
A Systematic Review of Physical Activity Intervention Programs in ASEAN Countries: Efficacy and Future Directions




Abstract
1. Introduction
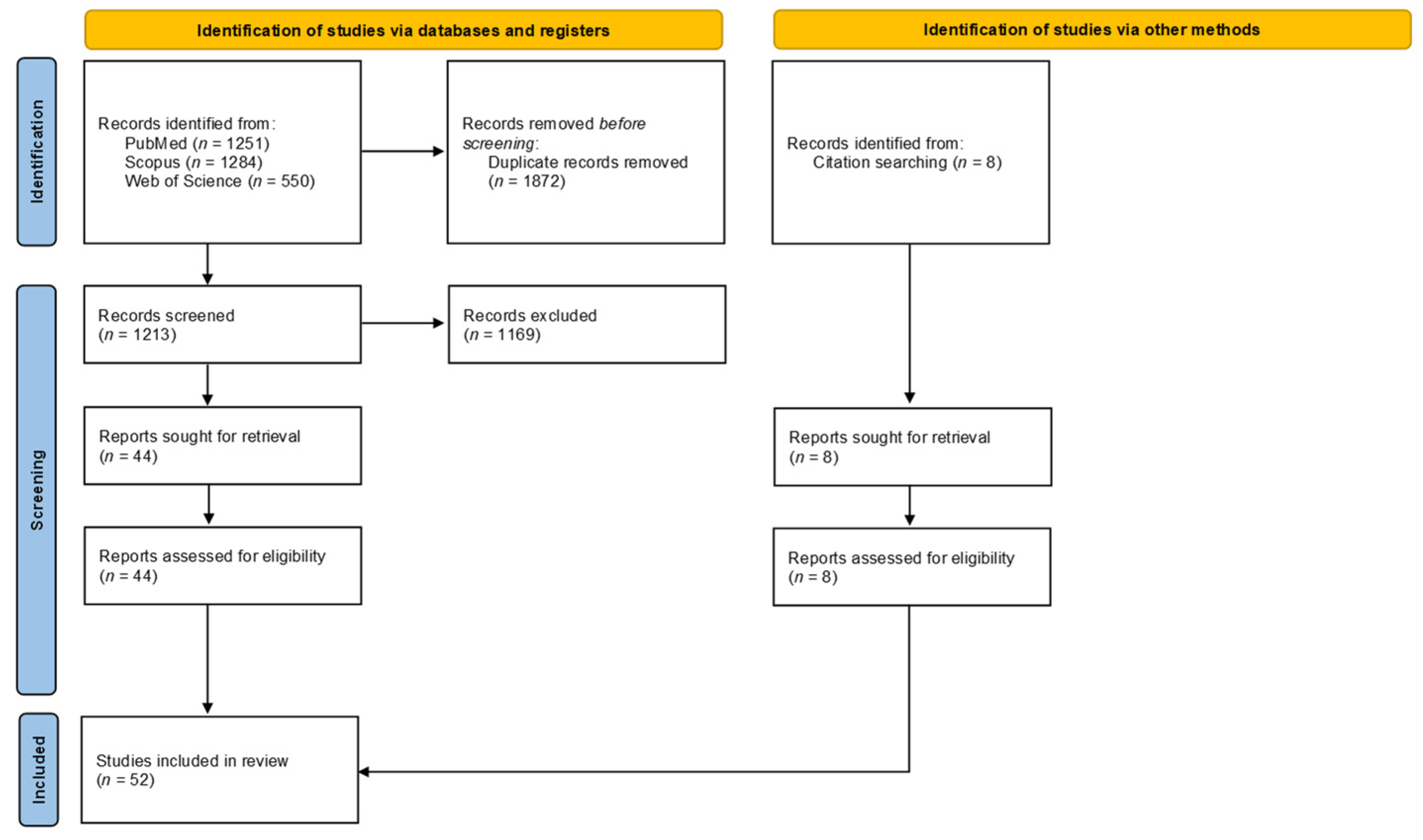
2. Materials and Methods
2.1. Search Process and Inclusion Criteria
- (a)
- P: Individuals of any age; males and females; from ASEAN countries;
- (b)
- I: Any type of intervention that is aimed at influencing PA levels, regardless of whether the intervention is aimed at influencing it as a primary or secondary variable;
- (c)
- C: Placebo;
- (d)
- O: PA level.
- (a)
- Physical Activity; AND
- (b)
- Indonesia OR Philippines OR Malaysia OR Singapore OR Laos OR Brunei OR Myanmar OR Burma OR Thailand OR Cambodia OR Vietnam OR ASEAN OR Southeast Asia; AND
- (c)
- Measurement OR Method OR Survey OR Consensus.
2.2. Quality Assessment and Level of Evidence
2.3. Selection of Outcomes for Review
2.4. Determination of Approach Categories
3. Results
3.1. Informational Approaches
3.1.1. School-Based Informational Provision
Efficacy
Applicability
3.1.2. Hospital-Based Informational Provision
Efficacy
Applicability
3.1.3. Home-Based Informational Provision
Efficacy
Applicability
3.1.4. Community-Wide Campaigns
Efficacy
Applicability
3.1.5. Point-of-Decision Prompts
Efficacy
Applicability
3.2. Behavioural and Social Approaches
3.2.1. Peer Support
Efficacy
Applicability
3.2.2. Incentivised Change
Efficacy
Applicability
3.2.3. Self-Regulation Strategy
Efficacy
Applicability
3.2.4. Individually Adapted Health Behaviour Change Program
Efficacy
Applicability
3.2.5. Family-Based Social Support
Efficacy
Applicability
3.2.6. Workplace-Based Social Support
Efficacy
Applicability
3.2.7. Healthcare Provider Training
Efficacy
Applicability
3.2.8. Self-Monitoring Tools
Efficacy
Applicability
3.3. Direct Approaches
3.3.1. Efficacy
3.3.2. Applicability
4. Discussion
4.1. Overall Efficacy of Reviewed Interventions
4.2. The Need to Account for Local Cultural Considerations in PA Promotion Programs
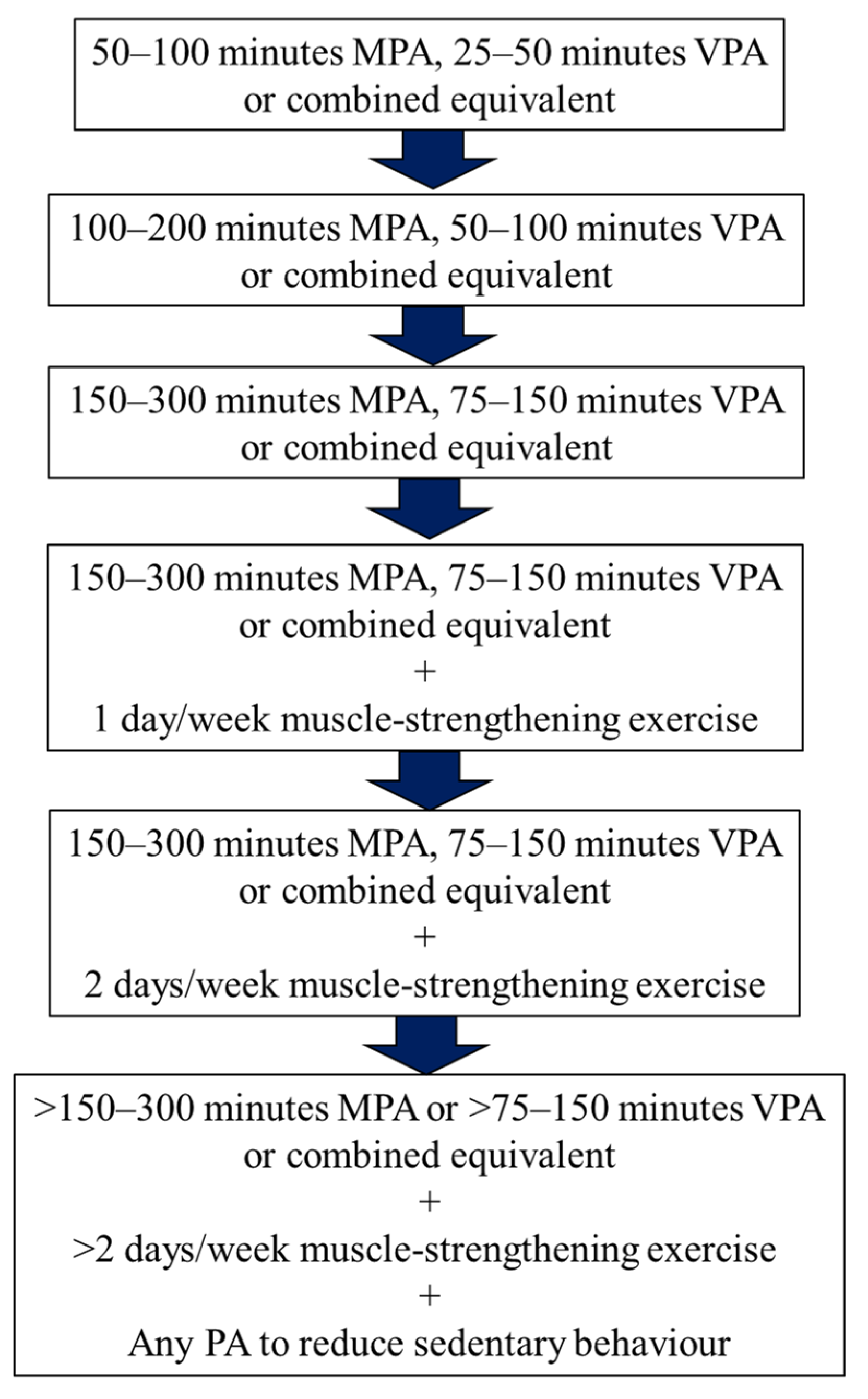
4.3. Towards a Potential Addendum for Local PA Guidelines
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2010. Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 27 August 2021).
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Condello, G.; Ling, F.C.M.; Bianco, A.; Chastin, S.; Cardon, G.; Ciarapica, D.; Conte, D.; Cortis, C.; De Craemer, M.; Di Blasio, A.; et al. Using concept mapping in the development of the EU-PAD framework (EUropean-Physical Activity Determinants across the life course): A DEDIPAC-study. BMC Public Health 2016, 16, 1145. [Google Scholar] [CrossRef]
- Deloitte. A Perspective of Future Healthcare Landscape in ASEAN and Singapore. 2015. Available online: https://www2.deloitte.com/content/dam/Deloitte/sg/Documents/risk/sea-risk-healthcare-3-0-model.pdf (accessed on 27 August 2021).
