
Meta-Analysis of Exploring the Effect of Curcumin Supplementation with or without Other Advice on Biochemical and Anthropometric Parameters in Patients with Metabolic-Associated Fatty Liver Disease (MAFLD)

 , , and
, , and 
Abstract
1. Introduction
2. Pathophysiology
3. Curcumin
4. Material and Methods
4.1. Types of Participants
4.2. Types of Interventions
4.3. Types of Comparisons
4.4. Types of Outcomes
4.5. Types of Studies
4.6. Search Strategy and Study Selection
4.7. Quality and Risk of Bias Assessment
4.8. Statistical Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Random Sequence Generation | Allocation Concealment | Blinding of Participant and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias | |
|---|---|---|---|---|---|---|---|
| Rahmani, 2016 [23] | + | + | + | + | + | + | + |
| Kelardeh, 2017 [24] | +/− | + | + | + | + | + | +/− |
| Navekar, 2017 [25] | + | + | + | + | + | + | + |
| Chashmniam, 2019 [26] | + | + | + | + | + | + | + |
| Mirhafez, 2019 [27] | +/− | + | + | + | + | + | + |
| Hariri, 2020 [28] | + | + | + | + | + | + | + |
| Kelardeh, 2020 [29] | +/− | + | + | + | + | + | +/− |
| Saberi-Karimian, 2020 [30] | + | + | + | + | + | + | + |
| Panahi, 2016 [31] | +/− | + | − | − | + | + | + |
| Panahi, 2017 [32] | + | + | + | + | + | + | + |
| Jazayeri-Tehrani, 2019 [33] | +/− | + | + | + | + | + | + |
| Saadati, 2019 (a) [34] | + | + | + | + | + | + | + |
| Saadati, 2019 (b) [35] | + | + | + | + | + | + | + |
| Cicero, 2020 [36] | + | + | + | + | + | + | + |
5. Results
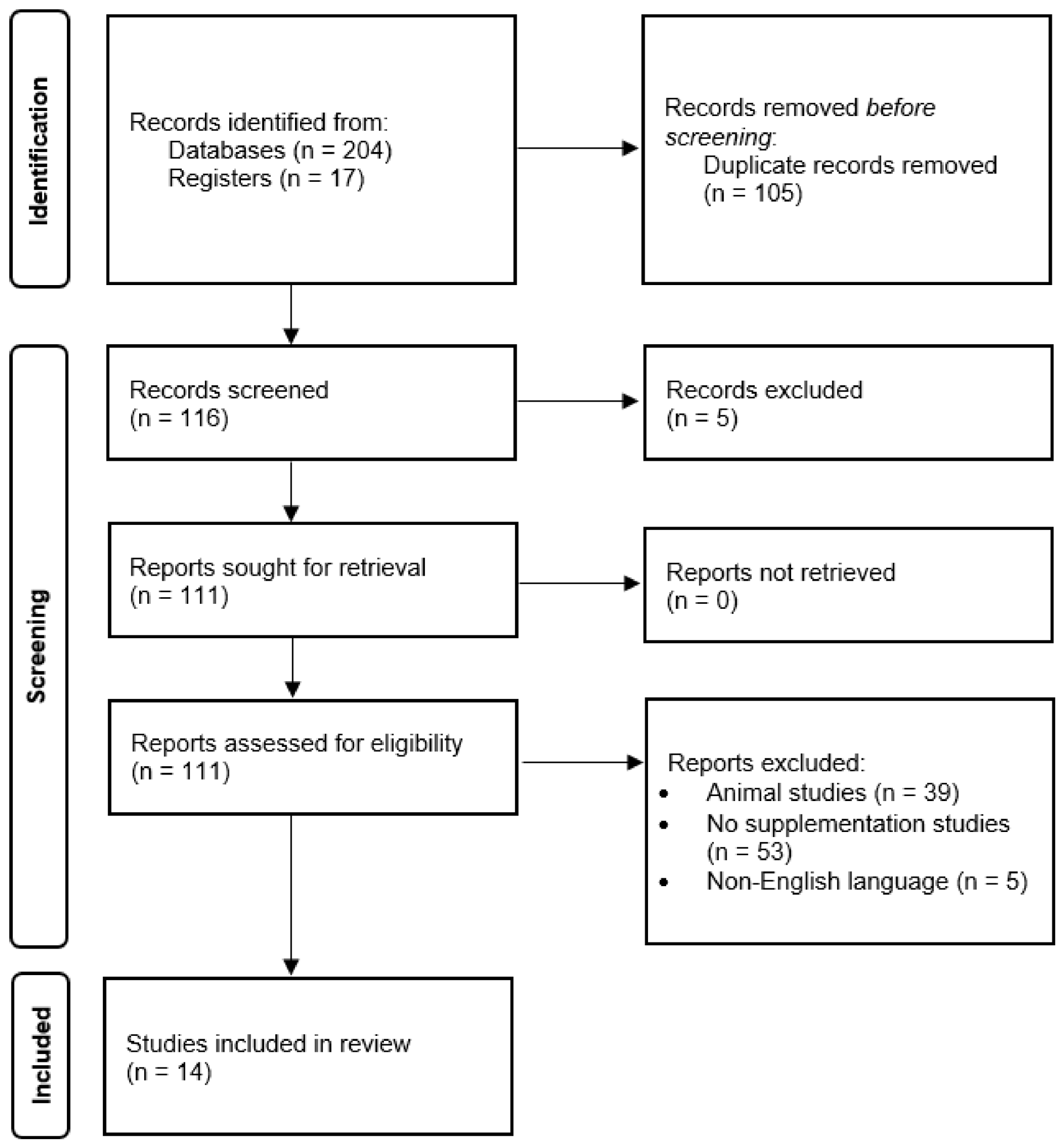
5.1. Study Selection
5.2. Participant and Study Characteristics
5.3. Interventions
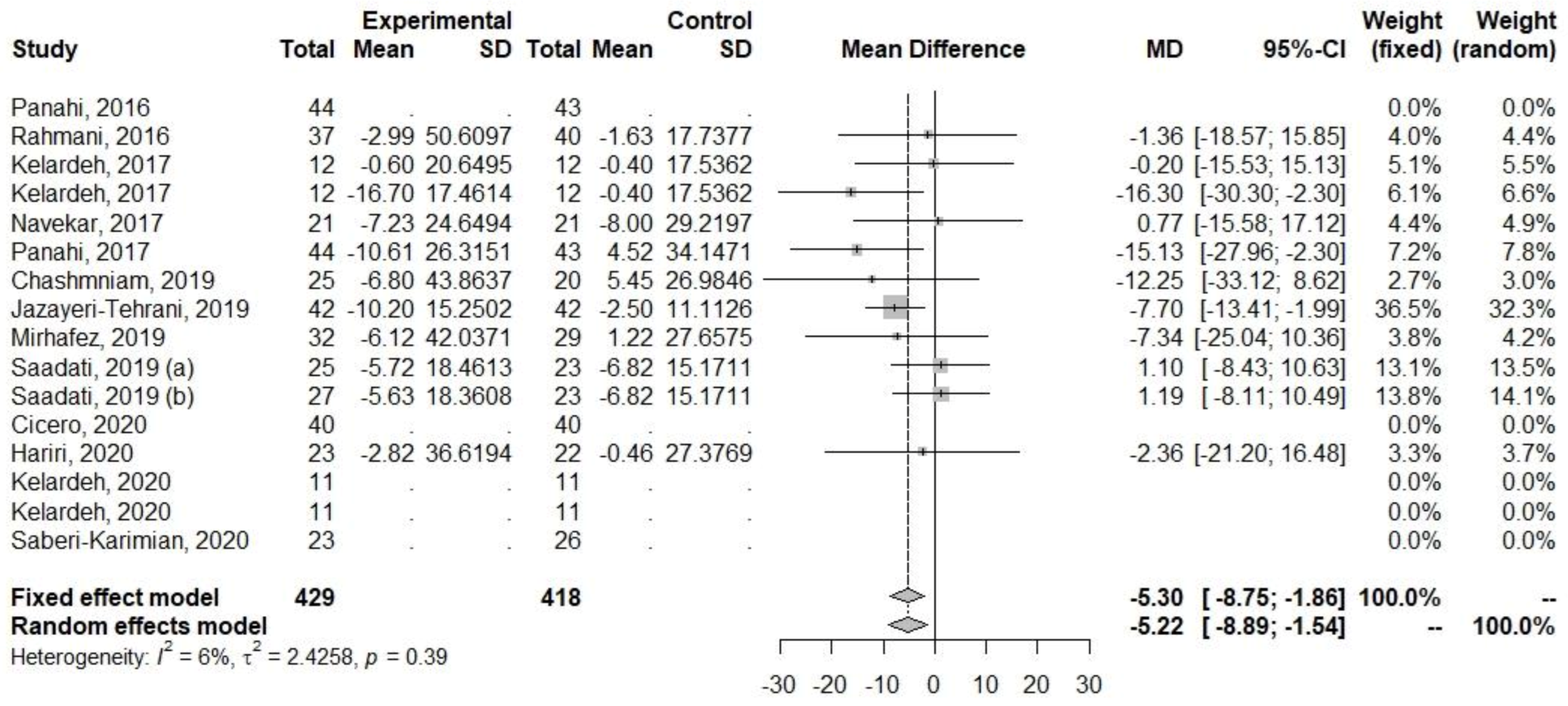
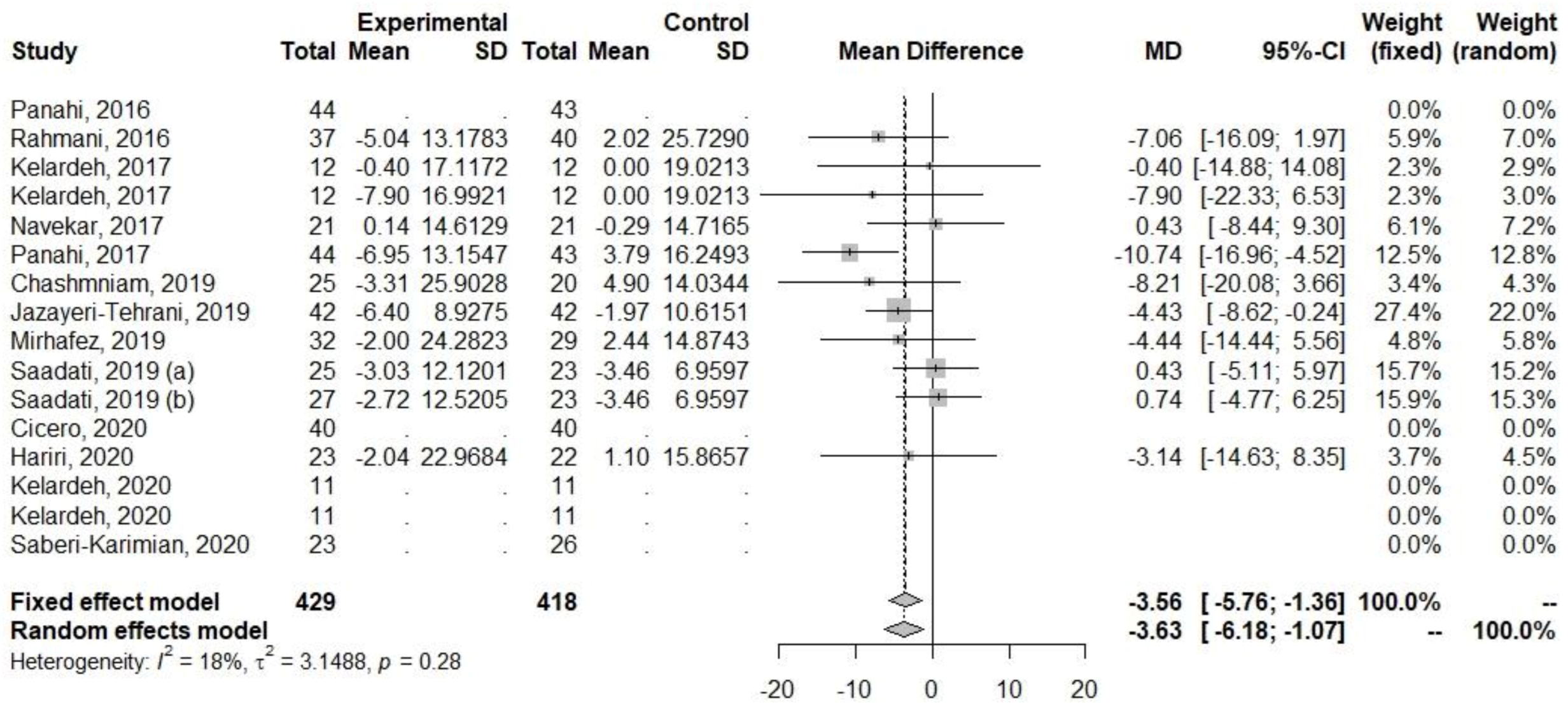
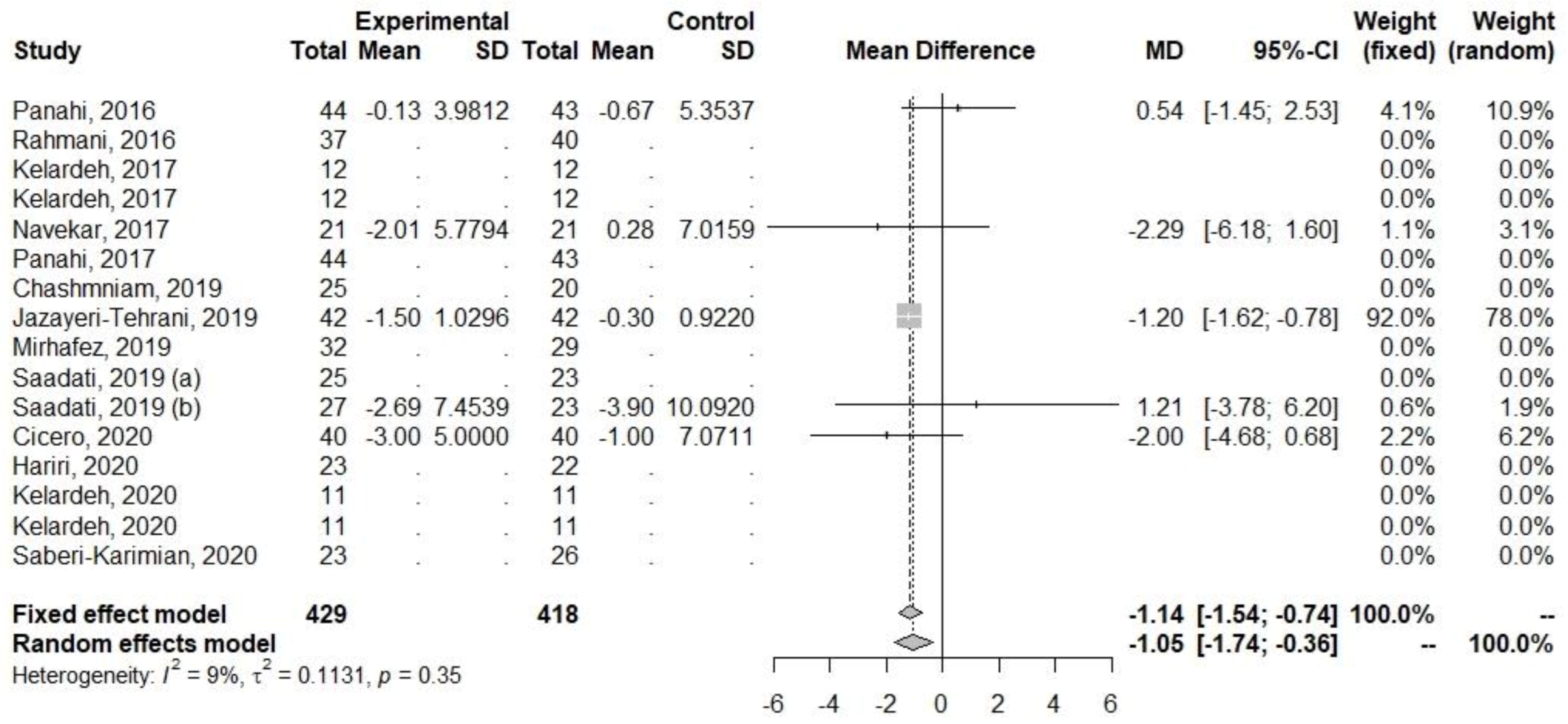
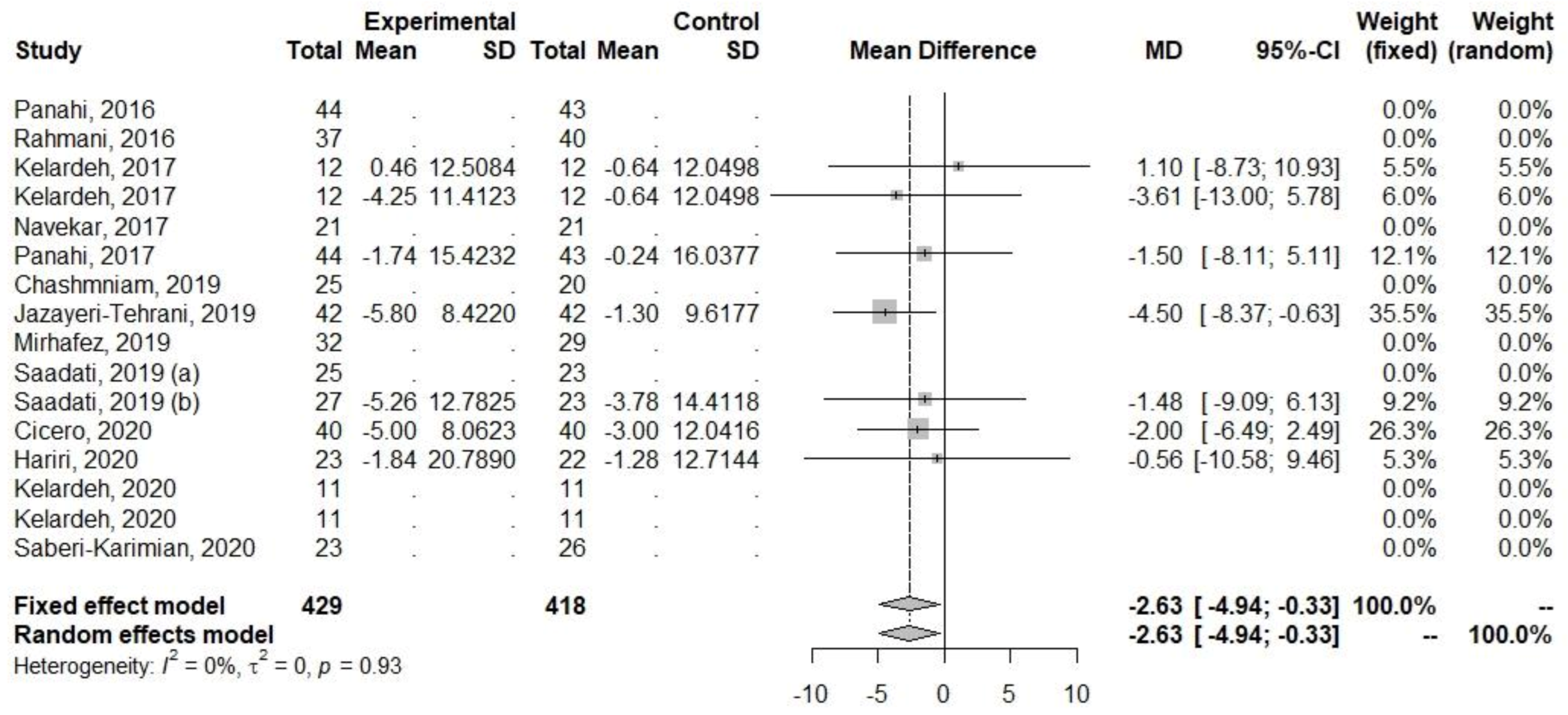
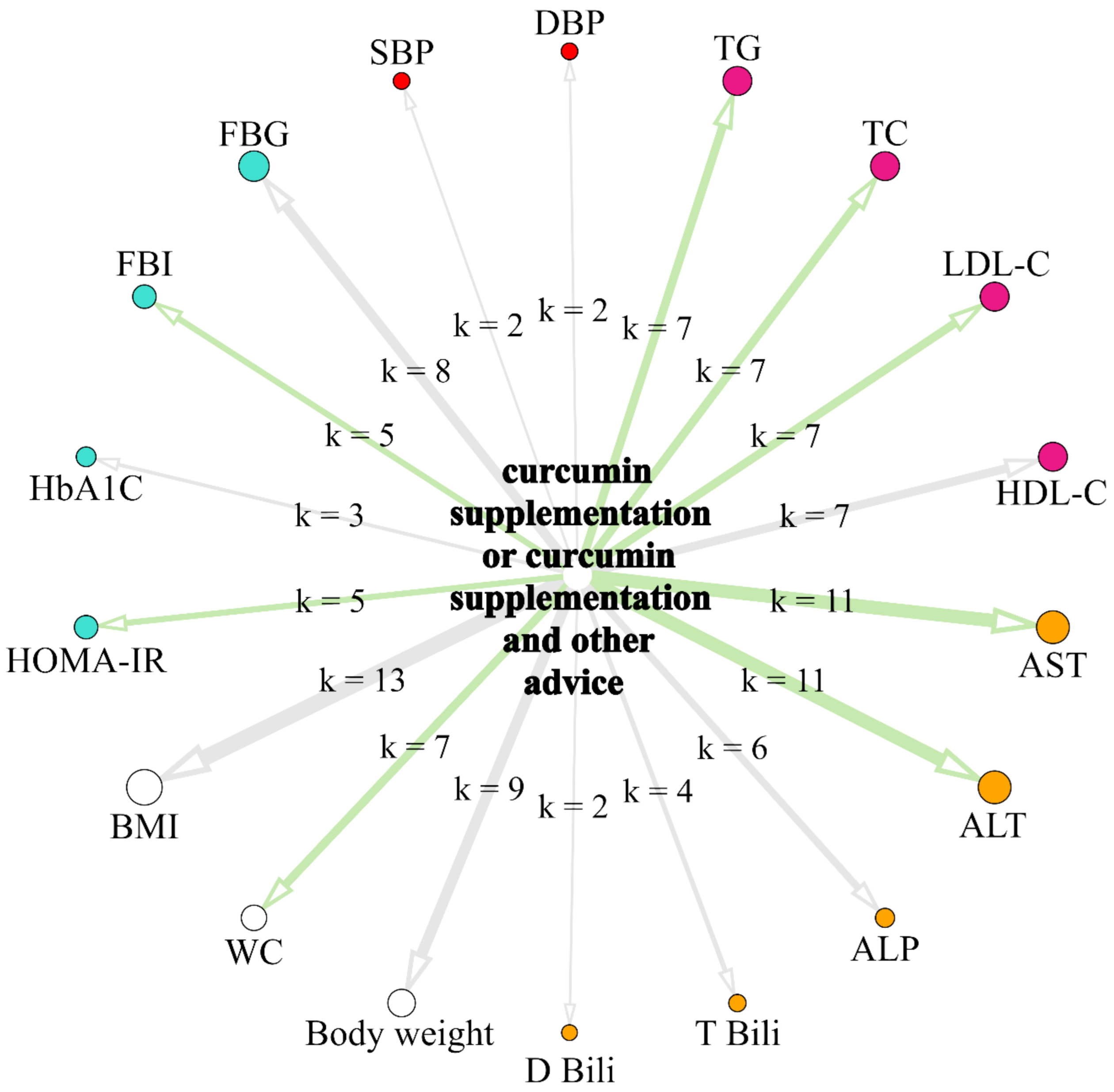
5.4. Effect of Curcumin Supplementation and Curcumin Supplementation with Physical Activity and/or Dietary Advice and/or Lifestyle Changes on the Levels of Biochemical Parameters
6. Discussion
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Younossi, Z.M. Non-Alcoholic Fatty Liver Disease—A Global Public Health Perspective. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.D.; Stengel, J.; Asike, M.I.; Torres, D.M.; Shaw, J.; Contreras, M.; Landt, C.L.; Harrison, S.A. Prevalence of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis among a Largely Middle-Aged Population Utilizing Ultrasound and Liver Biopsy: A Prospective Study. Gastroenterology 2011, 140, 124–131. [Google Scholar] [CrossRef]
