Case report
A 66-year-old man underwent aortic valve replacement (AVR) for severe aortic regurgitation in 2003. Macroscopic inspection at the time of surgery revealed a few old, healed vegetations on the nonand right-coronary cusps. Nine years later a second AVR (27-mm Trifecta bioprosthesis) was performed because of severe, symptomatic, transvalvular aortic regurgitation. Transthoracic echocardiography (TTE) at discharge and at 3 months showed a well-functioning bioprosthesis with normal leh ventricular ejection fraction (LVEF).
At six months, complaining of acute onset of leg pain in his leh thigh, the patient was referred by his angiologist for popliteal artery thrombosis and admitted directly to a medical ward at 5 pm the same evening. Upon admission he had no symptoms of heart failure and was not complaining of chest pain. Vital sign assessment showed no fever, heart rate was 85 bpm and blood pressure 110/60 mm Hg. The blood tests at admission revealed high BNP at 3281 ng/l, elevated CRP (71 mg/l) and leucocytosis (14.1 G/l), but no repartition was ordered. The ECG at admission showed conduction disturbances (Figure 1) including a very long first-degree atrioventricular block (460 ms), most probably intermittent Wenckebach block and leh bundle branch block.
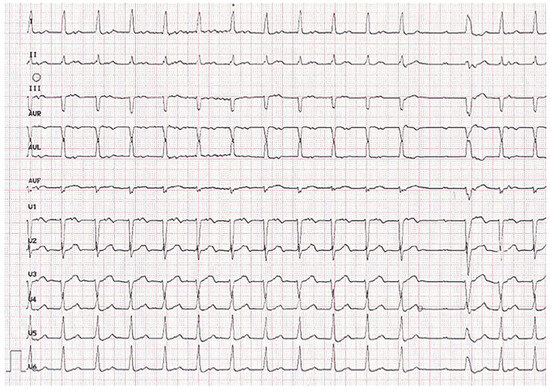
Figure 1.
ECG at admission. Showing conduction disturbances including a very long first degree atrioventricular block (460 ms), most probably intermittent Wenckebach block and left bundle branch block.
At 3 am, ten hours aher admission, he complained of sudden dyspnea and rapidly went into cardiac arrest. Cardiopulmonary resuscitation (CPR) was started. The initial rhythm was asystole. TTE revealed global hypokinesis (LEVF: 20%) and substantial rocking motion of the aortic bioprosthesis (Figure 2, panel A–B, video). The patient died despite CPR.
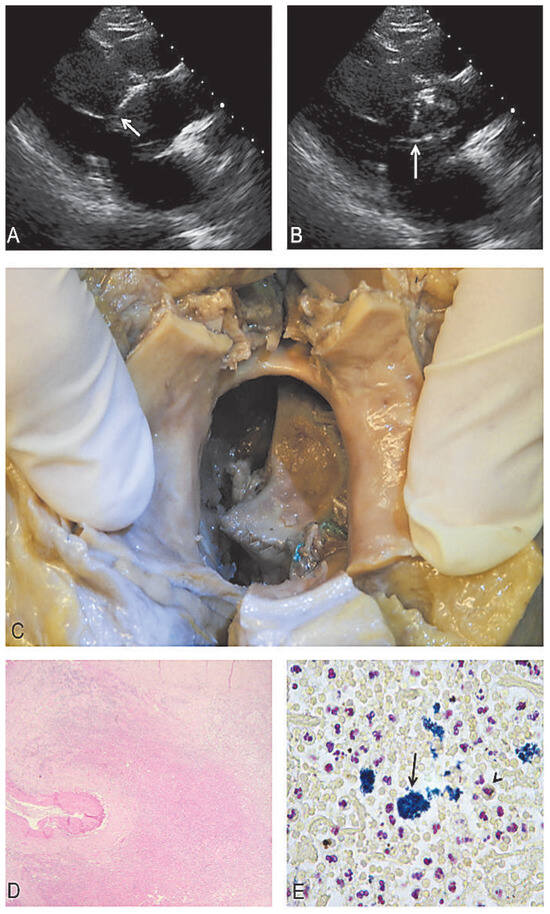
Figure 2.