- World Health Organization. Noncommunicable Diseases in the South-East Asia (N.D.). Available online: https://www.who.int/southeastasia/health-topics/noncommunicable-diseases (accessed on 27 August 2021).
- World Health Organization. Prevalence of Insufficient Physical Activity among Adults, Data by WHO Region. 2018. Available online: https://apps.who.int/gho/data/view.main.2482?lang=en (accessed on 27 August 2021).
- Coughlin, S.S.; Stewart, J. Use of consumer wearable devices to promote physical activity: A review of health intervention studies. J. Environ. Health Sci. 2016, 2, 1–6. [Google Scholar] [CrossRef]
- Kahn, E.B.; Ramsey, L.T.; Brownson, R.C.; Heath, G.W.; Howze, E.H.; Powell, K.E.; Stone, E.J.; Rajab, M.W.; Corso, P. The effectiveness of interventions to increase physical activity: A systematic review. Am. J. Prev. Med. 2002, 22, 73–107. [Google Scholar] [CrossRef]
- Laplante, C.; Peng, W. A Systematic review of e-health interventions for physical activity: An analysis of study design, intervention characteristics, and outcomes. Telemed. E-Health 2011, 17, 509–523. [Google Scholar] [CrossRef]
- Seo, D.-C.; Torabi, M.R.; Jiang, N.; Fernandez-Rojas, X.; Park, B.-H. Correlates of college students’ physical activity: Cross-cultural differences. Asia Pac. J. Public Health 2009, 21, 421–432. [Google Scholar] [CrossRef]
- Araki, K.; Kodani, I.; Gupta, N.; Gill, D.L. Experiences in sport, physical activity, and physical education among Christian, Buddhist, and Hindu Asian adolescent girls. J. Prev. Med. Public Health 2013, 46 (Suppl. S1), S43–S49. [Google Scholar] [CrossRef]
- Aljayyousi, G.F.; Abu Munshar, M.; Al-Salim, F.; Osman, E.R. Addressing context to understand physical activity among Muslim university students: The role of gender, family, and culture. BMC Public Health 2019, 19, 1452. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-S.; Komar, J.; Chia, M. Physical activity measurement methodologies: A systematic review in the association of South East Asian Nations (ASEAN). Sports 2021, 9, 69. [Google Scholar] [CrossRef]
- Barton, S. Which clinical studies provide the best evidence? The best RCT still trumps the best observational study. BMJ 2000, 321, 255–256. [Google Scholar] [CrossRef]
- Nardini, C. The ethics of clinical trials. Ecancermedicalscience 2014, 8, 387. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Hooper, P.; Jutai, J.; Strong, G.; Russell-Minda, E. Age-related macular degeneration and low-vision rehabilitation: A systematic review. Can. J. Ophthalmol. 2008, 43, 180–187. [Google Scholar] [CrossRef]
- OCEBM Levels of Evidence Working Group. The Oxford Levels of Evidence 2. 2011. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 27 August 2021).
