
Asbestos Exposure in Patients with Malignant Pleural Mesothelioma included in the PRIMATE Study, Lombardy, Italy

 ,
,  ,
,  ,
,  ,
,  , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Malignant Pleural Mesothelioma Patients
2.2. Retrospective Assessment of Exposure to Asbestos
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Subjects Classified as Occupationally Exposed by Experts and Non-Exposed by JEM
4.2. Subjects Classified as Occupationally Exposed by JEM and Non-Exposed by Experts
4.3. Advantages and Limitations of the Two Approaches
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institute for Occupational Safety and Health (NIOSH). Asbestos Fibers and Other Elongate Mineral Particles: State of the Science and Roadmap for Research (Current Intelligence Bulletin 62). DHHS Publ. No. 2011-159 2011, Cincinnati, USA. Available online: https://www.cdc.gov/niosh/docs/2011-159/default.html (accessed on 4 March 2022).
- Cherrie, J.W.; McElvenny, D.; Blyth, K.G. Estimating past inhalation exposure to asbestos: A tool for risk attribution and disease screening. Int. J. Hyg. Environ. Health 2018, 221, 27–32. [Google Scholar] [CrossRef] [Green Version]
- IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans Volume 100C—Arsenic, Metals, Fibres, and Dusts; IARC: Lyon, France, 2012; ISBN 978-92-832-1320-8.
- ATSDR. Toxicological Profile for Asbestos; US Department of Health and Human Services: Atlanta, GA, USA, 2001.
- Mensi, C.; Riboldi, L.; De Matteis, S.; Bertazzi, P.A.; Consonni, D. Impact of an asbestos cement factory on mesothelioma incidence: Global assessment of effects of occupational, familial, and environmental exposure. Environ. Int. 2015, 74, 191–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensi, C.; De Matteis, S.; Dallari, B.; Riboldi, L.; Bertazzi, P.A.; Consonni, D. Incidence of mesothelioma in Lombardy, Italy: Exposure to asbestos, time patterns and future projections. Occup. Environ. Med. 2016, 73, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mensi, C.; De Matteis, S.; Catelan, D.; Dallari, B.; Riboldi, L.; Pesatori, A.C.; Consonni, D. Geographical patterns of mesothelioma incidence and asbestos exposure in Lombardy, Italy. Med. Lav. 2016, 107, 340–355. [Google Scholar] [PubMed]
- Mensi, C.; Mendola, M.; Dallari, B.; Sokooti, M.; Tabibi, R.; Riboldi, L.; Consonni, D. Differences between peritoneal and pleural mesothelioma in Lombardy, Italy. Cancer Epidemiol. 2017, 51, 67–73. [Google Scholar] [CrossRef]
- Consonni, D.; Calvi, C.; De Matteis, S.; Mirabelli, D.; Landi, M.T.; Caporaso, N.E.; Peters, S.; Vermeulen, R.; Kromhout, H.; Dallari, B.; et al. Peritoneal mesothelioma and asbestos exposure: A population-based case-control study in Lombardy, Italy. Occup. Environ. Med. 2019, 76, 545–553. [Google Scholar] [CrossRef] [Green Version]
- Consonni, D.; De Matteis, S.; Dallari, B.; Pesatori, A.C.; Riboldi, L.; Mensi, C. Impact of an asbestos cement factory on mesothelioma incidence in a community in Italy. Environ. Res. 2020, 183, 108968. [Google Scholar] [CrossRef]
- Marinaccio, A.; Consonni, D.; Mensi, C.; Mirabelli, D.; Migliore, E.; Magnani, C.; Di Marzio, D.; Gennaro, V.; Mazzoleni, G.; Girardi, P.; et al. Association between asbestos exposure and pericardial and tunica vaginalis testis malignant mesothelioma: A case–control study and epidemiological remarks. Scand. J. Work. Environ. Health 2020, 46, 609–617. [Google Scholar] [CrossRef] [Green Version]
