



Health Risk Assessment of Exposure to Air Pollutants Exceeding the New WHO Air Quality Guidelines (AQGs) in São Paulo, Brazil


 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
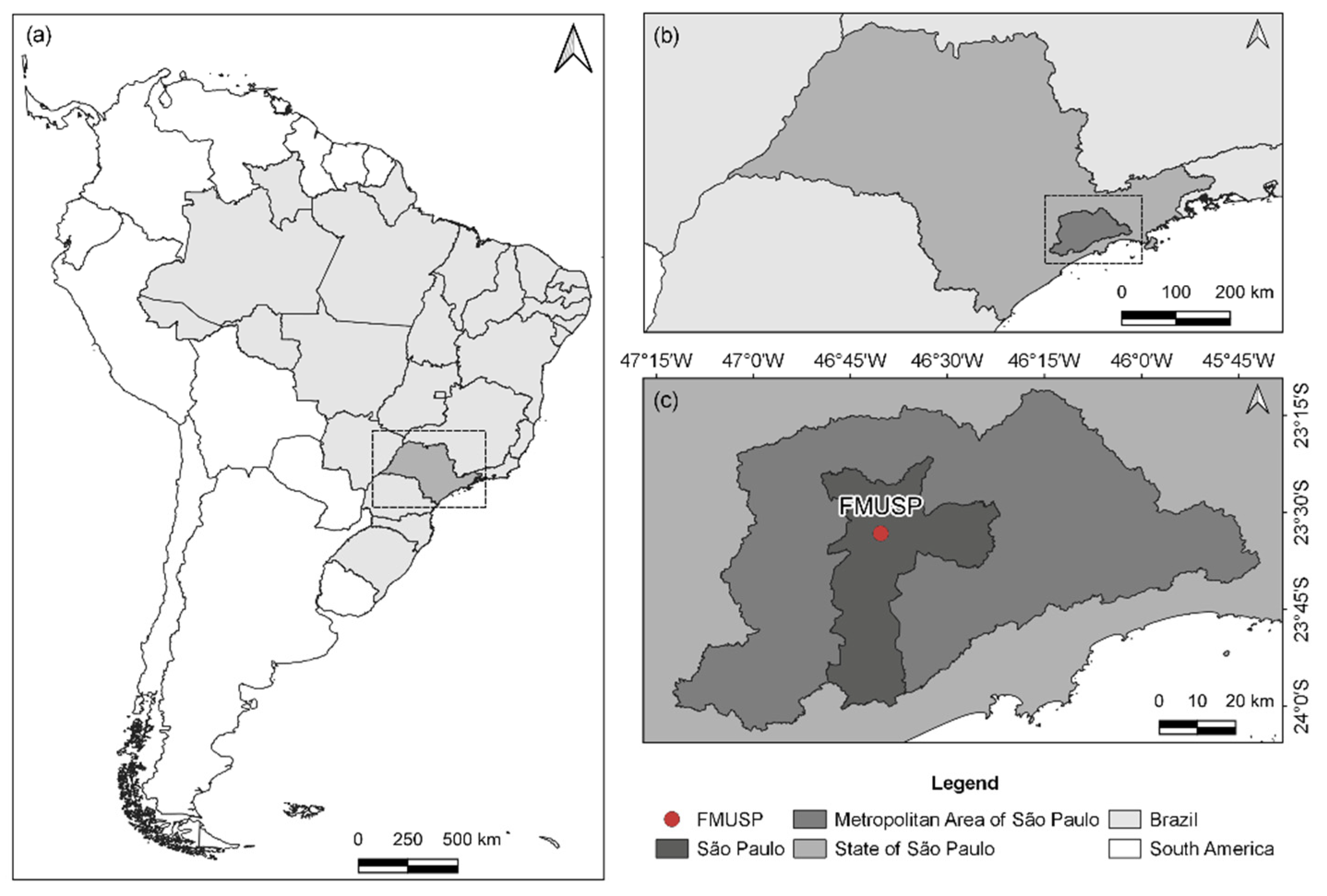
2.1. Study Site
