
Empowering Women, Enhancing Health: The Role of Education in Water, Sanitation, and Hygiene (WaSH) and Child Health Outcomes



Abstract
1. Introduction
2. Methods
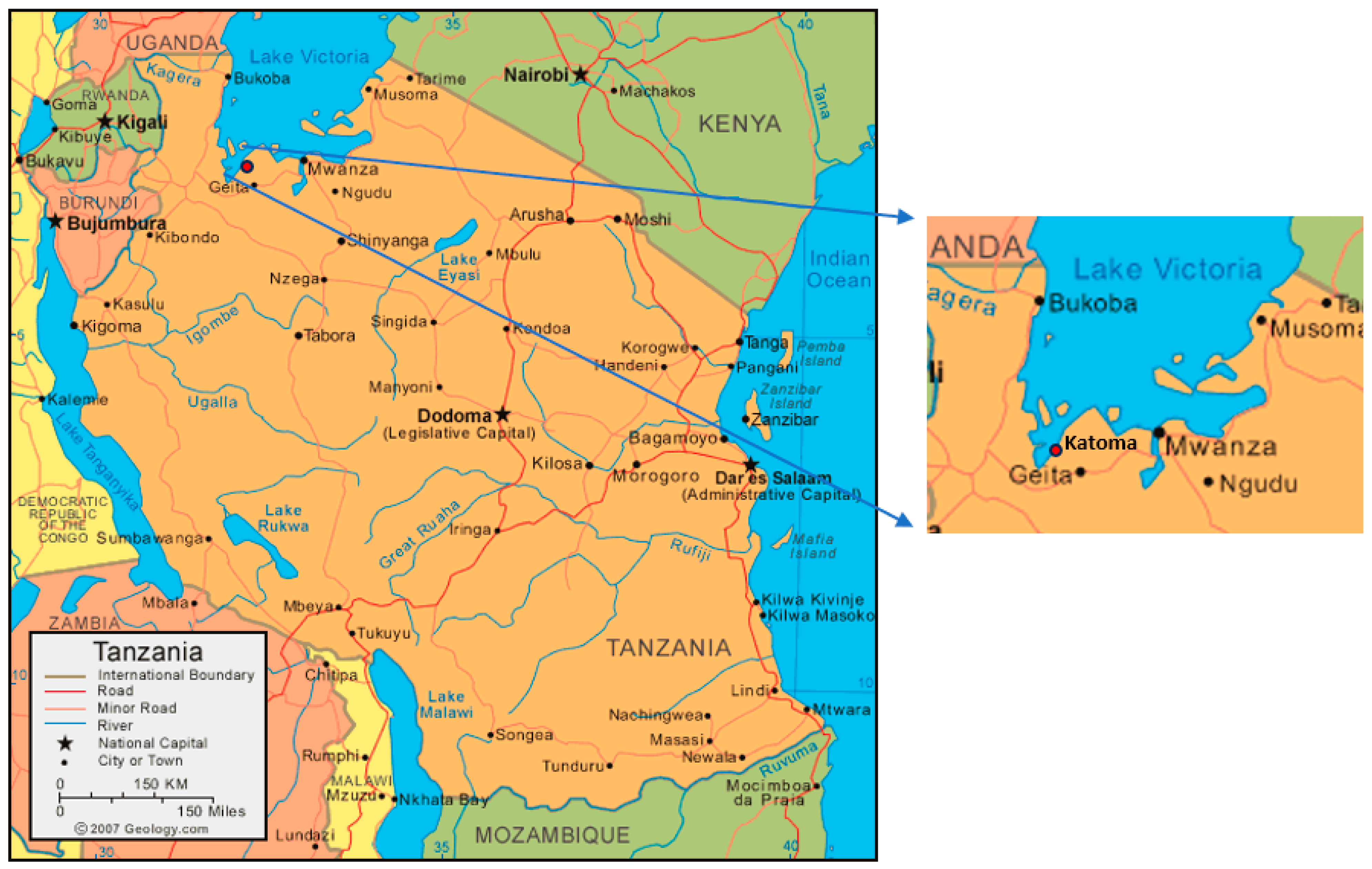
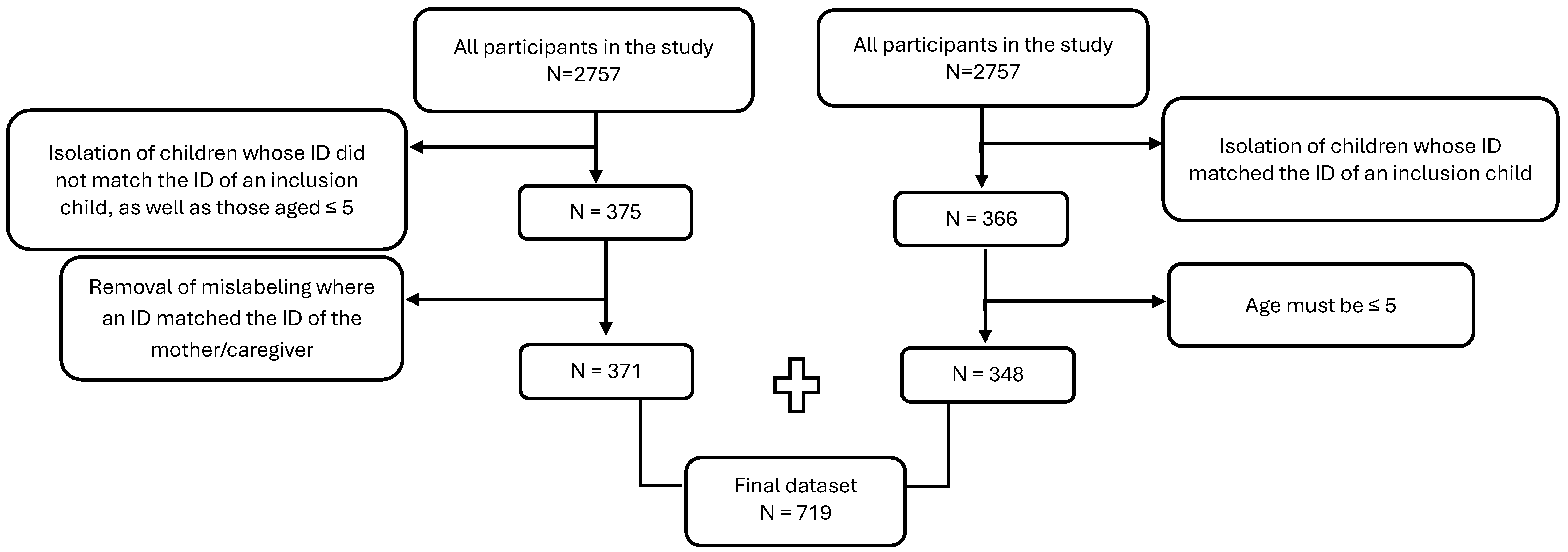
2.1. Study Design, Setting, and Participants
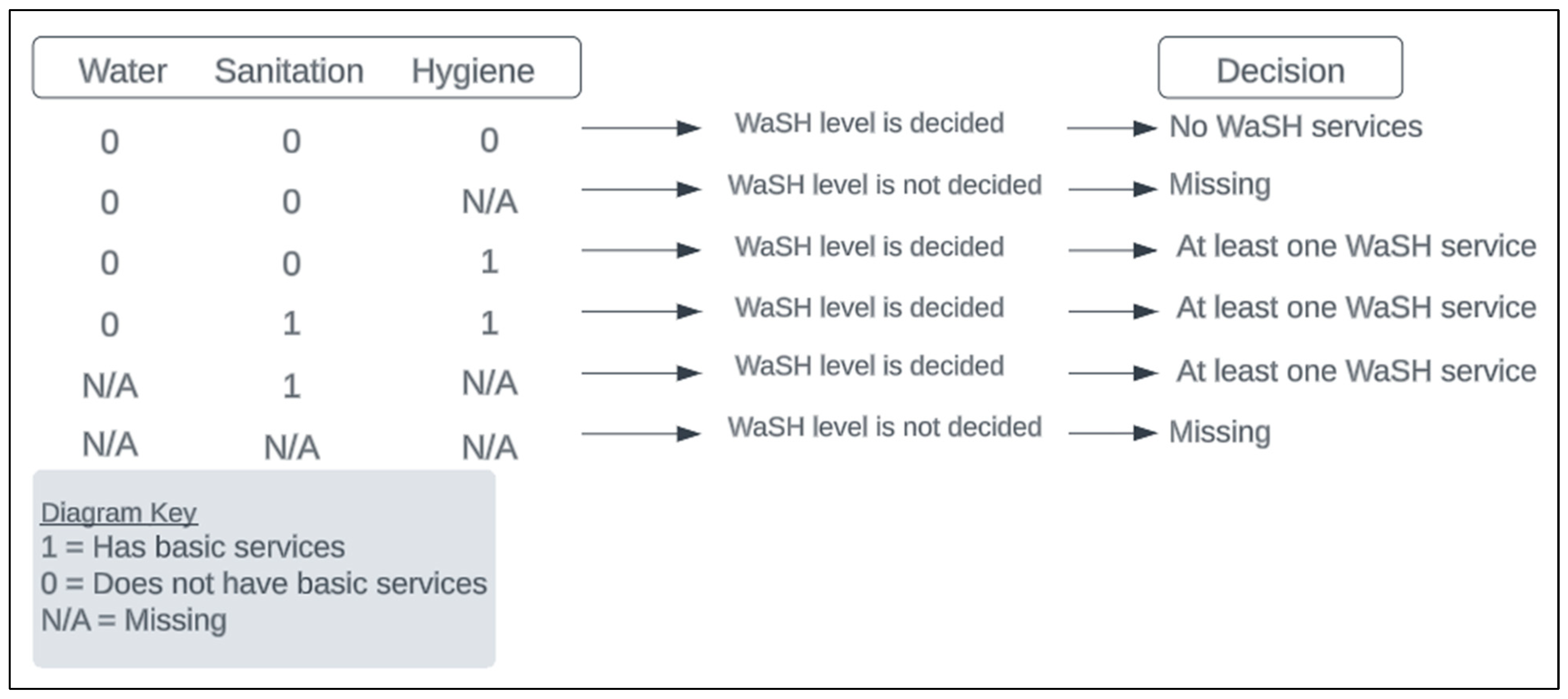
2.2. Outcome
2.3. Covariates
2.4. Missingness
2.5. Statistical Methods
3. Results
3.1. Study Participants
3.2. Exposure to Inadequate WaSH
3.3. Incidence of Diarrhea
3.4. Associations Between Inadequate WaSH and Diarrhea
3.5. Significant Predictors of Diarrhea
4. Discussion
5. Conclusions