- Słomko, J.; Zalewska, M.; Niemiro, W.; Kujawski, S.; Słupski, M.; Januszko-Giergielewicz, B.; Zawadka-Kunikowska, M.; Newton, J.; Hodges, L.; Kubica, J.; et al. Evidence-Based Aerobic Exercise Training in Metabolic-Associated Fatty Liver Disease: Systematic Review with Meta-Analysis. J. Clin. Med. 2021, 10, 1659. [Google Scholar] [CrossRef] [PubMed]
- Welsh, J.A.; Karpen, S.; Vos, M.B. Increasing Prevalence of Nonalcoholic Fatty Liver Disease Among United States Adolescents, 1988–1994 to 2007–2010. J. Pediatr. 2013, 162, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Pavlides, M.; Cobbold, J. Non-Alcoholic Fatty Liver Disease. Medicine 2019, 47, 728–733. [Google Scholar] [CrossRef]
- Buzzetti, E.; Pinzani, M.; Tsochatzis, E.A. The Multiple-Hit Pathogenesis of Non-Alcoholic Fatty Liver Disease (NAFLD). Metabolism 2016, 65, 1038–1048. [Google Scholar] [CrossRef]
- Tilg, H.; Effenberger, M. From NAFLD to MAFLD: When Pathophysiology Succeeds. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 387–388. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The Diagnosis and Management of Nonalcoholic Fatty Liver Disease: Practice Guidance from the American Association for the Study of Liver Diseases: Hepatology, Vol. XX, No. X, 2017. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Mantovani, A.; Byrne, C.D.; Bonora, E.; Targher, G. Nonalcoholic Fatty Liver Disease and Risk of Incident Type 2 Diabetes: A Meta-Analysis. Diabetes Care 2018, 41, 372–382. [Google Scholar] [CrossRef]
- Targher, G.; Day, C.P.; Bonora, E. Risk of Cardiovascular Disease in Patients with Nonalcoholic Fatty Liver Disease. N. Engl. J. Med. 2010, 363, 1341–1350. [Google Scholar] [CrossRef]
- Haddad, T.M.; Hamdeh, S.; Kanmanthareddy, A.; Alla, V.M. Nonalcoholic Fatty Liver Disease and the Risk of Clinical Cardiovascular Events: A Systematic Review and Meta-Analysis. Diabetes Metab. Syndr. 2017, 11 (Suppl. S1), S209–S216. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Priyadarshi, R.N.; Anand, U. Non-Alcoholic Fatty Liver Disease: Growing Burden, Adverse Outcomes and Associations. J. Clin. Transl. Hepatol. 2020, 8, 76–86. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the Management of Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Hewlings, S.; Kalman, D. Curcumin: A Review of Its’ Effects on Human Health. Foods 2017, 6, 92. [Google Scholar] [CrossRef]
- Sohn, S.-I.; Priya, A.; Balasubramaniam, B.; Muthuramalingam, P.; Sivasankar, C.; Selvaraj, A.; Valliammai, A.; Jothi, R.; Pandian, S. Biomedical Applications and Bioavailability of Curcumin—An Updated Overview. Pharmaceutics 2021, 13, 2102. [Google Scholar] [CrossRef]
- Chong, L.; Zhang, W.; Nie, Y.; Yu, G.; Liu, L.; Lin, L.; Wen, S.; Zhu, L.; Li, C. Protective Effect of Curcumin on Acute Airway Inflammation of Allergic Asthma in Mice through Notch1-GATA3 Signaling Pathway. Inflammation 2014, 37, 1476–1485. [Google Scholar] [CrossRef]