2.2. Data Sampling and Analysis
3. Results and Discussion
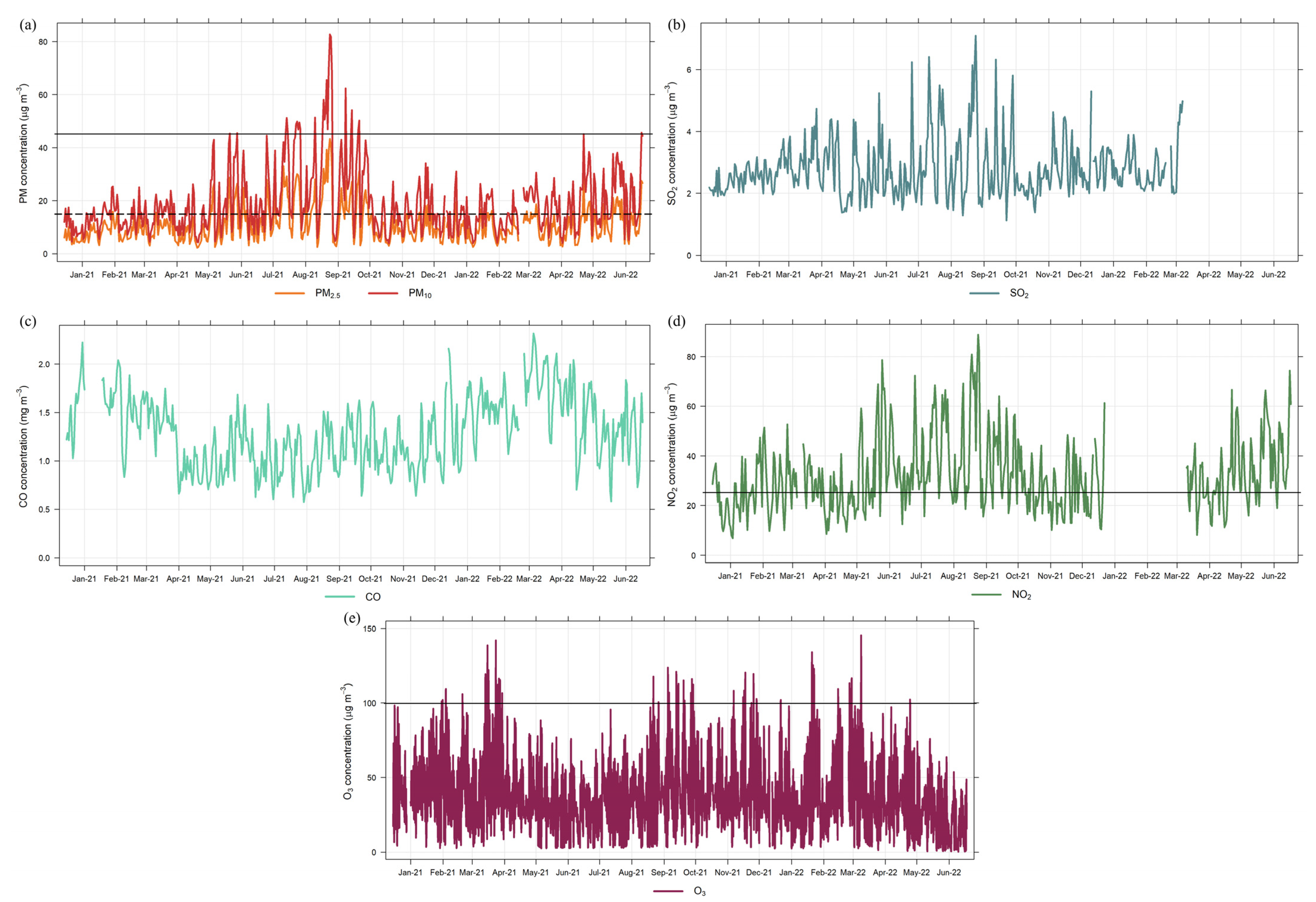
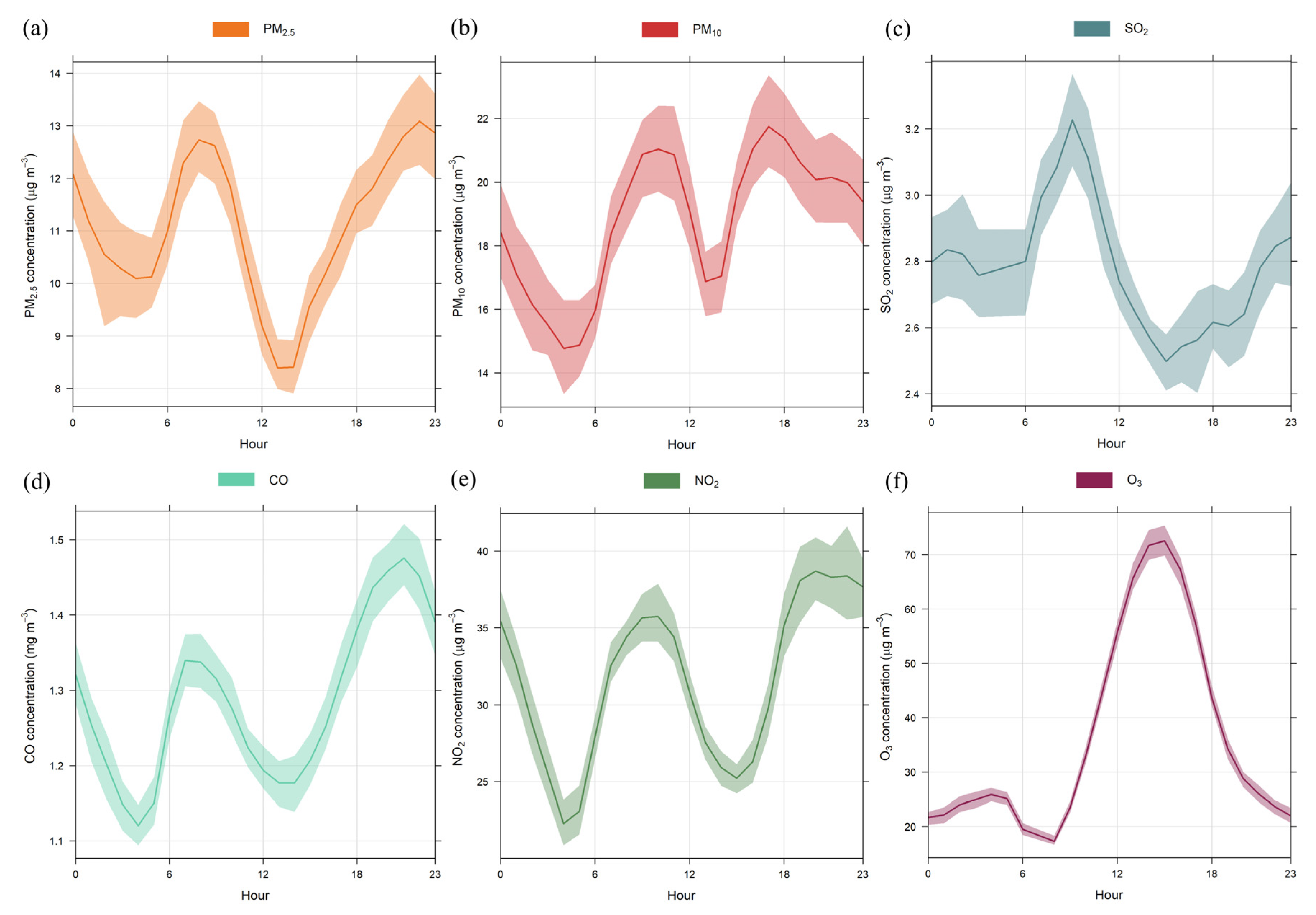
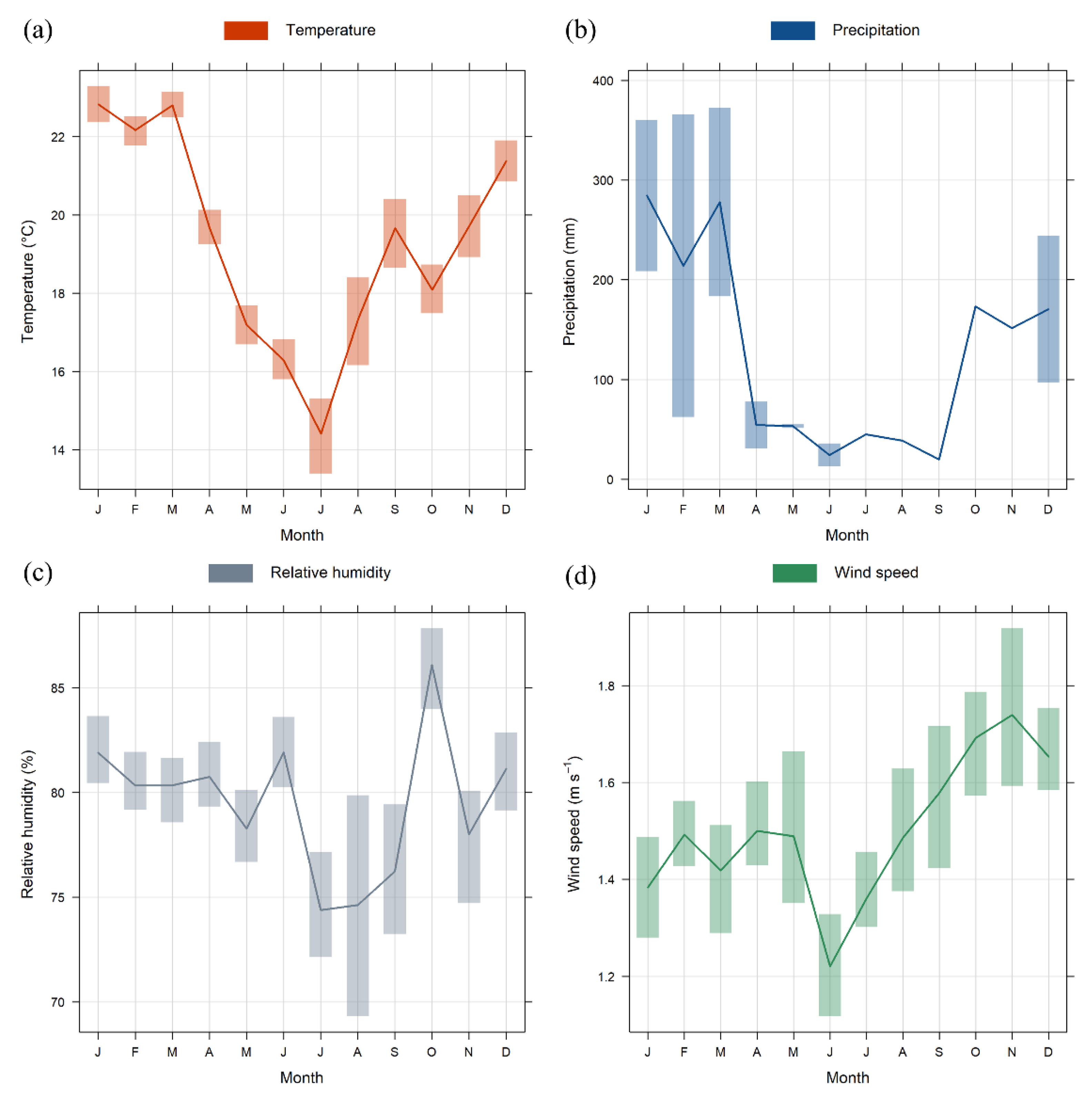
3.1. Pollutant Concentrations and Meteorological Variables Overview
3.2. Health Risk Assessment
