Could the Long-Term Oncological Safety of Laparoscopic Surgery in Low-Risk Endometrial Cancer also Be Valid for the High–Intermediate- and High-Risk Patients? A Multi-Center Turkish Gynecologic Oncology Group Study Conducted with 2745 Endometrial Cancer Cases. (TRSGO-End-001)

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
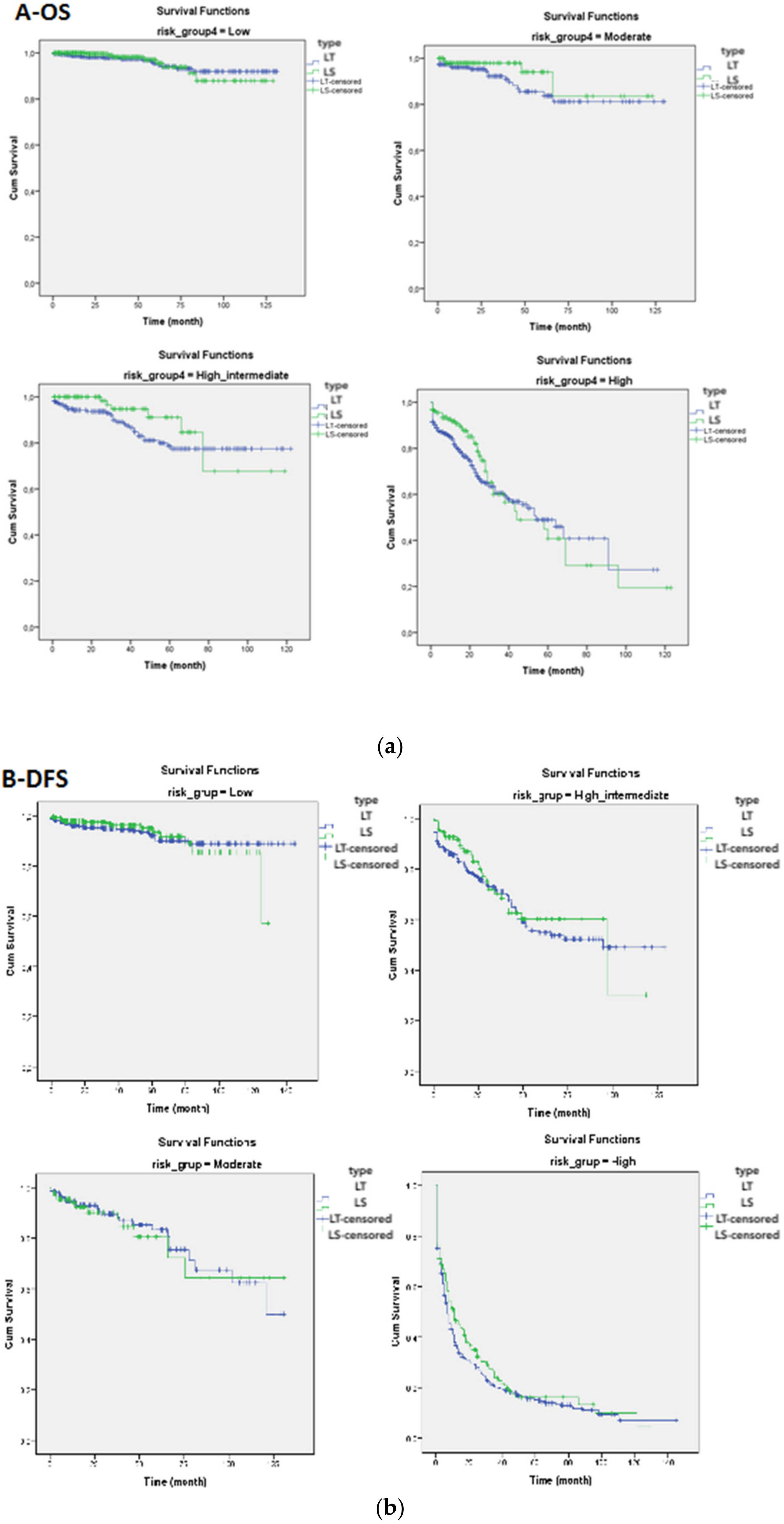
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amant, F.; Moerman, P.; Neven, P.; Timmerman, D.; Van Limbergen, E.; Vergote, I. Endometrial cancer. Lancet 2005, 366, 491–505. [Google Scholar] [CrossRef]
- Zullo, F.; Falbo, A.; Palomba, S. Safety of laparoscopy vs laparotomy in the surgical staging of endometrial cancer: A systematic review and metaanalysis of randomized controlled trials. Am. J. Obs. Gynecol. 2012, 207, 94–100. [Google Scholar] [CrossRef]
- Palomba, S.; Falbo, A.; Mocciaro, R.; Russo, T.; Zullo, F. Laparoscopic treatment for endometrial cancer: A meta-analysis of randomized controlled trials (RCTs). Gynecol. Oncol. 2009, 112, 415–421. [Google Scholar] [CrossRef]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; Gonzalez-Martin, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, Treatment and Follow-up. Int. J. Gynecol. Cancer 2016, 26, 2–30. [Google Scholar] [CrossRef] [PubMed]
- Dargent, D. A new future for Schauta’s operation through presurgical retroperitoneal. pelviscopy. Eur. J. Gynaecol. Oncol. 1987, 8, 292–296. [Google Scholar]
- Querleu, D.; Leblanc, E.; Castelain, B. Laparoscopic pelvic lymphadenectomy in the staging of early carcinoma of the cervix. Am. J. Obs. Gynecol. 1991, 164, 579–581. [Google Scholar] [CrossRef]
- Childers, J.M.; Hatch, K.D.; Tran, A.N.; Surwit, E.A. Laparoscopic para-aortic lymphadenectomy in gynecologic malignancies. Obstet. Gynecol. 1993, 82, 741–747. [Google Scholar] [CrossRef]
- Spirtos, N.M.; Schlaerth, J.B.; Spirtos, T.W.; Schlaerth, A.C.; Indman, P.D.; Kimball, R.E. Laparoscopic bilateral pelvic and paraaortic lymph node sampling: An evolving technique. Am. J. Obs. Gynecol. 1995, 173, 105–111. [Google Scholar] [CrossRef]
- Lee, C.L.; Kusunoki, S.; Huang, K.G.; Wu, K.Y.; Huang, C.Y.; Yen, C.F. Long-term survival outcomes of laparoscopic staging surgery in treating endometrial cancer: 20 Years of follow-up. Taiwan J. Obs. Gynecol. 2016, 55, 545–551. [Google Scholar] [CrossRef][Green Version]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.; Ribeiro, R.; Buda, A.; Yan, X.; Shuzhong, Y.; Chetty, N.; et al. Minimally Invasive versus Abdominal Radical Hysterectomy for Cervical Cancer. N. Engl. J. Med. 2018, 379, 1895–1904. [Google Scholar] [CrossRef]