- Ramírez-Tortosa, M.C.; Mesa, M.D.; Aguilera, M.C.; Quiles, J.L.; Baró, L.; Ramirez-Tortosa, C.L.; Martinez-Victoria, E.; Gil, A. Oral Administration of a Turmeric Extract Inhibits LDL Oxidation and Has Hypocholesterolemic Effects in Rabbits with Experimental Atherosclerosis. Atherosclerosis 1999, 147, 371–378. [Google Scholar] [CrossRef]
- Quiles, J.L.; Mesa, M.D.; Ramírez-Tortosa, C.L.; Aguilera, C.M.; Battino, M.; Gil, A.; Ramírez-Tortosa, M.C. Curcuma Longa Extract Supplementation Reduces Oxidative Stress and Attenuates Aortic Fatty Streak Development in Rabbits. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 1225–1231. [Google Scholar] [CrossRef]
- Burge, K.; Gunasekaran, A.; Eckert, J.; Chaaban, H. Curcumin and Intestinal Inflammatory Diseases: Molecular Mechanisms of Protection. Int. J. Mol. Sci. 2019, 20, 1912. [Google Scholar] [CrossRef]
- Giordano, A.; Tommonaro, G. Curcumin and Cancer. Nutrients 2019, 11, 2376. [Google Scholar] [CrossRef]
- Różański, G.; Kujawski, S.; Newton, J.L.; Zalewski, P.; Słomko, J. Curcumin and Biochemical Parameters in Metabolic-Associated Fatty Liver Disease (MAFLD)—A Review. Nutrients 2021, 13, 2654. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, S.; Asgary, S.; Askari, G.; Keshvari, M.; Hatamipour, M.; Feizi, A.; Sahebkar, A. Treatment of Non-Alcoholic Fatty Liver Disease with Curcumin: A Randomized Placebo-Controlled Trial. Phytother. Res. 2016, 30, 1540–1548. [Google Scholar] [CrossRef]
- Kelardeh, B.M.; Keshavarz, S.; Karimi, M. Effects of Nonlinear Resistance Training with Curcumin Supplement on Liver Enzymes in Men with Non- Alcoholic Fatty Liver Disease. Rep. Health Care 2017, 3, 1–9. [Google Scholar]
- Navekar, R.; Rafraf, M.; Ghaffari, A.; Asghari-Jafarabadi, M.; Khoshbaten, M. Turmeric Supplementation Improves Serum Glucose Indices and Leptin Levels in Patients with Nonalcoholic Fatty Liver Diseases. J. Am. Coll. Nutr. 2017, 36, 261–267. [Google Scholar] [CrossRef]
- Chashmniam, S.; Mirhafez, S.R.; Dehabeh, M.; Hariri, M.; Nezhad, M.A.; Nobakht, M.; Gh, B.F. A Pilot Study of the Effect of Phospholipid Curcumin on Serum Metabolomic Profile in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Trial. Eur. J. Clin. Nutr. 2019, 73, 1224–1235. [Google Scholar] [CrossRef]
- Mirhafez, S.R.; Farimani, A.R.; Dehhabe, M.; Bidkhori, M.; Hariri, M.; Ghouchani, F.N.M.; Abdollahi, F. Effect of Phytosomal Curcumin on Circulating Levels of Adiponectin and Leptin in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. J. Gastrointestin. Liver Dis. 2019, 28, 7. [Google Scholar] [CrossRef]