- O’Connor, S.R.; Tully, M.; Ryan, B.; Bradley, J.M.; Baxter, G.D.; McDonough, S.M. Failure of a numerical quality assessment scale to identify potential risk of bias in a systematic review: A comparison study. BMC Res. Notes 2015, 8, 224. [Google Scholar] [CrossRef]
- Rizal, H.; Hajar, M.S.; Muhamad, A.S.; Kueh, Y.C.; Kuan, G. The effect of brain breaks on physical activity behaviour among primary school children: A transtheoretical perspective. Int. J. Environ. Res. Public Health 2019, 16, 4283. [Google Scholar] [CrossRef]
- Mok, W.K.H.; Poh, B.K.; Wee, L.H.; Devanthini, D.G.; Ruzita, A.T. Juara sihat: Assessing the sustained impact of a schoolbased obesity intervention. Med. J. Malays. 2018, 73, 100–105. [Google Scholar]
- Chawla, N.; Panza, A.; Sirikulchayanonta, C.; Kumar, R.; Taneepanichskul, S. Effectiveness of a school-based multicomponent intervention on nutritional status among primary school children in Bangkok, Thailand. J. Ayub. Med. Coll. Abbottabad 2017, 29, 13–20. [Google Scholar]
- Lua, P.L.; Wan Dali, W.P.E.; Shahril, M.R. Multimodal nutrition education intervention: A cluster randomised controlled trial study on weight gain and physical activity pattern among university students in Terengganu, Malaysia. Mal. J. Nutr. 2013, 19, 339–352. [Google Scholar]
- Soon, H.K.; Saad, H.A.; Taib, M.N.M.; Rahman, H.A.; Mun, C.Y. Effects of combined physical activity and dietary intervention on obesity and metabolic parameters in adults with abdominal obesity. Southeast Asian J. Trop. Med. Public Health 2013, 44, 295–308. [Google Scholar] [PubMed]
- Teo, C.; Chin, Y.; Lim, P.; Masrom, S.; Shariff, Z. Impacts of a school-based intervention that incorporates nutrition education and a supportive healthy school canteen environment among primary school children in malaysia. Nutrition 2021, 13, 1712. [Google Scholar] [CrossRef] [PubMed]
- Eaton, C.B.; McPhillips, J.B.; Gans, K.M.; Garber, C.E.; Assaf, A.R.; Lasater, T.M.; Carleton, R.A. Cross-sectional relationship between diet and physical activity in two southeastern new England communities. Am. J. Prev. Med. 1995, 11, 238–244. [Google Scholar] [CrossRef]
- Pichayapinyo, P.; Saslow, L.R.; Aikens, J.E.; Marinec, N.; Sillabutra, J.; Rattanapongsai, P.; Piette, J.D. Feasibility study of automated interactive voice response telephone calls with community health nurse follow-up to improve glycaemic control in patients with type 2 diabetes. Int. J. Nurs. Pract. 2019, 25, e12781. [Google Scholar] [CrossRef]
- Cramer, J.A.; Scheyer, R.D.; Mattson, R.H. Compliance declines between clinic visits. Arch. Intern. Med. 1990, 150, 1509–1510. [Google Scholar] [CrossRef] [PubMed]
- Hidrus, A.; Kueh, Y.C.; Norsaádah, B.; Chang, Y.-K.; Hung, T.-M.; Naing, N.N.; Kuan, G. Effects of brain breaks videos on the motives for the physical activity of Malaysians with type-2 diabetes mellitus. Int. J. Environ. Res. Public Health 2020, 17, 2507. [Google Scholar] [CrossRef]
- Suttanon, P.; Piriyaprasarth, P.; Krootnark, K.; Aranyavalai, T. Effectiveness of falls prevention intervention programme in community-dwelling older people in Thailand: Randomized controlled trial. Hong Kong Physiother. J. 2018, 38, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Yatim, H.M.; Wong, Y.Y.; Lim, S.H.; Hassali, M.A.; Hong, Y.H.; Dali, A.F.; Neoh, C.F. Evaluation of a group-based hypertension self-management education programme among hypertensive community dwellers. Eur. J. Integr. Med. 2018, 24, 79–84. [Google Scholar] [CrossRef]
- Juliana, N.; Shahar, S.; Sahar, M.A.; Ghazali, A.R.; Manaf, Z.A.; Noah, R.M. ‘Her Shape’ intervention programme for obese women with high breast adiposity. Asia Pac. J. Clin. Nutr. 2017, 26, 278–286. [Google Scholar] [CrossRef]
- Ethisan, P.; Chapman, R.; Kumar, R.; Somrogthong, R. Effectiveness of group-mediated lifestyle physical activity (Glpa) program for health benefit in physical activity among elderly people at rural thailand. J. Ayub. Med. Coll. Abbottabad 2015, 27, 292–295. [Google Scholar] [PubMed]
- Ngo, C.S.; Pan, C.-W.; Finkelstein, E.A.; Lee, C.-F.; Wong, I.B.; Ong, J.; Ang, M.; Wong, T.-Y.; Saw, S.-M. A cluster randomised controlled trial evaluating an incentive-based outdoor physical activity programme to increase outdoor time and prevent myopia in children. Ophthalmic Physiol. Opt. 2014, 34, 362–368. [Google Scholar] [CrossRef]
- Finkelstein, E.A.; Tan, Y.-T.; Malhotra, R.; Lee, C.-F.; Goh, S.-S.; Saw, S.-M. A cluster randomized controlled trial of an incentive-based outdoor physical activity program. J. Pediatr. 2013, 163, 167–172.e1. [Google Scholar] [CrossRef]
- Tan, M.Y.; Magarey, J.M.; Chee, S.S.; Lee, L.F. A brief structured education programme enhances self-care practices and improves glycaemic control in Malaysians with poorly controlled diabetes. Health Educ. Res. 2011, 26, 896–907. [Google Scholar] [CrossRef]
- Müller, A.M.; Khoo, S.; Morris, T. Text messaging for exercise promotion in older adults from an upper-middle-income country: Randomized controlled trial. J. Med. Internet Res. 2016, 18, e5. [Google Scholar] [CrossRef]
- Tran, V.D.; James, A.P.; Lee, A.H.; Jancey, J.; Howat, P.A.; Mai, L.T.P. Effectiveness of a community-based physical activity and nutrition behavior intervention on features of the metabolic syndrome: A cluster-randomized controlled trial. Metab. Syndr. Relat. Disord. 2017, 15, 63–71. [Google Scholar] [CrossRef]
- Ibrahim, N.; Moy, F.M.; Awalludin, I.A.N.; Ali, Z.M.; Ismail, I.S. Effects of a community-based healthy lifestyle intervention program (Co-HELP) among adults with prediabetes in a developing country: A quasi-experimental study. PLoS ONE 2016, 11, e0167123. [Google Scholar] [CrossRef]
- Nguyen, Q.N.; Pham, S.T.; Nguyen, V.L.; Weinehall, L.; Wall, S.; Bonita, R.; Byass, P. Effectiveness of community-based comprehensive healthy lifestyle promotion on cardiovascular disease risk factors in a rural Vietnamese population: A quasi-experimental study. BMC Cardiovasc. Disord. 2012, 12, 56. [Google Scholar] [CrossRef]
- Juniarti, N.; Mz, I.A.; Sari, C.W.M.; Haroen, H. The effect of exercise and learning therapy on cognitive functions and physical activity of older people with dementia in indonesia. J. Aging Res. 2021, 2021, 6647029. [Google Scholar] [CrossRef]
- Soler, R.E.; Leeks, K.D.; Buchanan, L.R.; Brownson, R.C.; Heath, G.W.; Hopkins, D.H. Point-of-decision prompts to increase stair use. Am. J. Prev. Med. 2010, 38, S292–S300. [Google Scholar] [CrossRef]
- Chee Huei, P.; Saad, H.A.; Barakatun Nisak, M.Y.; Mohd Nasir, M.T. Effectiveness of physical activity intervention among government employees with metabolic syndrome. J. Exerc. Sci. Fit. 2017, 15, 55–62. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K.; Jayasvasti, I.; Aekplakorn, W.; Puckpinyo, A.; Nanthananate, P.; Mansin, A. Two-year results of a community-based randomized controlled lifestyle intervention trial to control prehypertension and/or prediabetes in Thailand: A brief report. Int. J. Gen. Med. 2019, 12, 131–135. [Google Scholar] [CrossRef]
- Nguyen, H.L.; Ha, D.A.; Goldberg, R.J.; Kiefe, C.I.; Chiriboga, G.; Ly, H.N.; Nguyen, C.K.; Phan, N.T.; Vu, N.C.; Nguyen, Q.P. Culturally adaptive storytelling intervention versus didactic intervention to improve hypertension control in Vietnam- 12 month follow up results: A cluster randomized controlled feasibility trial. PLoS ONE 2018, 13, e0209912. [Google Scholar] [CrossRef]
