How Canadian Oncologists Use Oncotype DX for Treatment of Breast Cancer Patients

 ,
,
Abstract
1. Background
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ER | estrogen receptor |
| HER2 | human epidermal growth factor receptor 2 |
| HR | hormone receptor |
| LN | lymph node |
| ODX | Oncotype DX |
| PR | progesterone receptor |
| RS | recurrence score |
References
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) Comparisons between different polychemotherapy regimens for early breast cancer: Meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 2012, 379, 432–444. [CrossRef]
- Brewer, N.T.; Richman, A.R.; DeFrank, J.T.; Reyna, V.F.; Carey, L.A. Improving communication of breast cancer recurrence risk. Breast Cancer Res. Treat. 2012, 133, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Galea, M.H.; Blamey, R.W.; Elston, C.E.; Ellis, I.O. The Nottingham prognostic index in primary breast cancer. Breast Cancer Res. Treat. 1992, 22, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Fisher, B.; Jeong, J.; Bryant, J.; Anderson, S.; Dignam, J.; Fisher, E.R.; Wolmark, N. Treatment of lymph-node-negative, oestrogen-receptor-positive breast cancer: Long-term findings from National Surgical Adjuvant Breast and Bowel Project randomised clinical trials. Lancet 2004, 364, 858–868. [Google Scholar] [CrossRef]
- Foulkes, W. Size surprise? Tumour size, nodal status, and outcome after breast cancer. Curr. Oncol. 2012, 19, 241–243. [Google Scholar] [CrossRef] [PubMed]
- Oakman, C.; Bessi, S.; Zafarana, E.; Galardi, F.; Biganzoli, L.; Di Leo, A. Recent advances in systemic therapy. New diagnostics and biological predictors of outcome in early breast cancer. Breast Cancer Res. 2009, 11, 205. [Google Scholar] [CrossRef] [PubMed]
- Boughey, J.C.; McCall, L.M.; Ballman, K.V.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Flippo-Morton, T.; Hunt, K.K. Tumor Biology Correlates with Rates of Breast-Conserving Surgery and Pathologic Complete Response after Neoadjuvant Chemotherapy for Breast Cancer. Ann. Surg. 2014, 260, 608–616. [Google Scholar] [CrossRef]
- Blows, F.M.; Driver, K.E.; Schmidt, M.K.; Broeks, A.; Van Leeuwen, F.E.; Wesseling, J.; Cheang, M.C.; Gelmon, K.; Nielsen, T.O.; Blomqvist, C.; et al. Subtyping of Breast Cancer by Immunohistochemistry to Investigate a Relationship between Subtype and Short and Long Term Survival: A Collaborative Analysis of Data for 10,159 Cases from 12 Studies. PLoS Med. 2010, 7, e1000279. [Google Scholar] [CrossRef]
- Kudela, E.; Samec, M.; Kubatka, P.; Nachajova, M.; Laucekova, Z.; Liskova, A.; Dokus, K.; Biringer, K.; Simova, D.; Gabonova, E.; et al. Breast Cancer in Young Women: Status Quo and Advanced Disease Management by a Predictive, Preventive, and Personalized Approach. Cancers 2019, 11, 1791. [Google Scholar] [CrossRef]
- Cronin, M.; Sangli, C.; Liu, M.-L.; Pho, M.; Dutta, D.; Nguyen, A.; Jeong, J.; Wu, J.; Langone, K.C.; Watson, D. Analytical Validation of the Oncotype DX Genomic Diagnostic Test for Recurrence Prognosis and Therapeutic Response Prediction in Node-Negative, Estrogen Receptor–Positive Breast Cancer. Clin. Chem. 2007, 53, 1084–1091. [Google Scholar] [CrossRef]
- Sparano, J.A.; Paik, S. Development of the 21-Gene Assay and Its Application in Clinical Practice and Clinical Trials. J. Clin. Oncol. 2008, 26, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Mamounas, E.P.; Tang, G.; Fisher, B.; Paik, S.; Shak, S.; Costantino, J.P.; Watson, D.; Geyer, C.E., Jr.; Wickerham, D.L.; Wolmark, N. Association Between the 21-Gene Recurrence Score Assay and Risk of Locoregional Recurrence in Node-Negative, Estrogen Receptor–Positive Breast Cancer: Results from NSABP B-14 and NSABP B-20. J. Clin. Oncol. 2010, 28, 1677–1683. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Shak, S.; Paik, S.; Anderson, S.J.; Costantino, J.P.; Geyer, C.E., Jr.; Mamounas, E.P.; Wickerham, D.L.; Wolmark, N. Comparison of the prognostic and predictive utilities of the 21-gene Recurrence Score assay and Adjuvant for women with node-negative, ER-positive breast cancer: Results from NSABP B-14 and NSABP B-20. Breast Cancer Res. Treat. 2011, 127, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; Olson, J.A., Jr.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Albain, K.S.; Barlow, W.E.; Shak, S.; Hortobagyi, G.N.; Livingston, R.B.; Yeh, I.-T.; Ravdin, P.; Bugarini, R.; Baehner, F.L.; Davidson, N.E.; et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: A retrospective analysis of a randomised trial. Lancet Oncol. 2010, 11, 55–65. [Google Scholar] [CrossRef]
- Helwick, C. RxPONDER Study Shows Postmenopausal Patients with Node-Positive Breast Cancer May Be Able to Avoid Chemotherapy—The ASCO Post. American Society of Clinical Oncology Inc. Available online: https://ascopost.com/news/december-2020/rxponder-study-shows-postmenopausal-patients-with-node-positive-breast-cancer-may-be-able-to-avoid-chemotherapy/ (accessed on 23 December 2020).