- Hariri, M.; Gholami, A.; Mirhafez, S.R.; Bidkhori, M.; Sahebkar, A. A Pilot Study of the Effect of Curcumin on Epigenetic Changes and DNA Damage among Patients with Non-Alcoholic Fatty Liver Disease—A Randomized, Double-Blind, Placebo-Controlled, Clinical Trial. Complement. Ther. Med. 2020, 51, 102447. [Google Scholar] [CrossRef]
- Kelardeh, B.M.; Rahmati-Ahmadabad, S.; Farzanegi, P.; Helalizadeh, M.; Azarbayjani, M.-A. Effects of Non-Linear Resistance Training and Curcumin Supplementation on the Liver Biochemical Markers Levels and Structure in Older Women with Non-Alcoholic Fatty Liver Disease. J. Bodyw. Mov. Ther. 2020, 24, 154–160. [Google Scholar] [CrossRef]
- Saberi-Karimian, M.; Keshvari, M.; Ghayour-Mobarhan, M.; Salehizadeh, L.; Rahmani, S.; Behnam, B.; Jamialahmadi, T.; Asgary, S.; Sahebkar, A. Effects of Curcuminoids on Inflammatory Status in Patients with Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Complement. Ther. Med. 2020, 49, 102322. [Google Scholar] [CrossRef]
- Panahi, Y.; Kianpour, P.; Mohtashami, R.; Jafari, R.; Simental-Mendía, L.E.; Sahebkar, A. Curcumin Lowers Serum Lipids and Uric Acid in Subjects With Nonalcoholic Fatty Liver Disease: A Randomized Controlled Trial. J. Cardiovasc. Pharmacol. 2016, 68, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Panahi, Y.; Kianpour, P.; Mohtashami, R.; Jafari, R.; Simental-Mendía, L.; Sahebkar, A. Efficacy and Safety of Phytosomal Curcumin in Non-Alcoholic Fatty Liver Disease: A Randomized Controlled Trial. Drug Res. 2017, 67, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Jazayeri-Tehrani, S.A.; Rezayat, S.M.; Mansouri, S.; Qorbani, M.; Alavian, S.M.; Daneshi-Maskooni, M.; Hosseinzadeh-Attar, M.-J. Nano-Curcumin Improves Glucose Indices, Lipids, Inflammation, and Nesfatin in Overweight and Obese Patients with Non-Alcoholic Fatty Liver Disease (NAFLD): A Double-Blind Randomized Placebo-Controlled Clinical Trial. Nutr. Metab. 2019, 16, 8. [Google Scholar] [CrossRef] [PubMed]
- Saadati, S.; Sadeghi, A.; Mansour, A.; Yari, Z.; Poustchi, H.; Hedayati, M.; Hatami, B.; Hekmatdoost, A. Curcumin and Inflammation in Non-Alcoholic Fatty Liver Disease: A Randomized, Placebo Controlled Clinical Trial. BMC Gastroenterol. 2019, 19, 133. [Google Scholar] [CrossRef] [PubMed]
- Saadati, S.; Hatami, B.; Yari, Z.; Shahrbaf, M.A.; Eghtesad, S.; Mansour, A.; Poustchi, H.; Hedayati, M.; Aghajanpoor-pasha, M.; Sadeghi, A.; et al. The Effects of Curcumin Supplementation on Liver Enzymes, Lipid Profile, Glucose Homeostasis, and Hepatic Steatosis and Fibrosis in Patients with Non-Alcoholic Fatty Liver Disease. Eur. J. Clin. Nutr. 2019, 73, 441–449. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Sahebkar, A.; Fogacci, F.; Bove, M.; Giovannini, M.; Borghi, C. Effects of Phytosomal Curcumin on Anthropometric Parameters, Insulin Resistance, Cortisolemia and Non-Alcoholic Fatty Liver Disease Indices: A Double-Blind, Placebo-Controlled Clinical Trial. Eur. J. Nutr. 2020, 59, 477–483. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Easterbrook, P.J.; Gopalan, R.; Berlin, J.A.; Matthews, D.R. Publication Bias in Clinical Research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A Software Environment for Integrated Models of Biomolecular Interaction Networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef] [PubMed]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The Well-Built Clinical Question: A Key to Evidence-Based Decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef] [PubMed]
- Pulido-Moran, M.; Moreno-Fernandez, J.; Ramirez-Tortosa, C.; Ramirez-Tortosa, M. Curcumin and Health. Molecules 2016, 21, 264. [Google Scholar] [CrossRef] [PubMed]
- Keating, S.E.; Adams, L.A. Exercise in NAFLD: Just Do It. J. Hepatol. 2016, 65, 671–673. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. Br. J. Sport. Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Machado, M.; Cortez-Pinto, H. Diet, Microbiota, Obesity, and NAFLD: A Dangerous Quartet. Int. J. Mol. Sci. 2016, 17, 481. [Google Scholar] [CrossRef]
- Ngu, M.H.; Norhayati, M.N.; Rosnani, Z.; Zulkifli, M.M. Curcumin as Adjuvant Treatment in Patients with Non-Alcoholic Fatty Liver (NAFLD) Disease: A Systematic Review and Meta-Analysis. Complement. Ther. Med. 2022, 68, 102843. [Google Scholar] [CrossRef]
- Goodarzi, R.; Sabzian, K.; Shishehbor, F.; Mansoori, A. Does Turmeric/Curcumin Supplementation Improve Serum Alanine Aminotransferase and Aspartate Aminotransferase Levels in Patients with Nonalcoholic Fatty Liver Disease? A Systematic Review and Meta-Analysis of Randomized Controlled Trials: Turmeric/Curcumin Supplementation and Liver Enzymes. Phytother. Res. 2019, 33, 561–570. [Google Scholar] [CrossRef]
- Yang, K.; Chen, J.; Zhang, T.; Yuan, X.; Ge, A.; Wang, S.; Xu, H.; Zeng, L.; Ge, J. Efficacy and Safety of Dietary Polyphenol Supplementation in the Treatment of Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Front. Immunol. 2022, 13, 949746. [Google Scholar] [CrossRef]
- Jalali, M.; Mahmoodi, M.; Mosallanezhad, Z.; Jalali, R.; Imanieh, M.H.; Moosavian, S.P. The Effects of Curcumin Supplementation on Liver Function, Metabolic Profile and Body Composition in Patients with Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Complement. Ther. Med. 2020, 48, 102283. [Google Scholar] [CrossRef]
- Wei, Z.; Liu, N.; Tantai, X.; Xing, X.; Xiao, C.; Chen, L.; Wang, J. The Effects of Curcumin on the Metabolic Parameters of Non-Alcoholic Fatty Liver Disease: A Meta-Analysis of Randomized Controlled Trials. Hepatol. Int. 2019, 13, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Baziar, N.; Parohan, M. The Effects of Curcumin Supplementation on Body Mass Index, Body Weight, and Waist Circumference in Patients with Nonalcoholic Fatty Liver Disease: A Systematic Review and Dose–Response Meta-analysis of Randomized Controlled Trials. Phytother. Res. 2020, 34, 464–474. [Google Scholar] [CrossRef] [PubMed]











