
Intrinsic Capacities, Functional Ability, Physiological Systems, and Caregiver Support: A Targeted Synthesis of Effective Interventions and International Recommendations for Older Adults

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Document Selection
3.2. Document Characteristics
3.2.1. Study Design
3.2.2. Participants and Settings
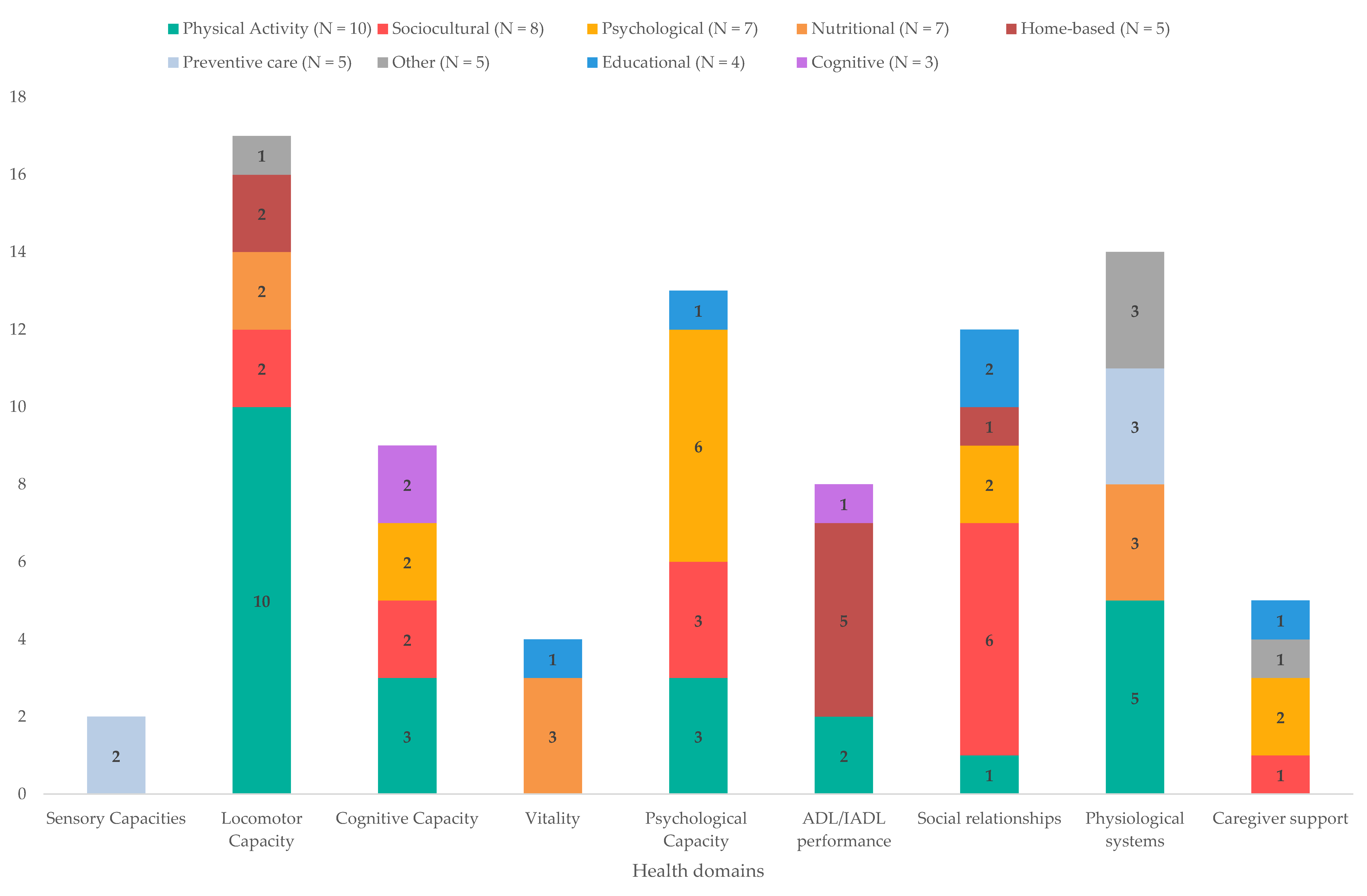
3.3. Summary and Classification of Identified Interventions
3.4. Interventions and Recommendations for Intrinsic Capacity
3.4.1. Sensory Capacities (Vision and Audition)
3.4.2. Locomotor Capacity
3.4.3. Cognitive Capacity
3.4.4. Vitality (Nutrition)
3.4.5. Psychological Capacity
3.5. Interventions and Recommendations for Functional Ability
3.5.1. Activities of Daily Living and Instrumental Activities of Daily Living
3.5.2. Social Relationships
3.6. Interventions and Recommendations for Physiological System Health
3.6.1. Behavioural Factors
3.6.2. Cardiovascular System
3.6.3. Osteoarticular System
3.6.4. Genitourinary System
3.6.5. Respiratory, Digestive, Renal, Lymphatic, and Immune Systems
3.7. Interventions for Caregiver Support
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations, Department of Economic and Social Affrairs Population Division. World Population Prospects 2019: Ten Key Findings; United Nations: New York, NY, USA, 2019; Available online: https://population.un.org/wpp/Publications/Files/WPP2019_10KeyFindings.pdf (accessed on 15 December 2022).