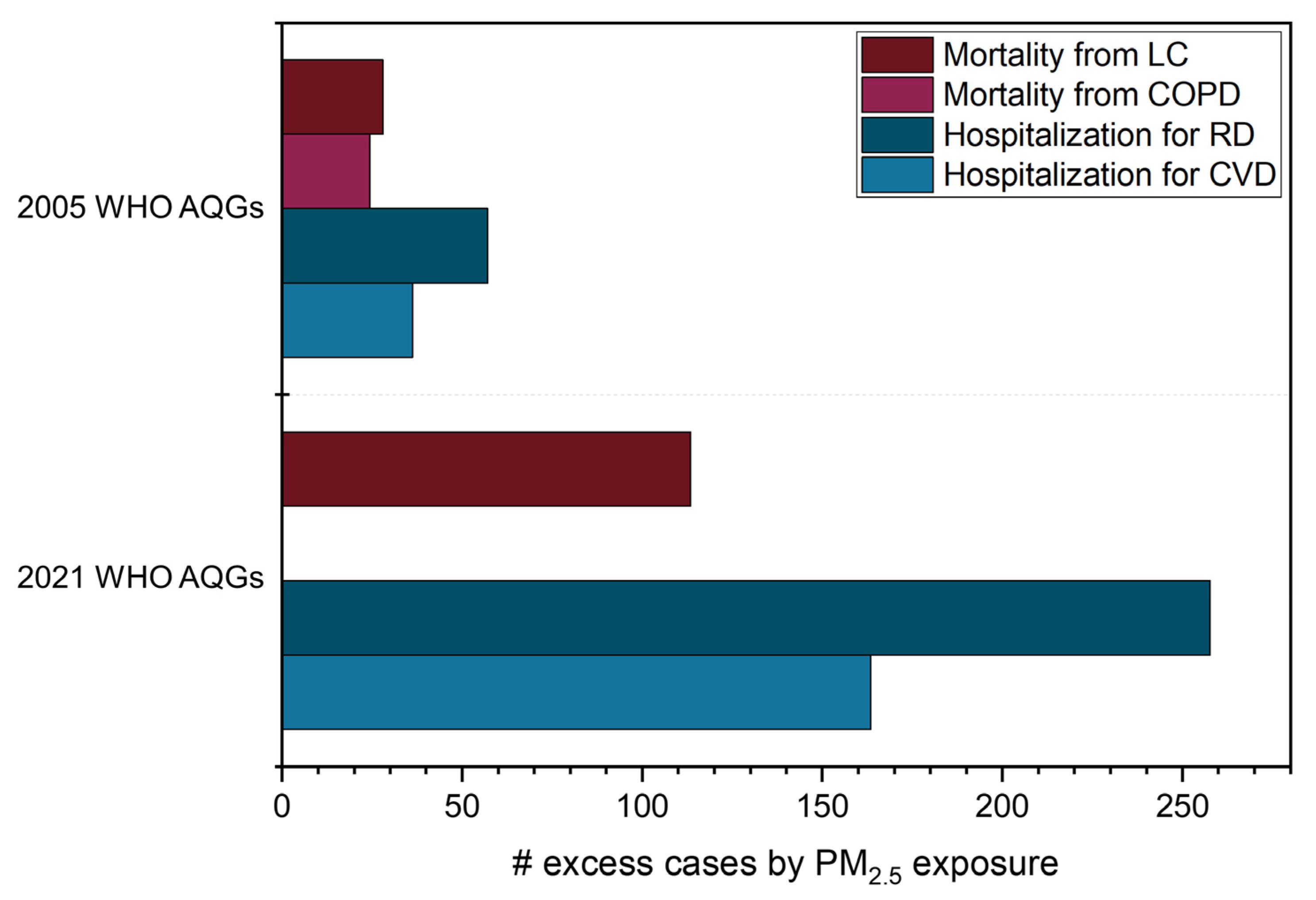
3.2.1. Outcomes from PM2.5 Exposure
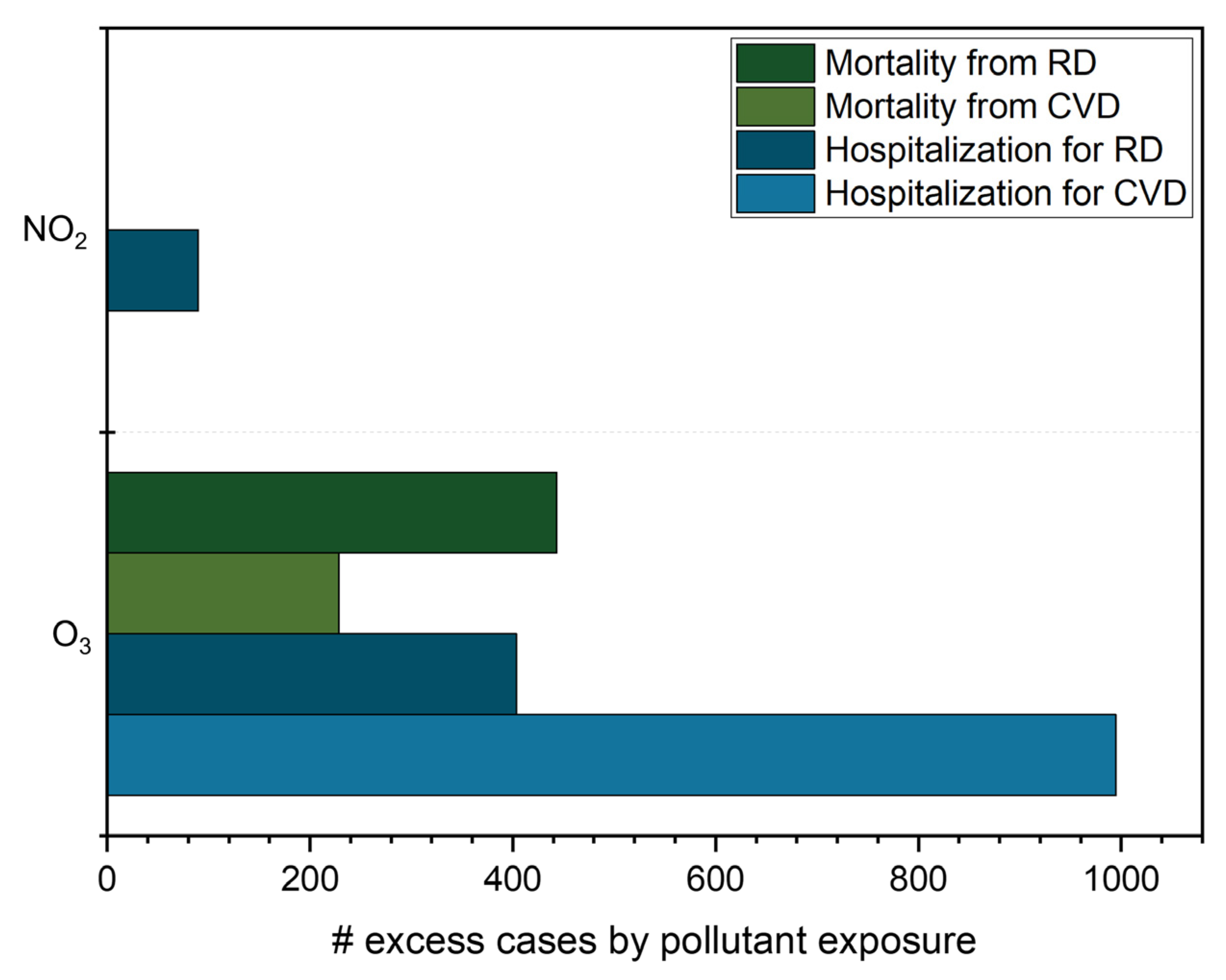
3.2.2. Outcomes from O3 and NO2 Exposure
3.2.3. Discussion of Health Outcomes Results
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-Year Trends of the Global Burden of Disease Attributable to Ambient Air Pollution: An Analysis of Data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ambient (Outdoor) Air Pollution. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 15 August 2022).
