
Efficacy of the Virtual Reality Intervention VR FestLab on Alcohol Refusal Self-Efficacy: A Cluster-Randomized Controlled Trial

 ,
,  , and
, and 
Abstract
1. Introduction
Aims and Objectives
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Data Collection
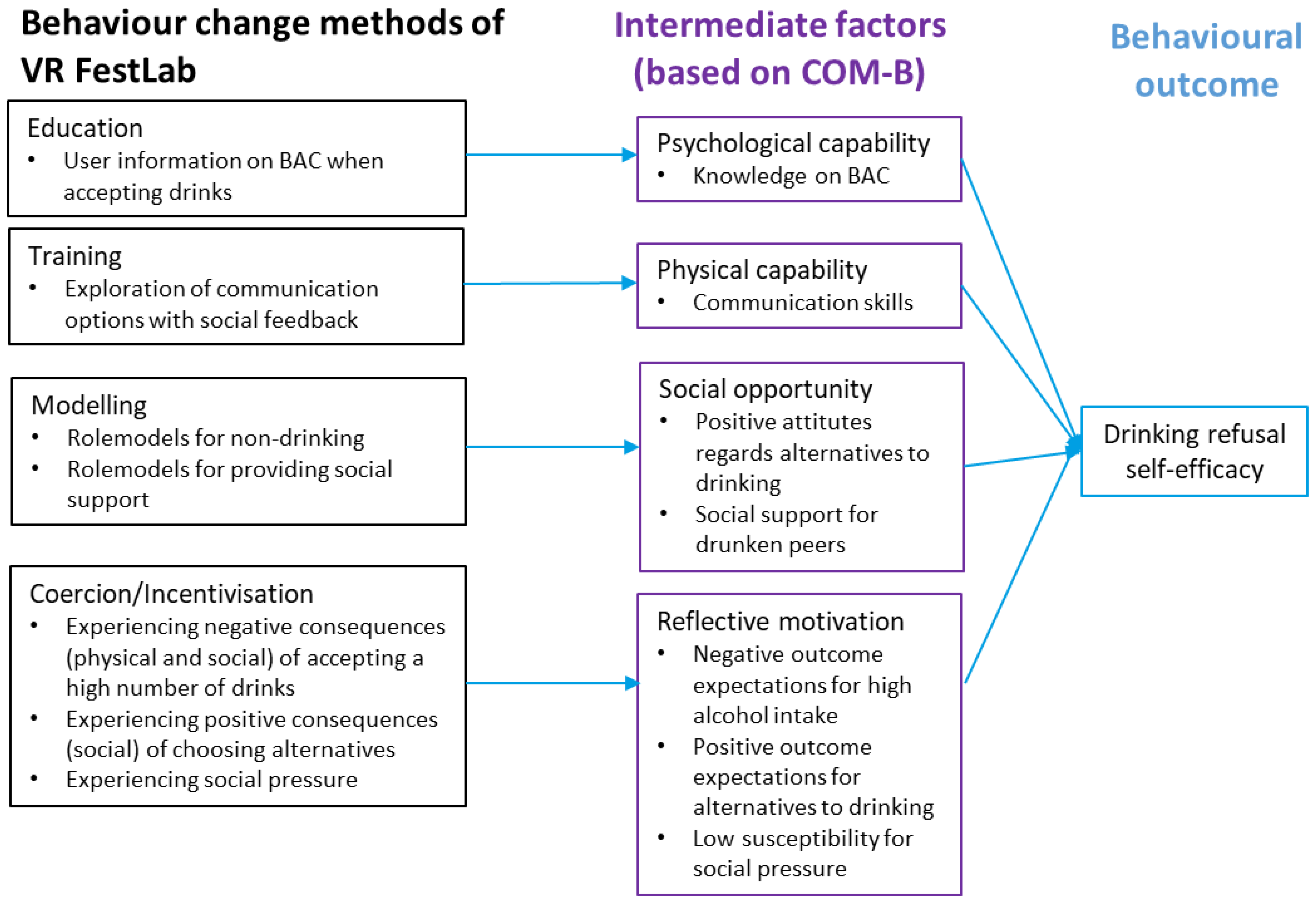
2.4. VR FestLab: An Alcohol Prevention Intervention
2.4.1. Gameplay Session
2.4.2. Intervention Schools
2.4.3. Active Control Intervention
2.5. Questionnaires and Outcomes

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Data Collection Time | Question | Original Response Categories | Collapsed Response Categories |
|---|---|---|---|---|
| Sex | T0 | Are you a girl or a boy? (State what you most identify as right now) | Boy/Girl | None |
| Age | T0 | How old are you? | ||
