
Prevalence and Correlates of Water, Sanitation, and Hygiene (WASH) and Spatial Distribution of Unimproved WASH in Nepal

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Sample Selection
2.3. Predictors
2.4. Outcome Variables
2.5. Statistical Analysis
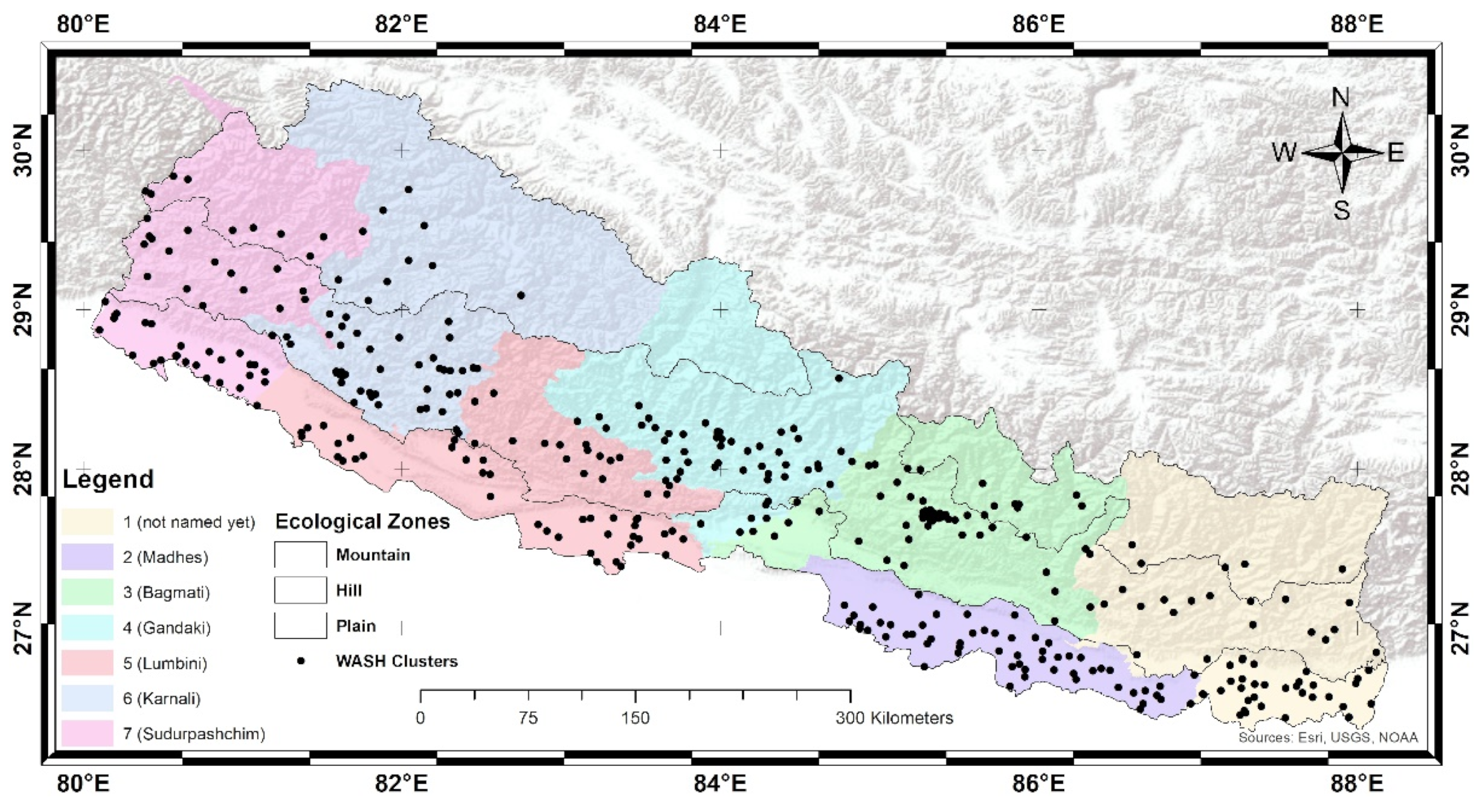
2.6. Spatial Analysis
2.7. Ethical Consideration
3. Results
3.1. Descriptive Statistics