- Yaacob, L.H.; Azidah, A.K. Pedometer-based walking intervention with and without group support among sedentary adults in primary care patients in north-east Malaysia: A randomized controlled trial. Bangladesh J. Med. Sci. 2018, 17, 52–57. [Google Scholar] [CrossRef]
- Sanee, A.; Somrongthong, R.; Plianbangchang, S. The positive effects of a peer-led intervention system for individuals with a risk of metabolic syndrome. J. Multidiscip. Healthc. 2017, 10, 293–300. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Finkelstein, E.A.; Haaland, B.A.; Bilger, M.; Sahasranaman, A.; Sloan, R.A.; Nang EE, K.; Evenson, K.R. Effectiveness of activity trackers with and without incentives to increase physical activity (TRIPPA): A randomised controlled trial. Lancet Diabetes Endocrinol. 2016, 4, 983–995. [Google Scholar] [CrossRef]
- Bilger, M.; Shah, M.; Tan, N.C.; Tan, C.Y.L.; Bundoc, F.G.; Bairavi, J.; Finkelstein, E.A. Process- and outcome-based financial incentives to improve self-management and glycemic control in people with type 2 diabetes in Singapore: A randomized controlled trial. Patient 2021, 14, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Chew, L.; Tavitian-Exley, I.; Lim, N.; Ong, A. Can a multi-level intervention approach, combining behavioural disciplines, novel technology and incentives increase physical activity at population-level? BMC Public Health 2021, 21, 120. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Vohs, K.D. Understanding self-regulation: An introduction. In Handbook of Self-Regulation: Research, Theory, and Applications, 1st ed.; Guilford Press: New York, NY, USA, 2004; p. 1. [Google Scholar]
- Liau, A.K.; Neihart, M.; Teo, C.T.; Goh, L.S.; Chew, P. A Quasi-experimental study of a fitbit-based self-regulation intervention to improve physical activity, well-being, and mental health. Cyberpsychology Behav. Soc. Netw. 2018, 21, 727–734. [Google Scholar] [CrossRef]
- Marquardt, M.K.; Oettingen, G.; Gollwitzer, P.M.; Sheeran, P.; Liepert, J. Mental contrasting with implementation intentions (MCII) improves physical activity and weight loss among stroke survivors over one year. Rehabil. Psychol. 2017, 62, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective techniques in healthy eating and physical activity interventions: A meta-regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Prochaska, J.O.; DiClemente, C.C. The Transtheoretical Approach: Crossing Traditional Boundaries of Change; Dorsey Press: Homewood, IL, USA, 1984. [Google Scholar]
- Karintrakul, S.; Angkatavanich, J. A randomized controlled trial of an individualized nutrition counseling program matched with a transtheoretical model for overweight and obese females in Thailand. Nutr. Res. Pract. 2017, 11, 319–326. [Google Scholar] [CrossRef]
- Sazlina, S.-G.; Browning, C.J.; Yasin, S. Effectiveness of personalized feedback alone or combined with peer support to improve physical activity in sedentary older Malays with type 2 diabetes: A randomized controlled trial. Front. Public Health 2015, 3, 178. [Google Scholar] [CrossRef]
- Suwanpasu, S.; Aungsuroch, Y.; Jitapanya, C. Post-surgical physical activity enhancing program for elderly patients after hip fracture: A randomized controlled trial. Asian Biomed. 2014, 8, 525–532. [Google Scholar] [CrossRef]
- Muda, S.H.; Kadir, A.A. The effectiveness of physical activity counselling in Primary Care Clinic University Science Malaysia Hospital. Int. Med. J. 2006, 13, 249–253. [Google Scholar]
- Haya, M.; Mexitalia, M.; Margawati, A. Effect of maternal health education on physical activity and body mass index of overweight children. Paediatr. Indones. 2016, 56, 73–78. [Google Scholar] [CrossRef][Green Version]
- Huynh, D.T.T.; Estorninos, E.; Capeding, R.Z.; Oliver, J.S.; Low, Y.L.; Rosales, F.J. Longitudinal growth and health outcomes in nutritionally at-risk children who received long-term nutritional intervention. J. Hum. Nutr. Diet. 2015, 28, 623–635. [Google Scholar] [CrossRef] [PubMed]
- Wafa, S.W.; Talib, R.A.; Hamzaid, N.H.; McColl, J.; Rajikan, R.; Ng, L.O.; Ramli, A.H.; Reilly, J.J. Randomized controlled trial of a good practice approach to treatment of childhood obesity in Malaysia: Malaysian Childhood Obesity Treatment Trial (MASCOT). Pediatr. Obes. 2011, 6, e62–e69. [Google Scholar] [CrossRef][Green Version]
- Maphong, R.; Nakhonket, K.; Sukhonthasab, S. The effectiveness of two levels of active office interventions to reduce sedentary behavior in office workers: A mixed-method approach. Arch. Environ. Occup. Health 2021, 1–10. [Google Scholar] [CrossRef]
- Zahtamal, Z.; Rochmah, W.; Prabandari, Y.S.; Setyawati, L.K. Effects of multilevel intervention in workplace health promotion on workers’ metabolic syndrome components. Kesmas: Natl. Public Health J. 2017, 11, 198. [Google Scholar] [CrossRef]
- Jafar, T.H.; Tan, N.C.; Allen, J.C.; Pradhan, S.S.; Goh, P.; Tavajoh, S.; Keng, F.M.; Chan, J. Management of hypertension and multiple risk factors to enhance cardiovascular health—A feasibility study in Singapore polyclinics. BMC Health Serv. Res. 2016, 16, 229. [Google Scholar] [CrossRef]
- Bice, M.R.; Ball, J.W.; McClaren, S. Technology and physical activity motivation. J. Sport Exerc. Psychol. 2016, 14, 295–304. [Google Scholar] [CrossRef]
- Duncan, M.; Birch, S.; Woodfield, L. Efficacy of an integrated school curriculum pedometer intervention to enhance physical activity and to reduce weight status in children. Eur. Phys. Educ. Rev. 2012, 18, 396–407. [Google Scholar] [CrossRef]
- Zulkifli, A.F. Student-centered approach and alternative assessments to improve students’ learning domains during health education sessions. Biomed. Hum. Kinet. 2019, 11, 80–86. [Google Scholar] [CrossRef]
- Lim, S.L.; Ong, K.W.; Johal, J.; Han, C.Y.; Yap, Q.V.; Chan, Y.H.; Chooi, Y.C.; Zhang, Z.P.; Chandra, C.C.; Thiagarajah, A.G.; et al. Effect of a smartphone App on weight change and metabolic outcomes in Asian adults with type 2 diabetes. JAMA Netw. Open 2021, 4, e2112417. [Google Scholar] [CrossRef] [PubMed]
- Petrunoff, N.; Yao, J.; Sia, A.; Ng, A.; Ramiah, A.; Wong, M.; Han, J.; Tai, B.C.; Uijtdewilligen, L.; Müller-Riemenschneider, F. Activity in nature mediates a park prescription intervention’s effects on physical activity, park use and quality of life: A mixed-methods process evaluation. BMC Public Health 2021, 21, 204. [Google Scholar] [CrossRef] [PubMed]
- Bin Saad, M.F.; Cheah, W.L.; Hazmi, H. The effects of a 7000-step goal and weekly group walking program for overweight and obese elderly people in Sarawak, Malaysia: A quasi-experimental study. J. Prev. Med. Public Health 2021, 54, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Cheah, W.L.; Chang, C.T.; Helmy, H.; Wan Manan, W.M. An intervention based on the stages of change, health profiles and physical activity levels of overweight and obese adults In Sarawak, Malaysia—A feasibility study. Malays. Fam. Physician 2019, 14, 46–54. [Google Scholar]
- Yahya, N.S.R.N.; Jamaludin, F.I.C.; Firdaus, M.K.Z.H.; Hasan, M.K.C. A feasibility of simulation-based exercise programme for overweight adult in higher learning institutions. Enfermería Clínica 2019, 29, 521–527. [Google Scholar] [CrossRef]