- Binette, J.; Vasold, K. Home and Community Preferences Survey: A National Survey of Adults Ages 18-Plus; AARP Research: Washington, DC, USA, 2018. [Google Scholar]
- van Leeuwen, K.M.; van Loon, M.S.; van Nes, F.A.; Bosmans, J.E.; de Vet, H.C.W.; Ket, J.C.F.; Widdershoven, G.A.M.; Ostelo, R. What does quality of life mean to older adults? A thematic synthesis. PLoS ONE 2019, 14, e0213263. [Google Scholar] [CrossRef] [PubMed]
- Roth, S.; Pellegrini, S. Virage Ambulatoire, Transfert ou Expansion de L'offre de Soins? Observatoire suisse de la santé: Neuchâtel, Switzerland, 2015; p. 68. [Google Scholar]
- Baltes, P.B.; Baltes, M.M. Successful Aging: Perspectives from the Behavorial Sciences; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar] [CrossRef]
- Araujo de Carvalho, I.; Epping-Jordan, J.; Pot, A.M.; Kelley, E.; Toro, N.; Thiyagarajan, J.A.; Beard, J.R. Organizing integrated health-care services to meet older people's needs. Bull. World Health Organ. 2017, 95, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U.; Morris, P.A. The Bioecological Model of Human Development. In Handbook of Child Psychology: Theoretical Models of Human Development, 6th ed.; Lerner, R.M., Damon, W., Eds.; John Wiley & Sons Inc: Hoboken, NJ, US, 2006; Volume 1, pp. 793–828. [Google Scholar]
- International Health Conference. Summary Report on Proceedings Minutes and Final Acts of the International Health Conference held in New York from 19 June to 22 July 1946; United Nations, World Health Organization, Interim Commission: Geneva, Switzerland, 1948; Available online: https://apps.who.int/iris/handle/10665/85573 (accessed on 1 December 2021).
- World Health Organization. World Report on Ageing; World Health Organization: Geneva, Switzerland, 2015; Available online: https://apps.who.int/iris/handle/10665/186463 (accessed on 1 December 2021).
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [PubMed]
- Håkansson Eklund, J.; Holmström, I.K.; Kumlin, T.; Kaminsky, E.; Skoglund, K.; Höglander, J.; Sundler, A.J.; Condén, E.; Summer Meranius, M. “Same same or different?” A review of reviews of person-centered and patient-centered care. Patient Educ. Couns. 2019, 102, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Arias-Casais, N.; Amuthavalli Thiyagarajan, J.; Rodrigues Perracini, M.; Park, E.; Van den Block, L.; Sumi, Y.; Sadana, R.; Banerjee, A.; Han, Z.A. What long-term care interventions have been published between 2010 and 2020? Results of a WHO scoping review identifying long-term care interventions for older people around the world. BMJ Open 2022, 12, e054492. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Marzetti, E.; Thiem, U.; Perez-Zepeda, M.U.; Abellan Van Kan, G.; Landi, F.; Petrovic, M.; Cherubini, A.; Bernabei, R. The geriatric management of frailty as paradigm of “The end of the disease era”. Eur. J. Intern. Med. 2016, 31, 11–14. [Google Scholar] [CrossRef]
- Belloni, G.; Cesari, M. Frailty and Intrinsic Capacity: Two Distinct but Related Constructs. Front. Med. 2019, 6, 133. [Google Scholar] [CrossRef]
- World Health Organization. Integrated Care for Older People: Guidelines on Community-Level Interventions; World Health Organization: Geneva, Switzerland, 2017; Available online: https://apps.who.int/iris/handle/10665/258981 (accessed on 1 December 2021).