| Perceived family affluence | T0 | How well-off do you think your family is? | Very well-off/Quite well-off/Average/ Not so well-off/ Not at all well-off | Low to medium (Not at all well-off/Not so well-off/ average) High (Quite well-off/ Very well-off) |
| Lifetime binge drinking | T0 | Have you ever drank five or more drinks on a single occasion? | Yes/No | None |
| Sensation seeking | T0 | Eight-item Brief Sensation-Seeking Scale (BSSS) | Five-point Likert scale from disagree strongly to agree strongly | Sum score |
| Potential adverse effects | T1 | Did you experience any side effects when trying VR FestLab? | Open question | Responses grouped into the categories of; no side effects, cybersickness (from symptoms of cybersickness [36,37]), physical distress from wearing the VR equipment [38], and other symptoms/not specified |
| Drinking refusal self-efficacy | T0/T1/T2 | Five-item Social Pressure subscale of the Drinking Refusal Self-Efficacy Questionnaire (DRSEQ-RA) | Six-point Likert scale from “I am very sure I could NOT resist drinking” to “I am very sure I could resist drinking” | Sum score |
| Drug refusal skills | T0/T1/T2 | Seven-item drug refusal skills subscale from the Brief Assessment life skills Training Tool | Not refuse/likely not refuse/likely refuse/refuse | Sum score |
| Knowledge/Awareness of blood alcohol concentration | T0/T1/T2 | “It is easy for me to estimate my own alcohol tolerance”, “I know how much alcohol I can drink before I get drunk” | Five-point Likert scale from disagree strongly to agree strongly | Sum score |