- Mezei, G.; Chang, E.; Mowat, F.; Moolgavkar, S. Comments on a recent case-control study of malignant mesothelioma of the pericardium and the tunica vaginalis testis. Scand. J. Work. Environ. Health 2020, 47, 85–86. [Google Scholar] [CrossRef]
- Marinaccio, A.; Consonni, D.; Mensi, C.; Mirabelli, D.; Migliore, E.; Magnani, C.; Di Marzio, D.; Gennaro, V.; Mazzoleni, G.; Girardi, P.; et al. Authors’ response: Mezei et al.’s “Comments on a recent case-control study of malignant mesothelioma of the pericardium and the tunica vaginalis testis.”. Scand. J. Work. Environ. Health 2021, 47, 87–89. [Google Scholar] [CrossRef]
- Kazan-Allen, L. Asbestos and mesothelioma: Worldwide trends. Lung Cancer 2005, 49, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Sly, P.D.; Chase, R.; Kolbe, J.; Thompson, P.; Gupta, L.; Daube, M.; Olver, I.; Vallance, D. Asbestos still poses a threat to global health: Now is the time for action. Med. J. Aust. 2010, 193, 198–199. [Google Scholar] [CrossRef] [PubMed]
- Borghi, F.; Mazzucchelli, L.A.; Campagnolo, D.; Rovelli, S.; Fanti, G.; Keller, M.; Cattaneo, A.; Spinazzè, A.; Cavallo, D.M. Retrospective Exposure Assessment Methods Used in Occupational Human Health Risk Assessment: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6190. [Google Scholar] [CrossRef] [PubMed]
- Sahmel, J.; Devlin, K.; Paustenbach, D.; Hollins, D.; Gaffney, S. The role of exposure reconstruction in occupational human health risk assessment: Current methods and a recommended framework. Crit. Rev. Toxicol. 2010, 40, 799–843. [Google Scholar] [CrossRef] [PubMed]
- Nesti, M.; Adamoli, S.; Ammirabile, F.; Ascoli, V.; Barbieri, P.; Cacciarini, V.; Candela, S.; Cavone, D.; Cuzillo, G.; Chellini, E.; et al. Linee Guida per la Rilevazione e la Definizione dei casi di Mesothelioma Maligno e la Trasmissione delle Informazioni all’ISPESL da parte dei Centri Operativi Regionali; ISPESL: Roma, Italy, 2003. [Google Scholar]
- Peters, S.; Vermeulen, R.; Portengen, L.; Olsson, A.; Kendzia, B.; Vincent, R.; Savary, B.; LavouCrossed Sign, J.D.S.; Cavallo, D.; Cattaneo, A.; et al. SYN-JEM: A Quantitative Job-Exposure Matrix for Five Lung Carcinogens. Ann. Occup. Hyg. 2016, 60, 795–811. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.; Kromhout, H.; Portengen, L.; Olsson, A.; Kendzia, B.; Vincent, R.; Savary, B.; Lavoué, J.; Cavallo, D.; Cattaneo, A.; et al. Sensitivity analyses of exposure estimates from a quantitative job-exposure matrix (SYN-JEM) for use in community-based studies. Ann. Occup. Hyg. 2013, 57, 98–106. [Google Scholar] [CrossRef] [Green Version]
- ISTAT—Istituto Nazionale di Statistica. Classificazione Delle Professioni. Metodi e Norme—Serie C—n.12; ISTAT: Roma, Itay, 1991. (In Italian)
- ISTAT—Istituto Nazionale di Statistica. Classificazione delle Attività Economiche Ateco 2007. Available online: https://www4.istat.it/it/strumenti/definizioni-e-classificazioni/ateco-2007 (accessed on 6 December 2021).
- Spinazzè, A.; Consonni, D.; Borghi, F.; Mazzucchelli, A.; Rovelli, S.; Cattaneo, A.; Zellino, C.; Dallari, B.; Pesatori, A.; Kromhout, H.; et al. Development of a crosswalk to translate Italian occupation codes to ISCO-68 codes. Ann. Work Expo. Health, 2022; in press. [Google Scholar] [CrossRef]
- ILO—International Labour Organization; ISCO—International Standard Classification of Occupations. Available online: https://www.ilo.org/public/english/bureau/stat/isco/ (accessed on 4 March 2022).
