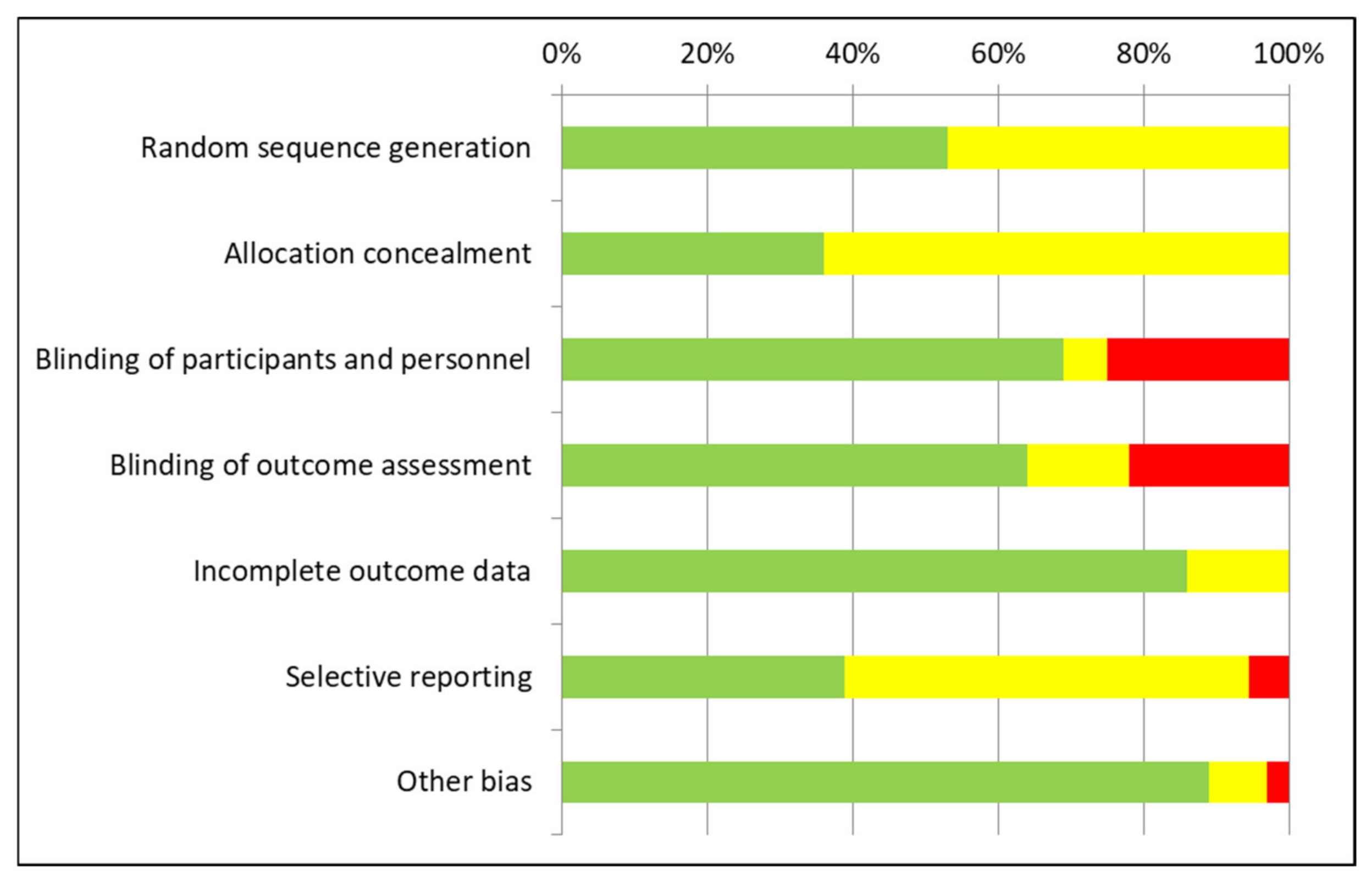
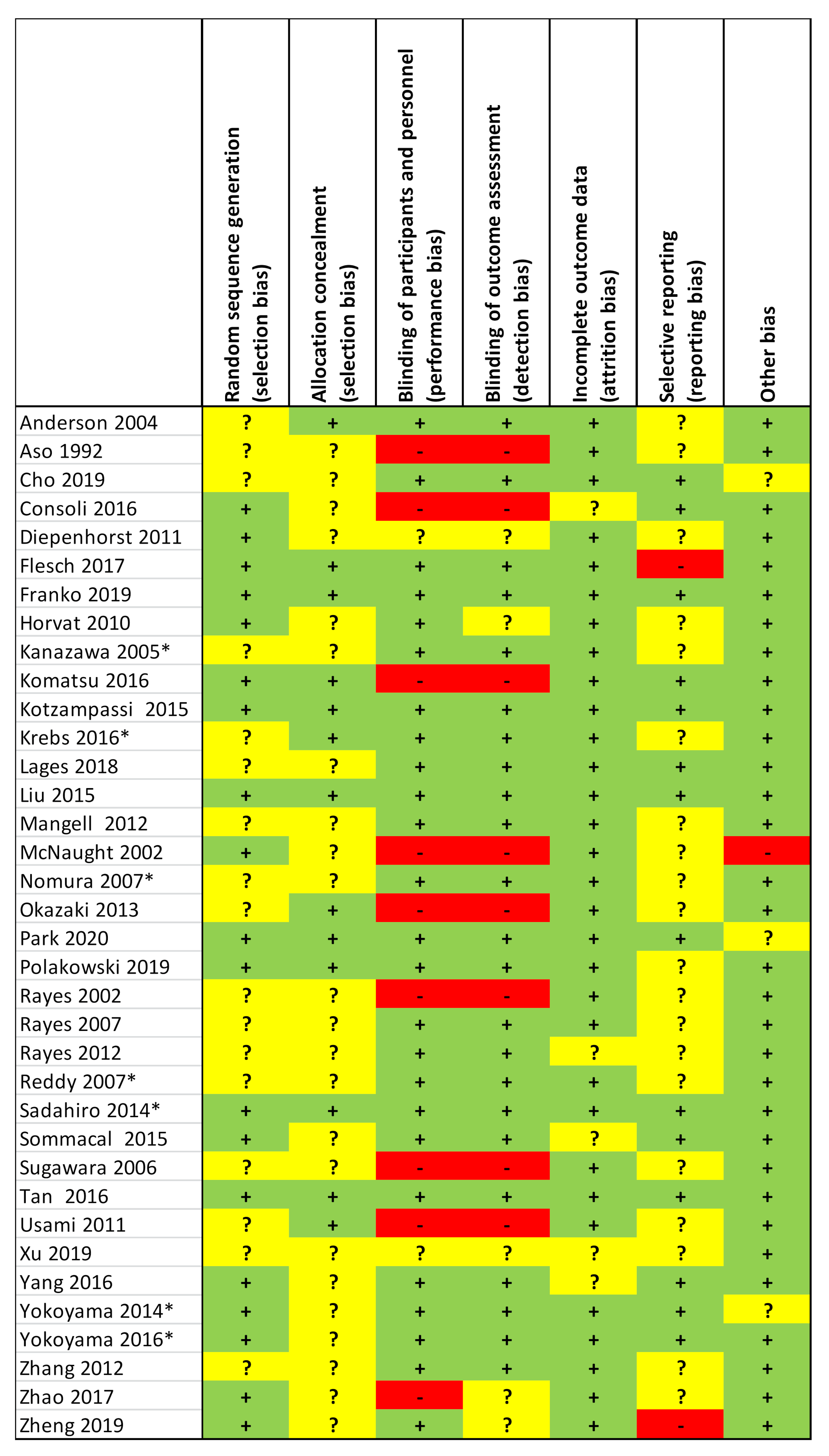
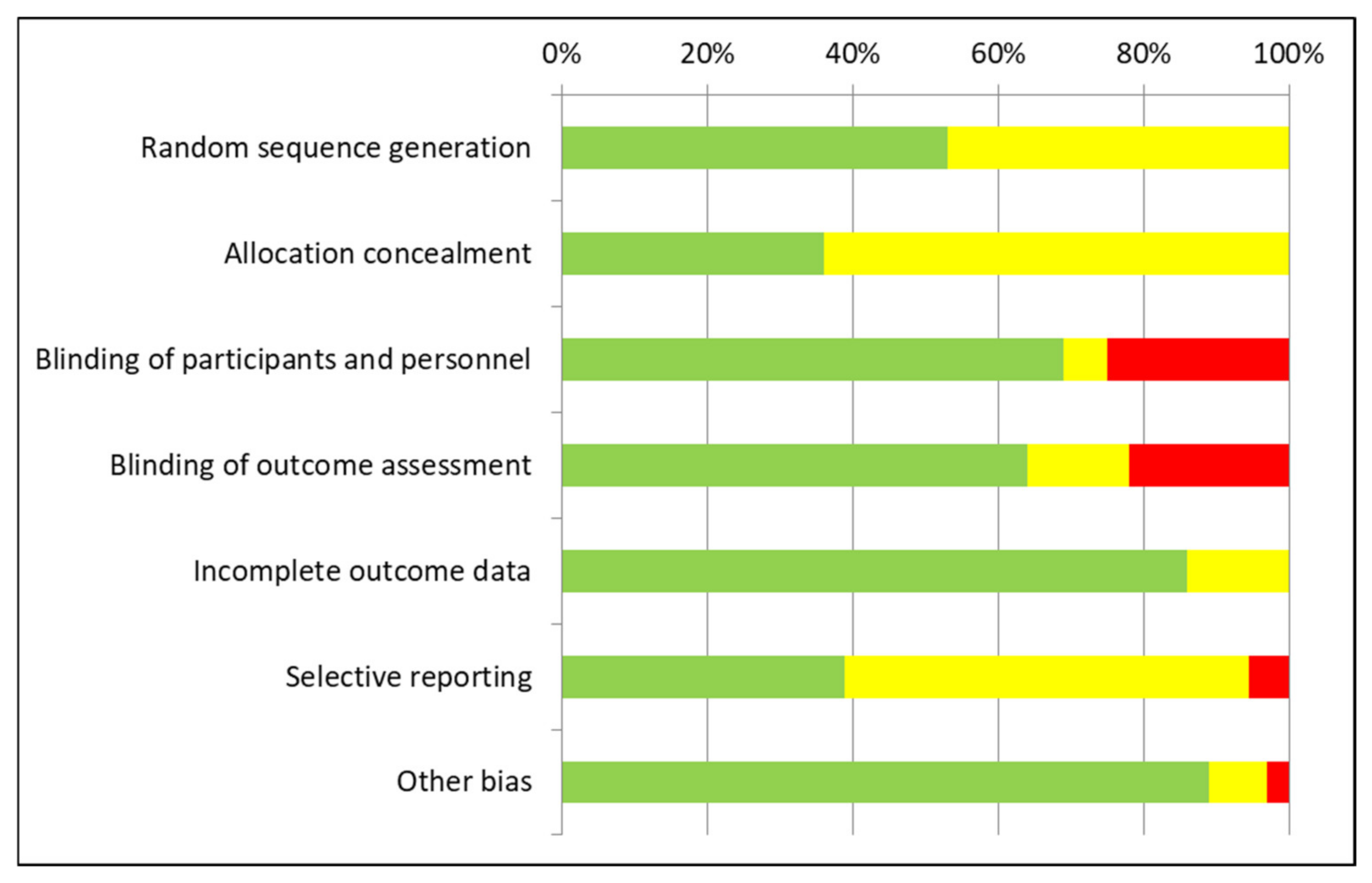
3.2. Risk-of-Bias Appraisal
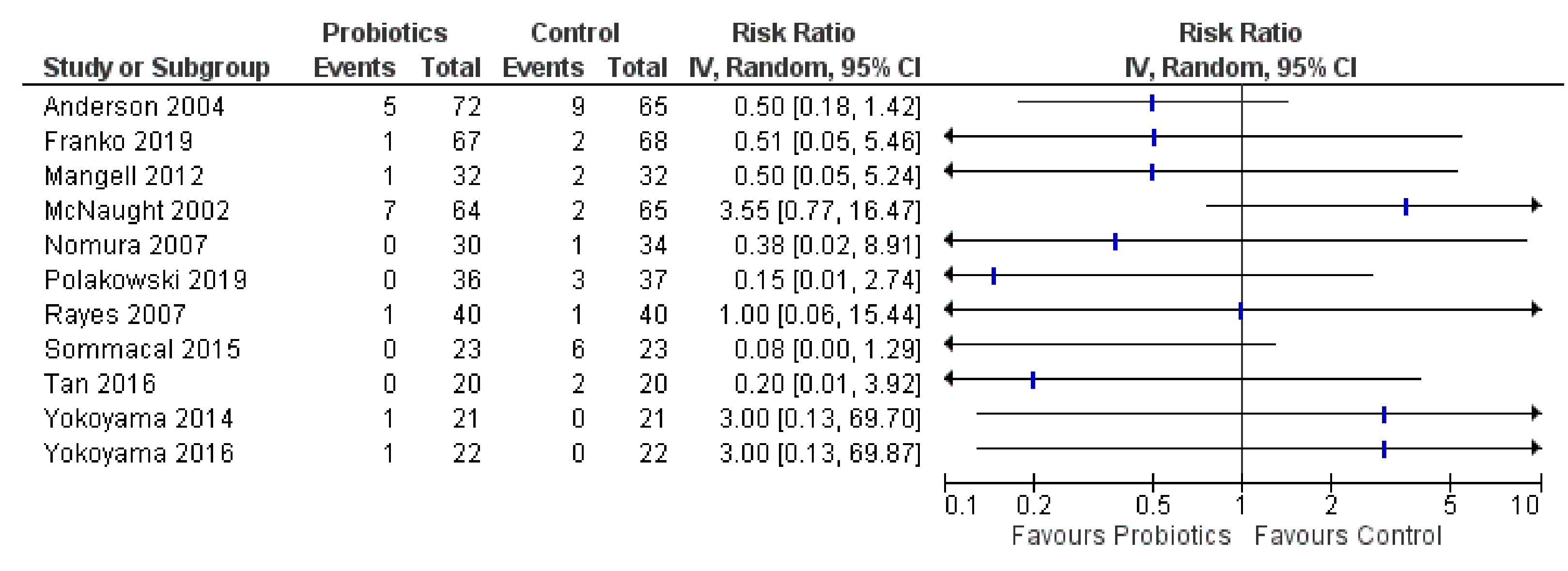
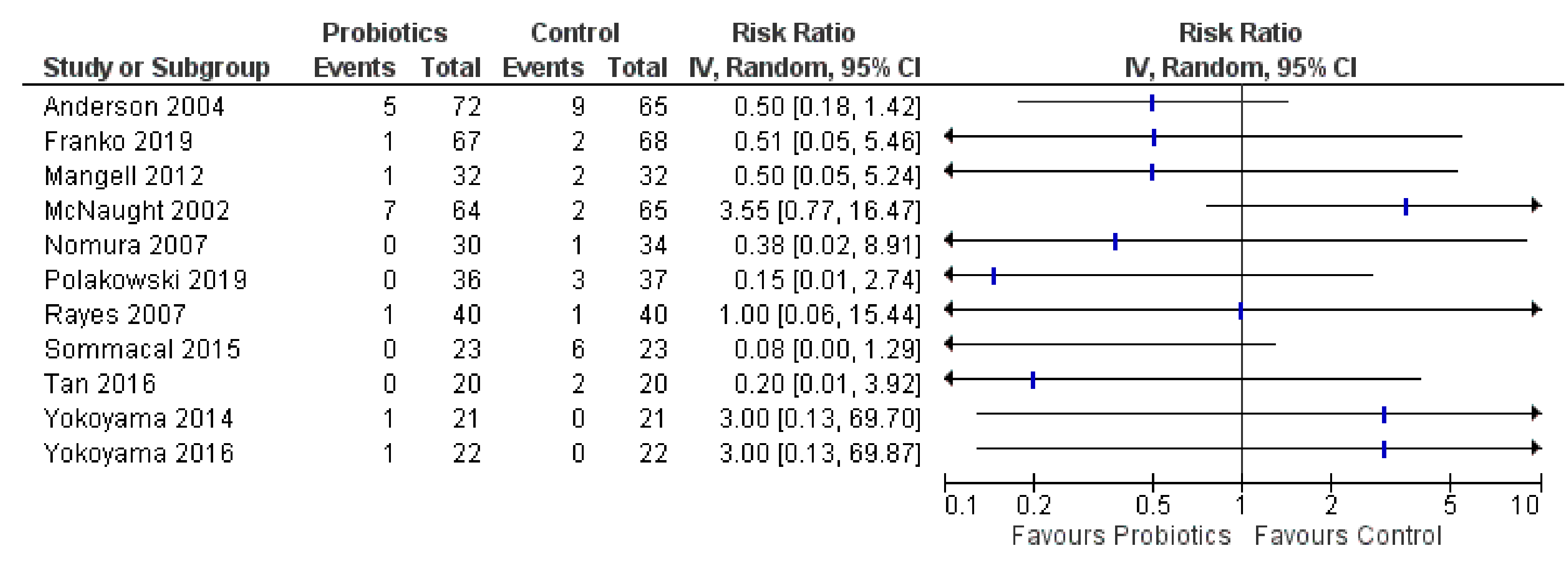
3.3. Mortality and Recurrence
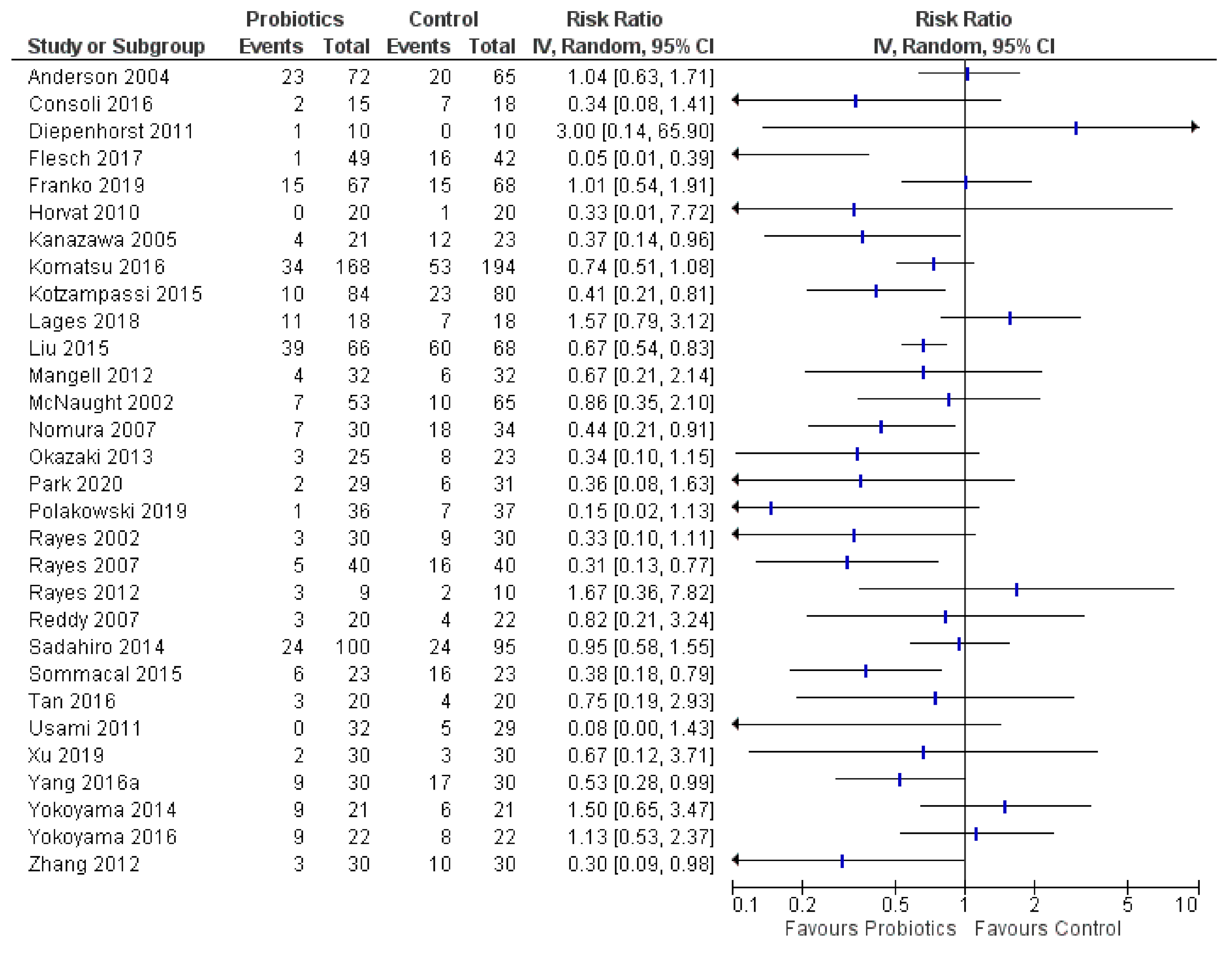
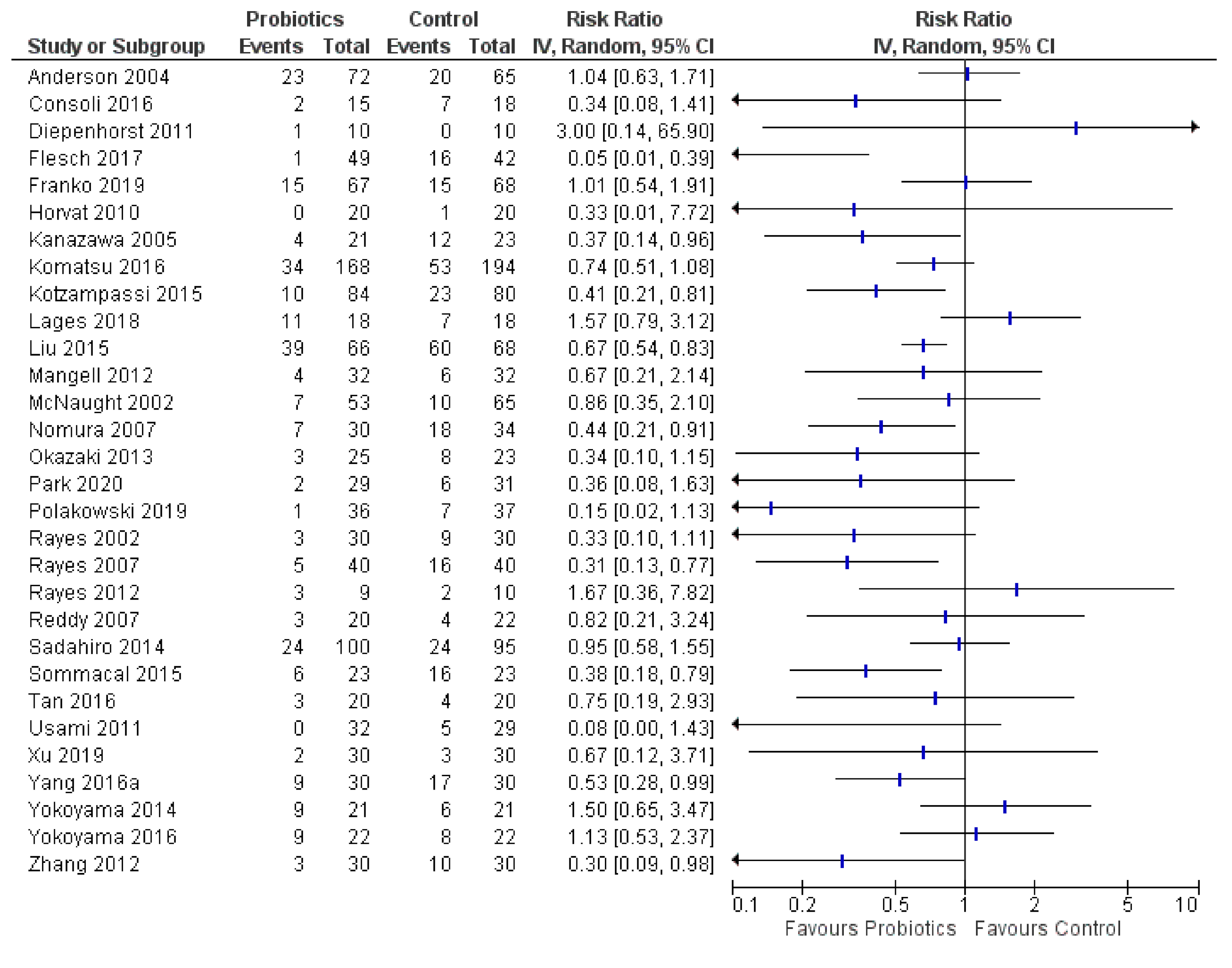
3.4. Postoperative Infections
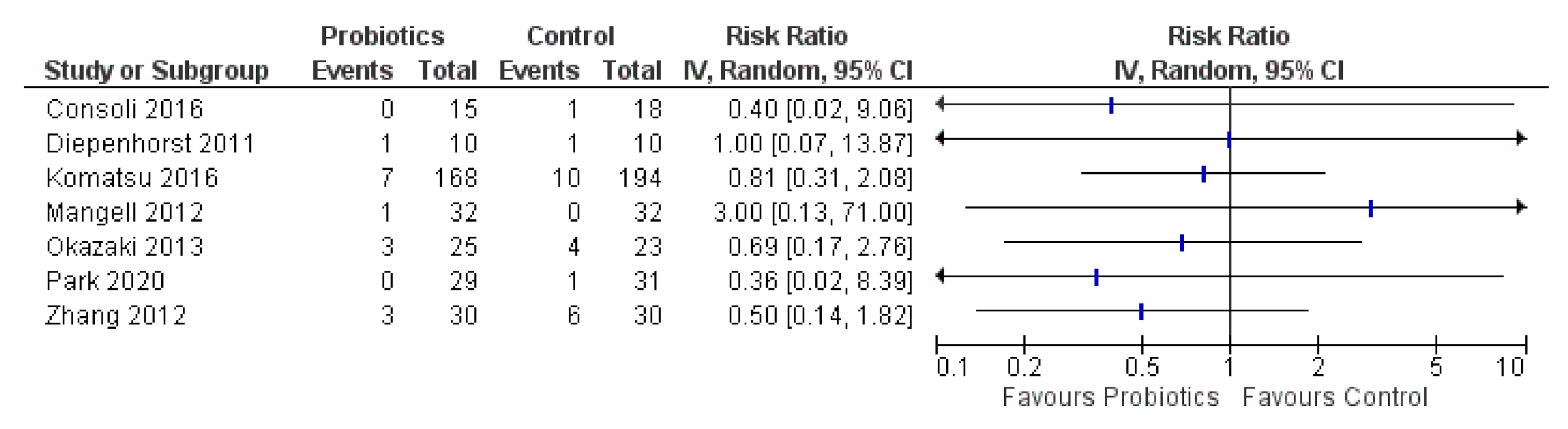
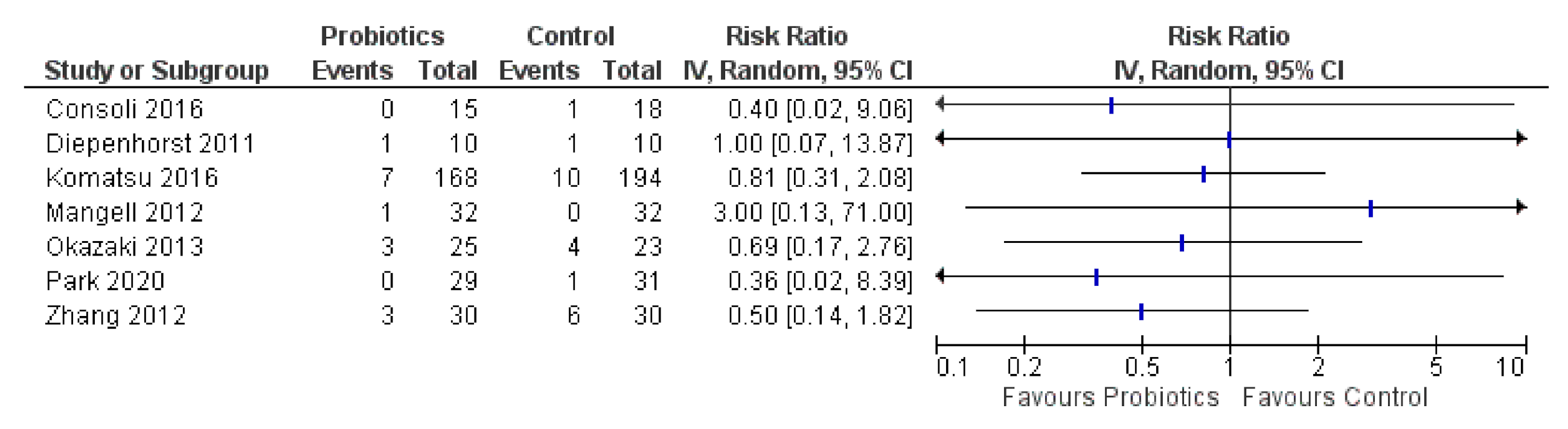
3.5. Ileus and Intestinal Obstruction
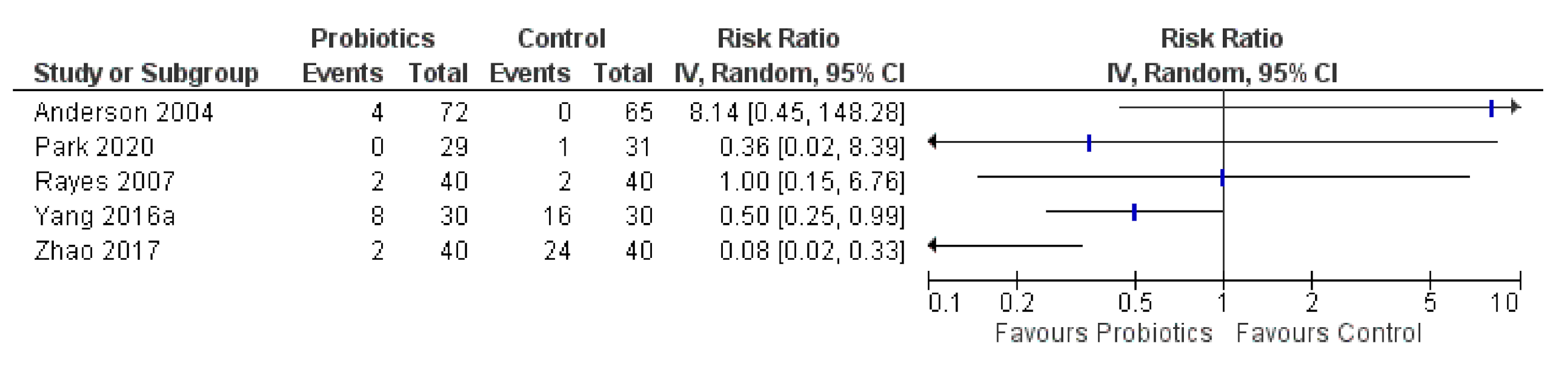
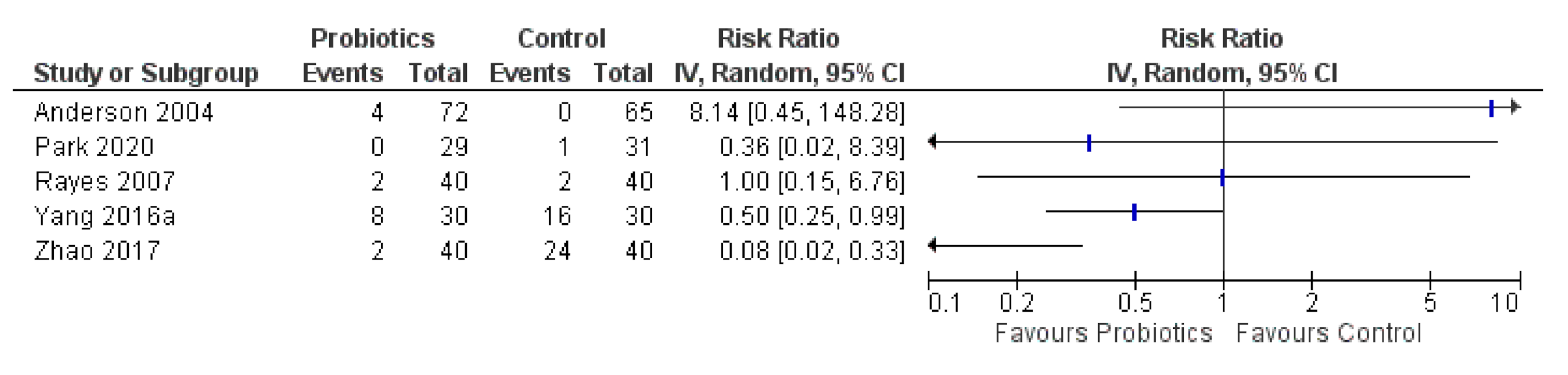
3.6. Diarrhea
3.7. White Blood Cells and C-Reactive Protein
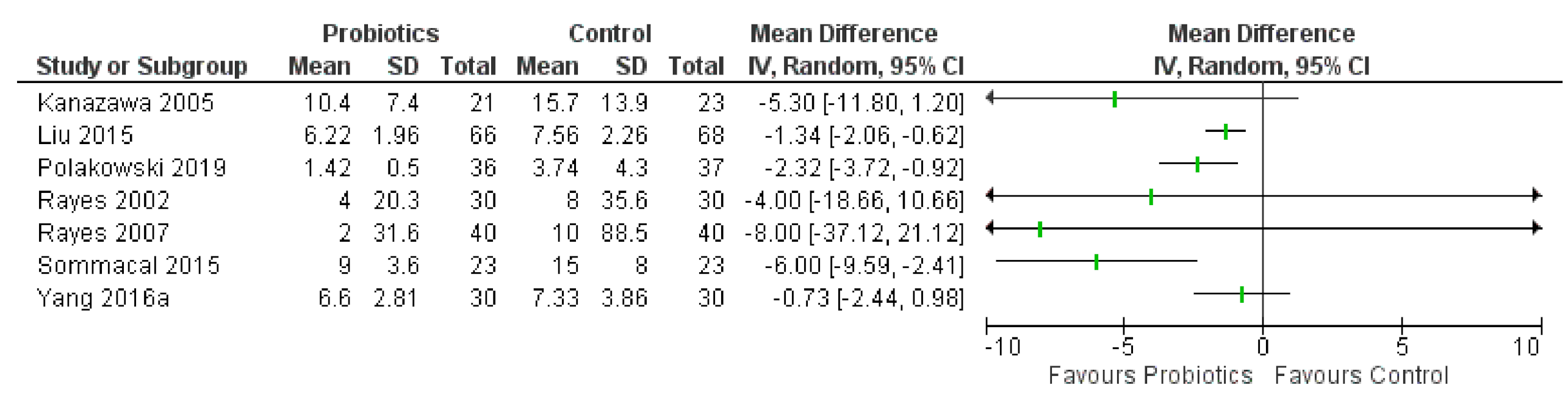
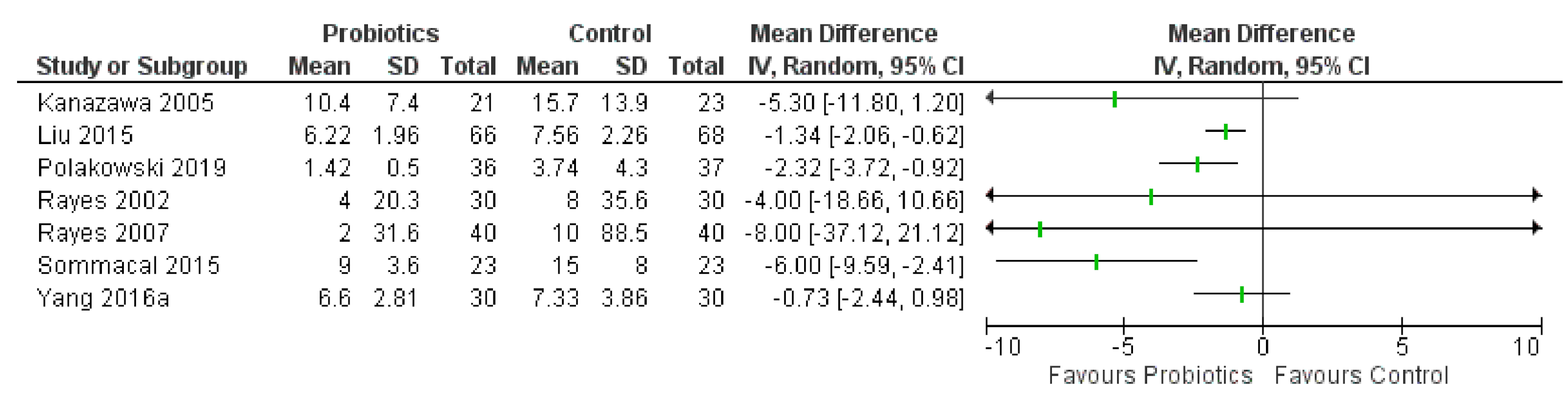
3.8. Hospital Length of Stay
3.9. Additional Outcomes
3.10. Adverse Events in RCTs
3.11. Nonrandomized and Observational Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Integrative HMP (iHMP) Research Network Consortium. The Integrative Human Microbiome Project. Nature 2019, 569, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Sanders, M.E.; Merenstein, D.J.; Reid, G.; Gibson, G.R.; Rastall, R.A. Probiotics and prebiotics in intestinal health and disease: From biology to the clinic. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Farhana, L.; Banerjee, H.N.; Verma, M.; Majumdar, A.P.N. Role of Microbiome in Carcinogenesis Process and Epigenetic Regulation of Colorectal Cancer. Methods Mol. Biol. 2018, 1856, 35–55. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, R.F.; Jobin, C. The microbiome and cancer. Nat. Rev. Cancer 2013, 13, 800–812. [Google Scholar] [CrossRef] [Green Version]
- Round, J.L.; Mazmanian, S.K. The gut microbiota shapes intestinal immune responses during health and disease. Nat. Rev. Immunol. 2009, 9, 313–323. [Google Scholar] [CrossRef]
- Zitvogel, L.; Galluzzi, L.; Viaud, S.; Vetizou, M.; Daillere, R.; Merad, M.; Kroemer, G. Cancer and the gut microbiota: An unexpected link. Sci. Transl. Med. 2015, 7, 271ps1. [Google Scholar] [CrossRef] [Green Version]
- Lederer, A.K.; Pisarski, P.; Kousoulas, L.; Fichtner-Feigl, S.; Hess, C.; Huber, R. Postoperative changes of the microbiome: Are surgical complications related to the gut flora? A systematic review. BMC Surg. 2017, 17, 125. [Google Scholar] [CrossRef] [Green Version]
- Kusachi, S.; Kashimura, N.; Konishi, T.; Shimizu, J.; Kusunoki, M.; Oka, M.; Wakatsuki, T.; Kobayashi, J.; Sawa, Y.; Imoto, H.; et al. Length of stay and cost for surgical site infection after abdominal and cardiac surgery in Japanese hospitals: Multi-center surveillance. Surg. Infect. 