- Dowsett, M.; Cuzick, J.; Wale, C.; Forbes, J.; Mallon, E.; Salter, J.; Quinn, E.; Dunbier, A.; Baum, M.; Buzdar, A.; et al. Prediction of Risk of Distant Recurrence Using the 21-Gene Recurrence Score in Node-Negative and Node-Positive Postmenopausal Patients with Breast Cancer Treated With Anastrozole or Tamoxifen: A TransATAC Study. J. Clin. Oncol. 2010, 28, 1829–1834. [Google Scholar] [CrossRef]
- Matikas, A.; Foukakis, T.; Swain, S.M.; Bergh, J. Avoiding over and undertreatment in patients with resected node-positive breast cancer with the use of gene expression signatures: Are we there yet? Ann. Oncol. 2019, 30, 1044–1050. [Google Scholar] [CrossRef]
- Nitz, U.; Gluz, O.; Christgen, M.; Kates, R.E.; Clemens, M.; Malter, W.; Nuding, B.; Aktas, B.; Kuemmel, S.; Reimer, T.; et al. Reducing chemotherapy use in clinically high-risk, genomically low-risk pN0 and pN1 early breast cancer patients: Five-year data from the prospective, randomised phase 3 West German Study Group (WSG) PlanB trial. Breast Cancer Res. Treat. 2017, 165, 573–583. [Google Scholar] [CrossRef]
- Loncaster, J.; Armstrong, A.; Howell, S.; Wilson, G.; Welch, R.; Chittalia, A.; Valentine, W.; Bundred, N. Impact of Oncotype DX breast Recurrence Score testing on adjuvant chemotherapy use in early breast cancer: Real world experience in Greater Manchester, UK. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 931–937. [Google Scholar] [CrossRef]
- Park, S.J.; Lee, M.H.; Kong, S.; Song, M.K.; Joo, J.; Kwon, Y.; Lee, E.-G.; Han, J.H.; Sim, S.H.; Jung, S.-Y.; et al. Use of adjuvant chemotherapy in hormone receptor-positive breast cancer patients with or without the 21-gene expression assay. Breast Cancer Res. Treat. 2018, 170, 69–76. [Google Scholar] [CrossRef]
- Sun, Z.; Prat, A.; Maggie, C.C.; Gelber, R.; Perou, C.M. Chemotherapy benefit for ‘ER-positive’ breast cancer and contamination of Nonluminal subtypes—Waiting for TAILORx and RxPONDER. Ann. Oncol. 2015, 26, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Henry, N.L.; Somerfield, M.R.; Abramson, V.G.; Ismaila, N.; Allison, K.H.; Anders, C.K.; Chingos, D.T.; Eisen, A.; Ferrari, B.L.; Openshaw, T.H.; et al. Role of Patient and Disease Factors in Adjuvant Systemic Therapy Decision Making for Early-Stage, Operable Breast Cancer: Update of the ASCO Endorsement of the Cancer Care Ontario Guideline. J. Clin. Oncol. 2019, 37, 1965–1977. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; King, T.A. Routine Use of Oncotype DX Recurrence Score Testing in Node-Positive Hormone Receptor-Positive HER2-Negative Breast Cancer: The Time Has Come. Ann. Surg. Oncol. 2019, 26, 1173–1175. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Dent, S.; Paquet, L.; Zhang, T.; Graham, N.; Song, X. Factors influencing Oncotype DX use in the management of early breast cancer: A single centre experience. Eur. J. Cancer 2014, 50, 2544–2549. [Google Scholar] [CrossRef]
- Nguyen, M.T.; Stessin, A.; Nagar, H.; D’Alfonso, T.M.; Chen, Z.; Cigler, T.; Hayes, M.K.; Shin, S.J. Impact of Oncotype DX Recurrence Score in the Management of Breast Cancer Cases. Clin. Breast Cancer 2014, 14, 182–190. [Google Scholar] [CrossRef]
- Eichler, C.; Fromme, J.; Thangarajah, F.; Puppe, J.; Paepke, S.; Warm, M.; Malter, W. Gene-expression Profiling—A Decision Impact Analysis: Decision Dependency on Oncotype DX® as a Function of Oncological Work Experience in 117 Cases. Anticancer. Res. 2019, 39, 297–303. [Google Scholar] [CrossRef]
- De Boer, R.H.; Baker, C.; Speakman, D.; Chao, C.Y.; Yoshizawa, C.; Mann, G.B. The impact of a genomic assay (Oncotype DX) on adjuvant treatment recommendations in early breast cancer. Med. J. Aust. 2013, 199, 205–208. [Google Scholar] [CrossRef]
- Albanell, J.; González, A.; Ruiz-Borrego, M.; Alba, E.; García-Saenz, J.A.; Corominas, J.M.; Burgues, O.; Furio, V.; Rojo, A.; Palacios, J.; et al. Prospective transGEICAM study of the impact of the 21-gene Recurrence Score assay and traditional clinicopathological factors on adjuvant clinical decision making in women with estrogen receptor-positive (ER+) node-negative breast cancer. Ann. Oncol. 2011, 23, 625–631. [Google Scholar] [CrossRef]