3.2. Correlation of WASH Factors
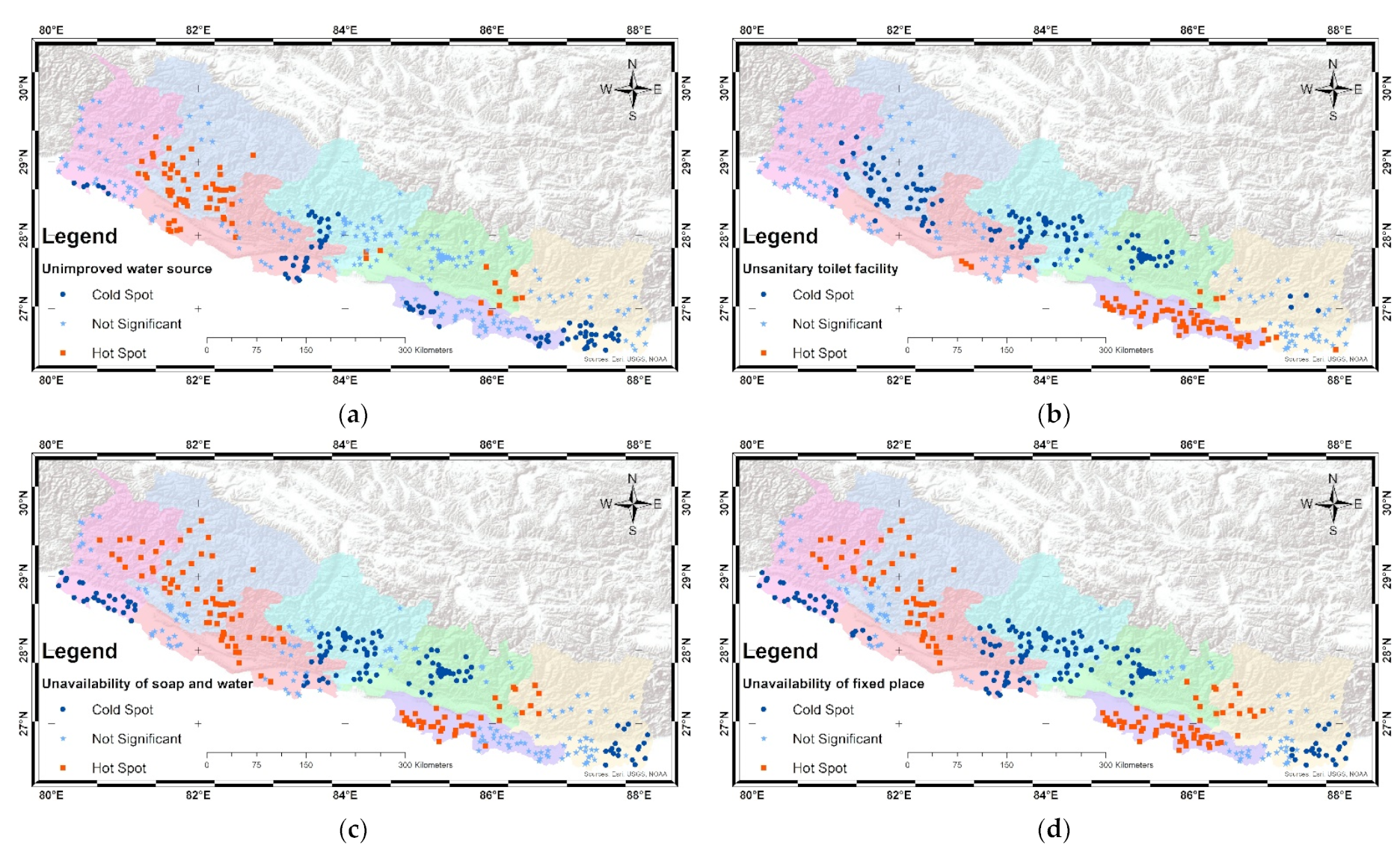
3.3. Visualization of WASH Hot and Cold Spots
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Progress on Household Drinking Water, Sanitation and Hygiene 2000–2020: Five Years into the SDGs; World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF): Geneva, Switzerland, 2021.