5.1. Strengths and Limitations
5.2. Future Research
5.3. Practical Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF). Progress on Household Drinking Water, Sanitation and Hygiene 2000–2020: Five Years into the SDGs. 2021. Available online: https://washdata.org/sites/default/files/2021-07/jmp-2021-wash-households.pdf (accessed on 24 August 2023).
- United Nations Children’s Fund (UNICEF). Progress on Drinking Water, Sanitation and Hygiene 2017 Update and SDG Baselines. 2017. Available online: https://data.unicef.org/resources/progress-drinking-water-sanitation-hygiene-2017-update-sdg-baselines/ (accessed on 24 August 2023).
- Giri, M.; Behera, M.R.; Behera, D.; Mishra, B.; Jena, D. Water, Sanitation, and Hygiene Practices and Their Association with Childhood Diarrhoea in Rural Households of Mayurbhanj District, Odisha, India. Cureus 2022, 14, e29888. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kugedera, Z.; Chaudhry, A.A. WASH Results: Behavioural Determinants for WASH (Water Sanitation and Hygiene) Practices in Urban Households in Pakistan. UNICEF WASH RESULTS R/03/2022. 2022. Available online: https://knowledge.unicef.org/resource/wash-results-behavioural-determinants-wash-water-sanitation-and-hygiene-practices-urban (accessed on 13 April 2024).