- Widyastuti, K.; Makhabah, D.; Setijadi, A.; Sutanto, Y.; Suradi; Ambrosino, N. Benefits and costs of home pedometer assisted physical activity in patients with COPD. A preliminary randomized controlled trial. Pulmonology 2018, 24, 211–218. [Google Scholar] [CrossRef]
- Chia, M. Play reconsidered, resurrected and repositioned in children: Case study results from Singapore. Sport Sci. 2009, 1, 44–48. [Google Scholar]
- Omar, A.; Husain, M.N.; Jamil, A.T.; Nor, N.S.M.; Ambak, R.; Fazliana, M.; Zamri, N.L.A.; Aris, T. Effect of physical activity on fasting blood glucose and lipid profile among low income housewives in the MyBFF@home study. BMC Women’s Health 2018, 18, 103. [Google Scholar] [CrossRef] [PubMed]
- Nhung, B.T.; Tuyen, L.D.; Linh, V.A.; Nguyen, D.V.; Nga, T.T.; Thuc, V.T.; Yui, K.; Ito, Y.; Nakashima, Y.; Yamamoto, S. Rice bran extract reduces the risk of atherosclerosis in post-menopausal Vietnamese women. J. Nutr. Sci. Vitaminol. 2016, 62, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, physical, cognitive, and combination interventions and frailty reversal among older adults: A randomized controlled trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef]
- Hadju, V.; Stephenson, L.S.; Mohammed, H.O.; Bowman, D.D.; Parker, R.S. Improvements of growth, appetite, and physical activity in helminth-infected schoolboys 6 months after single dose of albendazole. Asia Pacific J. Clin. Nutr. 1998, 7, 170–176. [Google Scholar]
- EENI Global Business School. ASEAN Religious Diversity. Strength or Threat? (n.d.). Available online: http://en.reingex.com/ASEAN-Religion.shtml#:%7E:text=About%2042%25%20of%20the%20ASEAN,%25)%20and%20Christianity%20(17%25) (accessed on 27 August 2021).
- Nakamura, Y. Beyond the hijab: Female Muslims and physical activity. Women Sport Phys. Act. J. 2002, 11, 21–48. [Google Scholar] [CrossRef]
- Zaman, H. Islam, well-being and physical activity: Perceptions of Muslim young women. In Researching Women and Sport; Clarke, G., Humberstone, B., Eds.; Palgrave Macmillan: London, UK, 1997; pp. 50–67. [Google Scholar]
- Kahan, D. Islam and physical activity: Implications for American sport and physical educators. J. Phys. Educ. Recreat. Dance 2003, 74, 48–54. [Google Scholar] [CrossRef]
- International Labour Organization. Labor Force Participation Rate, Female (% of Female Population Ages 15+) (Modeled ILO Estimate)|Data. 2021. Available online: https://data.worldbank.org/indicator/SL.TLF.CACT.FE.ZS (accessed on 27 August 2021).
- Erez, M.; Zidon, I. Effect of goal acceptance on the relationship of goal difficulty to performance. J. Appl. Psychol. 1984, 69, 69–78. [Google Scholar] [CrossRef]
- World Health Organisation. Every Move Counts Towards Better Health—Says WHO. 2020. Available online: https://www.who.int/news/item/25-11-2020-every-move-counts-towards-better-health-says-who (accessed on 27 August 2021).



{kind=link}
{kind=link}
| Article | OCEBM Level 1 | R 2 | EV 3 | IV:B 4 | IV:C 5 | P 6 | Total 7 |
|---|---|---|---|---|---|---|---|
| Bilger et al., 2021 | 2 | 8 | 3 | 5 | 6 | 0 | 22 |
| Chew et al., 2021 | 3 | 7 | 2 | 5 | 3 | 1 | 18 |
| Juniarti et al., 2021 | 2 | 8 | 3 | 5 | 4 | 1 | 21 |
| Lim et al., 2021 | 2 | 8 | 3 | 5 | 6 | 1 | 23 |
| Maphonga et al., 2021 | 3 | 7 | 2 | 5 | 1 | 1 | 16 |
| Petrunoff et al., 2021 | 2 | 8 | 3 | 5 | 4 | 0 | 20 |
| Saad et al., 2021 | 3 | 8 | 3 | 5 | 1 | 1 | 18 |
| Teo et al., 2021 | 3 | 7 | 3 | 5 | 1 | 1 | 17 |
| Hidrus et al., 2020 | 2 | 9 | 1 | 7 | 4 | 0 | 21 |
| Cheah et al., 2019 | 3 | 8 | 1 | 4 | 2 | 0 | 15 |
| Nik Yahya et al., 2019 | 3 | 7 | 1 | 3 | 2 | 0 | 13 |
| Pengpid et al., 2019 | 2 | 7 | 1 | 3 | 4 | 0 | 15 |
| Pichayapinyo et al., 2019 | 3 | 7 | 1 | 3 | 2 | 0 | 13 |
| Rizal et al., 2019 | 3 | 8 | 1 | 5 | 2 | 0 | 16 |
| Zulkifi et al., 2019 | 3 | 6 | 1 | 3 | 2 | 0 | 12 |
| Liau et al., 2018 | 3 | 9 | 1 | 3 | 3 | 0 | 16 |
| Mok et al., 2018 | 3 | 8 | 1 | 4 | 2 | 1 | 16 |
| Nguyen et al., 2018 | 3 | 9 | 2 | 5 | 0 | 0 | 16 |
| Nur Emilia et al., 2018 | 2 | 9 | 1 | 4 | 3 | 1 | 18 |
| Omar et al., 2018 | 3 | 8 | 1 | 3 | 1 | 0 | 13 |
| Suttanon et al., 2018 | 2 | 9 | 1 | 7 | 5 | 1 | 23 |
| Widyastuti et al., 2018 | 2 | 9 | 1 | 5 | 4 | 1 | 20 |
| Yatim et al., 2018 | 3 | 7 | 1 | 4 | 2 | 1 | 15 |
| Chawla et al., 2017 | 3 | 8 | 1 | 4 | 2 | 0 | 15 |
| Huei et al., 2017 | 2 | 8 | 1 | 4 | 3 | 0 | 16 |
| Juliana et al., 2017 | 2 | 8 | 1 | 4 | 4 | 1 | 18 |
| Karintrakul et al., 2017 | 2 | 8 | 1 | 3 | 4 | 0 | 16 |
| Sanee et al., 2017 | 3 | 7 | 1 | 4 | 0 | 1 | 13 |
| Tran et al., 2017 | 2 | 7 | 1 | 4 | 3 | 0 | 15 |
| Zahtamal et al., 2017 | 3 | 7 | 1 | 4 | 2 | 0 | 14 |
| Finkelstein et al., 2016 | 2 | 6 | 1 | 6 | 5 | 1 | 19 |
| Haya et al., 2016 | 3 | 8 | 1 | 4 | 3 | 1 | 17 |
| Ibrahim et al., 2016 | 3 | 9 | 1 | 4 | 3 | 1 | 18 |
| Jafar et al., 2016 | 3 | 9 | 1 | 5 | 2 | 0 | 17 |
| Müller-Riemenschneider et al., 2016 | 2 | 9 | 2 | 6 | 5 | 1 | 23 |
| Nhung et al., 2016 | 2 | 7 | 1 | 5 | 3 | 0 | 16 |
| Ethisan et al., 2015 | 3 | 8 | 2 | 4 | 3 | 0 | 17 |
| Huynh et al., 2015 | 3 | 8 | 1 | 5 | 3 | 0 | 17 |
| Ng et al., 2015 | 2 | 8 | 1 | 6 | 6 | 1 | 22 |
| Sazlina et al., 2015 | 2 | 10 | 1 | 6 | 6 | 1 | 24 |
| Ngo et al., 2014 | 2 | 8 | 1 | 5 | 5 | 0 | 19 |
| Sriramatr et al., 2014 | 2 | 6 | 1 | 4 | 5 | 1 | 17 |
| Suwanpasu et al., 2014 | 2 | 6 | 1 | 3 | 3 | 1 | 14 |
| Finkelstein et al., 2013 | 2 | 9 | 1 | 6 | 5 | 0 | 21 |
| Lua et al., 2013 | 2 | 9 | 1 | 3 | 4 | 1 | 18 |
| Soon et al., 2013 | 2 | 9 | 1 | 4 | 2 | 0 | 16 |
| Nguyen et al., 2012 | 3 | 7 | 2 | 4 | 1 | 0 | 14 |
| Tan et al., 2011 | 2 | 8 | 1 | 5 | 3 | 1 | 18 |
| Wafa et al., 2011 | 2 | 7 | 1 | 5 | 3 | 1 | 17 |
| Chia, 2009 | 3 | 3 | 1 | 5 | 2 | 0 | 11 |
| Muda et al., 2006 | 2 | 8 | 1 | 4 | 3 | 1 | 17 |
| Hadju et al., 1998 | 2 | 8 | 0 | 5 | 2 | 0 | 15 |
| Paper | Population 1 | Intervention | Results 2 |
|---|---|---|---|
| Bilger et al., 2021 | n = 240 Singapore Adults M/F Type 2 diabetes | All participants received usual care. There was one control group, one process-based incentive group, and one outcome-based incentive group. The process-based incentive participants earned financial incentives contingent on meeting specified intermediary health behaviours. The outcome-based incentive participants earned financial incentives contingent on meeting certain health behaviour outcomes. The intervention ran for 6 months. | Incentive groups’ mean number of physically active days during the last week of intervention was higher compared to the control group (2.35 vs. 1.24). |
| Chew et al., 2021 | n = 129,677 to 690,233 Singapore Adults M/F | Participants were given fitness trackers. Financial incentives were given to participants for hitting certain daily step goals. There were 3 waves of varying durations. | For all 3 waves, there was an increase in mean daily steps from baseline to the end of the intervention. Wave 1 (4512 to 8675), Wave 2 (6221 to 8463) and Wave 3 (7432 to 9077). |
| Juniarti et al., 2021 | n = 90 Indonesia Older adults M/F | Intervention group participants engaged in reading activities, listening, writing, drawing and exercise activities across a span of 4 weeks. Sessions were led by community volunteers. | The intervention group increased PA from 18.56 to 19.71 (PASE), while the control group did not increase PA. |