| Study Design | Duration | n (Study Group/ Control Group) | Age, Years | BMI | Dose | Control Group | Tested Parameters | |
|---|---|---|---|---|---|---|---|---|
| Rahmani, 2016 [23] | RCT | 8 weeks | 37/40 | 46.3 11.57 | 30.84 | 500 mg/day of an amorphous dispersion preparation comprising 70 mg curcuminoids | Received placebo | ALT, AST, BMI, FGB, HbA1c, HDL-C, LDL-C, TC, TG, body weight |
| Kelardeh, 2017 [24] | RCT | 12 weeks | 12/12 | 37.41 5.17 | 29.88 | 80 mg/day curcumin as a nanomicelle | Received one placebo (3 g dextrose) capsule per day | ALT, AST, ALP, BMI, WC |
| Navekar, 2017 [25] | DB, RCT | 12 weeks | 21/21 | 31.81 | 3 g/day turmeric (6 × 500 mg three times a day) | Patients were given six placebo capsules daily | ALT, AST, BMI, FGB, FBI, HOMA-IR, body weight | |
| Chashmniam, 2019 [26] | DB, RCT | 8 weeks | 25/20 | 46.56 2.25 | 30.03 | Phospholipid curcumin 250 mg/day (equivalent to 50 mg pure curcumin) | Received one placebo capsule per day | ALT, AST, ALP, BMI, D Bili, FGB, HDL-C, LDL-C, TC, TG, T Bili, body weight |
| Mirhafez, 2019 [27] | DB, RCT | 8 weeks | 32/29 | 44.8 | 30.06 | Phospholipid curcumin 250 mg/day (equivalent to 50 mg pure curcumin) | Received a placebo | ALT, AST, BMI, FGB, HDL-C, LDL-C, TC, TG, body weight |
| Hariri, 2020 [28] | DB, RCT | 8 weeks | 23/22 | 40.95 | 30.59 | Phospholipid curcumin 250 mg/day (equivalent to 50 mg pure curcumin) | Received a placebo | ALT, AST, BMI, WC, body weight |
| Kelardeh, 2020 [29] | RCT | 12 weeks | 11/11 | 66.72 | 27.60 | 80 mg/day curcumin as a nanomicelle | Received a placebo capsule | ALP, BMI, T Bili, body weight |
| Saberi-Karimian, 2020 [30] | RCT | 8 weeks | 23/26 | 18–70 | 30.02 | 500 mg curcuminoids + 5 mg piperine/day | Received one placebo capsule per day | ALT, AST, TG, TC, LDL-C, HDL-C, BDP, SBP, FBG, WC, BMI, body weight |
| Study Design | Duration | n (Study Group/ Control Group) | Age, Years | BMI | Dose | Other Advice | Control Group | Tested Parameters | |
|---|---|---|---|---|---|---|---|---|---|
| Panahi, 2016 [31] | RCT | 8 weeks | 44/43 | 45 12.59 | 28.97 ± 3.42 | 1000 mg/day in two divided doses | All patients received dietary and lifestyle advice before the start of the trial | Patients received lactose as a placebo | FGB, FBI, HbA1c, HDL, HOMA-IR, LDL-C, TC, TG |