- Walker, J.L.; Piedmonte, M.R.; Spirtos, N.M.; Eisenkop, S.M.; Schlaerth, J.B.; Mannel, R.S.; Spiegel, G.; Barakat, R.; Pearl, M.L.; Sharma, S.K. Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2. J. Clin. Oncol. 2009, 27, 5331–5336. [Google Scholar] [CrossRef]
- Janda, M.; Gebski, V.; Forder, P.; Jackson, D.; Williams, G.; Obermair, A.; Committee, L.T. Total laparoscopic versus open surgery for stage 1 endometrial cancer: The LACE randomized controlled trial. Contemp. Clin. Trials 2006, 27, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Piedmonte, M.R.; Spirtos, N.M.; Eisenkop, S.M.; Schlaerth, J.B.; Mannel, R.S.; Barakat, R.; Pearl, M.L.; Sharma, S.K. Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group LAP2 Study. J. Clin. Oncol. 2012, 30, 695–700. [Google Scholar] [CrossRef]
- Malzoni, M.; Tinelli, R.; Cosentino, F.; Perone, C.; Rasile, M.; Iuzzolino, D.; Malzoni, C.; Reich, H. Total laparoscopic hysterectomy versus abdominal hysterectomy with lymphadenectomy for early-stage endometrial cancer: A prospective randomized study. Gynecol. Oncol. 2009, 112, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Galaal, K.; Donkers, H.; Bryant, A.; Lopes, A.D. Laparoscopy versus laparotomy for the management of early stage endometrial cancer. Cochrane Database Syst. Rev. 2018, 10, CD006655. [Google Scholar] [CrossRef]
- Janda, M.; Gebski, V.; Davies, L.C.; Forder, P.; Brand, A.; Hogg, R.; Jobling, T.W.; Land, R.; Manolitsas, T.; Nascimento, M.; et al. Effect of Total Laparoscopic Hysterectomy vs Total Abdominal Hysterectomy on Disease-Free Survival Among Women With Stage I Endometrial Cancer: A Randomized Clinical Trial. JAMA 2017, 317, 1224–1233. [Google Scholar] [CrossRef] [PubMed]
- Deura, I.; Shimada, M.; Azuma, Y.; Komatsu, H.; Nagira, K.; Sawada, M.; Harada, T. Comparison of laparoscopic surgery and conventional laparotomy for surgical staging of patients with presumed low-risk endometrial cancer: The current state of Japan. Taiwan J. Obstet. Gynecol. 2019, 58, 99–104. [Google Scholar] [CrossRef]
- Fader, A.N.; Seamon, L.G.; Escobar, P.F.; Frasure, H.E.; Havrilesky, L.A.; Zanotti, K.M.; Secord, A.A.; Boggess, J.F.; Cohn, D.E.; Fowler, J.M.; et al. Minimally invasive surgery versus laparotomy in women with high grade endometrial cancer: A multi-site study performed at high volume cancer centers. Gynecol. Oncol. 2012, 126, 180–185. [Google Scholar] [CrossRef]