- Engel, G.L. The clinical application of the biopsychosocial model. Am. J. Psychiatry 1980, 137, 535–544. [Google Scholar]
- Baltes, P.B. Theoretical propositions of life-span developmental psychology: On the dynamics between growth and decline. Dev. Psychol. 1987, 23, 611–626. [Google Scholar] [CrossRef]
- Elder, G.H., Jr. The life course paradigm: Social change and individual development. In Examining Lives in Context: Perspectives on the Ecology of Human Development; Moen, P., Elder, G.H., Jr., Lüscher, K., Eds.; American Psychological Association: Washington, DC, USA, 1995; pp. 101–139. [Google Scholar] [CrossRef]
- Wallhagen, M.I.; Strawbridge, W.J.; Shema, S.J. The relationship between hearing impairment and cognitive function: A 5-year longitudinal study. Res. Gerontol. Nurs. 2008, 1, 80–86. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, B.J.; Jayakody, D.M.P.; Bennett, R.J.; Eikelboom, R.H.; Gasson, N.; Friedland, P.L. Hearing Loss and Depression in Older Adults: A Systematic Review and Meta-analysis. Gerontologist 2020, 60, e137–e154. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Martin, F.C.; Bergman, H.; Woo, J.; Romero-Ortuno, R.; Walston, J.D. Management of frailty: Opportunities, challenges, and future directions. Lancet 2019, 394, 1376–1386. [Google Scholar] [CrossRef] [PubMed]
- Bom, J.; Bakx, P.; Schut, F.; van Doorslaer, E. The Impact of Informal Caregiving for Older Adults on the Health of Various Types of Caregivers: A Systematic Review. Gerontologist 2019, 59, e629–e642. [Google Scholar] [CrossRef]
- Duplaga, M.; Grysztar, M.; Rodzinka, M.; Kopec, A. Scoping review of health promotion and disease prevention interventions addressed to elderly people. BMC Health Serv. Res. 2016, 16, 455–465. [Google Scholar] [CrossRef]
- Chiu, C.J.; Hu, J.C.; Lo, Y.H.; Chang, E.Y. Health Promotion and Disease Prevention Interventions for the Elderly: A Scoping Review from 2015-2019. Int. J. Environ. Res. Public Health 2020, 17, 5335. [Google Scholar] [CrossRef]
- Seah, B.; Kowitlawakul, Y.; Jiang, Y.; Ang, E.; Chokkanathan, S.; Wang, W. A review on healthy ageing interventions addressing physical, mental and social health of independent community-dwelling older adults. Geriatr. Nurs. 2019, 40, 37–50. [Google Scholar] [CrossRef]
- Campani, D.; Caristia, S.; Amariglio, A.; Piscone, S.; Ferrara, L.I.; Bortoluzzi, S.; Faggiano, F.; Dal Molin, A.; Group, I.W. Effective, sustainable, and transferable physical exercise interventions for fall prevention among older people. Public Health Nurs. 2021, 38, 1140–1176. [Google Scholar] [CrossRef]
- World Health Organization. WHO Evidence and Gap Maps for the UN Decade of Healthy Ageing. Available online: https://www.who.int/initiatives/decade-of-healthy-ageing/evidence-gap-map (accessed on 1 December 2022).
- Partridge, L.; Deelen, J.; Slagboom, P.E. Facing up to the global challenges of ageing. Nature 2018, 561, 45–56. [Google Scholar] [CrossRef]
- Welch, V.; Mathew, C.M.; Babelmorad, P.; Li, Y.; Ghogomu, E.T.; Borg, J.; Conde, M.; Kristjansson, E.; Lyddiatt, A.; Marcus, S.; et al. Health, social care and technological interventions to improve functional ability of older adults living at home: An evidence and gap map. Campbell Syst. Rev. 2021, 17, e1175. [Google Scholar] [CrossRef]
- World Health Organization. Decade of Healthy Ageing: Baseline Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Apostolo, J.; Cooke, R.; Bobrowicz-Campos, E.; Santana, S.; Marcucci, M.; Cano, A.; Vollenbroek-Hutten, M.; Germini, F.; D'Avanzo, B.; Gwyther, H.; et al. Effectiveness of interventions to prevent pre-frailty and frailty progression in older adults: A systematic review. JBI Database Syst. Rev. Implement Rep. 2018, 16, 140–232. [Google Scholar] [CrossRef] [PubMed]
- Burton, E.; Lewin, G.; Boldy, D. A Systematic Review of Physical Activity Programs for Older People Receiving Home Care Services. J. Aging Phys. Act. 2015, 23, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Franck, L.; Molyneux, N.; Parkinson, L. Systematic review of interventions addressing social isolation and depression in aged care clients. Qual. Life Res. 2016, 25, 1395–1407. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.; Peiris Casey, L.; Shields, N. Long-term home and community-based exercise programs improve function in community-dwelling older people with cognitive impairment: A systematic review. J. Physiother. 2017, 63, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.; Mackintosh, S.; Bird, E.; Ige, J.; Garrett, H.; Roys, M. The Role of Home Adaptations in Improving Later Life: A Systematic Review; Centre for Ageing Better: London, UK, 2017. [Google Scholar]
- Sims-Gould, J.; Tong, C.E.; Wallis-Mayer, L.; Ashe, M.C. Reablement, Reactivation, Rehabilitation and Restorative Interventions With Older Adults in Receipt of Home Care: A Systematic Review. J. Am. Med. Dir. Assoc. 2017, 18, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Smith Susan, M.; Wallace, E.; O'Dowd, T.; Fortin, M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings (Review). Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Weber, M.; Belala, N.; Clemson, L.; Boulton, E.; Hawley-Hague, H.; Becker, C.; Schwenk, M. Feasibility and Effectiveness of Intervention Programmes Integrating Functional Exercise into Daily Life of Older Adults: A Systematic Review. Gerontology 2018, 64, 172–187. [Google Scholar] [CrossRef] [PubMed]