| Kelardeh, 2017 [24] | RCT | 12 weeks | 12/12 | 38.24 6.59 | 30.27 | 80 mg curcumin as a nanomicelle | 12 weeks of non-linear resistance training. Each session took about 45–60 min, three days a week (non-consecutive), lasting 12 weeks | Received one placebo capsule per day | ALP, ALT, AST, BMI, WC |
| Panahi, 2017 [32] | RCT | 8 weeks | 44/43 | 44.98 12.59 | 28.97 | 1000 mg/day in 2 divided doses | All patients received dietary and lifestyle advice before the start of the trial | Received a placebo | ALP, ALT, AST, BMI, D Bili, T Bili, WC |
| Jazayeri-Tehrani, 2019 [33] | DB, RCT | 12 weeks | 42/42 | 41.8 5.6 | 30.6 | The sinacurcumin® dose was 80 mg/day (two 40 mg capsules per day) | The lifestyle advice was equally presented by a trained dietician (SAJT) at the hospital | Received two placebo capsules per day | ALT, AST, BMI, DBP, FGB, FBI, HbA1c, HDL-C, HOMA-IR, LDL-C, SBP, TC, TG, WC, Body weight |
| Saadati, 2019 (a) [34] | RCT | 12 weeks | 25/23 | 45.13 10.9 | 32.30 | 3 × 500 mg/day (95% curcuminoids) | Nutrient distribution was as follows: diet macronutrients 52 to 55% of energy from carbohydrates, less than 30% of energy from lipids, and 15–18% of energy from proteins was provided. Patients were advised to exercise ≥30 min, three times per week. | Received three placebo capsules per day | ALT, AST |
| Saadati, 2019 (b) [35] | RCT | 12 weeks | 27/23 | 45.13 10.9 | 32.3 | 3 × 500 mg/day (95% curcuminoids) | The distribution of nutrients: total fat less than 30% total energy value, protein 15–18%, and carbohydrates 52–55%. Patients are advised to exercise ≥30 min, three times per week | Received placebo capsules | ALT, AST, BMI, FGB, FBI, HDL-C, HOMA-IR, LDL-C, TC, TG, WC, Body weight |
| Cicero, 2020 [36] | DB, RCT | 8 weeks | 40/40 | 54 3 | 27.1 | 800 mg phytosomal curcumin (Curserin®: 200 mg curcumin, 120 mg phosphatidylserine, 480 mg phosphatidylcholine, and 8 mg piperine from Piper nigrum L. dry extract) | The patients were advised to follow the recommendations of the Mediterranean diet. Additionally, they were advised to engage in physical activity by walking briskly for 20–30 min, 3–5 times per week, or by cycling | Patients received a placebo | BMI, DBP, FGB, FBI, HDL-C, HOMA-IR, LDL-C, SBP, TC, TG, WC |
| Kelardeh, 2020 [29] | RCT | 12 weeks | 11/11 | 64.09 3.33 | 27.03 | 80 mg curcumin as a nanomicelle | The nonlinear resistance training program: each session took about 60–70 min for the main training (plus about 20 min for the warm-up and cool-down), three days a week (non-consecutive) which lasted 12 weeks. | Received one placebo capsule per day | ALP, BMI, T Bili, Body weight |
| Parameter | Defined Criteria for the Current Study |
|---|---|
| P (population) | Adult patients with MAFLD |
| I (intervention) | Curcumin supplementation or curcumin supplementation with lifestyle advice (e.g., diet and/or physical activity and/or other lifestyle modifications) |