- World Health Organization. Sanitation and Hygiene Promotion; WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Clasen, T.; Boisson, S.; Routray, P.; Torondel, B.; Bell, M.; Cumming, O.; Ensink, J.; Freeman, M.; Jenkins, M.; Odagiri, M.; et al. Effectiveness of a rural sanitation programme on diarrhoea, soil-transmitted helminth infection, and child malnutrition in Odisha, India: A cluster-randomised trial. Lancet Glob. Health 2014, 211, e645–e653. [Google Scholar] [CrossRef] [Green Version]
- Clasen, T.; Schmidt, W.-P.; Rabie, T.; Roberts, I.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea: Systematic review and meta-analysis. BMJ 2007, 334, 782. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Preventing Diarrhoea through Better Water, Sanitation and Hygiene: Exposures and Impacts in Low-and Middle-Income Countries; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Schwemlein, S.; Cronk, R.; Bartram, J. Indicators for monitoring water, sanitation, and hygiene: A systematic review of indicator selection methods. Int. J. Environ. Res. Public Health 2016, 133, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartram, J.; Cairncross, S. Hygiene, sanitation, and water: Forgotten foundations of health. PLoS Med. 2010, 711, e1000367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Sanitation Challenge: Turning Commitment into Reality; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- McGriff, J.A.; Denny, L. What COVID-19 reveals about the neglect of WASH within infection prevention in low-resource healthcare facilities. Am. J. Trop. Med. Hyg. 2020, 1035, 1762. [Google Scholar] [CrossRef]
- Cairncross, S.; Bartram, J.; Cumming, O.; Brocklehurst, C. Hygiene, sanitation, and water: What needs to be done? PLoS Med. 2010, 711, e1000365. [Google Scholar] [CrossRef] [Green Version]
- Kumwenda, S. Challenges to Hygiene Improvement in Developing Countries. In The Relevance of Hygiene to Health in Developing Countries, 1st ed.; Potgieter, N., Traore, A.N., Eds.; IntechOpen: London, UK, 2019; pp. 9–26. [Google Scholar]
- Pruss-Ustun, A.; World Health Organization. Safer Water, Better Health: Costs, Benefits and Sustainability of Interventions to Protect and Promote Health; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Sah, R.B.; Bhattarai, S.; Baral, D.; Pokharel, P. Knowledge and practice towards hygiene and sanitation amongst residents of Dhankuta Municipality. Health Renaiss. 2014, 121, 44–48. [Google Scholar] [CrossRef]
- Akter, T.; Ali, A.M. Factors influencing knowledge and practice of hygiene in Water, Sanitation and Hygiene (WASH) programme areas of Bangladesh Rural Advancement Committee. Rural. Remote Health 2014, 14, 31–40. [Google Scholar] [CrossRef]
- White, S.; Kuper, H.; Itimu-Phiri, A.; Holm, R.; Biran, A. A qualitative study of barriers to accessing water, sanitation and hygiene for disabled people in Malawi. PLoS ONE 2016, 115, e0155043. [Google Scholar] [CrossRef] [Green Version]
- Wasonga, J.; Okowa, M.; Kioli, F. Sociocultural determinants to adoption of safe water, sanitation, and hygiene practices in Nyakach, Kisumu County, Kenya: A descriptive qualitative study. J. Anthropol. 2016, 2016, 7434328. [Google Scholar] [CrossRef] [Green Version]
- Kafle, S.; Pradhan, B. Situation of Water, Sanitation and Hygiene and Diarrhoeal Diseases After Open Defecation Free Declaration. J. Nepal Health Res. Counc. 2018, 162, 160–164. [Google Scholar] [CrossRef]
- Wang, C.; Pan, J.; Yaya, S.; Yadav, R.B.; Yao, D. Geographic inequalities in accessing improved water and sanitation facilities in Nepal. Int. J. Environ. Res. Public Health 2019, 167, 1269. [Google Scholar] [CrossRef] [Green Version]
- Wali, N.; Georgeou, N.; Simmons, O.; Gautam, M.S.; Gurung, S. Women and WASH in Nepal: A scoping review of existing literature. Water Int. 2020, 453, 222–245. [Google Scholar] [CrossRef]
- Ministry of Health, New ERA, Inner City Fund International. Nepal Demographic and Health Survey 2016; Ministry of Health: Kathmandu, Nepal, 2017.