- Health Effects Institute (HEI). State of Global Air 2020; HEI: Boston, MA, USA, 2020. [Google Scholar]
- Murray, C.J.L.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; Abegaz, K.H.; Abolhassani, H.; et al. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Landrigan, P.J. Pollution and the Heart. N. Engl. J. Med. 2021, 385, 1881–1892. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Vohra, K.; Vodonos, A.; Schwartz, J.; Marais, E.A.; Sulprizio, M.P.; Mickley, L.J. Global Mortality from Outdoor Fine Particle Pollution Generated by Fossil Fuel Combustion: Results from GEOS-Chem. Environ. Res. 2021, 195, 110754. [Google Scholar] [CrossRef]
- Pope, C.A., III; Coleman, N.; Pond, Z.A.; Burnett, R.T. Fine Particulate Air Pollution and Human Mortality: 25+ Years of Cohort Studies. Environ. Res. 2020, 183, 108924. [Google Scholar] [CrossRef]
- Sokhi, R.S.; Moussiopoulos, N.; Baklanov, A.; Bartzis, J.; Coll, I.; Finardi, S.; Friedrich, R.; Geels, C.; Grönholm, T.; Halenka, T.; et al. Advances in Air Quality Research—Current and Emerging Challenges. Atmos. Chem. Phys. 2022, 22, 4615–4703. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021.
- World Health Organization (WHO). Air Pollution Data Portal. Available online: https://www.who.int/data/gho/data/themes/air-pollution (accessed on 15 August 2022).
- Nogueira, T.; Kamigauti, L.Y.; Pereira, G.M.; Gavidia-Calderón, M.E.; Ibarra-Espinosa, S.; De Oliveira, G.L.; De Miranda, R.M.; Vasconcellos, P.D.C.; Freitas, E.D.; Andrade, M.F. Evolution of Vehicle Emission Factors in a Megacity Affected by Extensive Biofuel Use: Results of Tunnel Measurements in São Paulo, Brazil. Environ. Sci. Technol. 2021, 55, 6677–6687. [Google Scholar] [CrossRef]
- Andrade, M.F.; Kumar, P.; Freitas, E.D.; Ynoue, R.Y.; Martins, J.; Martins, L.D.; Nogueira, T.; Perez-Martinez, P.; De Miranda, R.M.; Albuquerque, T.; et al. Air Quality in the Megacity of São Paulo: Evolution over the Last 30 Years and Future Perspectives. Atmos. Environ. 2017, 159, 66–82. [Google Scholar] [CrossRef]
- Miraglia, S.G.E.K.; Saldiva, P.H.N.; Böhm, G.M. An Evaluation of Air Pollution Health Impacts and Costs in São Paulo, Brazil. Environ. Manag. 2005, 35, 667–676. [Google Scholar] [CrossRef]
- Abe, K.C.; Miraglia, S.G.E.K. Health Impact Assessment of Air Pollution in São Paulo, Brazil. Int. J. Environ. Res. Public Health 2016, 13, 694. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Health Impact Assessment of Air Pollution: Introductory Manual to AirQ+; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- United Nations. The Sustainable Development Goals Report 2022; United Nations: New York, NY, USA, 2022.
- Brazilian Institute of Geography and Statistics (IBGE). São Paulo. Available online: https://cidades.ibge.gov.br/brasil/sp/sao-paulo/panorama (accessed on 1 September 2022).
- Brazilian Institute of Geography and Statistics (IBGE). Produto Interno Bruto Dos Municípios: São Paulo. Available online: https://cidades.ibge.gov.br/brasil/sp/sao-paulo/pesquisa/38/47001?tipo=ranking&indicador=46997 (accessed on 1 September 2022).
- Brazilian Institute of Geography and Statistics (IBGE). Produto Interno Bruto Dos Municípios: PIB por Município. Available online: https://www.ibge.gov.br/estatisticas/economicas/contas-nacionais/9088-produto-interno-bruto-dos-municipios.html?t=o-que-e&c=3550308 (accessed on 1 September 2022).
- IAG-USP. Estação Meteorológica Do IAG/USP. Available online: http://estacao.iag.usp.br/seasons/index.php# (accessed on 30 March 2020).
- De Almeida Albuquerque, T.T.; Andrade, M.F.; Ynoue, R.Y. Characterization of Atmospheric Aerosols in the City of São Paulo, Brazil: Comparisons between Polluted and Unpolluted Periods. Environ. Monit. Assess. 2012, 184, 969–984. [Google Scholar] [CrossRef]
- Environmental Company of the State of São Paulo (CETESB). Qualidade Do Ar No Estado de São Paulo 2020; Companhia Ambiental do Estado de São Paulo: São Paulo, Brasil, 2021. [Google Scholar]
- Brazilian Institute of Geography and Statistics (IBGE). Frota de Veículos. Available online: https://cidades.ibge.gov.br/brasil/sp/pesquisa/22/28120?localidade1=355030 (accessed on 1 September 2022).
- Squizzato, R.; Nogueira, T.; Martins, L.D.; Martins, J.A.; Astolfo, R.; Machado, C.B.; Andrade, M.F.; Freitas, E.D. Beyond Megacities: Tracking Air Pollution from Urban Areas and Biomass Burning in Brazil. Clim. Atmos. Sci. 2021, 4, 17. [Google Scholar] [CrossRef]
- Carslaw, D.C.; Ropkins, K. Openair—An R Package for Air Quality Data Analysis. Environ. Model. Softw. 2012, 27–28, 52–61. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2021. [Google Scholar]
- World Health Organization (WHO). AirQ+: Key Features; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Brazilian Ministry of Health Informações de Saúde. TABNET. Available online: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/ (accessed on 15 September 2022).