| Lim et al., 2021 | n = 204 Singapore Adults; older adults M/F | Participants assigned to the intervention group were required to use the app for 6 months to track weight twice weekly and diet and physical activity daily, and to communicate regularly with the research dietitians via the app. Intervention participants chose a weight loss goal and were encouraged to achieve both nutritional and PA goals. | Change in PA (min/wk) was higher in the intervention group compared to the control group by 53.4 and 62.4 at the 3-month and 6-month marks, respectively. |
| Maphong et al., 2021 | n = 78 Thailand Adults M/F | Participants in the intervention group were involved in sedentary behaviour-reducing activities over 8 weeks. At the individual level, participants were given information and at the organisational level, the physical and social environments of the organisation were adjusted. | Increase in METs for the intervention group (1.03 to 1.17), while there was no change for the control group. |
| Petrunoff et al., 2021 | n = 160 Singapore Adults M/F | Participants in the intervention group received face-to-face counselling on PA, during which they also completed a park prescription sheet with a trained study team member for 26 weeks. The prescription sheet outlined a goal they committed to specifying the frequency, intensity, time and location of exercise in parks. Participants subsequently received a sheet to plan their weekly park PA and information brochures about parks in their neighbourhood. | The amount of park PA (min/month) had a significant mediating effect on recreational MVPA (min/wk) at 26.50 [6.65, 49.37]. |
| Saad et al., 2021 | n = 128 Malaysia Older adults M/F | Participants in the intervention group were given pedometers for daily feedback for the 12-week intervention. | Number of daily steps increased from 3403 to 6975 for the intervention group, while there was no significant change in the control group. |
| Teo et al., 2021 | n = 582 Malaysia Children M/F | The 3-month intervention consisted of delivering nutrition education to the children through their teachers, providing the children with some exercise equipment, training the canteen food handlers to prepare a healthy menu. | PA score (PAQ-C) in the intervention group increased by 0.37 from baseline to post-intervention and increased by 0.18 from baseline to 3-month post-intervention, while there was no significant change in the control group. |
| Hidrus et al., 2020 | n = 70 Malaysia Adults M/F Type 2 diabetes | Brain breaks, 10-min exercise videos were uploaded to a WhatsApp group for the individuals in the intervention group to complete for 4 months. | The intervention group displayed a higher mean total PA compared to the control group across all time points (IPAQ-M). |
| Cheah et al., 2019 | n = 155 Malaysia Adults M/F | Intervention groups were assigned weekly 90-min aerobic exercise sessions for 6 months. | No significant findings with regards to PA data. |
| Nik Yahya et al., 2019 | n = 52 Indonesia Adults M/F | Intervention groups were assigned 3 times per week of 25-min aerobic exercise sessions for 10 weeks. | Significant increase in total PA (IPAQ) with intervention. Pre-intervention = 811.00 (648.50). Post-intervention = 1431.00 (459.00). No significant increase in the control group. |
| Pengpid et al., 2019 | n = 375 Thailand Adults M/F Pre-hypertension, pre-diabetes | The intervention group underwent 6 group lifestyle counselling sessions over a period of 6 months. | No significant findings with regards to PA data. |
| Pichayapinyo et al., 2019 | n = 35 Thailand Adults M/F Type 2 diabetes | Participants attended a 1-h group diabetes education session and received weekly 5 to 10-min interactive voice response calls for 12 weeks. | Pre-post changes in PA were significant with a mean increase of 0.7 (1.3) points out of 6 on the L-Cat scale. |
| Rizal et al., 2019 | n = 322 Malaysia Children M/F | Brain breaks, exercise videos accumulating to a weekly total of 30 min were shown to students for 12 weeks. | No significant findings with regards to PA data. |
| Zulkifi et al., 2019 | n = 65 Malaysia University students M/F | The 7-week intervention involved a student-centred approach and alternative assessments to evaluate students’ learning, focusing on accentuating participants’ roles during learning and assessing their knowledge and self-efficacy related to health education using alternative assessments. | Weekly recorded pedometer steps increased from 59,560 in week one to 87,286 in week seven, but no statistical test was done to determine significance. |
| Liau et al., 2018 | n = 85 Singapore Adults M/F | The intervention group was subjected to two sets of self-regulation strategies: self-regulation strategy of mental contrasting with implementation intentions and self-monitoring for 3 weeks. | For overall PA (steps per week), there was an increase in PA, only for men, from 7124.37 to 9180.44 steps per week and no change for the control group. For final-week PA (steps per week), there was an increase in PA, only for men, from 7124.37 to 9002.84 steps per week, and a decrease for the men in the control group from M = 8679.42 to 7769.86. |
| Mok et al., 2018 | n = 55 Malaysia Children M/F | An intervention involving nutrition education classes on healthy eating and active lifestyle; physical activity sessions; and active involvement of parents and teachers was conducted for 12 weeks. | There was a significant increase in PA levels (PAQ-C) from baseline to 15 months post-intervention, from 2.46 to 2.87. |
| Nguyen et al., 2018 | n = 157 Vietnam Adults M/F | Participants were subjected to either storytelling or didactic intervention for 12 months. | Low PA prevalence (<600 MET-min) decreased more in the storytelling (17.2%) than in the didactic intervention group (9.8%). However, there was no indication if there was a statistical test done to determine significance. |
| Nur Emilia et al., 2018 | n = 62 Malaysia Adults M/F | The intervention group had monthly meetings for 3 months to go through their log diaries and were given the motivation to increase their physical activity. | Pedometer step count between intervention and control group based on time: 1. Month 2: Mean difference (Control-Intervention) = −1165.00 [−2293.23, −36.76]. 2. Month 3: Mean difference (Control-Intervention) = −1619.00 [−2585.23, −652.76]. |
| Omar et al., 2018 | n = 178 Malaysia Adults F-only | The intervention group were encouraged to perform a physical activity package comprising: 1. 15-min daily brisk walking, 2. 30-min daily pillow dumbbell exercise, 3. Physical activity diary for self-monitoring, for 6 months. | No significant findings with regard to the PA data. |
| Suttanon et al., 2018 | n = 277 Thailand Older adults M/F | Participants in the intervention group were provided with a 4-month multifactorial falls prevention programme, with a focus on balance training exercises and had handrails installed in their homes, or given walking assistive devices. | Increase in exercise frequency but not modified PASE score or total exercise time in the intervention group. |
| Widyastuti et al., 2018 | n = 40 Indonesia Adults M/F | Participants in the control group were tasked to walk at the fastest pace possible at home for at least 30-min daily for 6 weeks, while participants in the intervention group were given 3 weekly 30-min sessions of supervised standard exercise training for 6 weeks in addition to the above. | No significant between-group differences. |