- Koskas, M.; Jozwiak, M.; Fournier, M.; Vergote, I.; Trum, H.; Lok, C.; Amant, F. Long-term oncological safety of minimally invasive surgery in high-risk endometrial cancer. Eur. J. Cancer 2016, 65, 185–191. [Google Scholar] [CrossRef]
- Favero, G.; Anton, C.; Le, X.; Silva, E.S.A.; Dogan, N.U.; Pfiffer, T.; Kohler, C.; Baracat, E.C.; Carvalho, J.P. Oncologic Safety of Laparoscopy in the Surgical Treatment of Type II Endometrial Cancer. Int. J. Gynecol. Cancer 2016, 26, 1673–1678. [Google Scholar] [CrossRef] [PubMed]
- Monterossi, G.; Ghezzi, F.; Vizza, E.; Zannoni, G.F.; Uccella, S.; Corrado, G.; Restaino, S.; Quagliozzi, L.; Casarin, J.; Dinoi, G.; et al. Minimally Invasive Approach in Type II Endometrial Cancer: Is It Wise and Safe? J. Minim. Invasive Gynecol. 2017, 24, 438–445. [Google Scholar] [CrossRef]
- Scaletta, G.; Dinoi, G.; Capozzi, V.; Cianci, S.; Pelligra, S.; Ergasti, R.; Fagotti, A.; Scambia, G.; Fanfani, F. Comparison of minimally invasive surgery with laparotomic approach in the treatment of high risk endometrial cancer: A systematic review. Eur. J. Surg. Oncol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Mariani, A.; Dowdy, S.C.; Cliby, W.A.; Gostout, B.S.; Jones, M.B.; Wilson, T.O.; Podratz, K.C. Prospective assessment of lymphatic dissemination in endometrial cancer: A paradigm shift in surgical staging. Gynecol. Oncol. 2008, 109, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Nieto, V.L.; Huang, Y.; Hou, J.Y.; Tergas, A.I.; St Clair, C.M.; Ananth, C.V.; Neugut, A.I.; Hershman, D.L.; Wright, J.D. Use and outcomes of minimally invasive hysterectomy for women with nonendometrioid endometrial cancers. Am. J. Obs. Gynecol. 2018, 219, 463.e1–463.e12. [Google Scholar] [CrossRef]
- Chu, L.H.; Chang, W.C.; Sheu, B.C. Comparison of the laparoscopic versus conventional open method for surgical staging of endometrial carcinoma. Taiwan J. Obs. Gynecol. 2016, 55, 188–192. [Google Scholar] [CrossRef][Green Version]
- Eisenkop, S.M. Total laparoscopic hysterectomy with pelvic/aortic lymph node dissection for endometrial cancer—A consecutive series without case selection and comparison to laparotomy. Gynecol. Oncol. 2010, 117, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Palomba, S.; Ghezzi, F.; Falbo, A.; Mandato, V.D.; Annunziata, G.; Lucia, E.; Cromi, A.; Abrate, M.; La Sala, G.B.; Giorda, G.; et al. Laparoscopic versus abdominal approach to endometrial cancer: A 10-year retrospective multicenter analysis. Int. J. Gynecol. Cancer 2012, 22, 425–433. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Zeng, D.; Ou, H.; Tang, Y.; Li, J.; Zhong, H. Laparoscopic treatment of endometrial cancer: Systematic review. J. Minim. Invasive Gynecol. 2013, 20, 413–423. [Google Scholar] [CrossRef]