- Torres, S.; Trudeau, M.E.; Gandhi, S.; Warner, E.; Verma, S.; Pritchard, K.I.; Petrella, T.M.; Hew-Shue, M.; Chao, C.; Eisen, A. Prospective Evaluation of the Impact of the 21-Gene Recurrence Score Assay on Adjuvant Treatment Decisions for Women with Node-Positive Breast Cancer in Ontario, Canada. Oncologist 2018, 23, 768–775. [Google Scholar] [CrossRef]
- Asad, J.; Jacobson, A.F.; Estabrook, A.; Smith, S.R.; Boolbol, S.K.; Feldman, S.M.; Osborne, M.P.; Boachie-Adjei, K.; Twardzik, W.; Tartter, P.I. Does oncotype DX recurrence score affect the management of patients with early-stage breast cancer? Am. J. Surg. 2008, 196, 527–529. [Google Scholar] [CrossRef]
- Eiermann, W.; Rezai, M.; Kümmel, S.; Kühn, T.; Warm, M.; Friedrichs, K.; Schneeweiss, A.; Markmann, S.; Eggemann, H.; Hilfrich, J.; et al. The 21-gene recurrence score assay impacts adjuvant therapy recommendations for ER-positive, node-negative and node-positive early breast cancer resulting in a risk-adapted change in chemotherapy use. Ann. Oncol. 2013, 24, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Henry, L.R.; Stojadinovic, A.; Swain, S.M.; Prindiville, S.; Cordes, R.; Soballe, P.W. The influence of a Gene expression profile on breast cancer decisions. J. Surg. Oncol. 2009, 99, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Lo, S.S.; Mumby, P.B.; Norton, J.; Rychlik, K.; Smerage, J.; Kash, J.; Chew, H.K.; Gaynor, E.R.; Hayes, D.F.; Epstein, A.; et al. Prospective Multicenter Study of the Impact of the 21-Gene Recurrence Score Assay on Medical Oncologist and Patient Adjuvant Breast Cancer Treatment Selection. J. Clin. Oncol. 2010, 28, 1671–1676. [Google Scholar] [CrossRef] [PubMed]
- McVeigh, T.P.; Kerin, M.J. Clinical use of the Oncotype DX genomic test to guide treatment decisions for patients with invasive breast cancer. Breast Cancer Targets Ther. 2017, 9, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Rutter, C.E.; Yao, X.; Mancini, B.R.; Aminawung, J.A.; Chagpar, A.B.; Saglam, O.; Hofstatter, E.; Abu-Khalaf, M.; Gross, C.P.; Evans, S.B.; et al. Influence of a 21-Gene Recurrence Score Assay on Chemotherapy Delivery in Breast Cancer. Clin. Breast Cancer 2016, 16, 59–62. [Google Scholar] [CrossRef] [PubMed]
- Bombard, Y.; Rozmovits, L.; Trudeau, M.; Leighl, N.B.; Deal, K.; Marshall, D.A. The Value of Personalizing Medicine: Medical Oncologists’ Views on Gene Expression Profiling in Breast Cancer Treatment. Oncologist 2015, 20, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Leggett, L.E.; Lorenzetti, D.L.; Noseworthy, T.; Tiwana, S.; MacKean, G.; Clement, F. Experiences and attitudes toward risk of recurrence testing in women with breast cancer: A systematic review. Breast Cancer Res. Treat. 2014, 144, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Murciano-Goroff, Y.R.; McCarthy, A.M.; Bristol, M.N.; Groeneveld, P.; Domchek, S.M.; Motanya, U.N.; Armstrong, K. Uptake of BRCA 1/2 and oncotype DX testing by medical and surgical oncologists. Breast Cancer Res. Treat. 2018, 171, 173–180. [Google Scholar] [CrossRef]
- Orucevic, A.; Bell, J.L.; King, M.; McNabb, A.; Heidel, R.E. Nomogram update based on TAILORx clinical trial results—Oncotype DX breast cancer recurrence score can be predicted using clinicopathologic data. Breast 2019, 46, 116–125. [Google Scholar] [CrossRef]
- Prat, A.; Parker, J.S.; Fan, C.; Cheang, M.C.U.; Miller, L.D.; Bergh, J.; Chia, S.K.L.; Bernard, P.S.; Nielsen, T.O.; Ellis, M.J.; et al. Concordance among gene expression-based predictors for ER-positive breast cancer treated with adjuvant tamoxifen. Ann. Oncol. 2012, 23, 2866–2873. [Google Scholar] [CrossRef]
- Zheng, A.; Zhang, L.; Ji, Z.; Fan, L.; Jin, F. Oncotype DX for Comprehensive Treatment in Male Breast Cancer: A Case Report and Literature Review. Am. J. Men’s Heal. 2019, 13. [Google Scholar] [CrossRef] [PubMed]
- Canadian Medical Association. Medical Oncology Profile. 2019. Available online: https://www.cma.ca/sites/default/files/2019-01/medical-oncology-e.pdf (accessed on 23 December 2020).