2012, 13, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization of the United Nations; World Health Organization. Guidelines for the Evaluation of Probiotics in Food, Report of a Joint FAO/WHO Working Group on Drafting Guidelines for the Evaluation of Probiotics in Food; World Health Organization: London, UK; Ottawa, ON, Canada, 2002. [Google Scholar]
- Wieërs, G.; Belkhir, L.; Enaud, R.; Leclercq, S.; de Foy, J.M.P.; Dequenne, I.; de Timary, P.; Cani, P.D. How Probiotics Affect the Microbiota. Front. Cell. Infect. Microbiol. 2020, 9, 454. [Google Scholar] [CrossRef] [Green Version]
- Darbandi, A.; Mirshekar, M.; Shariati, A.; Moghadam, M.T.; Lohrasbi, V.; Asadolahi, P.; Talebi, M. The effects of probiotics on reducing the colorectal cancer surgery complications: A periodic review during 2007–2017. Clin. Nutr. 2020, 39, 2358–2367. [Google Scholar] [CrossRef] [PubMed]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Markowiak, P.; Śliżewska, K. Effects of Probiotics, Prebiotics, and Synbiotics on Human Health. Nutrients 2017, 9, 1021. [Google Scholar] [CrossRef]
- Vlasova, A.N.; Kandasamy, S.; Chattha, K.S.; Rajashekara, G.; Saif, L.J. Comparison of probiotic lactobacilli and bifidobacteria effects, immune responses and rotavirus vaccines and infection in different host species. Vet. Immunol. Immunopathol. 2016, 172, 72–84. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.D.; Xu, W.; Liu, M.M.; Hu, K.J.; Sun, Y.Y.; Yang, X.F.; Zhu, G.Q.; Wang, Z.W.; Huang, W. Efficacy of prophylactic probiotics in combination with antibiotics versus antibiotics alone for colorectal surgery: A meta-analysis of randomized controlled trials. J. Surg. Oncol. 2018, 117, 1394–1404. [Google Scholar] [CrossRef]
- Thomas, C.M.; Versalovic, J. Probiotics-host communication: Modulation of signaling pathways in the intestine. Gut Microbes 2010, 1, 148–163. [Google Scholar] [CrossRef] [PubMed]
- McFarland, L.V.; Evans, C.T.; Goldstein, E.J.C. Strain-Specificity and Disease-Specificity of Probiotic Efficacy: A Systematic Review and Meta-Analysis. Front. Med. 2018, 5, 124. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.E.; Akkermans, L.M.; Haller, D.; Hammerman, C.; Heimbach, J.; Hörmannsperger, G.; Huys, G.; Levy, D.D.; Lutgendorff, F.; Mack, D.; et al. Safety assessment of probiotics for human use. Gut Microbes 2010, 1, 164–185. [Google Scholar] [CrossRef]
- World Gastroenterology Organisation (WGO), Guidelines and Publications Committee. WGO Global Guidelines: Probiotics and Prebiotics; World Gastroenterology Organisation: Milwaukee, WI, USA, 2017; Available online: https://www.worldgastroenterology.org/guidelines/global-guidelines/probiotics-and-prebiotics (accessed on 1 September 2021).