- Darvesh, N.; Das, J.K.; Vaivada, T.; Gaffey, M.F.; Rasanathan, K.; Bhutta, Z.A. Social Determinants of Health Study Team. Water, sanitation and hygiene interventions for acute childhood diarrhea: A systematic review to provide estimates for the Lives Saved Tool. BMC Public Health 2017, 17, 776. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ramesh, A.; Blanchet, K.; Ensink, J.H.; Roberts, B. Evidence on the Effectiveness of Water, Sanitation, and Hygiene (WASH) Interventions on Health Outcomes in Humanitarian Crises: A Systematic Review. PLoS ONE 2015, 10, e0124688. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- WHO Regional Office for Europe. Surveillance and Outbreak Management of Water-Related Infectious Diseases Associated with Water-Supply Systems. 2019. Available online: https://apps.who.int/iris/bitstream/handle/10665/329403/9789289054454-eng.pdf (accessed on 24 August 2023).
- Centers for Disease Control and Prevention (CDC). Global WASH Fast Facts. Global Water, Sanitation, & Hygiene (WASH). 2022. Available online: https://www.cdc.gov/global-water-sanitation-hygiene/about/index.html (accessed on 24 August 2023).
- UNICEF. Diarrhea Remains a Leading Killer of Young Children, Despite the Availability of a Simple Treatment Solution. Diarrhea. 2022. Available online: https://data.unicef.org/topic/child-health/diarrhoeal-disease/ (accessed on 24 August 2023).
- Mayo Clinic. Symptoms and Causes. Diarrhea. 2021. Available online: https://www.mayoclinic.org/diseases-conditions/diarrhea/symptoms-causes/syc-20352241 (accessed on 24 August 2023).
- Troeger, C.; Blacker, B.F.; Khalil, I.A.; Rao, P.C.; Cao, S.; Zimsen, S.R.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and etiologies of diarrhea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef]
- Zerbo, A.; Castro Delgado, R.; Arcos González, P. Water sanitation and hygiene in Sub-Saharan Africa: Coverage, risks of diarrheal diseases, and urbanization. J. Biosaf. Biosecur. 2021, 3, 41–45. [Google Scholar] [CrossRef]
- UNICEF. Water, Sanitation and Hygiene. United Republic of Tanzania. Available online: https://www.unicef.org/tanzania/what-we-do/wash (accessed on 24 August 2023).
- Black, R.; Fontaine, O.; Lamberti, L.; Bhan, M.; Huicho, L.; El Arifeen, S.; Masanja, H.; Walker, C.F.; Mengestu, T.K.; Pearson, L.; et al. Drivers of the reduction in childhood diarrhea mortality 1980–2015 and interventions to eliminate preventable diarrhea deaths by 2030. J. Glob. Health 2019, 9, 020801. [Google Scholar] [CrossRef] [PubMed]
- Fagbamigbe, A.F.; Uthman, A.O.; Ibisomi, L. Hierarchical disentanglement of contextual from compositional risk factors of diarrhea among under-five children in low- and middle-income countries. Sci. Rep. 2021, 11, 8564. [Google Scholar] [CrossRef] [PubMed]
- GISGeography. Tanzania Map—Cities and Parks. GISGeography. 2023. Available online: https://gisgeography.com/tanzania-map/ (accessed on 24 August 2023).
- WHO/UNICEF Joint Monitoring Programme (JMP). Drinking Water. Monitoring. Available online: https://washdata.org/monitoring/drinking-water (accessed on 24 August 2023).
- WHO/UNICEF JMP. Sanitation. Monitoring. Available online: https://washdata.org/monitoring/sanitation (accessed on 24 August 2023).
- WHO/UNICEF JMP. Hygiene. Monitoring. Available online: https://washdata.org/monitoring/hygiene (accessed on 24 August 2023).
- Food and Agriculture Organization of the United Nations (FAO). Hunger and Food Insecurity. Hunger. 2003. Available online: https://www.fao.org/hunger/en/ (accessed on 24 August 2023).