- World Health Organization (WHO). Air Quality Guidelines: Global Update 2005; WHO Regional Office for Europe: Copenhagen, Denmark, 2006. [Google Scholar]
- Fallahizadeh, S.; Kermani, M.; Esrafili, A.; Asadgol, Z.; Gholami, M. The Effects of Meteorological Parameters on PM10: Health Impacts Assessment Using AirQ+ Model and Prediction by an Artificial Neural Network (ANN). Urban Clim. 2021, 38, 100905. [Google Scholar] [CrossRef]
- Hadei, M.; Nazari, S.S.H.; Eslami, A.; Khosravi, A.; Yarahmadi, M.; Naghdali, Z.; Shahsavani, A. Distribution and Number of Ischemic Heart Disease (IHD) and Stroke Deaths Due to Chronic Exposure to PM2.5 in 10 Cities of Iran (2013–2015); An AirQ+ Modelling. J. Air Pollut. Health 2017, 2, 129–136. [Google Scholar]
- Carvalho, V.S.B.; Freitas, E.D.; Martins, L.D.; Martins, J.A.; Mazzoli, C.R.; Andrade, M.F. Air Quality Status and Trends over the Metropolitan Area of São Paulo, Brazil as a Result of Emission Control Policies. Environ. Sci. Policy 2015, 47, 68–79. [Google Scholar] [CrossRef]
- Brazilian National Environmental Council Resolução CONAMA N° 491, de 19 de novembro de 2018. Dispõe sobre Padrões de Qualidade do Ar; Diário Oficial da União: Brasília, Brasil, 2018; pp. 155–156. [Google Scholar]
- Brazilian National Environmental Council Resolução CONAMA N° 18, de 6 de maio de 1986. Dispõe sobre a Criação Do Programa de Controle de Poluição do Ar Por Veículos Automotores—PROCONVE; Diário Oficial da União: Brasília, Brazil, 1986; pp. 8792–8795. [Google Scholar]
- Brazililian National Environmental Council Resolução CONAMA N° 297, de 26 de fevereiro de 2002. Estabelece Os Limites Para Emissões de Gases Poluentes por Ciclomotores, Motociclos e Veículos Similares Novos; Diário Oficial da União: Brasília, Brazil, 2002; pp. 86–88. [Google Scholar]
- Seinfeld, J.H.; Pandis, S.N. Atmospheric Chemistry and Physics: From Air Pollution to Climate Change, 3rd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2016. [Google Scholar]
- Massambani, O.; Andrade, M.F. Seasonal Behavior of Tropospheric Ozone in the Sao Paulo (Brazil) Metropolitan Area. Atmos. Environ. 1994, 28, 3165–3169. [Google Scholar] [CrossRef]
- Andrade, M.F.; Fornaro, A.; Freitas, E.D.; Mazzoli, C.R.; Martins, L.D.; Boian, C.; Oliveira, M.G.L.; Peres, J.; Carbone, S.; Alvalá, P.; et al. Ozone Sounding in the Metropolitan Area of São Paulo, Brazil: Wet and Dry Season Campaigns of 2006. Atmos. Environ. 2012, 61, 627–640. [Google Scholar] [CrossRef]
- Traffic Engineering Company of São Paulo (CET). Especial COVID-19. Available online: http://www.cetsp.com.br/consultas/especial-covid-19.aspx (accessed on 20 July 2022).
- Alvim, D.S.; Gatti, L.V.; Corrêa, S.M.; Chiquetto, J.B.; Santos, G.M.; De Souza Rossatti, C.; Pretto, A.; Rozante, J.R.; Figueroa, S.N.; Pendharkar, J.; et al. Determining VOCs Reactivity for Ozone Forming Potential in the Megacity of São Paulo. Aerosol Air Qual. Res. 2018, 18, 2460–2474. [Google Scholar] [CrossRef]
- Schuch, D.; Freitas, E.D.; Espinosa, S.I.; Martins, L.D.; Carvalho, V.S.B.; Ramin, B.F.; Silva, J.S.; Martins, J.A.; Andrade, M.F. A Two Decades Study on Ozone Variability and Trend over the Main Urban Areas of the São Paulo State, Brazil. Environ. Sci. Pollut. Res. 2019, 26, 31699–31716. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Health Risks of Ozone from Long-Range Transboundary Air Pollution; WHO Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- Foster, W.M.; Freed, A.N. Regional Clearance of Solute from Peripheral Airway Epithelia: Recovery after Sublobar Exposure to Ozone. J. Appl. Physiol. 1999, 86, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Gryparis, A.; Forsberg, B.; Katsouyanni, K.; Analitis, A.; Touloumi, G.; Schwartz, J.; Samoli, E.; Medina, S.; Anderson, H.R.; Niciu, E.M.; et al. Acute Effects of Ozone on Mortality from the “Air Pollution and Health: A European Approach” Project. Am. J. Respir. Crit. Care Med. 2004, 170, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Yin, P.; Meng, X.; Wang, L.; Liu, C.; Niu, Y.; Lin, Z.; Liu, Y.; Liu, J.; Qi, J.; et al. Associations between Ambient Nitrogen Dioxide and Daily Cause-Specific Mortality: Evidence from 272 Chinese Cities. Epidemiology 2018, 29, 482–489. [Google Scholar] [CrossRef]