- Dhital, S.R. Household Water, Sanitation and Hygiene and Their Effects on Child Health in Nepal. Ph.D. Thesis, The University of Newcastle, Newcastle, Australia, 2021. [Google Scholar]
- Gautam, O.P.; Schmidt, W.P.; Cairncross, S.; Cavill, S.; Curtis, V. Trial of a Novel Intervention to Improve Multiple Food Hygiene Behaviors in Nepal. Am. J. Trop. Med. Hyg. 2017, 966, 1415–1426. [Google Scholar] [CrossRef]
- Shrestha, S.K.; Vicendese, D.; Erbas, B. Water, sanitation and hygiene practices associated with improved height-for-age, weight-for-height and weight-for-age z-scores among under-five children in Nepal. BMC Pediatr. 2020, 201, 134. [Google Scholar] [CrossRef] [PubMed]
- Hosmer, D.W.; Lemesbow, S. Goodness of fit tests for the multiple logistic regression model. Commun. Stat.-Theory Methods 1980, 910, 1043–1069. [Google Scholar] [CrossRef]
- Hulland, K.R.; Leontsini, E.; Dreibelbis, R.; Unicomb, L.; Afroz, A.; Dutta, N.C.; Nizame, F.A.; Luby, S.P.; Ram, P.K.; Winch, P.J. Designing a handwashing station for infrastructure-restricted communities in Bangladesh using the integrated behavioural model for water, sanitation and hygiene interventions (IBM-WASH). BMC Public Health 2013, 131, 877. [Google Scholar] [CrossRef] [Green Version]
- Simons, K.L. Useful Stata Commands (for Stata versions 13, 14, & 15). 2019. Available online: http://homepages.rpi.edu/~simonk/pdf/UsefulStataCommands.pdf (accessed on 29 December 2019).
- Rao, J.N.; Scott, A.J. On simple adjustments to chi-square tests with sample survey data. Ann. Stat. 1987, 15, 385–397. [Google Scholar] [CrossRef]
- National Planning Commission. Nepal in Figure 2021; Central Bureau of Statistics: Kathmandu, Nepal, 2021.
- Ord, J.K.; Getis, A. Local spatial autocorrelation statistics: Distributional issues and an application. Geogr. Anal. 1995, 274, 286–306. [Google Scholar] [CrossRef]
- Islam, N.; Koju, P.; Manandhar, R.; Shrestha, S.; Smith, C. Assessing the Impacts of Relative Wealth and Geospatial Factors on Water Access in Rural Nepal: A Community Case Study. Int. J. Environ. Res. Public Health 2020, 1718, 6517. [Google Scholar] [CrossRef] [PubMed]
- Flores Baquero, Ó.G.G.R.; Pérez Foguet, A.; Jiménez Fdez de Palencia, A. Post-2015 WASH Targets and Indicators: A Review from a Human Rights Perspective; University Research Institute for Sustainability Science and Technology—IS.UPC at the Universitat Politècnica de Catalunya: Barcelona, Spain, 2013. [Google Scholar]
- World Health Organization; United Nations Children’s Fund. Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- United Nations Educational Scientific and Cultural Organisation (UNESCO). The United Nations World Water Development Report 2019: Leaving No One Behind; UNESCO: Paris, France, 2019; p. 13. [Google Scholar]
- Ministry of Health and Population, New ERA, Macro International Inc. Nepal Demographic and Health Survey 2006; Ministry of Health and Population: Kathmandu, Nepal, 2007.