- Kim, J.H. Multicollinearity and misleading statistical results. Korean J. Anesthesiol. 2019, 72, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Brannick, M.; Collinearity. Regression. Available online: http://faculty.cas.usf.edu/mbrannick/regression/Collinearity.html (accessed on 24 August 2023).
- Vrieze, S.I. Model selection and psychological theory: A discussion of the differences between the Akaike information criterion (AIC) and the Bayesian information criterion (BIC). Psychol. Methods 2012, 17, 228–243. [Google Scholar] [CrossRef]
- Kalton, G.; Flores-Cervantes, I. Weighting Methods. J. Off. Stat. 2003, 19, 81–97. Available online: https://www.scb.se/contentassets/ca21efb41fee47d293bbee5bf7be7fb3/weighting-methods.pdf (accessed on 24 August 2023).
- Sibhatu, K.T.; Qaim, M. Rural food security, subsistence agriculture, and seasonality. PLoS ONE 2017, 12, e0186406. [Google Scholar] [CrossRef]
- Giller, K.E.; Delaune, T.; Silva, J.V.; van Wijk, M.; Hammond, J.; Descheemaeker, K.; van de Ven, G.; Schut, A.G.; Taulya, G.; Chikowo, R.; et al. Small farms and development in sub-Saharan Africa: Farming for food, for income or for lack of better options? Food Secur. 2021, 13, 1431–1454. [Google Scholar] [CrossRef]
- Vyas, S.; Kumaranayake, L. Constructing socio-economic status indices: How to use principal components analysis. Health Policy Plan. 2006, 21, 459–468. [Google Scholar] [CrossRef]
- Armah, G.; Pringle, K.; Enweronu-Laryea, C.C.; Ansong, D.; Mwenda, J.M.; Diamenu, S.K.; Narh, C.; Lartey, B.; Binka, F.; Grytdal, S.; et al. Impact and Effectiveness of Monovalent Rotavirus Vaccine Against Severe Rotavirus Diarrhea in Ghana. Clin. Infect. Dis. 2016, 62, S200–S207. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, L.M.; Ashraf, S.; Fischer Walker, C.L.; Black, R.E. A Systematic Review of the Effect of Rotavirus Vaccination on Diarrhea Outcomes Among Children Younger Than 5 Years. Pediatr. Infect. Dis. J. 2016, 35, 992–998. [Google Scholar] [CrossRef] [PubMed]
- Malakalinga, J.J.; Misinzo, G.; Msalya, G.M.; Kazwala, R.R. Rotavirus Burden, Genetic Diversity and Impact in Children under Five in Tanzania. Pathogens 2019, 8, 210. [Google Scholar] [CrossRef] [PubMed]
- Guerrant, R.L.; Schorling, J.B.; McAuliffe, J.F.; De Souza, M.A. Diarrhea as a cause and an effect of malnutrition: Diarrhea prevents catch-up growth and malnutrition increases diarrhea frequency and duration. Am. J. Trop. Med. Hyg. 1992, 47 Pt 2, 28–35. [Google Scholar] [CrossRef]
- Mills, A. Health Care Systems in Low- and Middle-Income Countries. N. Engl. J. Med. 2014, 370, 552–557. [Google Scholar] [CrossRef] [PubMed]
- United Nations Sustainable Development. Goal 6: Ensure Access to Water and Sanitation for All. Sustainable Development Goals. Available online: https://www.un.org/sustainabledevelopment/water-and-sanitation/ (accessed on 24 August 2023).
- United Nations Secretary-General’s Special Advocate for Inclusive Finance for Development (UNSGSA). Investing in Digital Financial Infrastructure Key to Secure More Financial Inclusion Gains in Tanzania. Country Visits. 2022. Available online: https://www.unsgsa.org/country-visits/investing-digital-financial-infrastructure-key-secure-more-financial-inclusion-gains-tanzania (accessed on 24 August 2023).