- Health Canada, Natural and Non-Prescription Health Products Directorate. Probiotics Monograph; Health Canada: Ottawa, ON, Canada, 2019. Available online: http://webprod.hc-sc.gc.ca/nhpid-bdipsn/atReq.do?atid=probio&lang=eng (accessed on 1 September 2021).
- Didari, T.; Solki, S.; Mozaffari, S.; Nikfar, S.; Abdollahi, M. A systematic review of the safety of probiotics. Expert. Opin. Drug Saf. 2014, 13, 227–239. [Google Scholar] [CrossRef]
- Natural Medicines. Probiotics Professional Monograph; Therapeutic Research Center: Denver, CO, USA, 2020; Available online: https://naturalmedicines.therapeuticresearch.com/ (accessed on 1 September 2021).
- Cogo, E.; Elsayed, M.; Liang, V.; Cooley, K.; Guerin, C.; Psihogios, A.; Papadogianis, P. Are Supplemental Branched-Chain Amino Acids Beneficial During the Oncological Peri-Operative Period: A Systematic Review and Meta-Analysis. Integr. Cancer Ther. 2021, 20, 1–25. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2 (Updated February 2021); Cochrane: London, UK, 2021; Available online: https://training.cochrane.org/handbook (accessed on 1 September 2021).
- CIOMS Working Group. Evidence Synthesis and Meta-Analysis for Drug Safety: Report of CIOMS Working Group X; Council for International Organizations of Medical Sciences (CIOMS): Geneva, Switzerland, 2016; Available online: https://cioms.ch/publications/product/evidence-synthesis-and-meta-analysis-report-of-cioms-working-group-x/ (accessed on 1 September 2021).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Cogo, E.; Papadogianis, P. Characteristics of 218 Recent Reviews on Natural Health Products in Integrative Cancer Care: A bibliometric analysis of trends in the human research literature. J. Orthomol. Med. 2018, 33, 1–13. [Google Scholar]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 September 2021).
- The Cochrane Collaboration. Review Manager (RevMan), version 5.4; The Cochrane Collaboration: London, UK, 2020.
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, 16890. [Google Scholar] [CrossRef] [Green Version]
- Anderson, A.D.; McNaught, C.E.; Jain, P.K.; MacFie, J. Randomised clinical trial of synbiotic therapy in elective surgical patients. Gut 2004, 53, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Aso, Y.; Akazan, H. Prophylactic effect of a Lactobacillus casei preparation on the recurrence of superficial bladder cancer. BLP Study Group. Urol. Int. 1992, 49, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.R.; Yoon, B.J.; Oh, H.K. Effect of Probiotics on Bowel Function Restoration after Ileostomy Reversal in Patients with Rectal Cancer: A Double-Blind Randomized Controlled Trial. Gastroenterology 2019, 156, S-1421. [Google Scholar] [CrossRef]
- Consoli, M.L.; da Silva, R.S.; Nicoli, J.R.; Bruna, R.; da Silva, R.G.; de Vasconcelos Generoso, S.; Correia, M.I. Randomized Clinical Trial: Impact of Oral Administration of Saccharomyces boulardii on Gene Expression of Intestinal Cytokines in Patients Undergoing Colon Resection. JPEN J. Parenter. Enteral Nutr. 2016, 40, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Diepenhorst, G.M.; van Ruler, O.; Besselink, M.G.; van Santvoort, H.C.; Wijnandts, P.R.; Renooij, W.; Gouma, D.J.; Gooszen, H.G.; Boermeester, M.A. Influence of prophylactic probiotics and selective decontamination on bacterial translocation in patients undergoing pancreatic surgery: A randomized controlled trial. Shock 2011, 35, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Flesch, A.T.; Tonial, S.T.; Contu, P.C.; Damin, D.C.; Flesch, A.T.; Tonial, S. Perioperative synbiotics administration decreases postoperative infections in patients with colorectal cancer: A randomized, double-blind clinical trial. Rev. Col. Bras. Cir. 2017, 44, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Franko, J.; Raman, S.; Krishnan, N.; Frankova, D.; Tee, M.C.; Brahmbhatt, R.; Goldman, C.D.; Weigel, R.J. Randomized Trial of Perioperative Probiotics Among Patients Undergoing Major Abdominal Operation. J. Am. Coll. Surg. 2019, 229, 533–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horvat, M.; Krebs, B.; Potrc, S.; Ivanecz, A.; Kompan, L. Preoperative synbiotic bowel conditioning for elective colorectal surgery. Wien. Klin. Wochenschr. 2010, 122 (Suppl. 2), 26–30. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, H.; Nagino, M.; Kamiya, S.; Komatsu, S.; Mayumi, T.; Takagi, K.; Asahara, T.; Nomoto, K.; Tanaka, R.; Nimura, Y. Synbiotics reduce postoperative infectious complications: A randomized controlled trial in biliary cancer patients undergoing hepatectomy. Langenbecks Arch. Surg. 2005, 390, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, S.; Sakamoto, E.; Norimizu, S.; Shingu, Y.; Asahara, T.; Nomoto, K.; Nagino, M. Efficacy of perioperative synbiotics treatment for the prevention of surgical site infection after laparoscopic colorectal surgery: A randomized controlled trial. Surg. Today 2016, 46, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Kotzampassi, K.; Stavrou, G.; Damoraki, G.; Georgitsi, M.; Basdanis, G.; Tsaousi, G.; Giamarellos-Bourboulis, E. A Four-Probiotics Regimen Reduces Postoperative Complications After Colorectal Surgery: A Randomized, Double-Blind, Placebo-Controlled Study. World J. Surg. 2015, 39, 2776–2783. [Google Scholar] [CrossRef]
- Krebs, B.; Horvat, M.; Golle, A.; Krznaric, Z.; Papes, D.; Augustin, G.; Arslani, N.; Potrc, S. A randomized clinical trial of synbiotic treatment before colorectal cancer surgery. Am. Surg. 2013, 79, E340–E342. [Google Scholar] [CrossRef]
- Krebs, B.; Krebs, B. Prebiotic and Synbiotic Treatment before Colorectal Surgery--Randomised Double Blind Trial. Coll. Antropol. 2016, 40, 35–40. [Google Scholar] [PubMed]
- Lages, P.C.; Generoso, S.V.; Correia, M. Postoperative symbiotic in patients with head and neck cancer: A double-blind randomised trial. Br. J. Nutr. 2018, 119, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Qin, H.; Yang, Z.; Xia, Y.; Liu, W.; Yang, J.; Jiang, Y.; Zhang, H.; Yang, Z.; Wang, Y.; et al. Randomised clinical trial: The effects of perioperative probiotic treatment on barrier function and post-operative infectious complications in colorectal cancer surgery—A double-blind study. Aliment. Pharmacol. Ther. 2011, 33, 50–63. [Google Scholar] [CrossRef]
- Liu, Z.H.; Huang, M.J.; Zhang, X.W.; Wang, J.P.; Liu, Z.-H.; Huang, M.-J.; Zhang, X.-W.; Wang, L.; Huang, N.-Q.; Peng, H.; et al. The effects of perioperative probiotic treatment on serum zonulin concentration and subsequent postoperative infectious complications after colorectal cancer surgery: A double-center and double-blind randomized clinical trial. Am. J. Clin. Nutr. 2013, 97, 117–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Li, C.; Huang, M.; Tong, C.; Zhang, X.; Wang, L.; Peng, H.; Lan, P.; Zhang, P.; Huang, N.; et al. Positive regulatory effects of perioperative probiotic treatment on postoperative liver complications after colorectal liver metastases surgery: A double-center and double-blind randomized clinical trial. BMC Gastroenterol. 2015, 15, 34. [Google Scholar] [CrossRef] [Green Version]
- Mangell, P.; Thorlacius, H.; Syk, I.; Ahrne, S.; Molin, G.; Olsson, C.; Jeppsson, B. Lactobacillus plantarum 299v does not reduce enteric bacteria or bacterial translocation in patients undergoing colon resection. Dig. Dis. Sci. 2012, 57, 1915–1924. [Google Scholar] [CrossRef]
- McNaught, C.E.; Woodcock, N.P.; Macfie, J.; Mitchell, C.J. A prospective randomised study of the probiotic Lactobacillus plantarum 299V on indices of gut barrier function in elective surgical patients. Gut 2002, 51, 827–831. [Google Scholar] [CrossRef]
- Nomura, T.; Tsuchiya, Y.; Nashimoto, A.; Yabusaki, H.; Takii, Y.; Nakagawa, S.; Sato, N.; Kanbayashi, C.; Tanaka, O. Probiotics reduce infectious complications after pancreaticoduodenectomy. Hepato-Gastroenterology 2007, 54, 661–663. [Google Scholar] [PubMed]
- Okazaki, M.; Matsukuma, S.; Suto, R.; Miyazaki, K.; Hidaka, M.; Matsuo, M.; Noshima, S.; Zempo, N.; Asahara, T.; Nomoto, K. Perioperative synbiotic therapy in elderly patients undergoing gastroenterological surgery: A prospective, randomized control trial. Nutrition 2013, 29, 1224–1230. [Google Scholar] [CrossRef]
- Park, I.J.; Lee, J.H.; Kye, B.H.; Oh, H.K.; Cho, Y.B.; Kim, Y.T.; Kim, J.Y.; Sung, N.Y.; Kang, S.B.; Seo, J.M.; et al. Effects of PrObiotics on the Symptoms and Surgical ouTComes after Anterior REsection of Colon Cancer (POSTCARE): A Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Med. 2020, 9, 2181. [Google Scholar] [CrossRef] [PubMed]