- Zubala, A.; MacGillivray, S.; Frost, H.; Kroll, T.; Skelton, D.A.; Gavine, A.; Gray, N.M.; Toma, M.; Morris, J. Promotion of physical activity interventions for community dwelling older adults: A systematic review of reviews. PLoS ONE 2017, 12, e0180902. [Google Scholar] [CrossRef]
- Baxter, S.; Johnson, M.; Payne, N.; Buckley-Woods, H.; Blank, L.; Hock, E.; Daley, A.; Taylor, A.; Pavey, T.; Mountain, G.; et al. Promoting and maintaining physical activity in the transition to retirement: A Systematic Review of interventions for adults around retirement age. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 12. [Google Scholar] [CrossRef]
- Burton, E.; Cavalheri, V.; Adams, R.; Browne, C.O.; Bovery-Spencer, P.; Fenton, A.M.; Campbell, B.W.; Hill, K.D. Effectiveness of exercise programs to reduce falls in older people with dementia living in the community: A Systematic Review and Meta-analysis. Clin. Interv. Aging 2015, 10, 421–434. [Google Scholar] [CrossRef]
- Munk, T.; Tolstrup, U.; Beck, A.M.; Holst, M.; Rasmussen, K.; Hovhannisyan, K.; Thomsen, T. Individualized dietary counselling for nutritionally at-risk older patients following discharge from acute hospital to home: A systematic review and meta-analysis. J. Hum. Nutr. Diet. 2016, 29, 196–208. [Google Scholar] [CrossRef] [PubMed]
- van Abbema, R.; De Greef, M.; Crajé, C.; Krijnen, W.; Hobbelen, H.; Van Der Schans, C. What type or combination of exercise can improve preferred gait speed in older adults? A meta-analysis: Systematic review. BMC Geriatr. 2015, 15, 72. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Evidence Profile: Visual Impairment; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Evidence Profile: Hearing Loss; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- U.S. Preventive Services Task Force; Mangione, C.M.; Barry, M.J.; Nicholson, W.K.; Cabana, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Epling, J.W., Jr.; et al. Screening for Impaired Visual Acuity in Older Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2022, 327, 2123–2128. [Google Scholar] [CrossRef] [PubMed]
- U.S. Preventive Services Task Force; Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Epling, J.W., Jr.; et al. Screening for Hearing Loss in Older Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 1196–1201. [Google Scholar] [CrossRef]
- World Health Organization. Evidence Profile: Mobility Loss; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Evidence Profile: Risk of Falls; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Lacroix, A.; Hortobágyi, T.; Beurskens, R.; Granacher, U. Effects of Supervised vs. Unsupervised Training Programs on Balance and Muscle Strength in Older Adults: A Systematic Review and Meta-Analysis. Sport. Med. 2017, 47, 2341–2361. [Google Scholar] [CrossRef]
- Mareschal, J.; Genton, L.; Collet, T.H.; Graf, C. Nutritional Intervention to Prevent the Functional Decline in Community-Dwelling Older Adults: A Systematic Review. Nutrients 2020, 12, 2820. [Google Scholar] [CrossRef]
- World Health Organization. Evidence Profile: Cognitive Impairment; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Kim, S.J.; Yoo, G.E. Instrument Playing as a Cognitive Intervention Task for Older Adults: A Systematic Review and Meta-Analysis. Front. Psychol. 2019, 10, 151. [Google Scholar] [CrossRef]
- Meng, X.; Li, G.; Jia, Y.; Liu, Y.; Shang, B.; Liu, P.; Bao, X.; Chen, L. Effects of dance intervention on global cognition, executive function and memory of older adults: A meta-analysis and systematic review. Aging Clin. Exp. Res. 2020, 32, 7–19. [Google Scholar] [CrossRef]
- Vaportzis, E.; Niechcial, M.A.; Gow, A.J. A systematic literature review and meta-analysis of real-world interventions for cognitive ageing in healthy older adults. Ageing Res. Rev. 2019, 50, 110–130. [Google Scholar] [CrossRef]
- World Health Organization. Evidence Profile: Malnutrition; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Neves, F.J.; Tomita, L.Y.; Liu, A.; Andreoni, S.; Ramos, L.R. Educational interventions on nutrition among older adults: A systematic review and meta-analysis of randomized clinical trials. Maturitas 2020, 136, 13–21. [Google Scholar] [CrossRef]
- Raffaele, B.; Matarese, M.; Alvaro, R.; De Marinis, M.G. Health-promotion theories in nutritional interventions for community-dwelling older adults: A systematic review. Ann. Ist. Super. Sanita. 2017, 53, 146–151. [Google Scholar]
- Zhou, X.; Perez-Cueto, F.J.A.; Santos, Q.D.; Monteleone, E.; Giboreau, A.; Appleton, K.M.; Bjorner, T.; Bredie, W.L.P.; Hartwell, H. A Systematic Review of Behavioural Interventions Promoting Healthy Eating among Older People. Nutrients 2018, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Evidence Profile: Depressive Symptoms; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Li, S.Y.H.; Bressington, D. The effects of mindfulness-based stress reduction on depression, anxiety, and stress in older adults: A systematic review and meta-analysis. Int. J. Ment. Health Nurs. 2019, 28, 635–656. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Bai, Z.G.; Bo, A.; Chi, I. A systematic review and meta-analysis of music therapy for the older adults with depression. Int. J. Geriatr. Psychiatry 2016, 31, 1188–1198. [Google Scholar] [CrossRef] [PubMed]