- Eisenkop, S.M. Total Laparoscopic Hysterectomy with Pelvic/Aortic Lymph Node Dissection for Endometrial Cancer Using Passive Instrument Positioners: A Retrospective Case-Control Series. J. Minim. Invasive Gynecol. 2018, 25, 800–809. [Google Scholar] [CrossRef]
- Bergstrom, J.; Aloisi, A.; Armbruster, S.; Yen, T.T.; Casarin, J.; Leitao, M.M., Jr.; Tanner, E.J.; Matsuno, R.; Machado, K.K.; Dowdy, S.C.; et al. Minimally invasive hysterectomy surgery rates for endometrial cancer performed at National Comprehensive Cancer Network (NCCN) Centers. Gynecol. Oncol. 2018, 148, 480–484. [Google Scholar] [CrossRef]
- Vardar, M.A.; Gulec, U.K.; Guzel, A.B.; Gumurdulu, D.; Khatib, G.; Seydaoglu, G. Laparoscopic surgery for low, intermediate and high-risk endometrial cancer. J. Gynecol. Oncol. 2019, 30, e24. [Google Scholar] [CrossRef] [PubMed]
- Fader, A.N.; Java, J.; Tenney, M.; Ricci, S.; Gunderson, C.C.; Temkin, S.M.; Spirtos, N.; Kushnir, C.L.; Pearl, M.L.; Zivanovic, O.; et al. Impact of histology and surgical approach on survival among women with early-stage, high-grade uterine cancer: An NRG Oncology/Gynecologic Oncology Group ancillary analysis. Gynecol. Oncol. 2016, 143, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, F.; Cromi, A.; Uccella, S.; Siesto, G.; Giudici, S.; Serati, M.; Franchi, M. Laparoscopic versus open surgery for endometrial cancer: A minimum 3-year follow-up study. Ann. Surg Oncol. 2010, 17, 271–278. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | LT | LS | p | |||
|---|---|---|---|---|---|---|
| (Mean)/n | SD/(%) | (Mean)/n | SD/(%) | |||
| Age (years) | (59,3) | 10,7 | (57,5) | 10,1 | <0.05 | |
| Parity | (3,1) | 2,3 | (2,7) | 1,9 | <0.05 | |
| BMI (kg/m2) | (32,1) | 5,9 | (38,8) | 4,7 | <0.05 | |
| BMI group | <30 | 449 | (33,2) | 331 | (36,8) | <0.001 |
| 30–35 | 560 | (41,5) | 258 | (28,7) | ||
| 35–40 | 184 | (13,6) | 171 | (19,0) | ||
| >40 | 158 | (11,7) | 139 | (15,5) | ||
| Comorbidities | No | 565 | (34,5) | 480 | (48,0) | <0.001 |
| Yes | 1072 | (65,5) | 521 | (52,0) | ||
| Menopausal status | Premenopausal | 307 | (35,2) | 248 | (32,8) | <0.001 |
| Postmenopausal | 566 | (64,8) | 507 | (67,2) | ||
| Operation type | TH + BSO | 510 | (29) | 329 | (32,9) | <0.001 |
| TH + BSO + BPLND ± OMENTECTOMY | 386 | (21,3) | 440 | (44,0) | ||
| TH + BSO + BPPALND ± OMENTECTOMY | 847 | (49,7) | 233 | (14,2) | ||
| Perioperative complications | No | 1255 | (95,2) | 736 | (97,0) | <0.001 |
