

The Other Side of the ACEs Pyramid: A Healing Framework for Indigenous Communities

{kind=link}
Abstract
1. Introduction
2. The ACEs Pyramid and ACEs
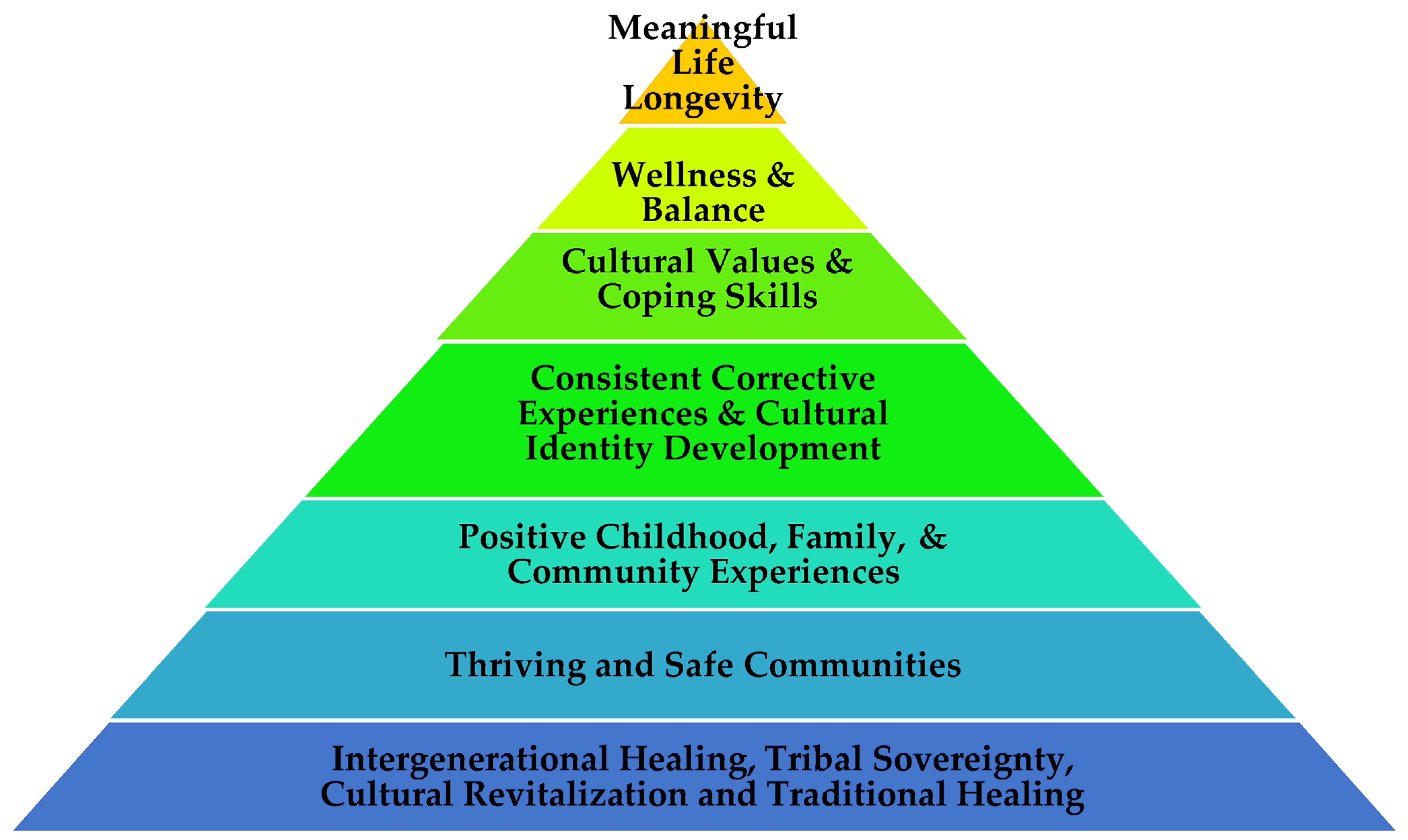
3. The Indigenous Wellness Pyramid
3.1. Historical Trauma—Intergenerational Healing/Indigenous Sovereignty
3.2. Social Conditions/Local Context—Thriving Economic and Safe Communities
3.3. ACEs—Positive Childhood, Family, and Community Experiences
- Positive identity development, family and community belonging.
- Individual pride, family pride, and community pride.
- Self-actualization, family actualization, and community actualization.
3.4. Disrupted Neurodevelopment and Social/Emotional/Cognitive Impairment—Consistent Corrective Experiences and Cultural Identity Development
3.5. Adoption of Health Risk Behaviors—Cultural Values and Coping Skills
3.6. Disease Burden and Social Problems—Wellness and Balance
3.7. Early Death—Meaningful Life Longevity
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. International Day of the World’s Indigenous Peoples. Available online: https://www.un.org/en/observances/indigenous-day/background (accessed on 29 December 2022).