- De Coninck, L.; Bekkering, G.E.; Bouckaert, L.; Declercq, A.; Graff, M.J.L.; Aertgeerts, B. Home- and Community-Based Occupational Therapy Improves Functioning in Frail Older People: A Systematic Review. J. Am. Geriatr. Soc. 2017, 65, 1863–1869. [Google Scholar] [CrossRef] [PubMed]
- Hunter Elizabeth, G.; Kearney Pamalyn, J. Occupational Therapy Interventions to Improve Performance of Instrumental Activities of Daily Living for Community-Dwelling Older Adults: A Systematic Review. Am. J. Occup. Ther. 2018, 72, 1–9. [Google Scholar]
- Liu, C.J.; Chang, W.P.; Chang, M.C. Occupational Therapy Interventions to Improve Activities of Daily Living for Community-Dwelling Older Adults: A Systematic Review. Am. J. Occup. Ther. 2018, 72, 1–11. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Perach, R. Interventions for alleviating loneliness among older persons: A critical review. Am. J. Health Promot. 2015, 29, e109–e125. [Google Scholar] [CrossRef]
- Poscia, A.; Stojanovic, J.; La Milia, D.I.; Duplaga, M.; Grysztar, M.; Moscato, U.; Onder, G.; Collamati, A.; Ricciardi, W.; Magnavita, N. Interventions targeting loneliness and social isolation among the older people: An update systematic review. Exp. Gerontol. 2018, 102, 133–144. [Google Scholar] [CrossRef]
- Tong, F.; Yu, C.; Wang, L.; Chi, I.; Fu, F. Systematic Review of Efficacy of Interventions for Social Isolation of Older Adults. Front. Psychol. 2021, 12, 554145. [Google Scholar] [CrossRef]
- World Health Organization. Advocacy Brief: Social Isolation and Loneliness Among Older People; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Sanches Machado d’Almeida, K.; Ronchi Spillere, S.; Zuchinali, P.; Correa Souza, G. Mediterranean Diet and Other Dietary Patterns in Primary Prevention of Heart Failure and Changes in Cardiac Function Markers: A Systematic Review. Nutrients 2018, 10, 58. [Google Scholar] [CrossRef] [PubMed]
- Sadowski, I.J.; Boesch, A.; Biedermann, A.; Auer, R.; Battegay, E.; Guessous, I.; Huber, F.; Humair, J.-P.; Neuner-Jehle, S.; Rodondi, N.; et al. Recommandations suisses pour le bilan de santé au cabinet médical. Forum Med. Suisse 2021, 21, 888–894. [Google Scholar] [CrossRef]
- U.S. Preventive Services Task Force. The Guide to Clinical Preventive Services; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014. [Google Scholar]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Back, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; McCloskey, E.V.; Johansson, H.; Cooper, C.; Rizzoli, R.; Reginster, J.Y.; on behalf of the Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the Committees of Scientific Advisors of the International Osteoporosis Foundation (IOF). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 2019, 30, 3–44. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Evidence Profile: Urinary Incontinence; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Evidence Profile: Caregiver Support; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Vandepitte, S.; Van Den Noortgate, N.; Putman, K.; Verhaeghe, S.; Verdonck, C.; Annemans, L. Effectiveness of respite care in supporting informal caregivers of persons with dementia: A systematic review. Int. J. Geriatr. Psychiatry 2016, 31, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Campos, D.M.; Ferreira, D.L.; Goncalves, G.H.; Farche, A.C.S.; de Oliveira, J.C.; Ansai, J.H. Effects of aquatic physical exercise on neuropsychological factors in older people: A systematic review. Arch. Gerontol. Geriatr. 2021, 96, 104435. [Google Scholar] [CrossRef] [PubMed]
- Lamboy, B.; Cotton, N.; Hamel, E.; Soleymani, D. Synthèse sur les interventions probantes favorisant le vieillissement en bonne santé. Gérontologie Société 2019, 41, 97–120. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guidelines on Physical Activity and Sedenary Behaviour; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- National Institute for Health Care and Excellence (NICE). Older People: Independence and Mental Wellbeing; NICE Guideline: London, UK, 2015. [Google Scholar]
- McDaid, D.; Forsman, A.; Matosevic, T.; La Park, A.; Wahlbeck, K. Evidence review 1: What Are the Most Effective Ways to Improve or Protect the Mental Wellbeing and/or Independence of Older People? Available online: https://www.nice.org.uk/guidance/ng32/evidence/evidence-review-1-review-of-effects-pdf-2242568562 (accessed on 1 June 2022).
- World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour: Web Annex. Evidence Profiles. Available online: https://apps.who.int/iris/bitstream/handle/10665/336657/9789240015111-eng.pdf (accessed on 1 December 2021).
- Chou, R.; Bougatsos, C.; Jungbauer, R.; Grusing, S.; Blazina, I.; Selph, S.; Jonas, D.E.; Tehrani, S. Screening for Impaired Visual Acuity in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2022, 327, 2129–2140. [Google Scholar] [CrossRef]
- Feltner, C.; Wallace, I.F.; Kistler, C.E.; Coker-Schwimmer, M.; Jonas, D.E. Screening for Hearing Loss in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2021, 325, 1202–1215. [Google Scholar] [CrossRef]
- Commission Consultative Pour le Soutien des Proches Aidants Actifs à Domicile. Programme de Soutien Aux Proches Aidants du Canton De Genève; République et Canton de Genève: Geneva, Switzerland, 2017; Available online: https://www.ge.ch/document/4189/telecharger (accessed on 3 March 2022).