- Barbieri, P.G.; Lombardi, S.; Candela, A.; Pezotti, C.; Binda, I. Incidence of malignant mesothelioma (1980–1999) and asbestos exposure in 190 cases diagnosed in the population of the Province of Brescia. Med. Lav. 2001, 92, 249–262. [Google Scholar]
- Chiappino, G.; Mensi, C.; Riboldi, L.; Rivolta, G. Asbestos risk in the textile industry: Final confirmation of data from the Lombardy Mesothelioma Registry. Med. Lav. 2003, 94, 521–530. [Google Scholar]
- Chiappino, G.; Pellissetti, D.; Moretto, O.; Picchi, O. Asbestos risk in the textile industry: Braking systems on machinery used until the 1990’s. Med. Lav. 2005, 96, 250–257. [Google Scholar]
- Ascoli, V.; Calisti, R.; Carnovale-Scalzo, C.; Nardi, F. Malignant pleural mesothelioma in bakers and pastry cooks. Am. J. Ind. Med. 2001, 40, 371–373. [Google Scholar] [CrossRef]
- Carugno, M.; Mensi, C.; Sieno, C.; Consonni, D.; Riboldi, L. Asbestos exposure among hairdressers. Med. Lav. 2014, 103, 70–71. [Google Scholar]
- Mensi, C.; Macchione, M.; Terminne, L.; Rivolta, G.; Riboldi, L.; Chiappino, G. Information of the registry of mesothelioma in Lombardy: The asbestos risk in rotogravure. Med. Lav. 2006, 97, 726. (In Italian) [Google Scholar] [PubMed]
- Grandjean, P.; Bach, E. Indirect Exposures: The Significance of Bystanders at Work and at Home. Am. Ind. Hyg. Assoc. J. 2010, 47, 819–824. Available online: https://doi-org.insubria.idm.oclc.org/10.1080/15298668691390719 (accessed on 4 March 2022). [CrossRef] [PubMed]
- Donovan, E.P.; Donovan, B.L.; Sahmel, J.; Scott, P.K.; Paustenbach, D.J. Evaluation of bystander exposures to asbestos in occupational settings: A review of the literature and application of a simple eddy diffusion model. Crit. Rev. Toxicol. 2011, 41, 50–72. [Google Scholar] [CrossRef]
- Mangold, C.; Clark, K.; Madl, A.; Paustenbach, D. An exposure study of bystanders and workers during the installation and removal of asbestos gaskets and packing. J. Occup. Environ. Hyg. 2006, 3, 87–98. [Google Scholar] [CrossRef]
- Scopa, P. Reconstruction of asbestos exposure in workers suffering from pleural neoplasms and employed in sectors not generally associated with high exposure levels: The importance of an accurate standardized assessment of occupational medicine. J. Prev. Med. Hyg. 2021, 62, E148–E151. [Google Scholar] [CrossRef]
- Mensi, C.; Dallari, B.; Polonioli, M.; Riboldi, L.; Consonni, D.; Pesatori, A. Mesothelioma in Agriculture in Lombardy, Italy: An Unrecognized Risk. Int. J. Environ. Res. Public Health 2021, 18, 358. [Google Scholar] [CrossRef]