{kind=link}
{kind=link}
{kind=link}
| Oncologist Demographic and Practice Type | Survey Answer Frequency (%) |
|---|---|
| Percentage of breast cancer patients | |
| 0–25% | 10 (21.3) |
| 25–50% | 9 (19.2) |
| 50–75% | 11 (23.4) |
| >75% | 17 (36.2) |
| Province you practice | |
| Alberta | 4 (8.5) |
| British Columbia | 10 (21.3) |
| Manitoba | 2 (4.3) |
| New Brunswick | 1 (2.1) |
| Newfoundland and Labrador | 4 (8.5) |
| Nova Scotia | 1 (2.1) |
| Ontario | 22 (46.8) |
| Prince Edward Island | 1 (2.1) |
| Quebec | 2 (4.3) |
| Practice Setup | |
| Academic Cancer Center | 33 (73.3) |
| Community Cancer Center | 12 (26.7) |
| Years in Practice | |
| 0–10 years | 19 (40.4) |
| 10–20 years | 11 (23.4) |
| >20 years | 17 (36.2) |
| Gender | |
| Female | 24 (52.2) |
| Male | 22 (47.8) |
| Province fund the use of Oncotype Dx | |
| Yes | 25 (53.2) |
| No | 16 (34.0) |
| Limited/not sure | 6 (12.8) |
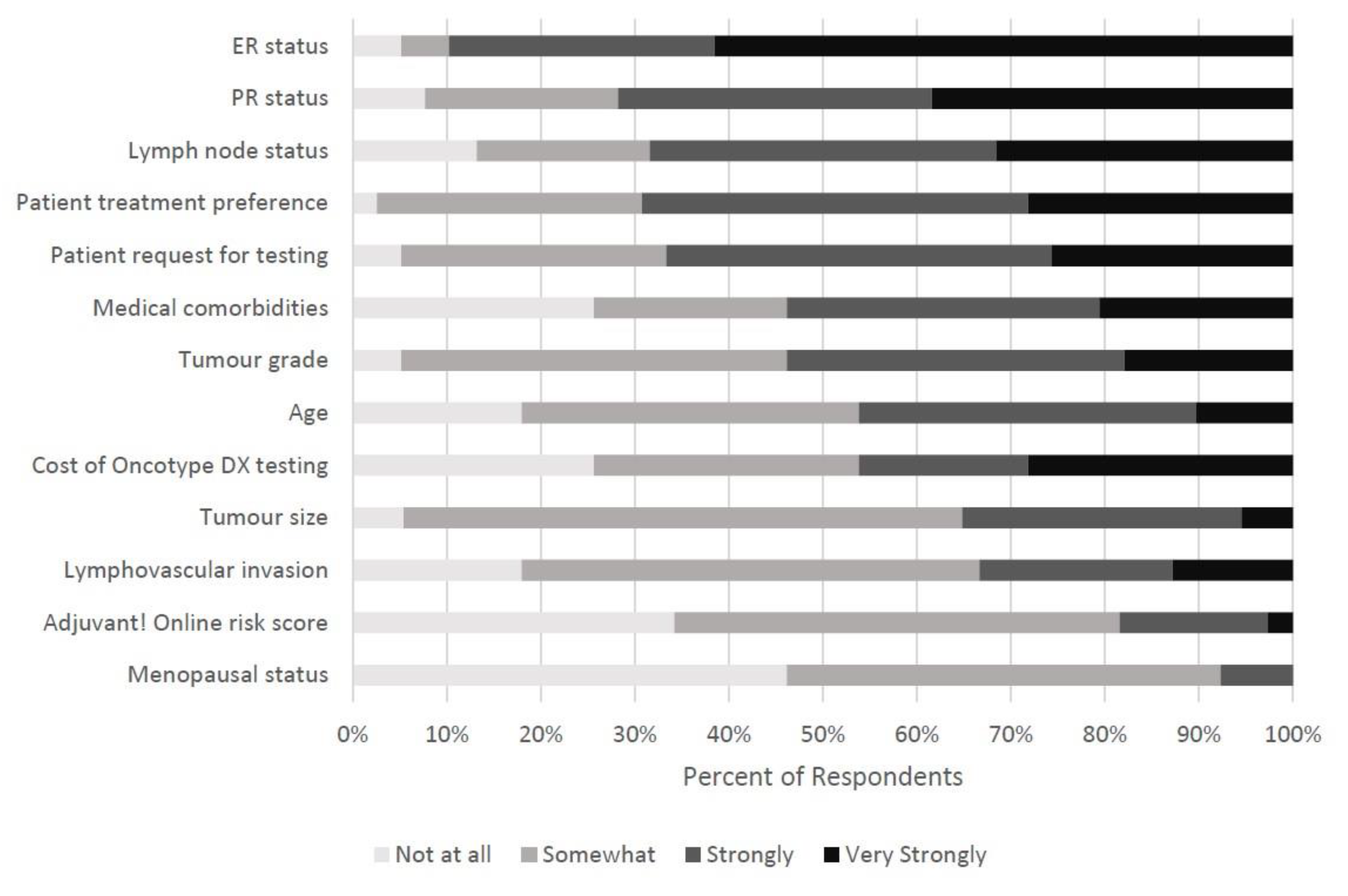
| Characteristic—No (%) | Not at All | Somewhat | Strongly | Very Strongly |
|---|---|---|---|---|
| ER status | 2 (5.1) | 2 (5.1) | 11 (28.2) | 24 (61.5) |
| PR status | 3 (7.7) | 8 (20.5) | 13 (33.3) | 15 (38.5) |
| Lymph node status | 5 (13.2) | 7 (18.4) | 14 (36.8) | 12 (31.6) |
| Patient treatment preference | 1 (2.6) | 11 (28.2) | 16 (41.0) | 11 (28.2) |
| Patient request for testing | 2 (5.1) | 11 (28.2) | 16 (41.0) | 10 (25.6) |
| Medical comorbidities | 10 (25.6) | 8 (20.5) | 13 (33.3) | 8 (20.5) |
| Tumor grade | 2 (5.1) | 16 (41.0) | 14 (35.9) | 7 (17.9) |
| Age | 7 (17.9) | 14 (35.9) | 14 (35.9) | 4 (10.3) |