- Gordon, E.H.; Hubbard, R.E. Frailty: Understanding the difference between age and ageing. Age Ageing 2022, 51, afac185. [Google Scholar] [CrossRef]
- Cesari, M.; Sumi, Y.; Han, Z.A.; Perracini, M.; Jang, H.; Briggs, A.; Amuthavalli Thiyagarajan, J.; Sadana, R.; Banerjee, A. Implementing care for healthy ageing. BMJ Glob. Health 2022, 7, e007778. [Google Scholar] [CrossRef] [PubMed]
- Keating, N. A research framework for the United Nations Decade of Healthy Ageing (2021–2030). Eur. J. Ageing 2022, 19, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Perracini, M.R.; Arias-Casais, N.; Thiyagarajan, J.A.; Rapson, C.; Isaac, V.; Ullah, S.; Hyobum, J.; Sadana, R.; Han, Z.A. A Recommended Package of Long-Term Care Services to Promote Healthy Ageing Based on a WHO Global Expert Consensus Study. J. Am. Med. Dir. Assoc. 2022, 23, 297–303. [Google Scholar] [CrossRef]
- Pin, S.; Spini, D.; Perrig-Chiello, P. Étude Sur Les Proches Aidants Et Les Professionnels de L’institution Genevoise de Maintien à Domicile Dans Le Canton de Genève—AGEneva Care; UNIL, imad: Lausanne, Switzerland, 2015. [Google Scholar]
- World Health Organization. Global Report on Ageism; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Hitzig, S.; Sheppard, C.; Kokorelias, K. The Use of Implementation Science to Foster Innovative Collaborations in Seniors Care. Int. J. Integr. Care 2022, 22, 251. [Google Scholar] [CrossRef]
- Sum, G.; Lau, L.K.; Jabbar, K.A.; Lun, P.; George, P.P.; Munro, Y.L.; Ding, Y.Y. The World Health Organization (WHO) Integrated Care for Older People (ICOPE) Framework: A Narrative Review on Its Adoption Worldwide and Lessons Learnt. Int. J. Environ. Res. Public Health 2022, 20, 154. [Google Scholar] [CrossRef]
- Briggs, A.M.; Araujo de Carvalho, I. Actions required to implement integrated care for older people in the community using the World Health Organization's ICOPE approach: A global Delphi consensus study. PLoS ONE 2018, 13, e0205533. [Google Scholar] [CrossRef] [PubMed]
- Bert, F.; Gualano, M.R.; Camussi, E.; Pieve, G.; Voglino, G.; Siliquini, R. Animal assisted intervention: A systematic review of benefits and risks. Eur. J. Integr. Med. 2016, 8, 695–706. [Google Scholar] [CrossRef]
- Gee, N.R.; Mueller, M.K.; Curl, A.L. Human–Animal Interaction and Older Adults: An Overview. Front. Psychol. 2017, 8, 1416. [Google Scholar] [CrossRef]
- Fancourt, D.; Tymoszuk, U. Cultural engagement and incident depression in older adults: Evidence from the English Longitudinal Study of Ageing. Br. J. Psychiatry 2019, 214, 225–229. [Google Scholar] [CrossRef]
- Fancourt, D.; Finn, S. What is the Evidence on the Role of the Arts in Improving Health and Well-Being? A Scoping Review; WHO Regional Office for Europe: Copenhagen, Denmark, 2019; Health Evidence Network (HEN) synthesis report 67. [Google Scholar]
- Beauchet, O.; Cooper-Brown, L.; Hayashi, Y.; Galery, K.; Vilcocq, C.; Bastien, T. Effects of “Thursdays at the Museum” at the Montreal Museum of Fine Arts on the mental and physical health of older community dwellers: The art-health randomized clinical trial protocol. Trials 2020, 21, 709. [Google Scholar] [CrossRef]
- Cotter, K.N.; Pawelski, J.O. Art museums as institutions for human flourishing. J. Posit. Psychol. 2022, 17, 288–302. [Google Scholar] [CrossRef]
- Busnel, C.; Ludwig, C. Vieillir en bonne santé. Gérontologie. 2002, 2, 10–12. [Google Scholar]
- Busnel, C.; Périvier, S.; Graf, G. Devenir l’acteur de son Vieillissement en Santé. 2022. Available online: https://www.svmed.ch/doc-mag/dossiers/geriatrie-vaudoise-du-pain-sur-la-planche/devenir-lacteur-de-son-vieillissement-en-sante/ (accessed on 1 September 2022).