| Yatim et al., 2018 | n = 45 Malaysia Adults M/F Hypertension | Participants were given a self-management guidebook, covering topics and hands-on self-management activities related to hypertension (i.e., living with hypertension, healthy eating and hypertension, physical activity for hypertensive patients, and know your medicines) for 4 weeks. | The number of days the participants spent on vigorous physical activity significantly increased from 0.56 to 1.81 (d/wk) between baseline and post-1 week, while walking time significantly. decreased from 33.33 to 23.33 (min/d) between baseline and post-1 month. |
| Chawla et al., 2017 | n = 490 Thailand Children M/F | The participants were subjected to a multicomponent healthy lifestyle program that focused on the promotion of healthy eating and being physically active for 6 months. | No significant findings with regards to PA data. |
| Huei et al., 2017 | n = 189 Malaysia Adults M/F | Participants were split into 1 control and 2 intervention groups for 16 weeks. The first intervention group was subjected to point-of-decision prompts to motivate them to walk more. The second intervention group was given a weekly 1-h aerobics class. | Only significant differences between the step count of the aerobics and control group but no indication of which time points the statistical significance applied to. |
| Juliana et al., 2017 | n = 31 Malaysia Adults F-only | The intervention group was given a package of a variety of diet and physical activity guidelines for 16 weeks. | Significant effect of intervention in the intervention group, when compared to control, for PA in min/wk (3171 at baseline to 3355 at 16 weeks) and PA in activity score (7457 at baseline to 8298 at 16 weeks) using Short Questionnaires to Assess Health-Enhancing Physical Activity (SQUASH). |
| Karintrakul et al., 2017 | n = 45 Thailand Adults F-only | The intervention group received nutrition counselling. The study mentions three, 30 to 45-min counselling sessions, followed by 5–10 min between sessions over a total of 12 weeks. | No significant findings with regards to PA data. |
| Sanee et al., 2017 | n = 100 Thailand Adults F-only | Participants were subjected to a two-part intervention for a total of 17 weeks, the first consisting of a peer leader training program and the second consisting of a peer leader-led program. The program consisted of whole-group and small-group peer support and discussion. Personalised goals were set, education for healthy eating habits and PA for weight management were disseminated, as well as addressing personal barriers to change, maintaining motivation and encouraging them to use the additional material available to them. | No significant findings with regards to PA data. |
| Tran et al., 2017 | n = 337 Vietnam Adults M/F | The intervention included four educational sessions, a booklet, a resistance band and walking groups for 6 months. | Significantly greater moderate activity (61 vs. 30), walking time (588.3 vs. 326.7 min/wk) and total PA (862.7 vs. 502.9 min/week) in the intervention compared to the control group post-intervention using IPAQ. |
| Zahtamal et al., 2017 | n = 34 Indonesia Adults M/F | One group received a multilevel educational intervention that targeted various levels of the individual’s social support system, while the other group only received health education at an individual level for 12 weeks. | No significant findings with regards to PA data. |
| Finkelstein et al., 2016 | n = 800 Singapore Adults M/F | There were 4 intervention groups: a control group, a group that was only given a Fitbit pedometer, a Fitbit and charity incentive, as well as a Fitbit and cash incentive group. Participants in the non-control groups were asked to complete a certain number of steps per week for 6 months. | After 12 months:
|
| Haya et al., 2016 | n = 48 Indonesia Adults F-only | Individuals in the intervention group were given maternal health education 6 times for 12 weeks (60 min per class period), using a participation discussion method and booklets containing practical guides on childhood obesity management. Mothers in the control group received health education only once for 60 min at the beginning of the study. | Significant increase in PA level in the intervention group (0.04) and a significant decrease in PA level in the control group (−0.01). |
| Ibrahim et al., 2016 | n = 268 Malaysia Adults M/F Pre-diabetes | Participants in the intervention group received twelve group-based sessions of 90 min each and a minimum of two individual counselling sessions with the dietician and researcher to reinforce behavioural change, for 12 months. | Significantly higher PA (MET-min/wk) in the intervention group than in the control group at 6-month (66.5) and 12-month (183.2) measures. |
| Jafar et al., 2016 | n = 100 Singapore Adults M/F Hypertension | The interventions were related to training the physicians in the treatment program algorithm, subsidy for antihypertensive medication, training nurses in motivational conversation and structured follow-up over the telephone over 8 weeks. | No significant findings with regards to PA data. |
| Müller-Riemenschneider et al., 2016 | n = 43 Malaysia Older adults M/F | Participants in the intervention group were sent 60 SMS text messages over the course of 12 weeks. These messages provided instructions for exercise and provided praise/rewards for efforts towards exercise behaviour. | No significant findings with regards to PA data. |
| Nhung et al., 2016 | n = 60 Vietnam Adults F-only Post-menopause | Participants in the intervention group received 6 capsules containing acylated steryl glucosides, while the placebo group took 6 placebo isocaloric capsules over 6 months. | No significant between-group differences. |
| Ethisan et al., 2015 | n = 102 Thailand Adults M/F | Participants in the intervention group received a Group-Mediated Lifestyle Physical Activity program for 6 months. This included group-based PA, group-mediated education and home-based PA. | Mean score of health benefits from physical activity increased from 23.2 to 40.7 in the intervention group, while it decreased from 20.7 to 4.6 in the control group. |
| Huynh et al., 2015 | n = 199 Philippines Children M/F | Parents received three sessions of dietary counselling administered at baseline, weeks 4 and 8 post-baseline, while children received two servings of oral nutrition supplement per day for 48 weeks. | Parent-reported children’s PA levels increased from 7.9 to 9.0 from baseline to 48 weeks (VAS). |
| Ng et al., 2015 | n = 246 Singapore Older adults M/F | The participants were split into 1 control and 4 intervention groups, including nutritional, cognitive training, physical training and a combined interventions group over 12 months. | Mean change from baseline (average time, min/d): 6 months × Nutritional = 96.2 [57.8, 134.7]. 12 months × Nutritional = 110.1 [71.9, 148.2]. |