- He, M.Z.; Kinney, P.L.; Li, T.; Chen, C.; Sun, Q.; Ban, J.; Wang, J.; Liu, S.; Goldsmith, J.; Kioumourtzoglou, M.-A. Short- and Intermediate-Term Exposure to NO2 and Mortality: A Multi-County Analysis in China. Environ. Pollut. 2020, 261, 114165. [Google Scholar] [CrossRef]
- Hvidtfeldt, U.A.; Sørensen, M.; Geels, C.; Ketzel, M.; Khan, J.; Tjønneland, A.; Overvad, K.; Brandt, J.; Raaschou-Nielsen, O. Long-Term Residential Exposure to PM2.5, PM10, Black Carbon, NO2, and Ozone and Mortality in a Danish Cohort. Environ. Int. 2019, 123, 265–272. [Google Scholar] [CrossRef]
- Zhao, S.; Liu, S.; Sun, Y.; Liu, Y.; Beazley, R.; Hou, X. Assessing NO2-Related Health Effects by Non-Linear and Linear Methods on a National Level. Sci. Total Environ. 2020, 744, 140909. [Google Scholar] [CrossRef]
- Kliengchuay, W.; Srimanus, W.; Srimanus, R.; Kiangkoo, N.; Moonsri, K.; Niampradit, S.; Suwanmanee, S.; Tantrakarnapa, K. The Association of Meteorological Parameters and AirQ+ Health Risk Assessment of PM2.5 in Ratchaburi Province, Thailand. Sci. Rep. 2022, 12, 12971. [Google Scholar] [CrossRef]
- Mirzaei, A.; Tahriri, H.; Khorsandi, B. Comparison between AirQ+ and BenMAP-CE in Estimating the Health Benefits of PM2.5 Reduction. Air Qual. Atmos. Health 2021, 14, 807–815. [Google Scholar] [CrossRef]
- Naghan, D.J.; Neisi, A.; Goudarzi, G.; Dastoorpoor, M.; Fadaei, A.; Angali, K.A. Estimation of the Effects PM2.5, NO2, O3 Pollutants on the Health of Shahrekord Residents Based on AirQ+ Software during (2012–2018). Toxicol. Rep. 2022, 9, 842–847. [Google Scholar] [CrossRef]
- Rovira, J.; Domingo, J.L.; Schuhmacher, M. Air Quality, Health Impacts and Burden of Disease Due to Air Pollution (PM10, PM2.5, NO2 and O3): Application of AirQ+ Model to the Camp de Tarragona County (Catalonia, Spain). Sci. Total Environ. 2020, 703, 135538. [Google Scholar] [CrossRef]
- Sacks, J.D.; Fann, N.; Gumy, S.; Kim, I.; Ruggeri, G.; Mudu, P. Quantifying the Public Health Benefits of Reducing Air Pollution: Critically Assessing the Features and Capabilities of WHO’s AirQ+ and U.S. EPA’s Environmental Benefits Mapping and Analysis Program—Community Edition (BenMAP—CE). Atmosphere 2020, 11, 516. [Google Scholar] [CrossRef]
- Brazilian Ministry of Health. Painel Coronavírus. Available online: https://covid.saude.gov.br/ (accessed on 10 April 2023).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Equipment. | Parameter | Model | Manufacturer | Unit |
|---|---|---|---|---|
| TEOM Continuous Ambient Particulate Monitor | PM2.5, PM10 | 1405 | Thermo Fisher Scientific | µg m−3 |
| SO2 Analyzer | SO2 | 43i | Thermo Fisher Scientific | µg m−3 |
| Photoacoustic Gas Monitor | CO | Innova 1512 | LumaSense Technologies | mg m−3 |
| NOx Analyzer | NO2 | 42i | Thermo Fisher Scientific | µg m−3 |
| O3 Analyzer | O3 | 49i | Thermo Fisher Scientific | µg m−3 |
| Pollutant | Overall Mean | 2021 Mean | 2022 Mean |
|---|---|---|---|
| PM2.5 (µg m−3) | 11.1 (±6.8) | 11.6 (±7.4) | 10.5 (±5.3) |
| PM10 (µg m−3) | 18.8 (±12.1) | 19.5 (±13.3) | 18.0 (±9.1) |
| SO2 (µg m−3) | 2.8 (±1.0) | 2.8 (±1.0) | 2.9 (±1.0) |
| CO (mg m−3) | 0.7 (±0.5) | 1.2 (±0.4) | 1.5 (± 0.4) |
| NO2 (µg m−3) | 32.2 (±15.0) | 32.2 (±15.4) | 33.8 (±13.9) |
| O3 (µg m−3) | 36.6 (±22.2) | 37.9 (±21.8) | 33.2 (±22.9) |
| Pollutant | Averaging Time | WHO | CONAMA | |
|---|---|---|---|---|
| PM2.5 | (μg m−3) | Annual | 5 | 20 |
| 24-h | 15 | 60 | ||
| PM10 | Annual | 15 | 40 | |
| 24-h | 45 | 120 | ||
| SO2 | 24-h | 40 | 125 | |
| CO | (mg m−3) | 4 | - | |
| (ppm) | 8-h | 9 | 9 | |
| NO2 | (μg m−3) | Annual | 10 | 60 |
| 24-h | 25 | - | ||
| 1-h | 200 | 260 | ||
| O3 | 8-h | 100 | 140 | |
| Health Endpoint | Timeframe | Age | 2005 WHO AQG | 2021 WHO AQG | ||||
|---|---|---|---|---|---|---|---|---|
| RR | B + c | N + c | RR | B + c | N + c | |||
| Mortality from LC | Long-term | 30+ | 1.0138 (1.0062–1.0210) | 0.46 (0.21–0.70) | 27.93 (12.76–42.32) | 1.0584 (1.0262–1.0902) | 1.89 (0.87–2.83) | 113.41 (52.42–169.94) |
| Mortality from COPD | 25+ | 1.0166 (1.0087–1.0258) | 0.34 (0.18–0.53) | 24.37 (12.93–37.53) | - | - | - | |
| Hospital admissions for RD | Short-term | Total population | 1.0008 (1.0000–1.0016) | 0.51 (0.00–1.07) | 57.07 (0.00–120.61) | 1.0034 (1.0000–1.0073) | 2.29 (0.00–4.84) | 257.65 (0.00–544.74) |
| Hospital admissions for CVD | 1.0004 (1.0001–1.0007) | 0.32 (0.06–0.59) | 36.20 (6.77–66.03) | 1.0017 (1.0003–1.0030) | 1.45 (0.27–2.65) | 163.42 (30.54–298.01) | ||
| Timeframe | Age | IHD | Stroke | ||||