{kind=link}
{kind=link}
| Intervention Type | Specific Intervention | ER | Specific Outcomes with Benefit |
|---|---|---|---|
| Preventive Care | Screening vs. no screening (vision and audition) [47,48] | NR | - |
| Screening and provision of care [45] | *** | Visual function and depression | |
| Screening and provision of hearing aids [46] | *** | Social function, depression, and hearing aid use |
| Intervention Type | Specific Intervention [Ref] | ER | Specific Outcomes with Benefit |
|---|---|---|---|
| Physical Activity | Physical activity interventions combined [80] | *** | Improved physical performance, muscle function, muscle mass, gait, balance, agility, and flexibility |
| Multimodal exercise ^ [49,50,81] | *** | Balance, muscle strength, physical functioning, and functional lower extremity strength. Rate of falls, fall-related injuries, the fear of falling ^ | |
| Aquatic exercise [79,80] | *** | Balance, flexibility, muscular strength and mass, walking capacity, and fear of falling | |
| Yoga [80] | ** | Balance and physical mobility | |
| Tai chi °^ [50,80] | ** | Muscular strength, joint stiffness, physical mobility, and a reduction in the risk of falling ° | |
| *** | Balance ^ | ||
| Digital exercise [80] | ** | Balance, physical performance, and physical activity uptake | |
| Supervised vs. unsupervised training programs [51] | *** | Balance and muscle strength | |
| Sedentary behaviour reduction [80,81] | ** | Physical function, activity level, risk of disability, muscle loss, and cardiometabolic capacities | |
| Progressive resistance training ^ [49,81] | *** | Muscle strength and mass and body weight ^ | |
| Dance [80] | ** | A decrease in the fear of falling | |
| Home-based | Multifactorial/unimodal multidisciplinary including OT ^ [50,64,80] | *** | Gait, balance abilities, fear of falling, and rate of falls ^ |
| Home modifications ^ [50] | *** | A decrease in the risk of falling ^ | |
| Sociocultural | Intergenerational activities [80] | *** | Physical strength and a reduction in sedentary behaviour |
| Music and singing [80] | ** | A reduction in falls | |
| Nutritional | Nutritional supplements ^ [52] | *** | Muscle mass, strength, and physical performance ^ |
| Nutritional interventions with physical exercise °^ [52] | *** | Muscle mass, strength, and physical performance ^ Sarcopenia prevention for healthy adults ° | |
| Other | The removal of psychotropic medications ^ [50] | *** | A reduction in the rate of falls ^ |
| Intervention Type | Specific Intervention | ER | Specific Outcomes with Benefit |
|---|---|---|---|
| Physical Activity | Physical activity interventions combined (including PRT and yoga) °^ [80] | *** | Improvement in cognitive function and risk reduction in cognitive decline °^ |
| Aquatic exercise [79] | *** | Improvements in visuospatial abilities, verbal short-term memory, and working memory | |
| Dance [55] | ** | Global cognition and memory | |
| Sociocultural | Intergenerational [80] | *** | Global cognition |
| Music (instrument playing) °^ [54] | *** | Improvements in processing speed, global cognition, attentional control, and executive function °^ | |
| Cognitive | Cognitive stimulation ^ [53] | *** | Global cognition ^ |
| Cognitive training °^ [53,80] | °*** ^** | Benefits in specific skills targeted °^ | |
| Psychological | Mindfulness [80] | ** | Improvements in attention, memory, cognitive flexibility, verbal fluency, and executive function |
| Meditation [80] | ** |
| Intervention Type | Specific Intervention [Ref] | Specific Outcomes with Benefit | |
|---|---|---|---|
| Nutritional | Meal service [60] | *** | Increase fruit consumption |
| Food aid (free meals and education) [80] | ** | Improved dietary intake | |
| Oral nutritional supplementation [57] | *** | Weight gain and improved handgrip strength | |
| Educational | Dietary education [58,59,60] | *** | An increase in the consumption of fruit, vegetable, fibre, micronutrients, and protein |
| Intervention Type | Specific Intervention [Ref] | ER | Specific Outcomes with Benefit |
|---|---|---|---|
| Physical activity | Physical activity interventions combined [80] | *** | Reduction in anxiodepressive symptoms |
| Aquatic exercise [79] | *** | Anxiety, tension, and fatigue | |
| Tai chi [80] | ** | Reduction in anxiodepressive symptoms | |
| Sociocultural | Intergenerational programs [80] | *** | Reduction in depressive symptoms |
| Music and singing [80,82] | ** | Reduction in anxiodepressive symptoms | |
| Music therapy ^ [63] | ** | Reduction in depressive symptoms ^ | |
| Educational | Continued education and learning [82] | ** | Increase in positive affect |
| Psychological | Mindfulness programs °^ [62,80] | ** | Reduction in depressive symptoms and increased positive affect ° Depressive symptoms ^ |
| Behavioural activation ^ [61] | Reduction in the incidence of depressive symptoms ^ | ||
| Cognitive behavioural therapy ^ [61] | |||
| Life-review therapy ^ [61] | *** | ||
| Problem-solving therapy ^ [61] | |||
| Interpersonal counselling ^ [61] |
| Intervention Type | Specific Intervention [Ref] | ER | Specific Outcomes with Benefit |
|---|---|---|---|
| Physical Activity | Accompanied by an occupational therapist [66] | *** | ADL performance in frail older adults (moderate benefits) |
| Multimodal exercise [49] | *** | ADL performance | |
| Home-based | Home modifications [66] | *** | ADL performance in adults with difficulties in ADL (high benefits) |
| Preventive home-based interventions including an occupational therapist [65] | *** | IADL performance and functional disability | |