| C (comparison) | No special comparison criteria |
| O (outcomes) | Changes in biochemical parameters or anthropometric measurements |
| S (study design) | Randomized controlled trial |
| Outcomes | MD | 95% CI | p-Value | I2 |
|---|---|---|---|---|
| ALT (U/L) | −5.3047 | −8.7520, −1.8573 | 0.0026 | 6.0 |
| AST (U/L) | −3.5597 | −5.7556, −1.3638 | 0.0015 | 17.5 |
| FBI (µU/mL) | −1.1430 | −1.5439, −0.7421 | <0.0001 | 9.3 |
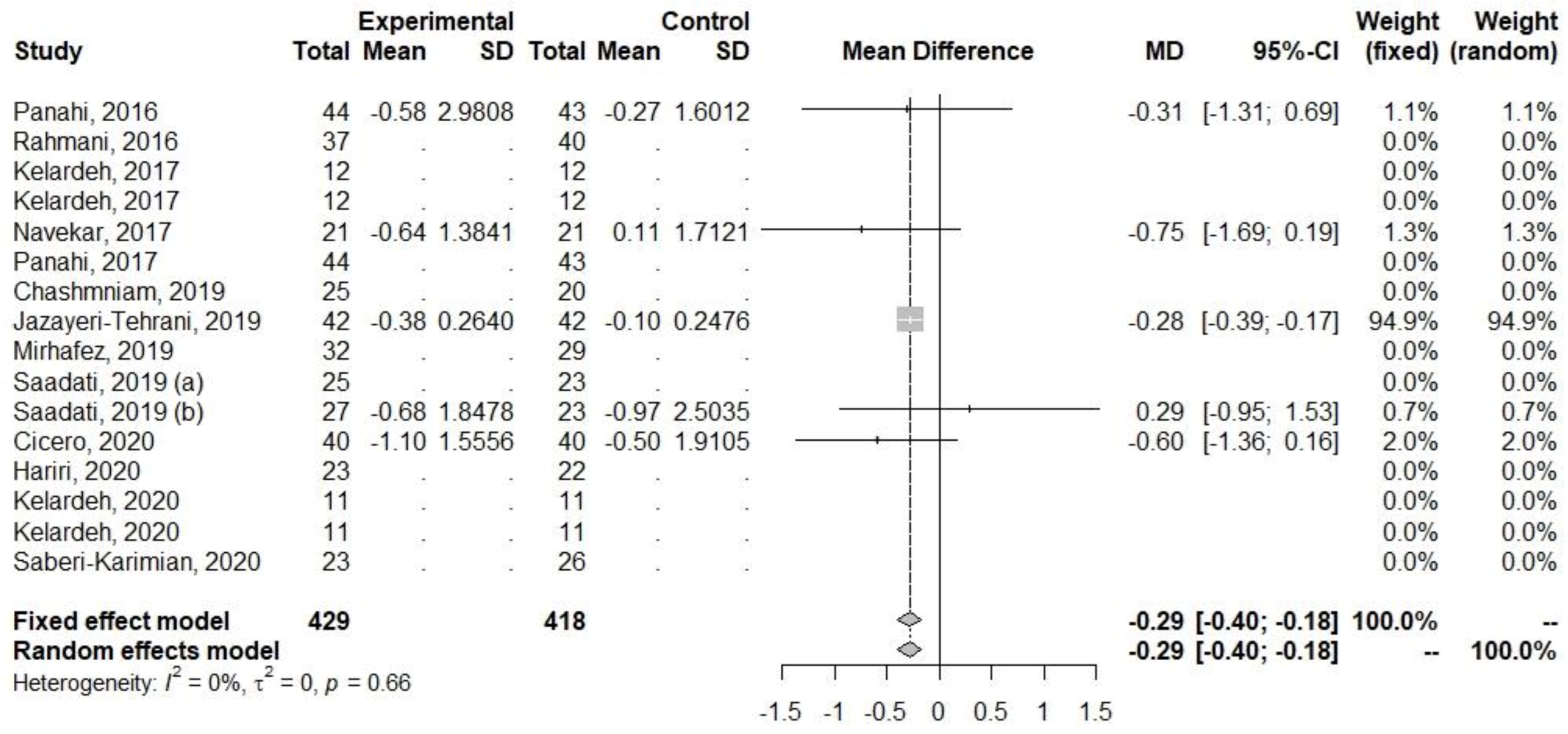
| HOMA-IR | −0.2884 | −0.3950, −0.1817 | <0.0001 | 0 |
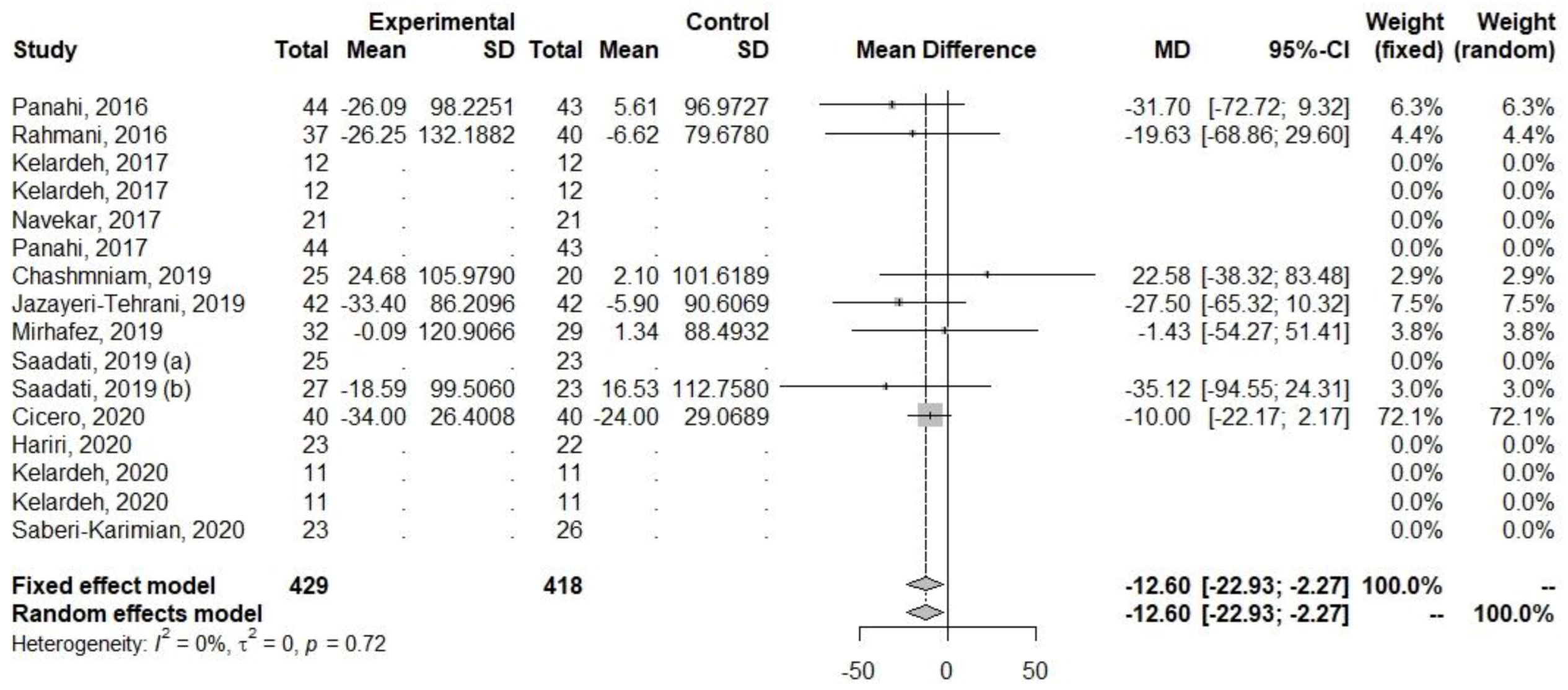
| TG (mg/dL) | −12.6001 | −22.9311, −2.2692 | 0.0168 | 0 |
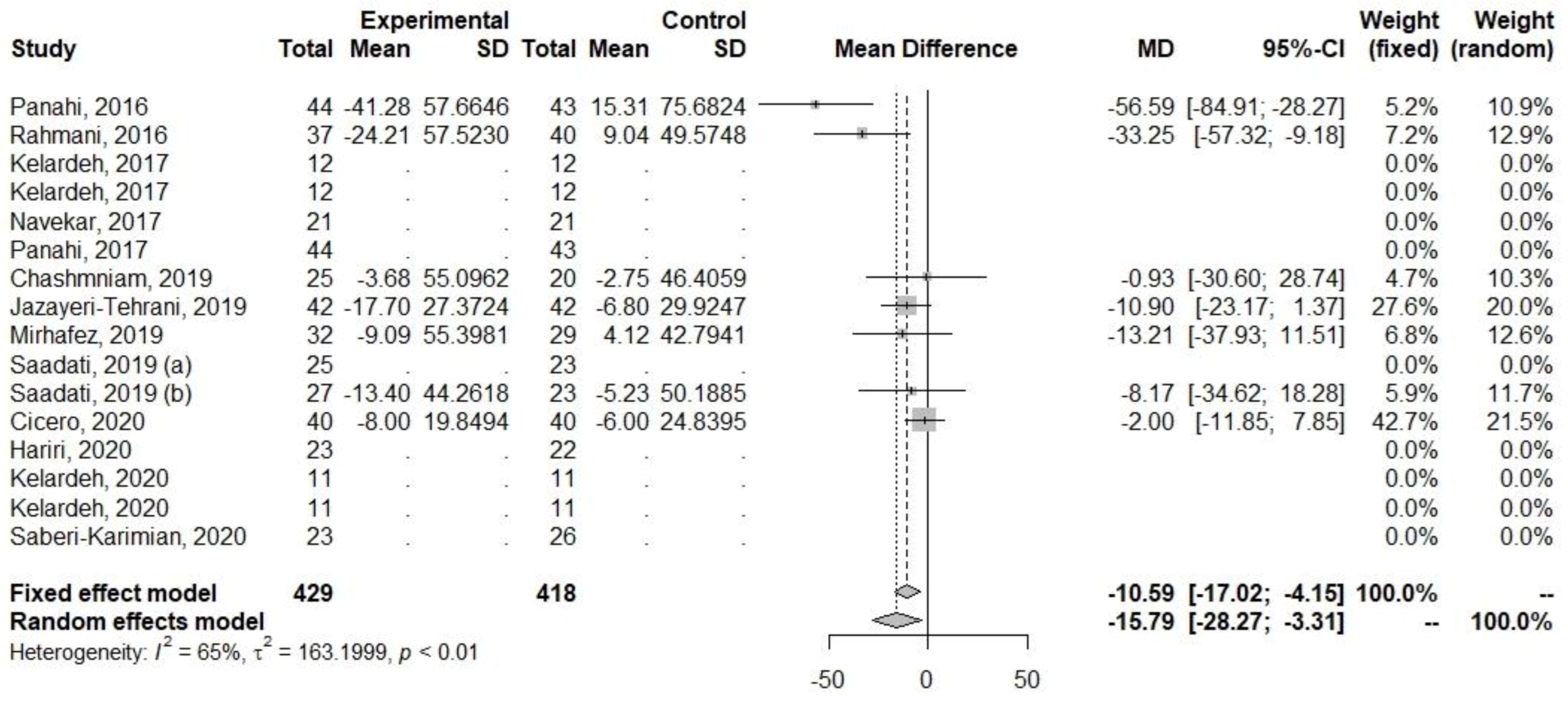
| TC (mg/dL) | −15.7896 | −28.2686, −3.3106 | 0.0131 | 64.6 |
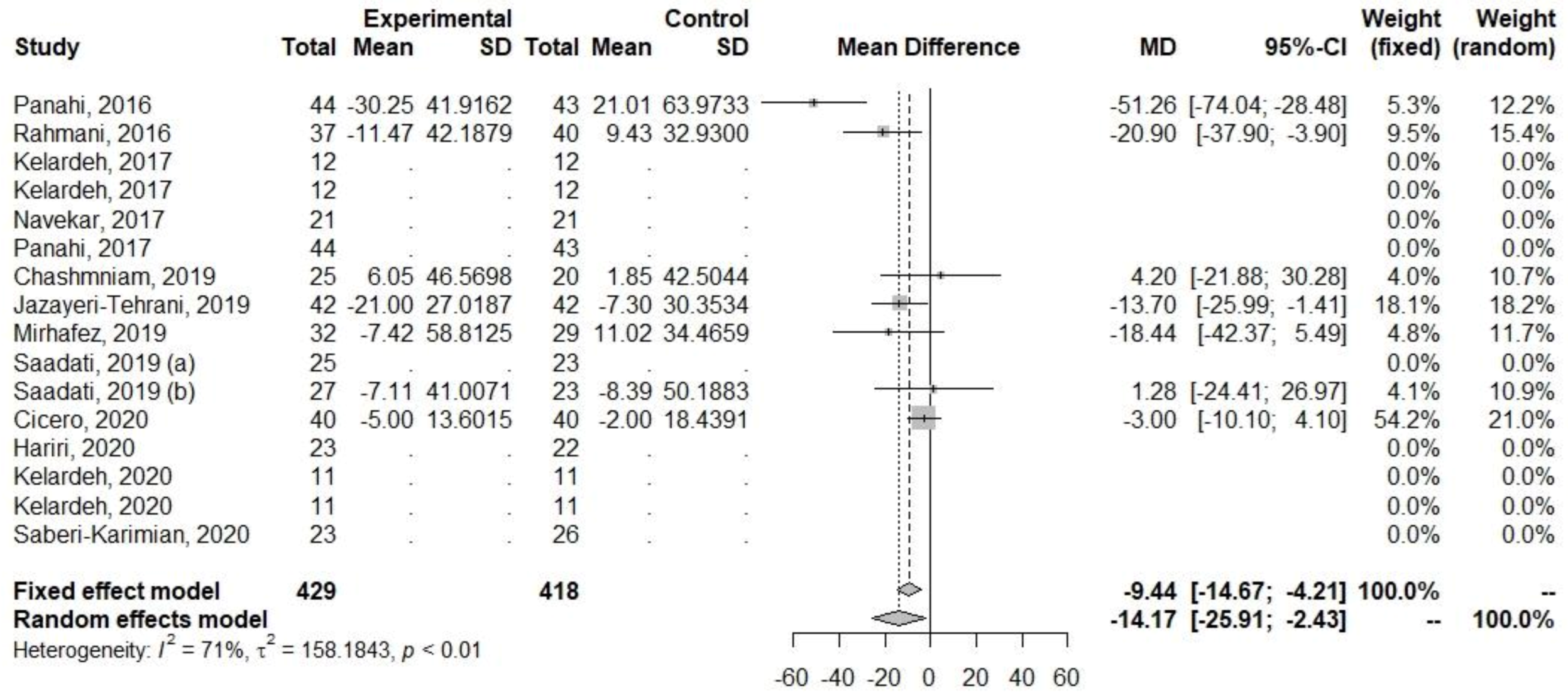
| LDL-C (mg/dL) | −14.1699 | −25.9117, −2.4281 | 0.0180 | 70.8 |
| WC (cm) | −2.6303 | −4.9350, −0.3256 | 0.0253 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Różański, G.; Tabisz, H.; Zalewska, M.; Niemiro, W.; Kujawski, S.; Newton, J.; Zalewski, P.; Słomko, J. Meta-Analysis of Exploring the Effect of Curcumin Supplementation with or without Other Advice on Biochemical and Anthropometric Parameters in Patients with Metabolic-Associated Fatty Liver Disease (MAFLD). Int. J. Environ. Res. Public Health 2023, 20, 4266. https://doi.org/10.3390/ijerph20054266
Różański G, Tabisz H, Zalewska M, Niemiro W, Kujawski S, Newton J, Zalewski P, Słomko J. Meta-Analysis of Exploring the Effect of Curcumin Supplementation with or without Other Advice on Biochemical and Anthropometric Parameters in Patients with Metabolic-Associated Fatty Liver Disease (MAFLD). International Journal of Environmental Research and Public Health. 2023; 20(5):4266. https://doi.org/10.3390/ijerph20054266
Chicago/Turabian StyleRóżański, Gracjan, Hanna Tabisz, Marta Zalewska, Wojciech Niemiro, Sławomir Kujawski, Julia Newton, Paweł Zalewski, and Joanna Słomko. 2023. "Meta-Analysis of Exploring the Effect of Curcumin Supplementation with or without Other Advice on Biochemical and Anthropometric Parameters in Patients with Metabolic-Associated Fatty Liver Disease (MAFLD)" International Journal of Environmental Research and Public Health 20, no. 5: 4266. https://doi.org/10.3390/ijerph20054266
APA StyleRóżański, G., Tabisz, H., Zalewska, M., Niemiro, W., Kujawski, S., Newton, J., Zalewski, P., & Słomko, J. (2023). Meta-Analysis of Exploring the Effect of Curcumin Supplementation with or without Other Advice on Biochemical and Anthropometric Parameters in Patients with Metabolic-Associated Fatty Liver Disease (MAFLD). International Journal of Environmental Research and Public Health, 20(5), 4266. https://doi.org/10.3390/ijerph20054266