- McGuire, V.; Nelson, L.M.; Koepsell, T.D.; Checkoway, H.; Longstreth, W.T. Assessment of occupational exposures in community-based case-control studies. Annu. Rev. Public Health 1998, 19, 35–53. [Google Scholar] [CrossRef] [Green Version]
- Siemiatycki, J.; Dewar, R.; Richardson, L. Costs and statistical power associated with five methods of collecting occupation exposure information for population-based case-control studies. Am. J. Epidemiol. 1989, 130, 1236–1246. [Google Scholar] [CrossRef]
- Peters, S.; Vermeulen, R.; Cassidy, A.; ’T Mannetje, A.; Van Tongeren, M.; Boffetta, P.; Straif, K.; Kromhout, H. Comparison of exposure assessment methods for occupational carcinogens in a multi-centre lung cancer case–control study. Occup. Environ. Med. 2011, 68, 148–153. [Google Scholar] [CrossRef]
- ’T Mannetje, A.; Fevotte, J.; Fletcher, T.; Brennan, P.; Legoza, J.; Szeremi, M.; Paldy, A.; Brzeznicki, S.; Gromiec, J.; Ruxanda-Artenie, C.; et al. Assessing exposure misclassification by expert assessment in multicenter occupational studies. Epidemiology 2003, 14, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Peters, S. Although a valuable method in occupational epidemiology, job-exposure matrices are no magic fix. Scand. J. Work. Environ. Health 2020, 46, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Kromhout, H.; Vermeulen, R. Application of job-exposure matrices in studies of the general population: Some clues to their performance. Eur. Respir. Rev. 2001, 11, 80–90. [Google Scholar]
- Petersen, S.B.; Flachs, E.M.; Svendsen, S.W.; Marott, J.L.; Budtz-Jørgensen, E.; Hansen, J.; Stokholm, Z.A.; Schlünssen, V.; Andersen, J.H.; Bonde, J.P. Influence of errors in job codes on job exposure matrix-based exposure assessment in the register-based occupational cohort doc*X. Scand. J. Work. Environ. Health 2020, 46, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Burstyn, I.; Slutsky, A.; Lee, D.G.; Singer, A.B.; An, Y.; Michael, Y.L. Beyond crosswalks: Reliability of exposure assessment following automated coding of free-text job descriptions for occupational epidemiology. Ann. Occup. Hyg. 2014, 58, 482–492. [Google Scholar] [CrossRef] [Green Version]
- Koeman, T.; Offermans, N.S.M.; Christopher-De Vries, Y.; Slottje, P.; Van Den Brandt, P.A.; Goldbohm, R.A.; Kromhout, H.; Vermeulen, R. JEMs and incompatible occupational coding systems: Effect of manual and automatic recoding of job codes on exposure assignment. Ann. Occup. Hyg. 2013, 57, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Rémen, T.; Richardson, L.; Siemiatycki, J.; Lavoué, J. Impact of Variability in Job Coding on Reliability in Exposure Estimates Obtained via a Job-Exposure Matrix. Ann. Work Expo. Health 2021. [Google Scholar] [CrossRef]