- Polakowski, C.B.; Kato, M.; Preti, V.B.; Schieferdecker, M.E.M.; Ligocki Campos, A.C. Impact of the preoperative use of synbiotics in colorectal cancer patients: A prospective, randomized, double-blind, placebo-controlled study. Nutrition 2019, 58, 40–46. [Google Scholar] [CrossRef]
- Rayes, N.; Hansen, S.; Seehofer, D.; Ma¬ller, A.R.; Serke, S.; Bengmark, S.; Neuhaus, P. Early enteral supply of fiber and Lactobacilli versus conventional nutrition: A controlled trial in patients with major abdominal surgery. Nutrition 2002, 18, 609–615. [Google Scholar] [CrossRef]
- Rayes, N.; Seehofer, D.; Theruvath, T.; Mogl, M.; Langrehr, J.M.; Nassler, N.C.; Bengmark, S.; Neuhaus, P. Effect of enteral nutrition and synbiotics on bacterial infection rates after pylorus-preserving pancreatoduodenectomy: A randomized, double-blind trial. Ann. Surg. 2007, 246, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Rayes, N.; Pilarski, T.; Stockmann, M.; Bengmark, S.; Neuhaus, P.; Seehofer, D. Effect of pre- and probiotics on liver regeneration after resection: A randomised, double-blind pilot study. Benef. Microbes 2012, 3, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Reddy, B.S.; Macfie, J.; Gatt, M.; Larsen, C.N.; Jensen, S.S.; Leser, T.D. Randomized clinical trial of effect of synbiotics, neomycin and mechanical bowel preparation on intestinal barrier function in patients undergoing colectomy. Br. J. Surg. 2007, 94, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Sadahiro, S.; Suzuki, T.; Tanaka, A.; Okada, K.; Kamata, H.; Ozaki, T.; Koga, Y. Comparison between oral antibiotics and probiotics as bowel preparation for elective colon cancer surgery to prevent infection: Prospective randomized trial. Surgery 2014, 155, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Sommacal, H.M.; Bersch, V.P.; Vitola, S.P.; Osvaldt, A.B.; Sommacal, H.M.; Bersch, V.P.; Vitola, S.P.; Osvaldt, A.B. Perioperative synbiotics decrease postoperative complications in periampullary neoplasms: A randomized, double-blind clinical trial. Nutr. Cancer 2015, 67, 457–462. [Google Scholar] [CrossRef]
- Sugawara, G.; Nagino, M.; Nishio, H.; Ebata, T.; Takagi, K.; Asahara, T.; Nomoto, K.; Nimura, Y. Perioperative synbiotic treatment to prevent postoperative infectious complications in biliary cancer surgery: A randomized controlled trial. Ann. Surg. 2006, 244, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.K.; Said, S.; Tan, C.K.; Said, S.; Rajandram, R.; Wang, Z.; Roslani, A.C.; Chin, K.F. Pre-surgical Administration of Microbial Cell Preparation in Colorectal Cancer Patients: A Randomized Controlled Trial. World J. Surg. 2016, 40, 1985–1992. [Google Scholar] [CrossRef]
- Usami, M.; Miyoshi, M.; Kanbara, Y.; Aoyama, M.; Sakaki, H.; Shuno, K.; Hirata, K.; Takahashi, M.; Ueno, K.; Tabata, S.; et al. Effects of perioperative synbiotic treatment on infectious complications, intestinal integrity, and fecal flora and organic acids in hepatic surgery with or without cirrhosis. JPEN J. Parenter. Enteral Nutr. 2011, 35, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Xu, P.; Cen, Y.; Li, W. Effects of preoperative oral administration of glucose solution combined with postoperative probiotics on inflammation and intestinal barrier function in patients after colorectal cancer surgery. Oncol. Lett. 2019, 18, 694–698. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Xia, Y.; Chen, H.; Hong, L.; Feng, J.; Yang, J.; Yang, Z.; Shi, C.; Wu, W.; Gao, R.; et al. The effect of perioperative probiotics treatment for colorectal cancer: Short-term outcomes of a randomized controlled trial. Oncotarget 2016, 7, 8432–8440. [Google Scholar] [CrossRef] [Green Version]
- Yokoyama, Y.; Nishigaki, E.; Abe, T.; Fukaya, M.; Asahara, T.; Nomoto, K.; Nagino, M. Randomized clinical trial of the effect of perioperative synbiotics versus no synbiotics on bacterial translocation after oesophagectomy. Br. J. Surg. 2014, 101, 189–199. [Google Scholar] [CrossRef]
- Yokoyama, Y.; Miyake, T.; Kokuryo, T.; Asahara, T.; Nomoto, K.; Nagino, M. Effect of Perioperative Synbiotic Treatment on Bacterial Translocation and Postoperative Infectious Complications after Pancreatoduodenectomy. Dig. Surg. 2016, 33, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.W.; Du, P.; Gao, J.; Yang, B.R.; Fang, W.J.; Ying, C.M. Preoperative probiotics decrease postoperative infectious complications of colorectal cancer. Am. J. Med. Sci. 2012, 343, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Wang, Y.; Huang, Y.; Cui, Y.; Xia, L.; Rao, Z.; Zhou, Y.; Wu, X. Effects of fiber and probiotics on diarrhea associated with enteral nutrition in gastric cancer patients: A prospective randomized and controlled trial. Medicine 2017, 96, e8418. [Google Scholar] [CrossRef]
- Zheng, C.; Chen, T.; Wang, Y.; Gao, Y.; Kong, Y.; Liu, Z.; Deng, X. A randomised trial of probiotics to reduce severity of physiological and microbial disorders induced by partial gastrectomy for patients with gastric cancer. J. Cancer 2019, 10, 568–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aisu, N.; Tanimura, S.; Yamashita, Y.; Yamashita, K.; Maki, K.; Yoshida, Y.; Sasaki, T.; Takeno, S.; Hoshino, S. Impact of perioperative probiotic treatment for surgical site infections in patients with colorectal cancer. Exp. Ther. Med. 2015, 10, 966–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, Y.; Gao, Z.; Sun, Z.; Zhang, Q.; Zhou, B.; Li, Z.; Zhang, W.; Jiang, Y.; Zhang, X.; Ge, G.; et al. Enhanced recovery program in liver resection surgery: A single center experience. Transl. Cancer Res. 2018, 7, 1112–1121. [Google Scholar] [CrossRef]
- Fujio, A.; Miyagi, S.; Tokodai, K.; Nakanishi, W.; Nishimura, R.; Mitsui, K.; Unno, M.; Kamei, T. Effects of a new perioperative enhanced recovery after surgery protocol in hepatectomy for hepatocellular carcinoma. Surg. Today 2020, 50, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.; Zhang, S.Z.; Du, P.; Cheng, Z.B.; Hu, H.; Wang, S.Y. Probiotics Can Boost the Antitumor Immunity of CD8(+)T Cells in BALB/c Mice and Patients with Colorectal Carcinoma. J. Immunol. Res. 2020, 2020, 4092472. [Google Scholar] [CrossRef]
- Mizuta, M.; Endo, I.; Yamamoto, S.; Inokawa, H.; Kubo, M.; Udaka, T.; Sogabe, O.; Maeda, H.; Shirakawa, K.; Okazaki, E.; et al. Perioperative supplementation with bifidobacteria improves postoperative nutritional recovery, inflammatory response, and fecal microbiota in patients undergoing colorectal surgery: A prospective, randomized clinical trial. Biosci. Microbiota Food Health 2016, 35, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rifatbegovic, Z.; Mesic, D.; Ljuca, F.; Zildzic, M.; Avdagic, M.; Grbic, K.; Agic, M.; Hadziefendic, B. Effect of probiotics on liver function after surgery resection for malignancy in the liver cirrhotic. Med. Arch. 2010, 64, 208–211. [Google Scholar]
- Amitay, E.L.; Carr, P.R.; Gies, A.; Laetsch, D.C.; Brenner, H. Probiotic/Synbiotic Treatment and Postoperative Complications in Colorectal Cancer Patients: Systematic Review and Meta-analysis of Randomized Controlled Trials. Clin. Transl. Gastroenterol. 2020, 11, e00268. [Google Scholar] [CrossRef]
- Ouyang, X.; Li, Q.; Shi, M.; Niu, D.; Song, W.; Nian, Q.; Li, X.; Ding, Z.; Ai, X.; Wang, J. Probiotics for preventing postoperative infection in colorectal cancer patients: A systematic review and meta-analysis. Int. J. Colorectal Dis. 2019, 34, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.D.; Liu, M.M.; Liang, X.; Hu, N.; Huang, W. Effects of perioperative supplementation with pro-/synbiotics on clinical outcomes in surgical patients: A meta-analysis with trial sequential analysis of randomized controlled trials. Clin. Nutr. 2018, 37, 505–515. [Google Scholar] [CrossRef]
- Zeng, J.; Ji, Y.; Liang, B.; Zhang, G.; Chen, D.; Zhu, M.; Wu, S.; Kuang, W. The effect of pro/synbiotics on postoperative infections in colorectal cancer patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2021, 43, 101370. [Google Scholar] [CrossRef] [PubMed]