| Cost of Oncotype DX testing | 10 (25.6) | 11 (28.2) | 7 (17.9) | 11 (28.2) |
| Tumor size | 2 (5.4) | 22 (59.5) | 11 (29.7) | 2 (5.4) |
| Lymphovascular invasion | 7 (17.9) | 19 (48.7) | 8 (20.5) | 5 (12.8) |
| Adjuvant! Online risk score | 13 (34.2) | 18 (47.4) | 6 (15.8) | 1 (2.6) |
| Menopausal status | 18 (46.2) | 18 (46.2) | 3 (7.7) | 0 (0.0) |
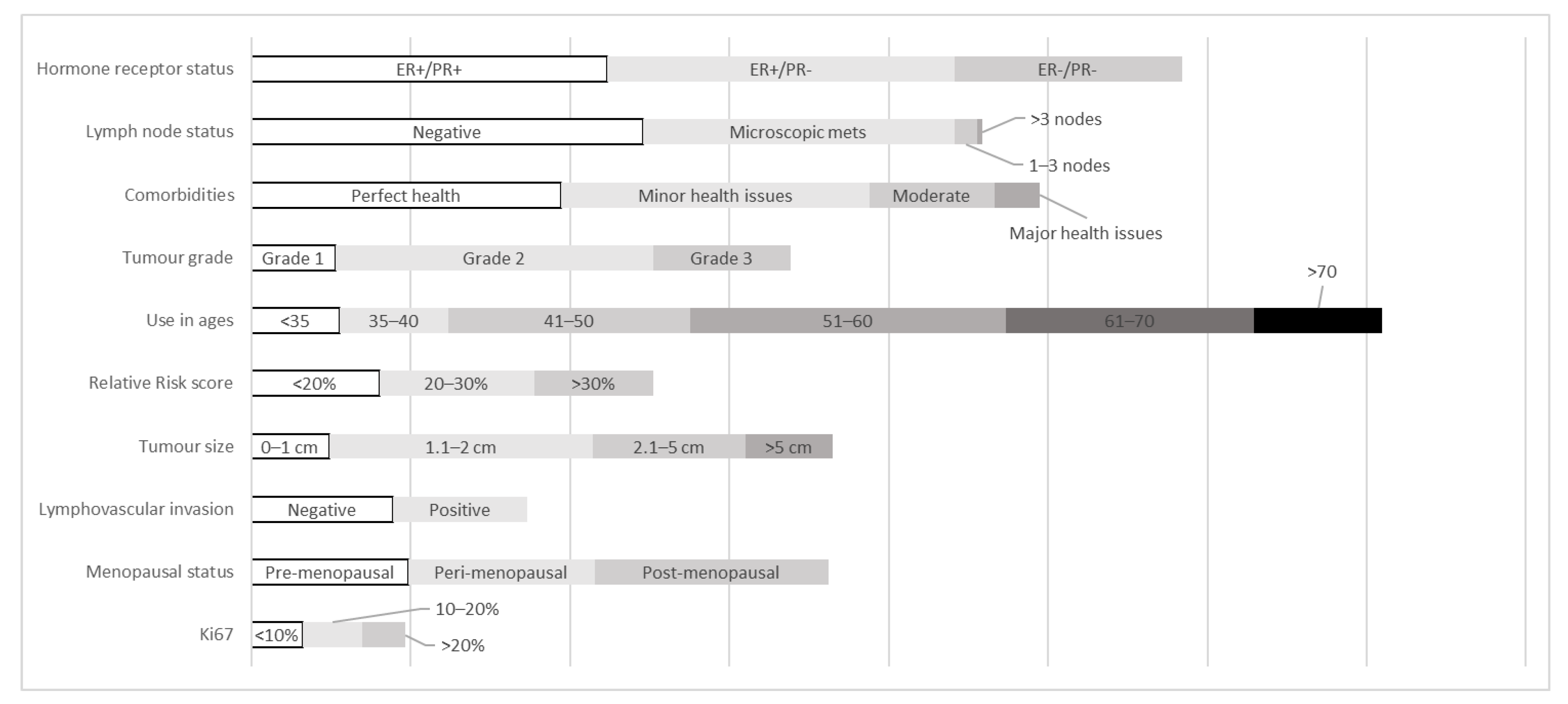
| Characteristic—No (%) | Never | Rarely | Sometimes | Often | Always |
|---|---|---|---|---|---|
| Hormone Stat | |||||
| ER+/PR+ | 2 (5.0) | 9 (22.5) | 16 (40.0) | 10 (25.0) | 3 (7.5) |
| ER+/PR− | 2 (5.0) | 8 (20.0) | 18 (45.0) | 9 (22.5) | 3 (7.5) |
| ER−/PR− | 14 (35.0) | 14 (35.0) | 3 (7.5) | 7 (17.5) | 2 (5.0) |
| Lymph node statu | |||||
| Negative | 1 (2.5) | 7 (17.5) | 16 (40.0) | 13 (32.5) | 3 (7.5) |
| Microscopic metastasis | 4 (10.0) | 9 (22.5) | 18 (45.0) | 6 (15.0) | 3 (7.5) |
| 1–3 nodes | 24 (60.0) | 10 (25.0) | 6 (15.0) | 0 (0.0) | 0 (0.0) |
| >3 nodes | 35 (87.5) | 5 (12.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Medical comorbidities | |||||
| Perfect Health | 2 (5.0) | 7 (17.5) | 18 (45.0) | 11 (27.5) | 2 (5.0) |
| Minor Health Issues | 2 (5.0) | 8 (20.0) | 17 (42.5) | 11 (27.5) | 2 (5.0) |
| Moderate Health Issues | 3 (7.9) | 14 (36.8) | 15 (39.5) | 6 (15.8) | 0 (0.0) |
| Major Health Issues | 16 (40.0) | 18 (45.0) | 4 (10.0) | 2 (5.0) | 0 (0.0) |
| Tumor grade | |||||
| Grade 1 | 9 (22.5) | 17 (42.5) | 10 (25.0) | 4 (10.0) | 0 (0.0) |
| Grade 2 | 2 (5.0) | 8 (20.0) | 16 (40.0) | 12 (30.0) | 2 (5.0) |
| Grade 3 | 6 (15.0) | 14 (35.0) | 12 (30.0) | 8 (20.0) | 0 (0.0) |
| Age | |||||