- Fadel, M.; Evanoff, B.A.; Andersen, J.H.; D’errico, A.; Dale, A.M.; Leclerc, A.; Descatha, A. Not just a research method: If used with caution, can job-exposure matrices be a useful tool in the practice of occupational medicine and public health? Scand. J. Work. Environ. Health 2020, 46, 552–553. [Google Scholar] [CrossRef]
- Armstrong, B. Effect of measurement error on epidemiological studies of environmental and occupational exposures. Occup. Environ. Med. 1998, 55, 651–656. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Men | Women | |||
|---|---|---|---|---|
| N | % | N | % | |
| Total | 372 | 100 | 190 | 100 |
| Age at diagnosis (years) mean (min-max) | 68.8 | (24.5–94.5) | 69.3 | (41.3–93.1) |
| Period of diagnosis | ||||
| 2000–2009 | 111 | 29.8 | 64 | 33.7 |
| 2010–2019 | 261 | 70.2 | 126 | 66.3 |
| Diagnosis | ||||
| Definite | 367 | 98.7 | 187 | 98.4 |
| Probable | 5 | 1.3 | 3 | 1.6 |
| Morphology (ICD-O code) # | ||||
| MM not otherwise specified (90503) | 6 | 1.6 | 5 | 2.6 |
| Fibrous/sarcomatoid/desmoplastic MM (90513) | 20 | 5.4 | 15 | 7.9 |
| Epithelioid MM (90523) | 262 | 70.4 | 148 | 77.9 |
| Biphasic MM (90533) | 84 | 22.1 | 22 | 11.6 |
| Presence of pleural plaques | 65 | 17.5 | 28 | 14.7 |
| Presence of asbestosis | 8 | 2.1 | 0 | 0.0 |
| Interview | ||||
| Patient | 279 | 75.0 | 131 | 69.0 |
| Relative | 93 | 25.0 | 59 | 31.0 |
| Vital status | ||||
| Dead | 352 | 94.6 | 177 | 92.7 |
| Alive | 20 | 5.4 | 13 | 6.8 |
| Asbestos exposure (ReNaM) | ||||
| Occupational, definite | 247 | 66.4 | 35 | 18.4 |
| Occupational, probable | 3 | 0.8 | 2 | 1.0 |
| Occupational, possible | 24 | 6.4 | 8 | 4.2 |
| Para-occupational | 7 | 1.9 | 18 | 9.5 |
| Home-related | 2 | 0.5 | 10 | 5.3 |
| Environmental | 20 | 5.4 | 42 | 22.1 |
| None identified | 69 | 18.5 | 75 | 39.5 |
| Years since first asbestos exposure (RML) mean (min–max) | 48.8 | (18.5–78.1) | 52.5 | (16.6–85.1) |
| Years since first occupational asbestos exposure (RML) mean (min–max) | 48.1 | (18.5–71.5) | 53.3 | (17.8–69.6) |
| Duration of occupational asbestos exposure (RML) mean (min–max) | 23.6 | (0.5–60.4) | 16.1 | (1.0–43.0) |
| Occupational asbestos exposure: industry * (RML) | ||||
| Metalworking and metallurgy | 92 | 33.6 | 5 | 11.1 |
| Construction | 73 | 26.6 | 0 | 0.0 |
| Asbestos-cement | 32 | 11.7 | 2 | 4.4 |
| Textile and clothing production | 8 | 2.9 | 22 | 48.9 |
| Motor vehicle production | 20 | 7.3 | 0 | 0.0 |
| Transport | 16 | 5.8 | 0 | 0.0 |
| Chemical | 15 | 5.5 | 0 | 0.0 |
| Railroad production and maintenance | 15 | 5.5 | 0 | 0.0 |