- Ministry of Health and Population, New ERA, Inner City Fund International. Nepal Demographic and Health Survey 2011; Ministry of Health and Population: Kathmandu, Nepal, 2012.
- Upadhyay, S.N.; Gaudel, P. Water resources development in Nepal: Myths and realities. Hydro Nepal J. Water Energy Environ. 2018, 23, 22–29. [Google Scholar] [CrossRef]
- Asian Development Bank. Drainage and Sanitation; Padeco Co. Ltd. in Association with Metcon Consultants: Kathmandu, Nepal; Tokyo, Japan, 2010. [Google Scholar]
- Sharma, B.; Nepal, S.; Gyawali, D.; Pokharel, G.S.; Wahid, S.; Mukherji, A.; Acharya, S.; Shrestha, A.B. Springs, Storage Towers, and Water Conservation in the Midhills of Nepal; International Centre for Integrated Mountain Development: Kathmandu, Nepal, 2016. [Google Scholar]
- Poudel, D.D.; Duex, T.W. Vanishing springs in Nepalese mountains: Assessment of water sources, farmers’ perceptions, and climate change adaptation. Mt. Res. Dev. 2017, 371, 35–46. [Google Scholar] [CrossRef]
- Johri, M.; Sylvestre, M.P.; Koné, G.K.; Chandra, D.; Subramanian, S.V. Effects of improved drinking water quality on early childhood growth in rural Uttar Pradesh, India: A propensity-score analysis. PLoS ONE 2019, 141, e0209054. [Google Scholar] [CrossRef] [Green Version]
- Bukhman, G.; Mocumbi, A.O.; Atun, R.; Becker, A.E.; Bhutta, Z.; Binagwaho, A.; Clinton, C.; Coates, M.M.; Dain, K.; Ezzati, M.; et al. The Lancet NCDI Poverty Commission: Bridging a gap in universal health coverage for the poorest billion. Lancet 2020, 396, 991–1044. [Google Scholar] [CrossRef]
- Mahmud, I.; Mbuya, N. Water, Sanitation, Hygiene, and Nutrition in Bangladesh: Can Building Toilets Affect Children’s Growth? World Bank Publications: Washington, DC, USA, 2015. [Google Scholar]
- Bain, R.; Cronk, R.; Wright, J.; Yang, H.; Slaymaker, T.; Bartram, J. Fecal contamination of drinking-water in low-and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2014, 115, e1001644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattarai, R.; Dahal, K. Review of water pollution with special focus on Nepal. J. Emerg. Tech. Innov. Res. 2020, 7, 100–101. [Google Scholar]
- Armah, F.A.; Ekumah, B.; Yawson, D.O.; Odoi, J.O.; Afitiri, A.R.; Nyieku, F.E. Access to improved water and sanitation in sub-Saharan Africa in a quarter century. Heliyon 2018, 4, e00931. [Google Scholar] [CrossRef] [Green Version]
- He, W.J.; Lai, Y.S.; Karmacharya, B.M.; Dai, B.F.; Hao, Y.T.; Xu, D.R. Geographical heterogeneity and inequality of access to improved drinking water supply and sanitation in Nepal. Int. J. Equity Health 2018, 17, 40. [Google Scholar] [CrossRef] [Green Version]
- Luby, S.P.; Agboatwalla, M.; Painter, J.; Altaf, A.; Billhimer, W.L.; Hoekstra, R.M. Effect of intensive handwashing promotion on childhood diarrhea in high-risk communities in Pakistan: A randomized controlled trial. JAMA 2004, 291, 2547–2554. [Google Scholar] [CrossRef] [PubMed]
- Dahal, K.R.; Adhikari, B.; Tamang, J. Sanitation coverage and impact of open defecation free (ODF) zone with special reference to Nepal: A review. Int. J. Eng. Res. Appl. 2014, 48, 1–11. [Google Scholar]
- Vyas, S.; Spears, D. Sanitation and religion in South Asia: What accounts for differences across countries? J. Dev. Stud. 2018, 54, 2119–2135. [Google Scholar] [CrossRef] [Green Version]
- Hutton, G.; Chase, C. The knowledge base for achieving the sustainable development goal targets on water supply, sanitation and hygiene. Int. J. Environ. Res. Public Health 2016, 13, 536. [Google Scholar] [CrossRef] [Green Version]
- WaterAid. Community Led Total Sanitation in Nepal Getting Us Back on Track; WaterAid Nepal: Lalitpur, Nepal, 2006. [Google Scholar]
- Central Bureau of Statistics. Report on the Nepal Labour Force Survey 2017/18; National Planning Commission: Kathmandu, Nepal, 2018.