{kind=link}
{kind=link}
{kind=link}
| Characteristics | No Basic WaSH a Status b n = 419 | At Least one Basic WaSH Status n = 204 |
|---|---|---|
| Sick c, (Yes), N (%) | 95 (22.67) | 42 (20.59) |
| Education of the mother d (completed primary), N (%) | 185 (44.15) | 100 (49.02) |
| Vaccination e (Yes), N (%) | 345 (82.34) | 163 (79.90) |
| Food insecurity f (Moderate or severe), N (%) | 214 (51.07) | 65 (31.86) |
| Income g (Income-generating), N (%) | 64 (15.27) | 21(10.29) |
| Wealth h, N (%) | ||
| Poor | 202 (48.21) | 39 (19.12) |
| Middle | 140 (33.41) | 90 (44.12) |
| Rich | 57 (13.60) | 62 (30.39) |
| Sex, Male, N (%) | 211 (50.36) | 108 (52.94) |
| Hamlet i, N (%) | ||
| Katoma Center | 119 (28.40) | 58(28.43) |
| Mataho | 91 (21.71) | 36 (17.65) |
| Chang’ombe | 143 (34.13) | 74 (36.27) |
| isoji | 44 (10.50) | 27 (13.24) |
| Ruchiri | 22 (5.25) | 9 (4.41) |
| Characteristics | Model I | Model II | Model III | Model IV |
|---|---|---|---|---|
| OR (95% CI) p-Value | OR (95% CI) p-Value | OR (95% CI) p-Value | OR (95% CI) p-Value | |
| WaSH | ||||
| No basic services | Reference | Reference | Reference | Reference |
| At least one basic service | 2.04 (1.05, 3.98) 0.036 * | 1.34 (0.68, 2.67) 0.397 | 1.5 (0.93, 2.64) 0.090 | 1.9 (0.66, 2.166) 0.558 |
| Food insecurity | ||||
| Mild or none | 1.25 (0.61, 2.59) 0.538 | 1.32 (0.73, 2.37) 0.354 | ||
| Moderate or severe | Reference | Reference | ||
| Education of the mother | ||||
| Did not complete primary | Reference | Reference | ||
| Completed primary | 1.72 (0.91, 3.25) 0.095 | 1.54 (0.94, 2.52) 0.089 | ||
| Vaccination card | ||||
| No | Reference | Reference | ||
| Yes | 0.67 (0.30, 1.50) 0.331 | 0.46 (0.20, 1.04) 0.063 | ||
| Income | ||||
| Sustenance | Reference | Reference | ||
| Income-generating | 1.13 (0.49, 2.65) 0.771 | 1.00 (0.50, 1.99) 0.997 | ||
| Hamlet | ||||
| Katoma Center | Reference | Reference | ||
| Mataho | 0.41 (0.17, 1.01) 0.053 | 0.51 (0.26, 1.01) 0.053 | ||
| Chang’ombe | 0.51 (0.24, 1.10) 0.084 | 0.60 (0.33, 1.08) 0.083 | ||
| Kisoji | 0.64 (0.23, 1.84) 0.411 | 0.94 (0.40, 2.22) 0.889 | ||
| Ruchiri | 0.07 (0.01, 0.65) 0.012 * | 0.09 (0.02, 0.37) 0.001 * |
| Characteristics | Model II | Model IV |
|---|---|---|
| OR (95% CI), p-Value | OR (95% CI), p-Value | |
| WaSH | ||
| No basic services | Reference | Reference |
| At least one basic service | 1.46 (0.70, 3. 04), 0.306 | 1.13 (0.62, 2.06), 0.696 |
| Food insecurity | ||
| Mild or none | 1.16 (0.52, 2.59), 0.708 | 1.21 (0.66, 2.21), 0.543 |
| Moderate or severe | Reference | Reference |
| Education of the mother | ||
| Did not complete primary | Reference | Reference |
| Completed primary | 1.58 (0.80, 3.10), 0.187 | 1.34 (0.79, 2.27), 0.281 |
| Vaccination card | ||
| No | Reference | Reference |
| Yes | 0.70 (0.30, 1.61), 0.398 | 0.50 (0.22, 1.12), 0.089 |
| Wealth | ||
| Poor | Reference | Reference |
| Middle | 1.64 (0.75, 3.59), 0.218 | 1.80 (1.00, 3.25), 0.051 |