| <35 | 8 (20.0) | 21 (52.5) | 6 (15.0) | 5 (12.5) | 0 (0.0) |
| 35–40 | 3 (7.5) | 17 (42.5) | 15 (37.5) | 5 (12.5) | 0 (0.0) |
| 41–50 | 2 (5.0) | 11 (27.5) | 15 (37.5) | 11 (27.5) | 1 (2.5) |
| 51–60 | 2 (5.0) | 9 (22.5) | 15 (37.5) | 12 (30.0) | 2 (5.0) |
| 61–70 | 2 (5.1) | 10 (25.6) | 15 (38.5) | 11 (28.2) | 1 (2.6) |
| >70 | 10 (25.6) | 19 (48.7) | 6 (15.4) | 3 (7.7) | 1 (2.6) |
| Relative Risk Score | |||||
| 10 year RR < 20% | 4 (10.0) | 16 (40.0) | 13 (32.5) | 7 (17.5) | 0 (0.0) |
| 10 year RR 20–30% | 6 (15.0) | 10 (25.0) | 15 (37.5) | 9 (22.5) | 0 (0.0) |
| 10 year RR > 30% | 12 (30.0) | 11 (27.5) | 10 (25.0) | 7 (17.5) | 0 (0.0) |
| Tumor size | |||||
| 0–1 cm | 5 (12.5) | 25 (62.5) | 6 (15.0) | 4 (10.0) | 0 (0.0) |
| 1.1–2 cm | 2 (5.0) | 10 (25.0) | 14 (35.0) | 13 (32.5) | 1 (2.5) |
| 2.1–5 cm | 3 (7.5) | 10 (25.0) | 19 (47.5) | 8 (20.0) | 0 (0.0) |
| >5 cm | 15 (37.5) | 18 (45.0) | 6 (15.0) | 0 (0.0) | 1 (2.5) |
| Lymphovascular invasion | |||||
| Negative | 4 (10.5) | 10 (26.3) | 17 (44.7) | 7 (18.4) | 0 (0.0) |
| Positive | 6 (15.4) | 11 (28.2) | 15 (38.5) | 7 (17.9) | 0 (0.0) |
| Menopausal Status | |||||
| Premenopausal | 1 (2.5) | 15 (37.5) | 15 (37.5) | 9 (22.5) | 0 (0.0) |
| Perimenopausal | 2 (5.0) | 9 (22.5) | 18 (45.0) | 11 (27.5) | 0 (0.0) |
| Postmenopausal | 2 (5.0) | 10 (25.0) | 17 (42.5) | 10 (25.0) | 1 (2.5) |
| Ki67 | |||||
| <10% | 14 (42.4) | 8 (24.2) | 10 (30.3) | 1 (3.0) | 0 (0.0) |
| 10–20% | 13 (39.4) | 6 (18.2) | 13 (39.4) | 1 (3.0) | 0 (0.0) |
| >20% | 18 (54.4) | 7 (21.2) | 7 (21.2) | 1 (3.0) | 0 (0.0) |
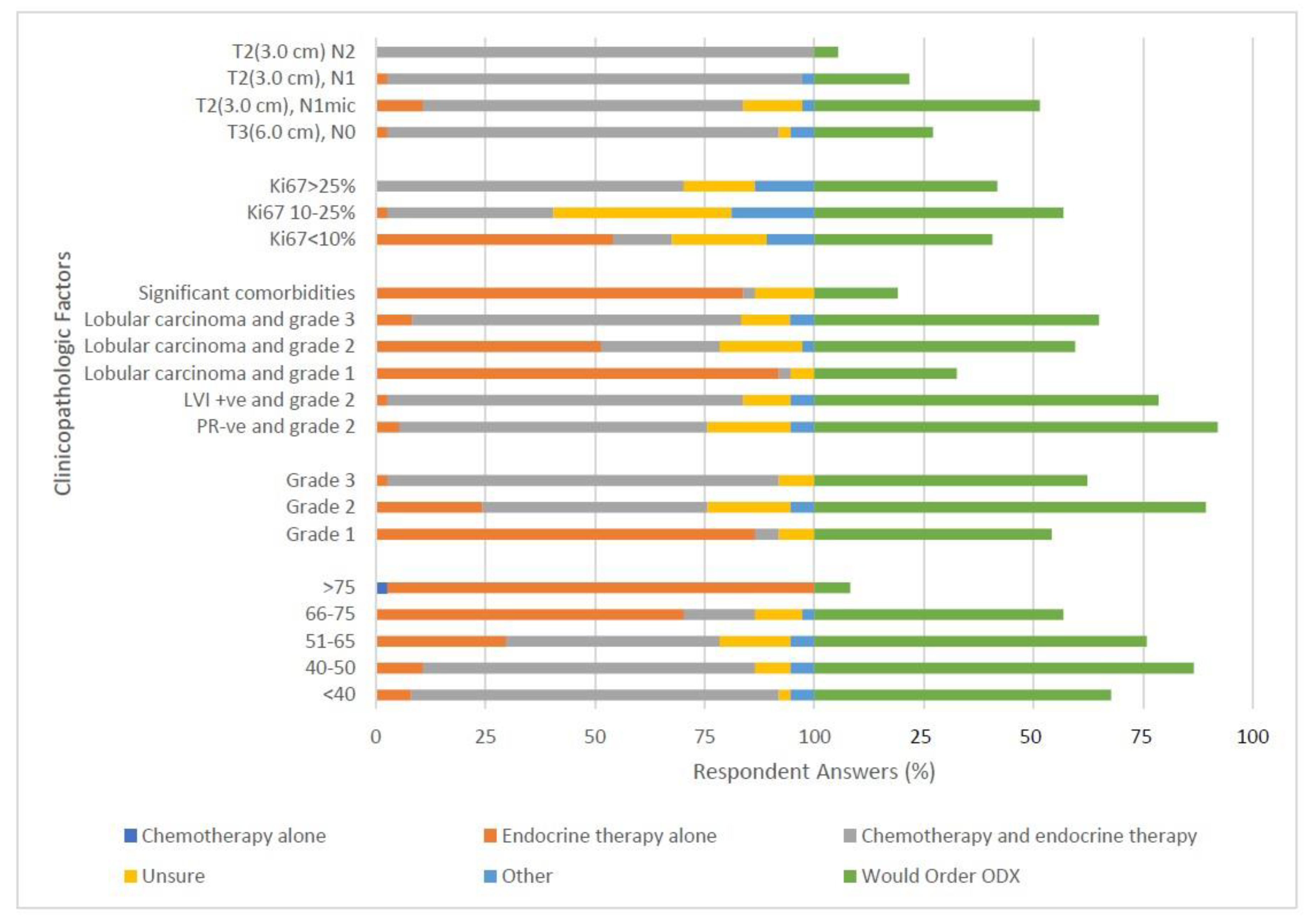