|---|---|---|---|---|---|---|---|
| RR | B + c | N + c | RR | B + c | N + c | ||
| Long-term | 25–29 | 1.0220 (1.0122–1.0453) | 0.04 (0.02–0.08) | 0.43 (0.24–0.87) | 1.0174 (1.0075–1.0274) | 0.00 (0.00–0.01) | 0.05 (0.02–0.08) |
| 30–34 | 1.0200 (1.0112–1.0418) | 0.04 (0.02–0.08) | 0.39 (0.22–0.80) | 1.0162 (1.0076–1.0262) | 0.02 (0.01–0.04) | 0.24 (0.11–0.38) | |
| 35–39 | 1.0185 (1.0100–1.0365) | 0.04 (0.02–0.08) | 0.36 (0.20–0.70) | 1.0153 (1.0074–1.0249) | 0.03 (0.01–0.04) | 0.23 (0.11–0.37) | |
| 40–44 | 1.0173 (1.0093–1.0377) | 0.16 (0.09–0.35) | 1.33 (0.72–2.83) | 1.0140 (1.0064–1.0231) | 0.09 (0.04–0.15) | 0.75 (0.34–1.22) | |
| 45–49 | 1.0159 (1.0088–1.0330) | 0.16 (0.09–0.34) | 1.22 (0.68–2.49) | 1.0131 (1.0064–1.0211) | 0.09 (0.05–0.15) | 0.70 (0.34–1.12) | |
| 50–54 | 1.0142 (1.0075–1.0298) | 0.37 (0.20–0.76) | 2.45 (1.31–5.07) | 1.0119 (1.0055–1.0190) | 0.25 (0.12–0.40) | 1.68 (0.79–2.67) | |
| 55–59 | 1.0128 (1.0073–1.0262) | 0.40 (0.23–0.81) | 2.21 (1.27–4.46) | 1.0108 (1.0053–1.0178) | 0.28 (0.14–0.46) | 1.53 (0.76–2.51) | |
| 60–64 | 1.0115 (1.0064–1.0233) | 0.86 (0.48–1.73) | 3.65 (2.03–7.32) | 1.0097 (1.0048–1.0160) | 0.62 (0.31–1.02) | 2.61 (1.30–4.30) | |
| 65–69 | 1.0102 (1.0058–1.0205) | 1.07 (0.61–2.14) | 3.25 (1.84–6.46) | 1.0088 (1.0040–1.0145) | 0.79 (0.36–1.29) | 2.39 (1.08–3.90) | |
| 70–74 | 1.0090 (1.0051–1.0191) | 1.31 (0.74–2.75) | 3.11 (1.76–6.53) | 1.0078 (1.0038–1.0127) | 1.12 (0.55–1.83) | 2.67 (1.30–4.35) | |
| 75–79 | 1.0077 (1.0048–1.0158) | 1.56 (0.97–3.18) | 2.67 (1.65–5.44) | 1.0066 (1.0034–1.0111) | 1.33 (0.69–2.23) | 2.28 (1.18–3.81) | |
| 80–84 | 1.0065 (1.0038–1.0118) | 2.77 (1.65–5.01) | 3.31 (1.97–5.99) | 1.0057 (1.0027–1.0098) | 3.23 (1.53–5.53) | 3.86 (1.83–6.60) | |
| 85–89 | 1.0054 (1.0031–1.0103) | 4.83 (2.80–9.21) | 2.76 (1.60–5.27) | 1.0047 (1.0023–1.0078) | 5.58 (2.70–9.24) | 3.19 (1.54–5.29) | |
| 90–94 | 1.0043 (1.0026–1.0081) | 10.30 (6.33–19.52) | 2.19 (1.35–4.14) | 1.0038 (1.0018–1.0062) | 12.17 (5.81–19.58) | 2.58 (1.23–4.16) | |
| 95+ | 1.0031 (1.0019–1.0056) | 24.65 (14.88–44.00) | 1.61 (0.97–2.87) | 1.0028 (1.0013–1.0046) | 29.05 (13.59–47.15) | 1.90 (0.89–3.08) | |
| Health Endpoint | Timeframe | Age | RR | B + c | N + c |
|---|---|---|---|---|---|
| Mortality from RD | Long-term | Total population | 1.0290 (1.0103–1.0499) | 3.94 (1.43–6.65) | 443.23 (160.46–748.56) |
| Short-term | 1.0060 (1.0000–1.0144) | 0.83 (0.00–1.99) | 93.37 (0.00–223.97) | ||
| Hospital admissions for RD | 1.0090 (1.0014–1.0171) | 3.59 (0.57–6.73) | 403.58 (64.57–756.81) | ||
| Mortality from CVD | 1.0101 (1.0027–1.0175) | 2.03 (0.54–3.50) | 228.18 (60.87–393.67) | ||
| Hospital admissions for CVD | 1.0184 (1.0103–1.0263) | 8.84 (5.00–12.54) | 994.69 (562.13–1411.28) |
| Health Endpoint | Timeframe | Age | RR | B + c | N + c |
|---|---|---|---|---|---|
| Hospital admissions for RD | Short-term | Total population | 1.0020 (1.0013–1.0027) | 0.80 (0.51–1.08) | 89.61 (57.25–121.93) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wikuats, C.F.H.; Nogueira, T.; Squizzato, R.; de Freitas, E.D.; Andrade, M.d.F. Health Risk Assessment of Exposure to Air Pollutants Exceeding the New WHO Air Quality Guidelines (AQGs) in São Paulo, Brazil. Int. J. Environ. Res. Public Health 2023, 20, 5707. https://doi.org/10.3390/ijerph20095707
Wikuats CFH, Nogueira T, Squizzato R, de Freitas ED, Andrade MdF. Health Risk Assessment of Exposure to Air Pollutants Exceeding the New WHO Air Quality Guidelines (AQGs) in São Paulo, Brazil. International Journal of Environmental Research and Public Health. 2023; 20(9):5707. https://doi.org/10.3390/ijerph20095707
Chicago/Turabian StyleWikuats, Caroline Fernanda Hei, Thiago Nogueira, Rafaela Squizzato, Edmilson Dias de Freitas, and Maria de Fatima Andrade. 2023. "Health Risk Assessment of Exposure to Air Pollutants Exceeding the New WHO Air Quality Guidelines (AQGs) in São Paulo, Brazil" International Journal of Environmental Research and Public Health 20, no. 9: 5707. https://doi.org/10.3390/ijerph20095707
APA StyleWikuats, C. F. H., Nogueira, T., Squizzato, R., de Freitas, E. D., & Andrade, M. d. F. (2023). Health Risk Assessment of Exposure to Air Pollutants Exceeding the New WHO Air Quality Guidelines (AQGs) in São Paulo, Brazil. International Journal of Environmental Research and Public Health, 20(9), 5707. https://doi.org/10.3390/ijerph20095707