- Kasatpibal, N.; Whitney, J.D.; Saokaew, S.; Kengkla, K.; Heitkemper, M.M.; Apisarnthanarak, A. Effectiveness of Probiotic, Prebiotic, and Synbiotic Therapies in Reducing Postoperative Complications: A Systematic Review and Network Meta-analysis. Clin. Infect. Dis. 2017, 64, S153–S160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skonieczna-Żydecka, K.; Kaczmarczyk, M.; Łoniewski, I.; Lara, L.F.; Koulaouzidis, A.; Misera, A.; Maciejewska, D.; Marlicz, W. A Systematic Review, Meta-Analysis, and Meta-Regression Evaluating the Efficacy and Mechanisms of Action of Probiotics and Synbiotics in the Prevention of Surgical Site Infections and Surgery-Related Complications. J. Clin. Med. 2018, 7, 556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhury, A.H.; Adiamah, A.; Kushairi, A.; Varadhan, K.K.; Krznaric, Z.; Kulkarni, A.D.; Neal, K.R.; Lobo, D.N. Perioperative Probiotics or Synbiotics in Adults Undergoing Elective Abdominal Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Ann. Surg. 2020, 271, 1036–1047. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Wu, Q.; Liu, Y.; Fan, D. Effect of Perioperative Probiotics and Synbiotics on Postoperative Infections after Gastrointestinal Surgery: A Systematic Review with Meta-Analysis. JPEN J. Parenter. Enteral Nutr. 2017, 41, 1051–1062. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Year. | Interventions and Comparators with Dosages | Freq. of Dose | Route of Admin. | Tx Duration Pre-op (Days) | Tx Duration Post-op (Days) | Tx Duration TOTAL (Days) |
|---|---|---|---|---|---|---|
| Anderson 2004 [33] | Lactobacillus acidophilus La5 + L. bulgaricus + Bifidobacterium lactis Bb-12 + Streptococcus thermophilus (4 billion CFU) capsule + oligofructose (11 g) powder a | TID | oral | 12 | 4 | 16 |
| Placebo capsule + sucrose placebo powder | TID | oral | 12 | 4 | 16 | |
| Aso 1992 [34] | Lactobacillus casei (10 billion viable cells) | TID | oral | NA | 365 | 365 |
| Standard care alone | NA | NA | ||||
| Cho 2019 [35] | Lactobacillus plantarum CJLP243 (10 billion) | QD | oral | 1 | 21 | 22 |
| Maltodextrin + glucose placebo (2 g) | QD | oral | 1 | 21 | 22 | |
| Consoli 2016 [36] | Saccharomyces boulardii (50 million CFU) | QD | oral | 9 | NA | 9 |
| Standard care alone | NA | NA | ||||
| Diepenhorst 2011 [37] | Bifidobacterium bifidum + B. infantis + Lactobacillus acidophilus + L. casei + L. salivarius + L. lactis (10 billion) | BID | oral | 7 | 7 | 14 |
| Standard tx control b [neither probiotics nor SDD] | NR | NA | NR | NR | NR | |
| Selective decontamination of the digestive tract (SDD antibiotics regimen) | 4 times daily | Multiple | 4 | 2 | 6 | |
| Flesch 2017 [38] | Lactobacillus acidophilus NCFM + L. rhamnosus HN001 + L. paracasei LPC-37 + Bifidobacterium lactis HN019 (1 billion CFU each) + fructooligosaccharides a (6 g) | BID | oral | 5 | 14 | 19 |
| Maltodextrin placebo (6 g) | BID | oral | 5 | 14 | 19 | |
| Franko 2019 [39] | Bifidobacterium breve + B. longum + B. infantis + Lactobacillus acidophilus + L. plantarum + L. paracasei + L. bulgaricus + Streptococcus thermophilus (112.5 billion CFU/capsule) | BID | oral | 1 | 6 | 7 |
| Placebo | BID | oral | 1 | 6 | 7 | |
| Horvat 2010 [40] | Pediacoccus pentosaceus 5–33:3 + Leuconostoc mesenteroides 32–77:1 + Lactobacillus paracasei subsp. paracasei 19 + L. plantarum 2362 (10 billion each) + betaglucan + inulin + pectin + resistant starch fibers a (2.5 g each) [without mechanical bowel preparation] | BID | oral | 3 | NA | 3 |
| Mechanical bowel preparation control b | QD | oral | 1 | NA | 1 | |
| Heat-inactivated lactobacilli + betaglucan + inulin + pectin + resistant starch fibers (2.5 g each) [without mechanical bowel preparation] | BID | oral | 3 | NA | 3 | |
| Kanazawa 2005 [41] | Lactobacillus casei strain Shirota (300 million) + Bifidobacterium breve strain Yakult (300 million) + galactooligosaccharides a (12 g) + EN + PN | QD | enteral | NA | 14 | 14 |
| Standard EN + PN | QD | NA | NA | 14 | 14 | |
| Komatsu 2016 [42] | Lactobacillus casei strain Shirota (40 billion) + Bifidobacterium breve strain Yakult (10 billion) + galactooligosaccharides a (2.5 g) | QD | oral | 7–11 | Yes | Total NR |
| Standard care alone | NA | NA | ||||
| Kotzampassi 2015 [43] | Lactobacillus acidophilus LA-5 (1.75 billion CFU) + L. plantarum (0.5 billion CFU) + Bifidobacterium lactis BB-12 (1.75 billion CFU) + Saccharomyces boulardii (1.5 billion CFU) | BID | oral | 1 | 15 | 16 |
| Glucose polymer placebo | BID | oral | 1 | 15 | 16 | |
| Krebs 2016 [45] | Pediacoccus pentosaceus 5–33:3 + Leuconostoc mesenteroides 32–77:1 + Lactobacillus paracasei subsp. paracasei 19 + L. plantarum 2362 (100 billion each) + betaglucan + inulin + pectin + resistant starch fibers a (2.5 g each) [without mechanical bowel preparation] | BID | oral | 3 | NA | 3 |
| Mechanical bowel preparation control | QD | oral | 1 | NA | 1 | |
| Betaglucan + inulin + pectin + resistant starch fibers (2.5 g each) [without mechanical bowel preparation] | BID | oral | 3 | NA | 3 | |
| Lages 2018 [46] | Lactobacillus paracasei LPC-31 + L. rhamnosus HN00l + L. acidophilus NCFM + Bifidobacterium lactis HN019 (1 billion CFU/mL each) + fructooligosaccharides a (6 g) diluted in 20 mL of water + standard EN | BID | enteral | NA | 5–7 | 5–7 |
| Maltodextrin placebo (6 g) + standard EN | BID | enteral | NA | 5–7 | 5–7 | |
| Liu 2015 [49] | Lactobacillus plantarum CGMCC No. 1258 (200 billion CFU) + L. acidophilus LA-11 (140 billion CFU) + Bifidobacterium longum BL-88 (100 billion CFU) | QD | oral | 6 | 10 | 16 |
| Maltodextrin placebo | QD | oral | 6 | 10 | 16 | |
| Mangell 2012 [50] | Lactobacillus plantarum 299v (100 billion CFU) in an oatmeal-based drink a (100 mL) | QD | oral | 8 | 5 | 13 |
| Oatmeal-based placebo drink without probiotics (100 mL) | QD | oral | 8 | 5 | 13 | |
| McNaught 2002 [51] | Lactobacillus plantarum 299v (25 billion CFU/day) in an oatmeal-based drink a | NR | oral | IQR: 7–12 | IQR: 4–9 | med.: 14 |
| Standard care alone | NA | NA | ||||
| Nomura 2007 [52] | Enterococcus fecalis T-110 (12 mg/day) + Clostridium butyricum TO-A (60 mg/day) + Bacillus mesentericus TO-A (60 mg/day) | NR | oral | 3–15 | 9–38 | 12–53 |
| Standard care alone | NA | NA | ||||
| Okazaki 2013 [53] | Lactobacillus casei strain Shirota (1 g) + Bifidobacterium breve strain Yakult (1 g) + galactooligosaccharides a (15 g) | QD | oral | 7 | 10 | 17 |
| Standard care alone | NA | NA | ||||
| Park 2020 [54] | Bifidobacterium animalis subsp. lactis HY8002 (100 million CFU) + Lactobacillus casei HY2782 (50 million CFU) + L. plantarum HY7712 (50 million CFU) + xylooligosaccharides (350 mg) + fructooligosaccharides (36 mg) | BID | oral | 7 | 21 | 28 |
| Xylooligosaccharides (350 mg) + fructooligosaccharides (36 mg) | BID | oral | 7 | 21 | 28 | |
| Polakowski 2019 [55] | Lactobacillus acidophilus NCFM + L. rhamnosus HN001 + L. paracasei LPC-37 + Bifidobacterium lactis HN019 (1 billion each) + fructooligosaccharides a (6 g) c | BID | oral | 7 | NA | 7 |
| Maltodextrin placebo | BID | oral | 7 | NA | 7 | |
| Rayes 2002 [56] | Live Lactobacillus plantarum 299 (1 billion) + oat fibe r a (11.3 g/L) + EN | BID | enteral | NA | 4–5 | 4–5 |
| Standard total parenteral nutrition or fiber-free EN control b | QD | IV | NA | 8 | 8 | |
| Heat-killed Lactobacillus plantarum 299 + oat fiber (11.3 g/L) + EN | QD | enteral | NA | 4–5 | 4–5 | |
| Rayes 2007 [57] | Pediacoccus pentosaceus 5–33:3 + Leuconostoc mesenteroides 32–77:1 + Lactobacillus paracasei subsp. paracasei 19 + L. plantarum 2362 (10 billion) + betaglucan + inulin + pectin + resistant starch fibers a (2.5 g each) + EN | BID | enteral | 1 | 8 | 9 |
| Betaglucan + inulin + pectin + resistant starch fibers (2.5 g each) + EN | BID | enteral | 1 | 8 | 9 | |
| Rayes 2012 [58] | Pediacoccus pentosaceus 5–33:3 + Leuconostoc mesenteroides 32–77:1 + Lactobacillus paracasei subsp. paracasei 19 + L. plantarum 2362 (10 billion) + betaglucan + inulin + pectin + resistant starch fibers a (2.5 g each) + EN | BID | enteral | 1 | 10 | 11 |
| Betaglucan + inulin + pectin + resistant starch fibers (2.5 g each) + EN | BID | enteral | 1 | 10 | 11 | |
| Reddy 2007 [59] | Lactobacillus acidophilus La5 + L. bulgaricus + Bifidobacterium lactis Bb-12 + Streptococcus thermophilus (4 billion CFU) + oligofructose a (10 g) + neomycin (3 g) + mechanical bowel preparation | TID | oral | NR | NA | NR |
| Neomycin (3 g) + mechanical bowel preparation control b | TID | oral | NR | NA | NR | |
| Lactobacillus acidophilus La5 + L. bulgaricus + Bifidobacterium lactis Bb-12 + Streptococcus thermophilus (4 billion CFU) + oligofructose (10 g) + neomycin (3 g) [without mechanical bowel preparation] | TID | oral | NR | NA | NR | |
| Mechanical bowel preparation only | QD | oral | 1 | NA | 1 | |
| Sadahiro 2014 [60] | Bifidobacterium bifidum (3.3 billion) + maltooligosaccharide [plus single IV dose of flomoxef; & standard mechanical bowel preparation] | TID | oral | 7 | 10 | 17 |
| Standard care alone control b [plus single IV dose of flomoxef; & standard mechanical bowel preparation. No probiotic or oral antibiotics] | NA | NA | ||||
| Kanamycin sulfate + metronidazole (500 mg each) [plus single IV dose of flomoxef; & standard mechanical bowel preparation] | TID | oral | 1 | NA | 1 | |
| Sommacal 2015 [61] | Lactobacillus acidophilus 10 + L. rhamnosus HS 111 + L. casei 10 + Bifidobacterium bifidum (1 billion CFU each) + fructooligosaccharides (100 mg) d | BID | oral | 4 | 10 | 14 |