| Bleeding | 54 | (4,1) | 9 | (1,2) | ||
| Urinary system injury | 4 | (,3) | 8 | (1,1) | ||
| Intestinal injury | 2 | (,2) | 4 | (,5) | ||
| Others | 3 | (,2) | 2 | (,3) | ||
| Postoperative complications | No | 1221 | (92,4) | 727 | (95,7) | <0.001 |
| Infection | 88 | (6,7) | 15 | (2,0) | ||
| Urinary system injury | 0 | (,0) | 1 | (,1) | ||
| Intestinal injury | 1 | (,1) | 2 | (,3) | ||
| Others | 12 | (,9) | 15 | (2,0) | ||
| Operation time (minute) | (119,3) | 42,8 | (142,2) | 66,4 | <0.05 | |
| Estimated blood loss (mL) | (243,3) | 167,2 | (114,6) | 81,7 | <0.05 | |
| Drop in hemoglobin (gr/dL) | (1,6) | 1,1 | (1,4) | 1,1 | <0.05 | |
| Conversion of laparoscopy to laparotomy | 27 | (3,0) | ||||
| Postoperative hospitalization (day) | (5.4) | 3.3 | (3.3) | 1.7 | <0.05 | |
| Variables | LT | LS | p | |||
|---|---|---|---|---|---|---|
| (Mean)/n | SD/(%) | (Mean)/n | SD/(%) | |||
| Stage | 1a | 825 | (47,3) | 664 | (66,2) | <0.001 |
| 1b | 372 | (21,4) | 195 | (19,4) | ||
| 2 | 130 | (7,4) | 31 | (3,1) | ||
| 3a + 3b + 3c + 4 | 414 | (23,9) | 114 | (11,3) | ||
| Histopathology | Endometrioid | 1280 | (79,1) | 875 | (87,9) | <0.001 |
| Serous | 113 | (7,0) | 38 | (3,8) | ||
| Clear | 33 | (2,0) | 2 | (,2) | ||
| Mixed | 128 | (7,9) | 67 | (6,7) | ||
| Carcinosarcoma | 65 | (4,0) | 14 | (1,4) | ||
| Histologic type | Type1 | 1280 | (79,1) | 875 | (87,9) | <0.001 |
| Type2 | 339 | (20,9) | 121 | (12,1) | ||
| Grade | 1 | 715 | (43,9) | 537 | (54,7) | <0.001 |
| 2 | 524 | (32,2) | 342 | (34,9) | ||
| 3 | 389 | (23,9) | 102 | (10,4) | ||
| Myometrial invasion | No | 324 | (20,1) | 239 | (24,0) | <0.001 |
| <%50 | 670 | (41,6) | 506 | (50,8) | ||
| ≥%50 | 615 | (38,2) | 252 | (25,3) | ||
| Cervical invasion | No | 1065 | (83,5) | 711 | (95,4) | <0.001 |
| Yes | 211 | (16,5) | 34 | (4,6) | ||
| LVSI | No | 988 | (64,0) | 749 | (77,3) | <0.001 |
| Yes | 555 | (36,0) | 220 | (22,7) | ||
| LN count | No lymphadenectomy | 510 | (29,3) | 329 | (32,7) | 0.037 |
| 1–20 | 460 | (26,3) | 267 | (26,7) | ||
| 21–40 | 453 | (26,1) | 259 | (25,9) | ||
| >40 | 320 | (18,3) | 147 | (14,6) | ||
| Metastatic LN | No | 1512 | (86,8) | 931 | (93,0) | <0.001 |
| Pelvic | 103 | (5,9) | 46 | (4,6) | ||
| Paraaortic | 41 | (2,3) | 8 | (0,7) | ||
| Pelvic + paraaortic | 87 | (5,0) | 17 | (1,7) | ||
| Risk Group | DFS | OS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| LT | LS | LT | LS | |||||||
| Total n/Censored% | Mean | Total n/Censored% | Mean | p | Total n/Censored% | Mean | Total n/Censored% | Mean | p | |