- Low, S.; Spindler, P.G. Child Care Arrangements of Working Mothers in the United States; US Government Printing Office: Washington, DC, USA, 1968.
- Central Bureau of Statistics. Nepal Multiple Indicator Cluster Survey (MICS), Final Report; National Planning Commission, Central Bureau Statistics (CBS), UNICEF: Kathmandu, Nepal, 2019.
- Kumar, S.; Loughnan, L.; Luyendijk, R.; Hernandez, O.; Weinger, M.; Arnold, F.; Ram, P.K. Handwashing in 51 countries: Analysis of proxy measures of handwashing behavior in multiple indicator cluster surveys and demographic and health surveys, 2010–2013. Am. J. Trop. Med. Hyg. 2017, 972, 447. [Google Scholar] [CrossRef] [PubMed]
- White, S.; Thorseth, A.H.; Dreibelbis, R.; Curtis, V. The determinants of handwashing behaviour in domestic settings: An integrative systematic review. Int. J. Hyg. Environ. Health 2020, 227, 113512. [Google Scholar] [CrossRef]
- Budhathoki, C.B. Water Supply, Sanitation and Hygiene Situation in Nepal: A Review. J. Health Promot. 2019, 7, 65–76. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | Class |
|---|---|
| Age of the household head (in years) | 15–24; 25–34; 35–44; 45 and above |
| Sex of the household head | Male; Female |
| Education level | No education: unable to read or write; Primary: completed Year 5 schooling; Secondary: completed Year 8 schooling; School Leaving Certificate (SLC) or higher: completed Year 10 or above schooling; Do Not Know |
| Marital status | Married; Unmarried; Widowed/divorced |
| Number of household family members | 1–2; 3–4; 5–6; 7+ |
| Place of residence | Rural; Urban |
| Ecological zone | Plains; Hills; Mountains |
| Province | 1, not named yet 1; 2, Madhes Pradesh; 3, Bagmati Pradesh; 4, Gandaki Pradesh 5, Lumbini Pradesh; 6, Karnali Pradesh; 7, Sudurpashchim Pradesh |
| Household wealth index | Poor; Middle; Rich |
| Distance to a water source | ≤30 min walk: 30 min or less walking time to water source; >30 min walk: more than 30 min walking time to water source; Do Not Know |
| Variables | Class | Weighted Frequencies (n) | Weighted Percentages (%) |
|---|---|---|---|
| Age of household head (in years) | 15–24 | 625 | 5.7 |
| 25–34 | 2240 | 20.3 | |
| 35–44 | 2562 | 23.2 | |
| 45 and above | 5613 | 50.8 | |
| Sex of household head | Male | 7581 | 68.7 |
| Female | 3459 | 31.3 | |
| Education of household head | No education | 4310 | 39.1 |
| Primary | 2492 | 22.5 | |
| Secondary | 2947 | 26.7 | |
| Higher | 1272 | 11.5 | |
| Do not know | 19 | 0.2 | |
| Marital status of household head | Married | 9499 | 86.0 |
| Unmarried | 337 | 3.1 | |
| Widowed and divorced | 1204 | 10.9 | |