| Characteristic—No (%) | Chemo Alone | Endocrine Tx Alone | Chemo + Endocrine | Unsure | Other | Would Use ODX |
|---|---|---|---|---|---|---|
| Case 1: Age–no (%) | ||||||
| <40 | 0 (0.0) | 3 (8.1) | 31 (83.8) | 1 (2.7) | 2 (5.4) | 25 (67.6) |
| 40–50 | 0 (0.0) | 4 (10.8) | 28 (75.7) | 3 (8.1) | 2 (5.4) | 32 (86.5) |
| 51–65 | 0 (0.0) | 11 (29.7) | 18 (48.6) | 6 (16.2) | 2 (5.4) | 28 (75.7) |
| 66–75 | 0 (0.0) | 26 (70.3) | 6 (16.2) | 4 (10.8) | 1 (2.7) | 21 (56.8) |
| >75 | 1 (2.7) | 36 (97.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (8.1) |
| Case 2: Tumor Grade–no (%) | ||||||
| Grade 1 | 0 (0.0) | 32 (86.5) | 2 (5.4) | 3 (8.1) | 0 (0.0) | 20 (54.1) |
| Grade 2 | 0 (0.0) | 9 (24.3) | 19 (51.4) | 7 (18.9) | 2 (5.4) | 33 (89.2) |
| Grade 3 | 0 (0.0) | 1 (2.7) | 33 (89.2) | 3 (8.1) | 0 (0.0) | 23 (62.2) |
| Case 3: Other Risk Factors–no (%) | ||||||
| PR-ve and grade 2 | 0 (0.0) | 2 (5.4) | 26 (70.3) | 7 (18.9) | 2 (5.4) | 34 (91.9) |
| LVI +ve and grade 2 | 0 (0.0) | 1 (2.7) | 30 (81.1) | 4 (10.8) | 2 (5.4) | 29 (78.4) |
| Lobular carcinoma and grade 1 | 0 (0.0) | 34 (91.9) | 1 (2.7) | 2 (5.4) | 0 (0.0) | 12 (32.4) |
| Lobular carcinoma and grade 2 | 0 (0.0) | 19 (51.4) | 10 (27.0) | 7 (18.9) | 1 (2.7) | 22 (59.5) |
| Lobular carcinoma and grade 3 | 0 (0.0) | 3 (8.3) | 27 (75.0) | 4 (11.1) | 2 (5.6) | 24 (64.9) |
| Significant comorbidities | 0 (0.0) | 31 (83.8) | 1 (2.7) | 5 (13.5) | 0 (0.0) | 7 (18.9) |
| Case 4: Ki67 Status–no (%) | ||||||
| Ki67 < 10% | 0 (0.0) | 20 (54.1) | 5 (13.5) | 8 (21.6) | 4 (10.8) | 15 (40.5) |