| Low | 668/96,4 | 121,6 | 564/98,2 | 120,7 | 0,274 | 668/96,9 | 122,8 | 564/98,4 | 121,2 | 0,320 |
| Intermediate | 234/84,2 | 89,6 | 130/91,5 | 105,3 | 0,180 | 234/90,6 | 109,7 | 130/96,2 | 110,8 | 0,129 |
| High-intermediate | 271/75,6 | 80,0 | 121/75,2 | 77,7 | 0,366 | 271/87,8 | 101,9 | 121/94,2 | 98,2 | 0,153 |
| High | 464/53,2 | 32,4 | 186/54,3 | 23,9 | 0,106 | 464/72,8 | 60,5 | 186/78,0 | 58,8 | 0,231 |
| p | <0.001 | <0.001 | <0.001 | <0.001 | ||||||
| Variables | Total/Dead n | DFS Mean | OS Mean |
|---|---|---|---|
| Metastatic lymph node | |||
| No | 2317/132 | 98.5 | 115.9 |
| Yes | 283/109 | 19.5 | 44.9 |
| p | <0.001 | <0.001 | |
| Stage | |||
| 1a | 1502/47 | 120.0 | 121.3 |
| 1b | 567/40 | 74.0 | 112.5 |
| 2 | 162/31 | 52.8 | 82.5 |
| 3a + 3b + 3c + 4 | 394/130 | 23.4 | 54.9 |
| p | <0.001 | <0.001 | |
| Grade | |||
| 1 | 1208/49 | 122.1 | 129.3 |
| 2 | 798/63 | 92.3 | 114.1 |
| 3 | 231/51 | 24.0 | 74.6 |
| p | <0.001 | <0.001 | |
| Myometrial invasion | |||
| None | 867/153 | 119.3 | 121.3 |
| <%50 | 1176/64 | 110.4 | 115.2 |
| ≥%50 | 271/80 | 51.5 | 93.3 |
| p | <0.001 | <0.001 | |
| Lymphovascular space invasion | |||
| No | 1737/77 | 110.9 | 118.4 |
| Yes | 775/154 | 51.8 | 85.3 |
| p | <0.001 | <0.001 | |
| Histopathological type | |||
| Type 1 | 2155/141 | 103.9 | 114.7 |
| Type 2 | 460/103 | 30.9 | 62.2 |
| p | <0.001 | <0.001 |
| Variables | HR (95,0% CI) | |||
|---|---|---|---|---|
| DFS | p | OS | p | |
| Age | 1,025 (1,012–1,038) | <0.001 | 1,038 (1,020–1,055) | <0.001 |
| Surgery type | 1,055 (0,869–1,282) | 0.587 | 1,338 (0,895–1,999) | 0.156 |
| Comorbidities | 0,980 (0,762–1,262) | 0.877 | 0,959 (0,669–1,374) | 0.820 |
| BMI <30 | ref | |||
| 30–40 | 1,281 (0,946–1,735) | 0.109 | 1,831 (1,150–2,914) | 0.011 |
| >40 | 1,386 (1,032–1,863) | 0.003 | 2,133 (1,353–3,361) | 0.001 |
| MI | ref | |||
| None | 0,689 (0,434–1,095) | 0.115 | 0,640 (0,381–1,076) | 0.092 |
| <%50 | 1,008 (0,599–1,698) | 0.975 | 0,770 (0,427–1,387) | 0.383 |
| >%50 | 0,887 (0,618–1,274) | 0.517 | 0,713 (0,398–1,275) | 0.253 |
| LVSI | 1,374 (0,987–1,912) | 0.060 | 1,982 (1,288–3,050) | 0.002 |
| Cervical invasion | 1,713 (1,131–2,595) | 0.011 | 3,139 (1,662–5,926) | <0.001 |
| Metastatic LN | ref | |||
| Stage 1a | 1,051 (0,669–1,652) | 0.828 | 0,576 (0,268–1,241) | 0.159 |
| 1b | 1,847 (1,083–3,150) | 0.024 | 1,379 (0,623–3,052) | 0.427 |
| 2 | 2,012 (1,226–3,303) | 0.006 | 1,519 (0,685–3,368) | 0.304 |
| 3a + 3b + 3c + 4 | ref | |||
| Grade 1 | 0,428 (0,313–0,585) | 0.146 | 0,643 (0,392–1,054) | 0.280 |
| 2 | 0,827 (0,641–1,067) | 0.761 | 0,791 (0,518–1,210) | 0.458 |