| Number of family members | 1–2 | 2160 | 19.6 |
| 3–4 | 4146 | 37.6 | |
| 5–6 | 3048 | 27.6 | |
| 7+ | 1685 | 15.2 | |
| Place of residence | Rural | 6019 | 54.5 |
| Urban | 5021 | 45.5 | |
| Ecological zone | Plains | 5125 | 46.4 |
| Hills | 5134 | 46.5 | |
| Mountains | 781 | 7.1 | |
| Province | 1 (not named yet) | 2004 | 18.2 |
| 2 (Madhes) | 2014 | 18.2 | |
| 3 (Bagmati) | 2521 | 22.9 | |
| 4 (Gandaki) | 1173 | 10.6 | |
| 5 (Lumbini) | 1793 | 16.2 | |
| 6 (Karnali) | 619 | 5.6 | |
| 7 (Sudurpashchim) | 916 | 8.3 | |
| Wealth index of household | Poor | 4459 | 40.4 |
| Middle | 2065 | 18.7 | |
| Rich | 4516 | 40.9 | |
| Source of water | Improved | 10,543 | 95.5 |
| Unimproved | 497 | 4.5 | |
| Distance to a water source | ≤30 min walk | 10,476 | 94.9 |
| >30 min walk | 562 | 5.1 | |
| Do not know | 2 | 0.1 | |
| Type of sanitation | Improved | 9246 | 83.8 |
| Unimproved | 1794 | 16.2 | |
| Handwashing place | Fixed | 8936 | 80.9 |
| Non-fixed | 2075 | 18.8 | |
| Missing (not observed) | 29 | 0.3 | |
| Soap and water | Available | 5185 | 46.9 |
| Not available | 5827 | 52.8 | |
| Missing (not observed) | 28 | 0.3 |
| Variables | Class | Improved Water | Improved Sanitation | Soap and Water | Fixed Place |
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| Age of household head (in years) | 15–24 | 1.14 (0.73–1.78) | 1.02 (0.76–1.39) | 1.11 (0.87–1.44) | 1.02 (0.81–1.27) |
| 25–34 | 0.95 (0.70–1.27) | 0.92 (0.78–1.07) | 1.13 (0.99–1.28) | 1.13 (0.96–1.32) | |
| 35–44 | 1.04 (0.84–1.29) | 1.07 (0.91–1.26) | 1.16 (1.04–1.29) | 1.05 (0.92–1.22) | |
| 45 and above | 1 | 1 | 1 | 1 | |
| Sex of household head | Male | 1 | 1 | 1 | 1 |
| Female | 0.87 (0.72–1.06) | 1.02 (0.85–1.22) | 0.96 (0.86–1.07) | 0.95 (0.83–1.09) | |
| Education of household head | No education | 1 | 1 | 1 | 1 |
| Primary | 1.11 (0.90–1.38) | 1.95 (1.63–2.33) | 1.78 (1.58–2.02) | 1.62 (1.39–1.89) | |
| Secondary | 1.81 (1.28–2.57) | 3.37 (2.71–4.19) | 2.85 (2.49–3.26) | 2.41 (1.99–2.92) | |
| Higher | 3.51 (1.86–6.62) | 13.43 (7.91–22.86) | 7.09 (5.73–8.70) | 6.01 (4.47–8.07) | |
| Marital status of household head | Married | 1 | 1 | 1 | 1 |
| Unmarried | 2.59 (0.94–7.16) | 2.50 (2.36–8.56) | 2.25 (1.66–3.31) | 1.96 (1.32–2.90) | |
| Widowed and divorced | 0.92 (0.68–1.23) | 0.95 (0.73–1.15) | 0.79 (0.69–0.92) | 0.76 (0.62–0.94) | |
| Number of family members | 1–2 | 0.96 (0.74–1.24) | 0.96 (0.81–1.14) | 0.80 (0.69–0.92) | 0.83 (0.70–0.99) |
| 3–4 | 1 | 1 | 1 | 1 | |
| 5–6 | 0.83 (0.65–1.05) | 0.77 (0.65–0.91) | 0.77 (0.69–0.86) | 0.78 (0.68–0.88) | |
| 7+ | 1.37 (0.98–1.92) | 0.56 (0.0.45–0.70) | 0.71 (0.60–84) | 0.78 (0.65–0.93) | |
| Place of residence | Rural | 1 | 1 | 1 | 1 |