| Sazlina et al., 2015 | n = 69 Malaysia Older adults M/F | Participants were split into personalised feedback (PF) about physical activity patterns group, peer support (PS) group and a control group. Both PF and PS groups received structured personalised feedback and usual diabetes care. Participants in the PS group received support from peer mentors in addition to the above. This was done over a period of 12 weeks. | The PS group demonstrated significantly greater mean daily pedometer readings compared to the PF group at weeks 12 (1416 steps/d) and 36 (1416 steps/d) and were significantly greater compared to the control group at weeks 12 (2265 steps/d), 24 (2586 steps/d) and 36 (2084 steps/d). |
| Ngo et al., 2014 | n = 285 Singapore Children M/F | The intervention comprised targeted education on myopia and good eye care habits, structured weekend outdoor activities and incentives for children to increase their daily steps, as measured via pedometers (step counters). The control group only received resources on myopia prevention and the health benefits of physical activity. The intervention lasted 9 months. | The intervention group reported higher outdoor time across the whole week (14.75 vs. 12.4 h/wk) and on the weekend (2.89 vs. 2.4 h/d) compared to the control group during a 6-month interim measure. However, there were no significant differences between both groups at the end of the entire intervention. |
| Sriramatr et al., 2014 | n = 220 Thailand Adults F-only | Participants were randomly allocated into 4 groups for 3 months: intervention with/out pre-test and control with/out pre-test. The intervention groups were subjected to an internet-based program where they recorded their average physical activity, set physical activity goals for the next week. | With pre-test: The intervention group recorded more steps/d than those in the control (11,654 vs. 8194 steps/d) and leisure time activity score (54.14 vs. 37.58). Without pre-test: The intervention group recorded more steps/d than those in the control (10,601 vs. 7570 steps/d) and leisure time activity sore (59.50 vs. 39.32). |
| Suwanpasu et al., 2014 | n = 46 Thailand Older adults M/F | Participants in the intervention group were subjected to a physical activity enhancing program with a physical training component and efficacy-based intervention. The total duration of the intervention was not stated. | Significantly higher post-test measures of PA in the intervention group compared to the control group (961.37 MET-min/wk). |
| Finkelstein et al., 2013 | n = 285 Singapore Children M/F | The intervention group received information on structured weekend outdoor activities and pedometer step programs for 3 months. Families were encouraged to attend sessions at least twice a month. | At follow-up, the intervention group had significantly higher pedometer steps than the control group across the entire week (958), weekdays (848) and weekends (1239). |
| Lua et al., 2013 | n = 380 Malaysia University students M/F | The intervention programme employed was developed based on the latest Malaysian dietary guidelines. All included messages were delivered through 3 modes: conventional lectures, brochures and text messaging. The intervention lasted 10 weeks. | After 10 weeks, the intervention group had higher MET-min/wk than the control group across walking (764.2), moderate activity (333.4), vigorous activity (413.4) and total (1548.8). |
| Soon et al., 2013 | n = 56 Malaysia Adults M/F | The intervention group was subjected to a combined physical activity and dietary intervention for 12 weeks. The intervention activities included lectures and group discussion sessions. | No significant findings with regards to PA. |
| Nguyen et al., 2012 | n = 4650 Vietnam Adults M/F | In the communes selected for intervention, a hypertension management programme was implemented and integrated with the primary health care system. The intervention lasted 3 years. | Physical inactivity levels increased in the intervention group after 3 years (6.8% to 12.8%). |
| Tan et al., 2011 | n = 164 Malaysia Adults M/F Type 2 diabetes | An education intervention was carried out consisting of 3 monthly sessions across 3 months, addressing the self-care practices of healthy eating, being active, medication adherence. and self-monitoring of blood glucose (SMBG). The 2nd and 3rd sessions centred around the SMBG results, exploring problem-solving skills related to hyperglycaemia, hypoglycaemia, sick day and emotional episodes. | After 12 weeks, total PA was higher in the intervention group (15.50) than the control group (12.73), but no difference within-group for either group (Revised Diabetes Self-care Activities Questionnaires modified from the Diabetes Self-care Activities Questionnaire). |
| Wafa et al., 2011 | n = 107 Malaysia Children M/F | The intervention group was subjected to a parent-centric intervention focused on changing the behaviours to treat childhood obesity. There was a total of 8 intervention sessions, over 26 weeks, directed at the parents and participating children attended a physical activity session led by an exercise instructor. | No significant findings with regards to PA. |
| Chia, 2009 | n = 490 Singapore Children M/F | The programme involved a 10-week infusion of daily physical play between 20 to 45 min during school curriculum hours, either as stand-alone additional play sessions or as part of an extended recess, where pupils could have light refreshments and play. | One school had an increase in the number of within-school-hours steps from 3742 to 4642, while another school had an increase from 4520 to 4984. |
| Muda et al., 2006 | n = 91 Malaysia Adults M-only | The intervention group was given individual counselling on physical activity by the main researcher based on patient-centred assessment and counselling for exercise and monthly aerobic exercise. Group education was given at month 3, followed by monthly phone calls for the last 3 months. | Total energy expenditure was higher in the intervention group (3.08 kcal/kg/d) compared to the control group (0.38 kcal/kg/d) at the end of the 6-month intervention (7-day Physical Activity Recall). |
| Hadju et al., 1998 | n = 129 Indonesia Children M-only | Individuals in the intervention group were subjected to albendazole injections for 6 months. | After 6 months, the activity increase in the intervention group (~0.3 METs) was higher than in the control group. Only graphical representations were provided. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-S.; Chia, M.; Komar, J. A Systematic Review of Physical Activity Intervention Programs in ASEAN Countries: Efficacy and Future Directions. Int. J. Environ. Res. Public Health 2022, 19, 5357. https://doi.org/10.3390/ijerph19095357
Lee Y-S, Chia M, Komar J. A Systematic Review of Physical Activity Intervention Programs in ASEAN Countries: Efficacy and Future Directions. International Journal of Environmental Research and Public Health. 2022; 19(9):5357. https://doi.org/10.3390/ijerph19095357
Chicago/Turabian StyleLee, Yi-Shin, Michael Chia, and John Komar. 2022. "A Systematic Review of Physical Activity Intervention Programs in ASEAN Countries: Efficacy and Future Directions" International Journal of Environmental Research and Public Health 19, no. 9: 5357. https://doi.org/10.3390/ijerph19095357
APA StyleLee, Y.-S., Chia, M., & Komar, J. (2022). A Systematic Review of Physical Activity Intervention Programs in ASEAN Countries: Efficacy and Future Directions. International Journal of Environmental Research and Public Health, 19(9), 5357. https://doi.org/10.3390/ijerph19095357