| Self-management home-based interventions including an occupational therapist [65] | *** | IADL performance and social participation | |
| Home-based multidisciplinary rehabilitation [65] | *** | Decelerated decline in IADL performance and improved mobility | |
| Multidisciplinary interventions including occupational therapy [64] | *** | ADL performance | |
| Cognitive | Functional cognitive interventions [65] | *** | Cognition, with lasting effects on IADL performance |
| Intervention Type | Specific Intervention [Ref] | ER | Specific Outcomes with Benefit |
|---|---|---|---|
| Physical activity | Physical activity interventions combined [80] | *** | Improvements in social health, socialization, and social connections |
| Sociocultural | Intergenerational programs [80,82] | *** | Reduction in loneliness and the development/maintenance of social links. The development of meaningful roles |
| Music and singing [67,80,82] | ** | ||
| Arts and crafts [67,68] | ** | ||
| Support groups/online [67] | ** | ||
| Befriending programs [70,82] | ** | ||
| Volunteering [70,82] | ** | ||
| Educational | Technology training/use in interventions [67,68,69,70,82] | *** | Enables social participation and reduces isolation |
| Social network/friendship training [67,70,82] | *** | Development/maintenance of social links | |
| Psychological | Cognitive behavioural therapy [70] | ** | Loneliness reduction |
| Mindfulness programs [70,80] | ** | Loneliness reduction | |
| Home-based | Multidisciplinary interventions including occupational therapy [64,65] | *** | Increase in social participation |
| Intervention Type | Specific Intervention [Ref] | ER | Specific Outcomes with Benefit |
|---|---|---|---|
| Physical activity | Multimodal exercise [80,81] | *** | Cardiovascular system aerobic activity (Vo2 max) |
| Physical activity interventions combined [80] | *** | Osteoarticular system (osteoporosis and sarcopenia) | |
| Tai chi [80] | ** | Cardiovascular system (hypertension) | |
| Dance [80] | ** | Cardiovascular system aerobic activity (Vo2 max) | |
| Sedentary behaviour reduction [80] | ** | Cardiometabolic capacities | |
| Preventive care | Screening cancers [72,73] | *** | The early detection and treatment of lung, colorectal, breast, cervical, and prostate cancers |
| Screening of risk factors [72,73,74] | *** | The early detection of cardiovascular and metabolic risk factors (hypertension and obesity) | |
| Vaccinations [72] | *** | Immunization against flu, pneumococcus, herpes zoster, and SARS-CoV-2 (COVID-19) | |
| Nutritional | Mediterranean diet [71,74] | *** | Cardiovascular-system-protective effect on the incidence of heart failure |
| DASH diet [71] | ** | Cardiovascular system primary prevention of heart failure | |
| Limiting alcohol consumption [72,74] | *** | Cardiovascular health | |
| Other | Smoking cessation (motivational and/or pharmacological) [74,80] | *** | Cardiovascular, respiratory, and sensory health |
| Prompted voiding [76] | ** | Urinary incontinence episodes | |
| Pelvic floor muscle training [76] | *** | Urinary incontinence episodes, symptoms, and quality of life |
| Intervention Type | Specific Intervention [Ref] | ER | Specific Outcomes with Benefit |
|---|---|---|---|
| Support groups/online [77] | ** | A decrease in burden and an increase in ability/knowledge | |
| Educational | Caregiver training [77] | *** | Increased subjective well-being |
| Psychological | Cognitive behavioural therapy [77] | *** | A decrease in burden and depression and an increase in ability, knowledge, well-being |
| Psychoeducation [77] | *** | A decrease in burden and depression and an increase in ability and knowledge | |
| Other | Respite care [77,78] | * | A reduction in depression, anger, burden, and quality of life. An acceleration of care receiver placement in nursing homes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashikali, E.-M.; Ludwig, C.; Mastromauro, L.; Périvier, S.; Tholomier, A.; Ionita, I.; Graf, C.; Busnel, C. Intrinsic Capacities, Functional Ability, Physiological Systems, and Caregiver Support: A Targeted Synthesis of Effective Interventions and International Recommendations for Older Adults. Int. J. Environ. Res. Public Health 2023, 20, 4382. https://doi.org/10.3390/ijerph20054382
Ashikali E-M, Ludwig C, Mastromauro L, Périvier S, Tholomier A, Ionita I, Graf C, Busnel C. Intrinsic Capacities, Functional Ability, Physiological Systems, and Caregiver Support: A Targeted Synthesis of Effective Interventions and International Recommendations for Older Adults. International Journal of Environmental Research and Public Health. 2023; 20(5):4382. https://doi.org/10.3390/ijerph20054382
Chicago/Turabian StyleAshikali, Eleni-Marina, Catherine Ludwig, Laura Mastromauro, Samuel Périvier, Aude Tholomier, Irina Ionita, Christophe Graf, and Catherine Busnel. 2023. "Intrinsic Capacities, Functional Ability, Physiological Systems, and Caregiver Support: A Targeted Synthesis of Effective Interventions and International Recommendations for Older Adults" International Journal of Environmental Research and Public Health 20, no. 5: 4382. https://doi.org/10.3390/ijerph20054382
APA StyleAshikali, E.-M., Ludwig, C., Mastromauro, L., Périvier, S., Tholomier, A., Ionita, I., Graf, C., & Busnel, C. (2023). Intrinsic Capacities, Functional Ability, Physiological Systems, and Caregiver Support: A Targeted Synthesis of Effective Interventions and International Recommendations for Older Adults. International Journal of Environmental Research and Public Health, 20(5), 4382. https://doi.org/10.3390/ijerph20054382