| Rich | 1.05 (0.40, 2.77), 0.916 | 1.24 (0.60, 2.60), 0.560 |
| Hamlet | ||
| Katoma Center | Reference | Reference |
| Mataho | 0.38 (0.15, 0.96), 0.041 * | 0.50 (0.25, 1.00), 0.049 * |
| Chang’ombe | 0.49 (0.22, 1.07), 0.074 | 0.60 (0.33, 1.09), 0.094 |
| Kisoji | 0.71 (0.23, 2.19), 0.547 | 1.23 (0.47, 3.17), 0.673 |
| Ruchiri | 0.06 (0.01, 0.71), 0.026 * | 0.08 (0.02, 0.34), 0.001 * |
| Characteristics | Model II | Model IV |
|---|---|---|
| OR (95% CI), p-Value | OR (95% CI), p-Value | |
| WaSH | ||
| No basic services | Reference | Reference |
| At least one basic service | 121 (0.56, 260), 0.631 | 0.94 (0.48, 1.82), 0.850 |
| At least two basic services | 1.53 (0.45, 5.16), 0.493 | 2.52 (0.71, 8.97) 0.512 |
| Food insecurity | ||
| Mild or none | 2.42 (1.03, 5.67), 0.042 * | 1.99 (0.97, 4.09), 0.060 |
| Moderate or severe | Reference | Reference |
| Education of the mother | ||
| Did not complete primary | Reference | Reference |
| Completed primary | 3.26 (1.29, 8.25), 0.013 * | 2.24 (1.10, 4.59), 0.027 * |
| Vaccination card | ||
| No | Reference | Reference |
| Yes | 0.53 (0.22, 1.28), 0.159 | 0.30 (0.10, 0.92), 0.036 * |
| Income | ||
| Sustenance | Reference | Reference |
| Income-generating | 1.57 (0.59, 4.19), 0.363 | 1.16 (0.57, 2.36), 0.683 |
| Hamlet | ||
| Katoma Center | Reference | Reference |
| Mataho | 1.83 (0.48, 7.05), 0.376 | 1.38 (0.44, 4.30), 0.581 |
| Chang’ombe | 1.33 (0.37, 4.85), 0.662 | 1.29 (0.40, 4.09), 0.669 |
| Kisoji | 1.75 (0.48, 6.33), 0.391 | 2.24 (0.76, 6.58), 0.143 |
| Ruchiri | 0.21 (0.02, 2.59), 0.224 | 0.23 (0.04, 1.22), 0.085 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kilungo, A.; Bayer, M.; Baccam, Z.; Malebo, H.; Alaofe, H. Empowering Women, Enhancing Health: The Role of Education in Water, Sanitation, and Hygiene (WaSH) and Child Health Outcomes. Int. J. Environ. Res. Public Health 2025, 22, 706. https://doi.org/10.3390/ijerph22050706
Kilungo A, Bayer M, Baccam Z, Malebo H, Alaofe H. Empowering Women, Enhancing Health: The Role of Education in Water, Sanitation, and Hygiene (WaSH) and Child Health Outcomes. International Journal of Environmental Research and Public Health. 2025; 22(5):706. https://doi.org/10.3390/ijerph22050706
Chicago/Turabian StyleKilungo, Aminata, Mark Bayer, Zoe Baccam, Hamisi Malebo, and Halima Alaofe. 2025. "Empowering Women, Enhancing Health: The Role of Education in Water, Sanitation, and Hygiene (WaSH) and Child Health Outcomes" International Journal of Environmental Research and Public Health 22, no. 5: 706. https://doi.org/10.3390/ijerph22050706
APA StyleKilungo, A., Bayer, M., Baccam, Z., Malebo, H., & Alaofe, H. (2025). Empowering Women, Enhancing Health: The Role of Education in Water, Sanitation, and Hygiene (WaSH) and Child Health Outcomes. International Journal of Environmental Research and Public Health, 22(5), 706. https://doi.org/10.3390/ijerph22050706