- Gone, J.P.; Hartmann, W.E.; Pomerville, A.; Wendt, D.C.; Klem, S.H.; Burrage, R.L. The impact of historical trauma on health outcomes for Indigenous populations in the USA and Canada: A systematic review. Amer. Psych. 2019, 74, 20–35. [Google Scholar] [CrossRef] [PubMed]
- Duran, E. Healing the Soul Wound: Counseling with American Indians and Other Native Peoples; Teachers College Press: New York, NY, USA, 2006; p. 11. [Google Scholar]
- Gracey, M.; King, M. Indigenous health part 1: Determinants and disease patterns. Lancet 2009, 374, 65–75. [Google Scholar] [CrossRef]
- Kirmayer, L.J.; Brass, G. Addressing global health disparities among Indigenous peoples. Lancet 2016, 388, 105–106. [Google Scholar] [CrossRef]
- Radford, A.; Toombs, E.; Zugic, K.; Boles, K.; Lund, J.; Mushquash, C.J. Examining Adverse Childhood Experiences (ACEs) within Indigenous populations: A systematic review. J. Child Adolesc. Trauma 2022, 15, 401–421. [Google Scholar] [CrossRef] [PubMed]
- Dube, S.R. Twenty years and counting: The past, present, and future of ACEs research. In Adverse Childhood Experiences; Asmundson, G., Afifi, T.O., Eds.; Academic Press: London, UK, 2020; pp. 3–16. [Google Scholar]
- Boullier, M.; Blair, M. Adverse childhood experiences. Paediatr. Child Health 2018, 28, 132–137. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention. About the CDC-Kaiser ACE Study. 2021. Available online: https://www.cdc.gov/violenceprevention/aces/about.html (accessed on 4 December 2022).
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Marks, J.S. Relationship of Childhood Abuse and Household Dysfunction to Many of the Leading Causes of Death in Adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 2019, 56, 774–786. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Zhang, H.; Berlin, K.S.; Levy, M.; Kabra, R. Adverse childhood experiences and childhood obesity: A path analysis approach. Child. Health Care 2020, 49, 247–266. [Google Scholar] [CrossRef]
- LaNoue, M.D.; George, B.J.; Helitzer, D.L.; Keith, S.W. Contrasting cumulative risk and multiple individual risk models of the relationship between Adverse Childhood Experiences (ACEs) and adult health outcomes. BMC Med. Res. Meth. 2020, 20, 239. [Google Scholar] [CrossRef]
- Thompson, M.P.; Kingree, J.B.; Lamis, D. Associations of adverse childhood experiences and suicidal behaviors in adulthood in a US nationally representative sample. Child Care Health Dev. 2019, 45, 121–128. [Google Scholar] [CrossRef]
- Anderson, I.; Robson, B.; Connolly, M.; Al-Yaman, F.; Bjertness, E.; King, A.; Tynan, M.; Madden, R.; Bang, A.; Coimbra, C.E., Jr.; et al. Indigenous and tribal peoples’ health (The Lancet–Lowitja Institute Global Collaboration): A population study. Lancet 2016, 388, 131–157. [Google Scholar] [CrossRef]
- Masten, A.S. Resilience in children threatened by extreme adversity: Frameworks for research, practice, and translational synergy. Dev. Psychopathol. 2011, 23, 493–506. [Google Scholar] [CrossRef]
- Masten, A.S. Pathways to integrated resilience science. Psychol. Inq. 2015, 26, 187–196. [Google Scholar] [CrossRef]
- Masten, A.S. Multisystem Resilience: Pathways to an Integrated Framework. Res. Hum. Dev. 2021, 18, 153–163. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. Available online: https://store.samhsa.gov/sites/default/files/d7/priv/sma15-4420.pdf (accessed on 5 December 2022).
- Paul, G.L. Strategy of Outcome Research in Psychotherapy. J. Consult. Psychol. 1967, 31, 109–118. [Google Scholar] [CrossRef]
- Brave Heart, M.Y.H. The historical trauma response among natives and its relationship with substance abuse: A Lakota illustration. J. Psychoact. Drugs 2003, 35, 7–13. [Google Scholar] [CrossRef]
- Sotero, M. A conceptual model of historical trauma: Implications for public health practice and research. J. Health Disparities Res. Pract. 2006, 1, 93–108. [Google Scholar]
- Mohatt, N.V.; Thompson, A.B.; Thai, N.D.; Tebes, J.K. Historical trauma as public narrative: A conceptual review of how history impacts present-day health. Soc. Sci. Med. 2014, 106, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Shaw, S.L.; Lombardero, A.; Babins-Wagner, R.; Sommers-Flanagan, J. Counseling Canadian Indigenous peoples: The therapeutic alliance and outcome. J. Multicult. Coun. Dev. 2019, 47, 49–68. [Google Scholar] [CrossRef]
- Trautman, A.; Maegan Rides At The Door. Considerations for implementing culturally grounded trauma-informed child welfare services: Recommendations for working with American Indian/Alaska Native populations. J. Public Child Welf. 2019, 13, 368–378. [Google Scholar]
- Asamoah, G.D.; Khakpour, M.; Carr, T.; Groot, G. Exploring Indigenous Traditional Healing programs in Canada, Australia, and New Zealand: A scoping review. Explore 2023, 19, 14–25. [Google Scholar] [CrossRef]
- Pesek, T.J.; Helton, L.R.; Nair, M. Healing across cultures: Learning from traditions. EcoHealth 2006, 3, 114–118. [Google Scholar] [CrossRef]
- Pan, S.Y.; Litscher, G.; Chan, K.; Yu, Z.L.; Chen, H.Q.; Ko, K.M. Traditional medicines in the world: Where to go next? Evid.-Based Comp. Alt. Med. 2014, 2014, 739895. [Google Scholar] [CrossRef] [PubMed]
- Olceri Eco-Ranch. The Eden Model. Olceri Eco-Ranch. Available online: https://www.olceri.org/eden-model (accessed on 29 December 2022).