| Urban | 1.10 (0.63–1.93) | 2.30 (1.52–3.49) | 3.58 (2.78–4.64) | 2.36 (1.82–3.06) | |
| Ecological zone | Plains | 1 | 1 | 1 | 1 |
| Hills | 0.32 (0.16–0.64) | 6.41 (4.39–9.37) | 1.25 (0.95–1.64) | 1.33 (1.01–1.77) | |
| Mountains | 0.62 (0.26–1.51) | 4.30 (2.52–7.35) | 0.48 (0.31–0.75) | 0.61 (0.41–0.91) | |
| Province | 1 (not named yet) | 1 | 1 | 1 | 1 |
| 2 (Madhes) | 1.01 (0.30–3.42) | 0.15 (0.08–0.28) | 0.54 (0.37–0.79) | 0.44 (0.29–0.67) | |
| 3 (Bagmati) | 0.54 (0.21–1.36) | 1.82 (0.93–3.54) | 1.90 (1.26–2.86) | 1.36 (0.87–2.11) | |
| 4 (Gandaki) | 0.54 (0.24–1.20) | 2.92 (1.52–5.61) | 1.23 (0.84–1.80) | 2.28 (1.50–3.46) | |
| 5 (Lumbini) | 0.99 (0.41–2.41) | 1.06 (0.51–2.20) | 0.80 (0.54–1.18) | 1.06 (0.68–1.66) | |
| 6 (Karnali) | 0.19 (0.09–0.43) | 2.69 (1.52–4.76) | 0.38 (0.25–0.58) | 0.49 (0.31–0.77) | |
| 7 (Sudurpashchim) | 0.65 (0.28–1.48) | 1.93 (1.03–3.58) | 0.96 (0.64–1.45) | 0.99 (0.61–1.63) | |
| Wealth index of household | Poor | 0.22 (0.10–0.50) | 0.17 (0.13–0.24) | 0.13 (0.10–0.15) | 0.25 (0.20–0.31) |
| Middle | 0.72 (0.31–1.66) | 0.13 (0.10–0.18) | 0.22 (0.18–0.26) | 0.33 (0.26–0.42) | |
| Rich | 1 | 1 | 1 | 1 | |
| Distance to a water source | >30 min walk | 0.07 (0.04–0.12) | 1.03 (0.69–1.54) | 0.36 (0.25–0.52) | 0.39 (0.27–0.57) |
| ≤30 min walk | 1 | 1 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dhital, S.R.; Chojenta, C.; Evans, T.-J.; Acharya, T.D.; Loxton, D. Prevalence and Correlates of Water, Sanitation, and Hygiene (WASH) and Spatial Distribution of Unimproved WASH in Nepal. Int. J. Environ. Res. Public Health 2022, 19, 3507. https://doi.org/10.3390/ijerph19063507
Dhital SR, Chojenta C, Evans T-J, Acharya TD, Loxton D. Prevalence and Correlates of Water, Sanitation, and Hygiene (WASH) and Spatial Distribution of Unimproved WASH in Nepal. International Journal of Environmental Research and Public Health. 2022; 19(6):3507. https://doi.org/10.3390/ijerph19063507
Chicago/Turabian StyleDhital, Shalik Ram, Catherine Chojenta, Tiffany-Jane Evans, Tri Dev Acharya, and Deborah Loxton. 2022. "Prevalence and Correlates of Water, Sanitation, and Hygiene (WASH) and Spatial Distribution of Unimproved WASH in Nepal" International Journal of Environmental Research and Public Health 19, no. 6: 3507. https://doi.org/10.3390/ijerph19063507
APA StyleDhital, S. R., Chojenta, C., Evans, T.-J., Acharya, T. D., & Loxton, D. (2022). Prevalence and Correlates of Water, Sanitation, and Hygiene (WASH) and Spatial Distribution of Unimproved WASH in Nepal. International Journal of Environmental Research and Public Health, 19(6), 3507. https://doi.org/10.3390/ijerph19063507