Endocarditis. (A,B) Extreme rocking motion of the aortic bioprosthetic valve. (C) Macroscopic view at autopsy showing partial detachment of the aortic bioprosthesis which is rotated by 90 degrees. Microscopic assessment showing severe subacute endocarditis with necrotic tissue (D) and gram-positive bacteria (E, arrow). (See also the video1: Extreme rocking motion of the aortic bioprosthetic valve.).
Discussion
Paravalvular leak (PVL) post valvular surgery is the most common cause of nonstructural dysfunction of prosthetic heart valves [1]. Beyond the early postoperative period, PVL is secondary to suture dehiscence or endocarditis [2,3]. In our case, despite suggestive blood tests and conduction disturbances on the initial ECG, the diagnosis of endocarditis was overlooked. Importantly new conduction disturbances such as first-degree AV block in the presence of an aortic prosthetic valve should have raised the suspicion of a perivalvular abscess, since the abscess can extend into the adjacent conduction tissues and cause heart block. Rapid echocardiographic assessment could have helped in the diagnostic process in the context of peripheral artery occlusion, especially in the absence of atrial fibrillation. Indeed, other than congestive heart failure, septic arterial embolisation and its sequelae are the most common complications of endocarditis [4]. Septic embolisms are diagnosed in at least 30% of patients referred for valve replacement in the presence of endocarditis and approximately one third of the embolic events are in the peripheral vasculature, as was the case for our patient [4]. Other sites of embolisation are most commonly: pulmonary, splenic, renal, cerebral and coronary arteries. Finally the acute PVL secondary to subacute endocarditis could explain the extreme and acute clinical presentation. We cannot exclude that CPR might have contributed to worsening of the bioprosthesis detachment although rocking motion of 75º has been described in an infected bioprosthesis despite the absence of CPR [5].
The insertion of an ECMO (Extracorporal Membrane Oxygenation) as soon as the extreme rocking motion was detected could have been considered in order to unload the leh ventricle and could have yielded sufficient time until surgical valvular treatment was possible. However given the poor tissue quality seen at autopsy, successful aortic valve replacement would have been very difficult if not a failure. An early diagnosis of infective sub-acute endocarditis would have assured the best chance of improving the outcome for this patient.
Funding/potential competing interests
No financial support and no other potential conflict of interest relevant to this article were reported.
References
- Akins, C.W.; Bitondo, J.M.; Hilgenberg, A.D.; Vlahakes, G.J.; Madsen, J.C.; MacGillivray, T.E. Early and late results of the surgical correction of cardiac prosthetic paravalvular leaks. J Heart Valve Dis. 2005, 14, 792–799. [Google Scholar] [PubMed]
- Genoni, M.; Franzen, D.; Vogt, P.; Seifert, B.; Jenni, R.; Künzli, A.; et al. Paravalvular leakage aher mitral valve replacement: improved long-term survival with aggressive surgery? Eur J Cardiothorac Surg. 2000, 17, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Ferrer, J.J.; Fernandez-Jimenez, R.; Perez de Isla, L.; Rocafort, A.G.; Zamorano, J.L. Rocking aortic valve prosthesis: a 3-dimensional transesophageal echocardiography view. J Am Coll Cardiol. 2010, 55, e135. [Google Scholar] [CrossRef][Green Version]
- Stoney, R.J.; Kitts, D.J.; Bongard, F.S. Septic embolism complicating infective endocarditis. J Vasc Surg. 1991, 14, 480–487. [Google Scholar] [CrossRef]
- Metz, E.; Hartmann, M.; von Birgelen, C.; Haalebos, M.M.; Verhorst, P.M. Major dehiscence of infected aortic valve prosthesis with “rocking motion” but without diastolic paravalvular regurgitation. Int J Cardiovasc Imaging. 2006, 22, 771–774. [Google Scholar] [CrossRef] [PubMed]


© 2015 by the author. Attribution-Non-Commercial-NoDerivatives 4.0.