- Morris, A.S.; Hays-Grudo, J.; Zapata, M.I.; Treat, A.; Kerr, K.L. Adverse and protective childhood experiences and parenting attitudes: The role of cumulative protection in understanding resilience. Advers. Resil. Sci. 2021, 2, 181–192. [Google Scholar] [CrossRef]
- Thornley, L.; Ball, J.; Signal, L.; Lawson-Te Aho, K.; Rawson, E. Building community resilience: Learning from the Canterbury earthquakes. Kotuitui N. Z. J. Soc. Sci. 2015, 10, 23–35. [Google Scholar] [CrossRef]
- Bethell, C.; Jones, J.; Gombojav, N.; Linkenbach, J.; Sege, R. Positive Childhood Experiences and Adult Mental and Relational Health in a Statewide Sample: Associations Across Adverse Childhood Experiences Levels. JAMA Pediatr. 2019, 173, e193007. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.M.; Beck, J.G.; Yasinski, C. A cognitive behavioral perspective on corrective experiences. In Transformation in Psychotherapy: Corrective Experiences across Cognitive Behavioral, Humanistic, and Psychodynamic Approaches; Castonguay, L.G., Hill, C.E., Eds.; American Psychological Association: Washington, DC, USA, 2012; pp. 69–83. [Google Scholar]
- Johnson-Jennings, M.; Billiot, S.; Walters, K. Returning to Our Roots: Tribal Health and Wellness through Land-Based Healing. Genealogy 2020, 4, 91. [Google Scholar] [CrossRef]
- Horowitz, M. Redefining identity after trauma or loss. Psychodyn. Psychiatry 2018, 46, 135–144. [Google Scholar] [CrossRef]
- Siegrist, J.; Rödel, A. Work stress and health risk behavior. Scand. J. Work. Environ. Health 2006, 1, 473–481. [Google Scholar] [CrossRef]
- Waajid, B.; Garner, P.W.; Owen, J.E. Infusing Social Emotional Learning into the Teacher Education Curriculum. Int. J. Emot. Educ. 2013, 5, 31–48. [Google Scholar]
- Leo, D.; Izadikhah, Z.; Fein, E.C.; Forooshani, S.A. The Effect of Trauma on Religious Beliefs: A Structured Literature Review and Meta-Analysis. Trauma Violence Abus. 2021, 22, 161–175. [Google Scholar] [CrossRef]
- Schwalm, F.D.; Zandavalli, R.B.; de Castro Filho, E.D.; Lucchetti, G. Is there a relationship between spirituality/religiosity and resilience? A systematic review and meta-analysis of observational studies. J. Health Psych. 2022, 27, 1218–1232. [Google Scholar] [CrossRef] [PubMed]
- Fijal, D.; Beagan, B.L. Indigenous perspectives on health: Integration with a Canadian model of practice. Can. J. Occup. Ther. 2019, 86, 220–231. [Google Scholar] [CrossRef] [PubMed]
- United Nations: Department of Economic and Social Affairs Indigenous Peoples. Health. Available online: https://www.un.org/development/desa/indigenouspeoples/mandated-areas1/health.html (accessed on 29 December 2022).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rides At The Door, M.; Shaw, S. The Other Side of the ACEs Pyramid: A Healing Framework for Indigenous Communities. Int. J. Environ. Res. Public Health 2023, 20, 4108. https://doi.org/10.3390/ijerph20054108
Rides At The Door M, Shaw S. The Other Side of the ACEs Pyramid: A Healing Framework for Indigenous Communities. International Journal of Environmental Research and Public Health. 2023; 20(5):4108. https://doi.org/10.3390/ijerph20054108
Chicago/Turabian StyleRides At The Door, Maegan, and Sidney Shaw. 2023. "The Other Side of the ACEs Pyramid: A Healing Framework for Indigenous Communities" International Journal of Environmental Research and Public Health 20, no. 5: 4108. https://doi.org/10.3390/ijerph20054108
APA StyleRides At The Door, M., & Shaw, S. (2023). The Other Side of the ACEs Pyramid: A Healing Framework for Indigenous Communities. International Journal of Environmental Research and Public Health, 20(5), 4108. https://doi.org/10.3390/ijerph20054108