| Sucrose placebo | BID | oral | 4 | 10 | 14 | |
| Sugawara 2006 [62] | Pre-op: Oral Lactobacillus casei strain Shirota (40 billion) + Bifidobacterium breve strain Yakult (10 billion) + galactooligosaccharides a (15 g). Post-op: Lactobacillus casei strain Shirota (300 million) + Bifidobacterium breve strain Yakult (300 million) + galactooligosaccharides a (15 g) + standard EN + PN. | QD | oral & enteral | 14 | 14 | 28 |
| Pre-op: Standard care alone. Post-op: Lactobacillus casei strain Shirota (300 million) + Bifidobacterium breve strain Yakult (300 million) + galactooligosaccharides a (15 g) + standard EN + PN. | QD | enteral | NA | 14 | 14 | |
| Tan 2016 [63] | Lactobacillus acidophilus BCMC12130 + L. casei BCMC12313 + L. lactis BCMC12451 + Bifidobacterium bifidum BCMC02290 + B. longum BCMC02120 + B. infantis BCMC02129 (30 billion CFU) | BID | oral | 7 | NA | 7 |
| Placebo (3 g) | BID | oral | 7 | NA | 7 | |
| Usami 2011 [64] | Lactobacillus casei strain Shirota (300 million) + Bifidobacterium breve strain Yakult (300 million) + galactooligosaccharides a (10 g) [+ PN for 4 days post-op] | QD | oral | 14 | 12 | 26 |
| Standard care alone [+ PN for 4 days post-op] | NA | NA | ||||
| Xu 2019 [65] | Bifidus-triple viable preparation e + glucose solution | QD | oral | 7 | NA | 7 |
| Glucose solution | QD | oral | 7 | NA | 7 | |
| Yang 2016 [66] | Bifidobacterium longum + Lactobacillus acidophilus + Enterococcus faecalis a (20 million CFU each) | TID | oral | 5 | 7 | 12 |
| Maltodextrin + sucrose placebo (2 g) | TID | oral | 5 | 7 | 12 | |
| Yokoyama 2014 [67] | Pre-op: Oral or enteral Lactobacillus casei strain Shirota (40 billion) + Bifidobacterium breve strain Yakult (10 billion) + galactooligosaccharides a (15 g). Post-op: Enteral Lactobacillus casei strain Shirota (300 million) + Bifidobacterium breve strain Yakult (300 million) + galactooligosaccharides (15 g) + EN. | QD | oral & enteral | 7 | 14 | 21 |
| Pre-op: standard care alone (ordinary diet). Post-op: standard EN. | QD | enteral | 7 | 14 | 21 | |
| Yokoyama 2016 [68] | Pre-op: Oral Lactobacillus casei strain Shirota (40 billion) + Bifidobacterium breve strain Yakult (10 billion) + galactooligosaccharides a (15 g). Post-op: Enteral Lactobacillus casei strain Shirota (300 million) + Bifidobacterium breve strain Yakult (300 million) + galactooligosaccharides (15 g) + EN. | QD | oral & enteral | 7 | 14 | 21 |
| Pre-op: Standard care alone. Post-op: Enteral Lactobacillus casei strain Shirota (300 million) + Bifidobacterium breve strain Yakult (300 million) + galactooligosaccharides (15 g) + EN. | QD | enteral | NA | 14 | 14 | |
| Zhang 2012 [69] | Bifidobacterium longum + Lactobacillus acidophilus + Enterococcus faecalis a (63 million CFU) | TID | oral | 3 | NA | 3 |
| Maltodextrin placebo | TID | oral | 3 | NA | 3 | |
| Zhao 2017 [70] | Bifidobacterium + Lactobacillus (6 g) + fiber f (30 g) + EN | QD | enteral | NA | 7 | 7 |
| Fiber-free EN control b | QD | enteral | NA | 7 | 7 | |
| Fiber-enriched EN (with 30 g of Shen JiaTM fiber) | QD | enteral | NA | 7 | 7 | |
| Zheng 2019 [71] | Bifidobacterium infantis (3 million CFU) + Lactobacillus acidophilus (3 million CFU) + Enterococcus faecalis (3 million CFU) + Bacillus cereus (300,000 CFU) | TID | oral | NA | 6–7 | 6–7 |
| Placebo | TID | oral | NA | 6–7 | 6–7 |
| Author Year | Sample Size | Country | Study Period | Cancer Types | Funding | Female (%) | Age Mean (Years) | Age Variance |
|---|---|---|---|---|---|---|---|---|
| Anderson 2004 [33] | 137 | UK | NR | Colon (majority) & other GI cancers | NR | 48 | 69 | NR |
| Aso 1992 [34] | 48 | Japan | 1988–1990 | Bladder cancer | NR | 13 | NR | NR |
| Cho 2019 [35] | 36 | South Korea | 2016–2017 | Rectal cancer | public | NR | NR | NR |
| Consoli 2016 [36] | 68 | Brazil | 2010–2013 | Colon cancer | public | 55 | 55 | Range 17–83 |
| Diepenhorst 2011 [37] | 30 | The Netherlands | 2005–2006 | Periampullary & ampullary pancreatic cancers | NR | 50 | 61 | NR |
| Flesch 2017 [38] | 91 | Brazil | 2013–2015 | Colorectal cancer | none | 59 | 63 | NR |
| Franko 2019 [39] | 135 | USA | 2015–2017 | Colorectal (70%), hepato-biliary & pancreatic cancers | public | 51 | 62.5 | SD 12.1 |
| Horvat 2010 [40] | 76 | Slovenia | NR | Colorectal cancer | unclear | 59 | 63 | Range 29–86 |
| Kanazawa 2005 [41] | 54 | Japan | 2000–2002 | Biliary cancers | NR | 34 | 64 | NR |
| Komatsu 2016 [42] | 379 | Japan | 2008–2014 | Colorectal cancer | private | 42 | 68 | NR |
| Kotzampassi 2015 [43] | 168 | Greece | 2013–2014 | Colorectal cancer | unclear | 30 | 66 | NR |
| Krebs 2016 [45] | 60 | Slovenia | 2009–2012 | Colorectal cancer | NR | 39 | 65 | Range 43–87 |
| Lages 2018 [46] | 40 | Brazil | 2014–2016 | Head & neck cancers | public | 19 | 60.5 | NR |
| Liu 2015 [49] | 161 | China | 2007–2013 | Colorectal cancer | public | 48 | 63 | NR |
| Mangell 2012 [50] | 72 | Sweden | NR | Colon cancer | public | 44 | 72 | NR |
| McNaught 2002 [51] | 129 | UK | NR | Colorectal (51%) & other GI cancers | NR | 42 | 69 | NR |
| Nomura 2007 [52] | 70 | Japan | 2004–2006 | Pancreatic biliary cancers | NR | 39 | 68 | Range 30–88 |
| Okazaki 2013 [53] | 48 | Japan | 2009–2011 | GI (88%) & hepatobiliary pancreatic cancers | NR | 46 | 79 | Range 70–92 |
| Park 2020 [54] | 68 | South Korea | 2016–2018 | Sigmoid colon cancer | private | 47 | 61 | NR |
| Polakowski 2019 [55] | 73 | Brazil | NR | Colorectal cancer | NR | 47 | 60 | NR |
| Rayes 2002 [56] | 90 | Germany | 1997–1999 | Hepatic (32%), pancreatic (29%), gastric (24%) & colon cancers | NR | 47 | 61 | NR |
| Rayes 2007 [57] | 89 | Germany | NR | Pancreatic cancer | NR | 44 | 58.5 | NR |
| Rayes 2012 [58] | 19 | Germany | 2007–2008 | Colorectal metastasis (53%), cholangiocellular carcinoma (42%) & liver cancers | NR | 26 | 60 | NR |
| Reddy 2007 [59] | 92 | UK | NR | Colorectal cancer | private | 50 | 69 | NR |
| Sadahiro 2014 [60] | 310 | Japan | 2008–2011 | Colon cancer | private | 47 | 67 | NR |
| Sommacal 2015 [61] | 48 | Brazil | 2010–2012 | Periampullary cancers | public | NR | 59 | Range 44–85 |
| Sugawara 2006 [62] | 101 | Japan | 2003–2005 | Biliary cancers | NR | 43 | 63 | NR |
| Tan 2016 [63] | 40 | Malaysia | 2012–2013 | Colorectal cancer | private | 40 | 66 | NR |
| Usami 2011 [64] | 67 | Japan | 2005–2008 | Hepatic cancer | mixed public & private | 10 | 65 | NR |
| Xu 2019 [65] | 60 | China | 2017–2018 | Colorectal cancer | none | 37 | NR | NR |
| Yang 2016 [66] | 79 | China | 2011–2012 | Colorectal cancer | public | 55 | 63 | NR |
| Yokoyama 2014 [67] | 42 | Japan | 2008–2011 | Esophageal cancer | private | 12 | 65.5 | Range 25–77 |
| Yokoyama 2016 [68] | 45 | Japan | 2010–2012 | Pancreatic & biliary cancers | private | 73 | 65 | Range 41–83 |
| Zhang 2012 [69] | 60 | China | 2006–2007 | Colorectal cancer | public | 60 | 65 | Range 45–87 |
| Zhao 2017 [70] | 120 | China | 2015–2016 | Gastric cancer | public | 48 | 66 | NR |
| Zheng 2019 [71] | 100 | China | 2017–2018 | Gastric cancer | public | 16 | 62 | NR |
| Author Year | Selection | Comparability | Outcome |
|---|---|---|---|
| Aisu 2015 [72] | ★★★ | ★★ | |
| Ding 2018 [73] | ★★★★ | ★★★ | |
| Fujio 2020 [74] | ★★★★ | ★★ | |
| Mao 2020 [75] | ★★★★ | ★★ | |
| Mizuta 2016 [76] | ★★★★ | ★ | ★★★ |
| Rifatbegovic 2010 [77] | ★★★★ | ★★ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cogo, E.; Elsayed, M.; Liang, V.; Cooley, K.; Guerin, C.; Psihogios, A.; Papadogianis, P. Probiotics Evaluation in Oncological Surgery: A Systematic Review of 36 Randomized Controlled Trials Assessing 21 Diverse Formulations. Curr. Oncol. 2021, 28, 5192-5214. https://doi.org/10.3390/curroncol28060435
Cogo E, Elsayed M, Liang V, Cooley K, Guerin C, Psihogios A, Papadogianis P. Probiotics Evaluation in Oncological Surgery: A Systematic Review of 36 Randomized Controlled Trials Assessing 21 Diverse Formulations. Current Oncology. 2021; 28(6):5192-5214. https://doi.org/10.3390/curroncol28060435
Chicago/Turabian StyleCogo, Elise, Mohamed Elsayed, Vivian Liang, Kieran Cooley, Christilynn Guerin, Athanasios Psihogios, and Peter Papadogianis. 2021. "Probiotics Evaluation in Oncological Surgery: A Systematic Review of 36 Randomized Controlled Trials Assessing 21 Diverse Formulations" Current Oncology 28, no. 6: 5192-5214. https://doi.org/10.3390/curroncol28060435
APA StyleCogo, E., Elsayed, M., Liang, V., Cooley, K., Guerin, C., Psihogios, A., & Papadogianis, P. (2021). Probiotics Evaluation in Oncological Surgery: A Systematic Review of 36 Randomized Controlled Trials Assessing 21 Diverse Formulations. Current Oncology, 28(6), 5192-5214. https://doi.org/10.3390/curroncol28060435