| Food and beverage | 11 | 4.0 | 2 | 4.4 |
| Health and social services | 4 | 1.5 | 8 | 17.8 |
| Military | 10 | 3.6 | 0 | 0.0 |
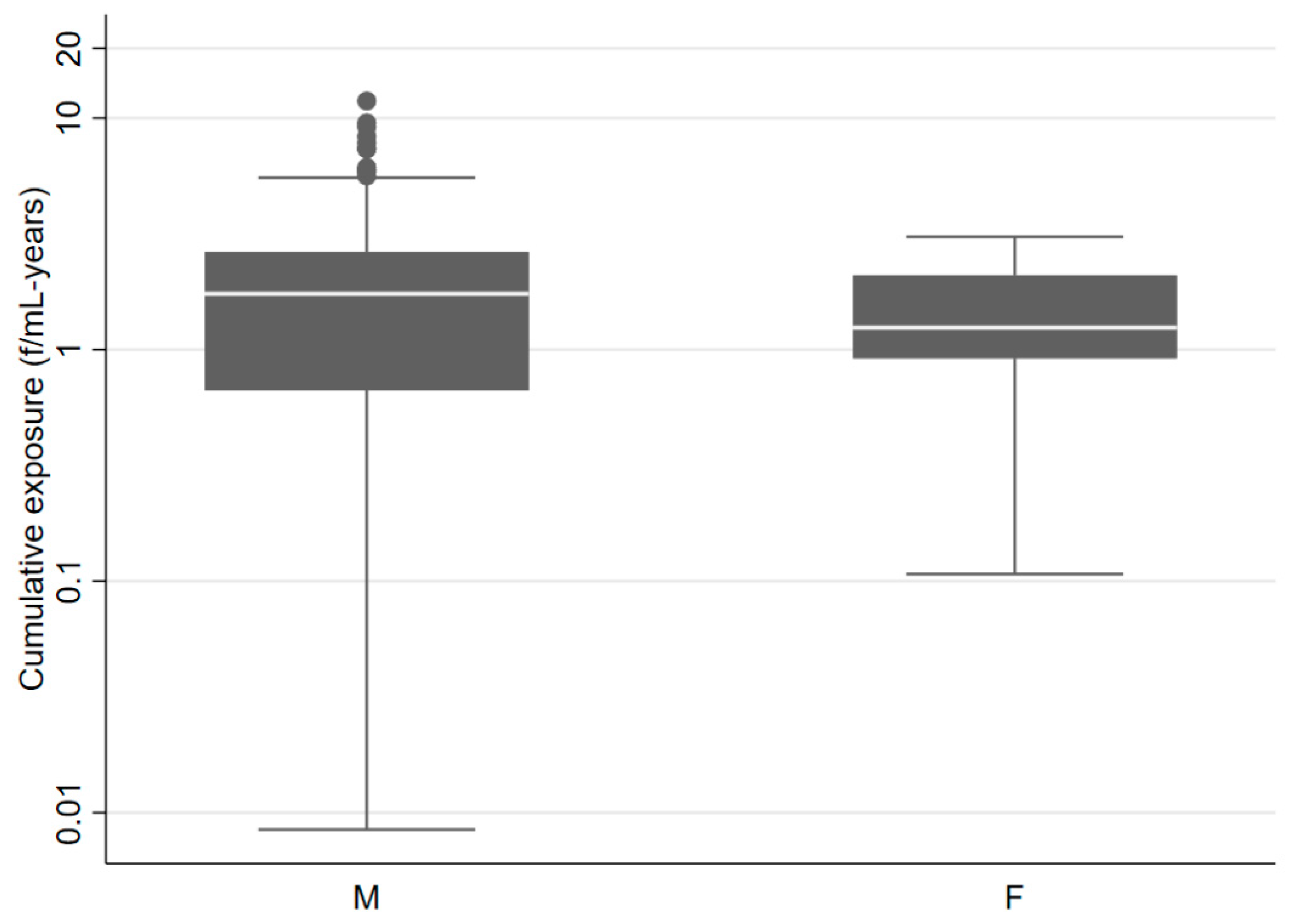
| Occupational asbestos exposure (SYN-JEM) | ||||
| Ever | 225 | 60.5 | 25 | 13.2 |
| Cumulative (f/mL-years) median (min–max) | 1.7 | (0.01–11.9) | 1.2 | (0.1–3.1) |
| Duration (years) median (min–max) | 24.5 | (1–61) | 11.4 | (2.0–28.0) |
| Occupational | Men | Women | All | |||
|---|---|---|---|---|---|---|
| Asbestos Exposure | RML | RML | RML | |||
| Ever | Never | Ever | Never | Ever | Never | |
| SYN-JEM | ||||||
| Ever | 200 | 25 | 8 | 17 | 208 | 42 |
| Never | 74 | 73 | 37 | 128 | 111 | 201 |
| Sensitivity | 0.73 | 0.18 | 0.65 | |||
| 95% CI * | 0.67; 0.78 | 0.09; 0.32 | 0.60; 0.70 | |||
| Specificity | 0.75 | 0.88 | 0.83 | |||
| 95% CI * | 0.65; 0.82 | 0.82; 0.93 | 0.77; 0.87 | |||
| Cohen’s kappa | 0.41 | 0.07 | 0.46 | |||
| 95% CI | 0.34; 0.48 | −0.01; 0.15 | 0.39; 0.53 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinazzè, A.; Consonni, D.; Borghi, F.; Rovelli, S.; Cattaneo, A.; Zellino, C.; Dallari, B.; Pesatori, A.C.; Kromhout, H.; Peters, S.; et al. Asbestos Exposure in Patients with Malignant Pleural Mesothelioma included in the PRIMATE Study, Lombardy, Italy. Int. J. Environ. Res. Public Health 2022, 19, 3390. https://doi.org/10.3390/ijerph19063390
Spinazzè A, Consonni D, Borghi F, Rovelli S, Cattaneo A, Zellino C, Dallari B, Pesatori AC, Kromhout H, Peters S, et al. Asbestos Exposure in Patients with Malignant Pleural Mesothelioma included in the PRIMATE Study, Lombardy, Italy. International Journal of Environmental Research and Public Health. 2022; 19(6):3390. https://doi.org/10.3390/ijerph19063390
Chicago/Turabian StyleSpinazzè, Andrea, Dario Consonni, Francesca Borghi, Sabrina Rovelli, Andrea Cattaneo, Carolina Zellino, Barbara Dallari, Angela Cecilia Pesatori, Hans Kromhout, Susan Peters, and et al. 2022. "Asbestos Exposure in Patients with Malignant Pleural Mesothelioma included in the PRIMATE Study, Lombardy, Italy" International Journal of Environmental Research and Public Health 19, no. 6: 3390. https://doi.org/10.3390/ijerph19063390
APA StyleSpinazzè, A., Consonni, D., Borghi, F., Rovelli, S., Cattaneo, A., Zellino, C., Dallari, B., Pesatori, A. C., Kromhout, H., Peters, S., Riboldi, L., Cavallo, D. M., & Mensi, C. (2022). Asbestos Exposure in Patients with Malignant Pleural Mesothelioma included in the PRIMATE Study, Lombardy, Italy. International Journal of Environmental Research and Public Health, 19(6), 3390. https://doi.org/10.3390/ijerph19063390