| Ki67 10–25% | 0 (0.0) | 1 (2.7) | 14 (37.8) | 15 (40.5) | 7 (18.9) | 21 (56.8) |
| Ki67 > 25% | 0 (0.0) | 0 (0.0) | 26 (70.3) | 6 (16.2) | 5 (13.5) | 15 (41.7) |
| Case 5: Tumor Size and Nodal Status–no (%) | ||||||
| T3(6.0 cm), N0 | 0 (0.0) | 1 (2.7) | 33 (89.2) | 1 (2.7) | 2 (5.4) | 10 (27.0) |
| T2(3.0 cm), N1mic | 0 (0.0) | 4 (10.8) | 27 (73.0) | 5 (13.5) | 1 (2.7) | 19 (51.4) |
| T2(3.0 cm), N1 | 0 (0.0) | 1 (2.7) | 35 (94.6) | 0 (0.0) | 1 (2.7) | 8 (21.6) |
| T2(3.0 cm) N2 | 0 (0.0) | 0 (0.0) | 37 (100.0) | 0 (0.0) | 0 (0.0) | 2 (5.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, X.; Dent, S.; Paquet, L.; Zhang, T.; Tesolin, D.; Graham, N.; Aseyev, O.; Song, X. How Canadian Oncologists Use Oncotype DX for Treatment of Breast Cancer Patients. Curr. Oncol. 2021, 28, 800-812. https://doi.org/10.3390/curroncol28010077
Zhu X, Dent S, Paquet L, Zhang T, Tesolin D, Graham N, Aseyev O, Song X. How Canadian Oncologists Use Oncotype DX for Treatment of Breast Cancer Patients. Current Oncology. 2021; 28(1):800-812. https://doi.org/10.3390/curroncol28010077
Chicago/Turabian StyleZhu, Xiaofu, Susan Dent, Lise Paquet, Tinghua Zhang, Daniel Tesolin, Nadine Graham, Olexiy Aseyev, and Xinni Song. 2021. "How Canadian Oncologists Use Oncotype DX for Treatment of Breast Cancer Patients" Current Oncology 28, no. 1: 800-812. https://doi.org/10.3390/curroncol28010077
APA StyleZhu, X., Dent, S., Paquet, L., Zhang, T., Tesolin, D., Graham, N., Aseyev, O., & Song, X. (2021). How Canadian Oncologists Use Oncotype DX for Treatment of Breast Cancer Patients. Current Oncology, 28(1), 800-812. https://doi.org/10.3390/curroncol28010077