| 3 | 1,973 (1,495–2,605) | <0.001 | 1,462 (0,974–2,196) | 0.067 |
| Histopathological type | ref | |||
| Risk group Low | 1,204 (0,935–1,549) | 0.082 | 2,411 (1,076–5,405) | 0.036 |
| Intermediate | 2,833 (1,452–5,529) | 0.002 | 2,406 (1,084–5,337) | 0.019 |
| High–intermediate | 6,349 (3,569–11,294) | <0.001 | 3,216 (1,482–6,978) | <0.001 |
| High | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vardar, M.A.; Guzel, A.B.; Taskin, S.; Gungor, M.; Ozgul, N.; Salman, C.; Kucukgoz-Gulec, U.; Khatib, G.; Taskiran, C.; Dünder, I.; et al. Could the Long-Term Oncological Safety of Laparoscopic Surgery in Low-Risk Endometrial Cancer also Be Valid for the High–Intermediate- and High-Risk Patients? A Multi-Center Turkish Gynecologic Oncology Group Study Conducted with 2745 Endometrial Cancer Cases. (TRSGO-End-001). Curr. Oncol. 2021, 28, 4328-4340. https://doi.org/10.3390/curroncol28060368
Vardar MA, Guzel AB, Taskin S, Gungor M, Ozgul N, Salman C, Kucukgoz-Gulec U, Khatib G, Taskiran C, Dünder I, et al. Could the Long-Term Oncological Safety of Laparoscopic Surgery in Low-Risk Endometrial Cancer also Be Valid for the High–Intermediate- and High-Risk Patients? A Multi-Center Turkish Gynecologic Oncology Group Study Conducted with 2745 Endometrial Cancer Cases. (TRSGO-End-001). Current Oncology. 2021; 28(6):4328-4340. https://doi.org/10.3390/curroncol28060368
Chicago/Turabian StyleVardar, Mehmet Ali, Ahmet Baris Guzel, Salih Taskin, Mete Gungor, Nejat Ozgul, Coskun Salman, Umran Kucukgoz-Gulec, Ghanim Khatib, Cagatay Taskiran, Ilkkan Dünder, and et al. 2021. "Could the Long-Term Oncological Safety of Laparoscopic Surgery in Low-Risk Endometrial Cancer also Be Valid for the High–Intermediate- and High-Risk Patients? A Multi-Center Turkish Gynecologic Oncology Group Study Conducted with 2745 Endometrial Cancer Cases. (TRSGO-End-001)" Current Oncology 28, no. 6: 4328-4340. https://doi.org/10.3390/curroncol28060368
APA StyleVardar, M. A., Guzel, A. B., Taskin, S., Gungor, M., Ozgul, N., Salman, C., Kucukgoz-Gulec, U., Khatib, G., Taskiran, C., Dünder, I., Ortac, F., Yuce, K., Terek, C., Simsek, T., Ozsaran, A., Onan, A., Coban, G., Topuz, S., Demirkiran, F., ... Ayhan, A. (2021). Could the Long-Term Oncological Safety of Laparoscopic Surgery in Low-Risk Endometrial Cancer also Be Valid for the High–Intermediate- and High-Risk Patients? A Multi-Center Turkish Gynecologic Oncology Group Study Conducted with 2745 Endometrial Cancer Cases. (TRSGO-End-001). Current Oncology, 28(6), 4328-4340. https://doi.org/10.3390/curroncol28060368