| Communication skills | T0/T1/T2 | “If my best friends want me to drink beer with them and I don’t want to, I have ways to say no” “If someone offers me a drink of alcohol and I say “no”, I can make them take “no” for an answer” | Same | Sum score |
| Social support willingness | T0/T1/T2 | “If someone is really drunk or sick at a party, the best thing to do is…” | Let him or her recover alone (0 point)/Help him or her to recover (1 point)/Ask an adult for help (1 point)/Call his or her parents (1 point) | Sum score for each item ticked |
| Susceptibility to peer pressure | T0/T1/T2 | “If I am at a party and my friends are drinking alcohol, I would feel left out if I were not drinking alcohol.” | Same | Item score |
| Outcome expectations | T0/T1/T2 | How much do you agree that the following happens to you if you drink alcohol? I become more fun/more happy I become more extroverted I become more confident I forget my problems | Five-point Likert scale from disagree strongly to agree strongly | Sum score |
2.5.1. Content of the Baseline Questionnaire (T0)
Primary Outcome Measure
Secondary Outcome Measures
2.5.2. Content of the Follow-Up Questionnaires
2.5.3. Questionnaire Development and Validation
2.6. Sample Size Calculation
2.7. Randomisation and Blinding
2.8. Statistical Analysis
3. Results
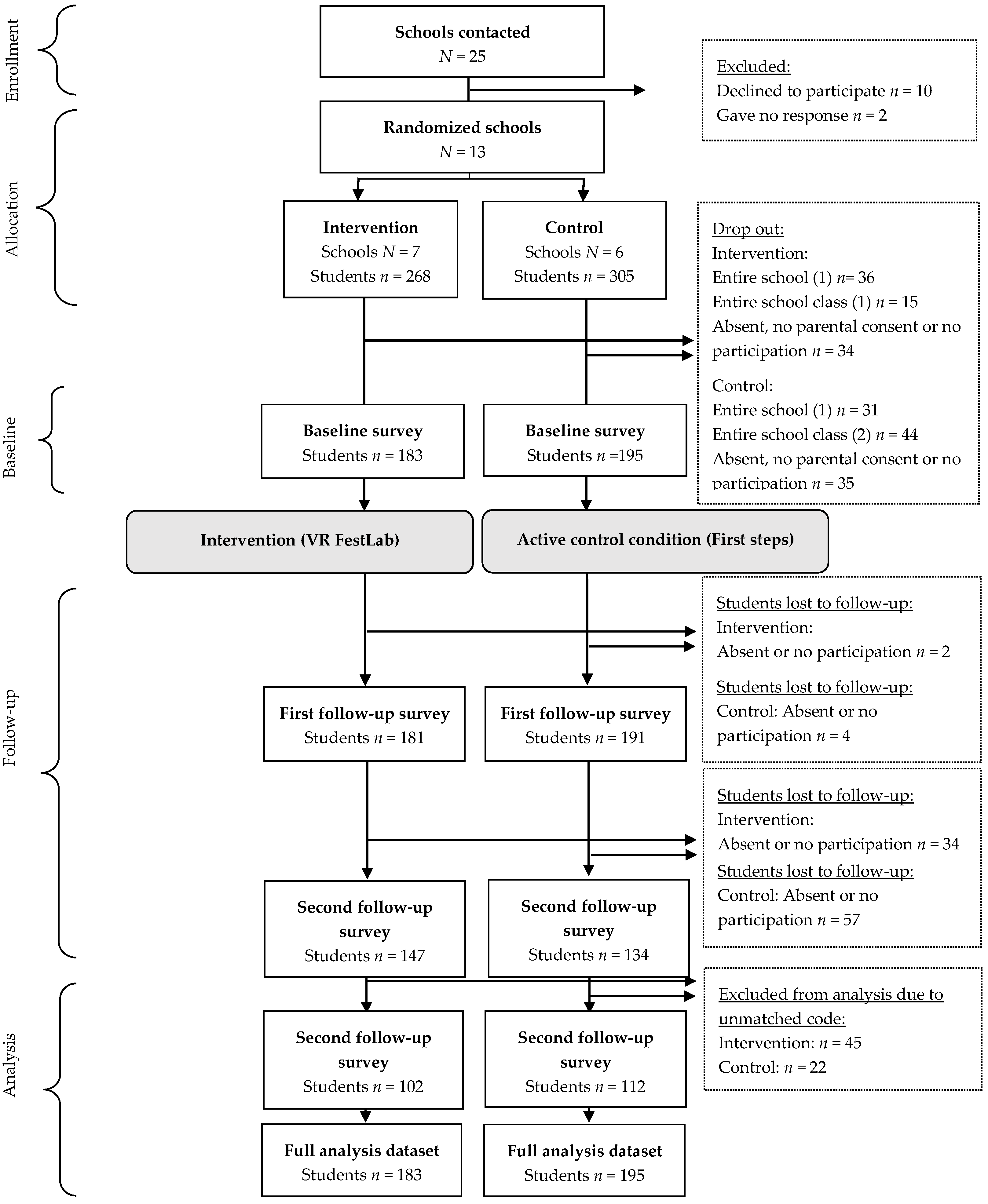
3.1. Participant Flow and Recruitment
3.2. Student Characteristics
3.3. Outcome Measures at T0, T1, and T2
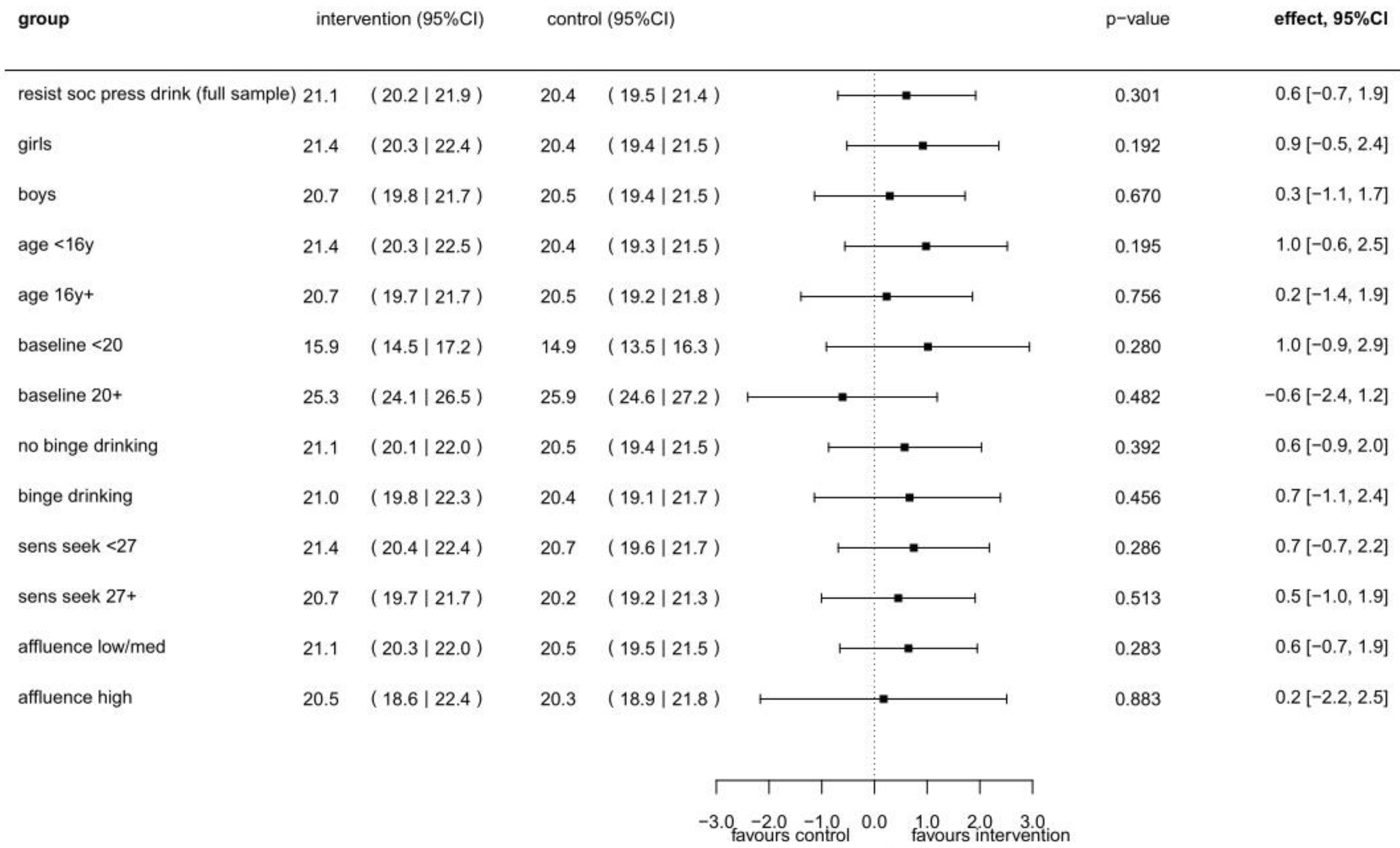
3.4. Multilevel Intervention Effects for the Primary Outcome and Sub-Group Effects at First Follow-Up
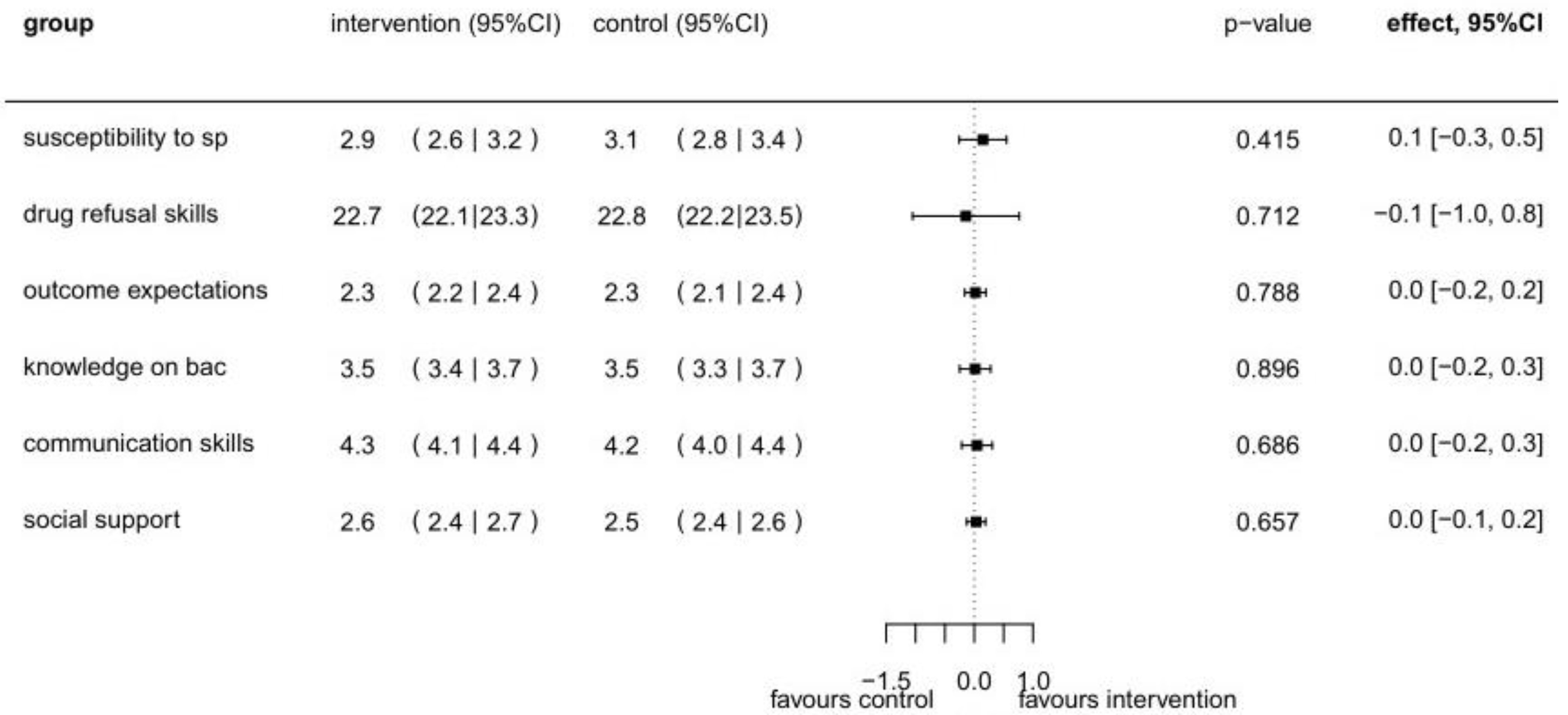
3.5. Multilevel Intervention Effects for Secondary Outcomes at First Follow-Up
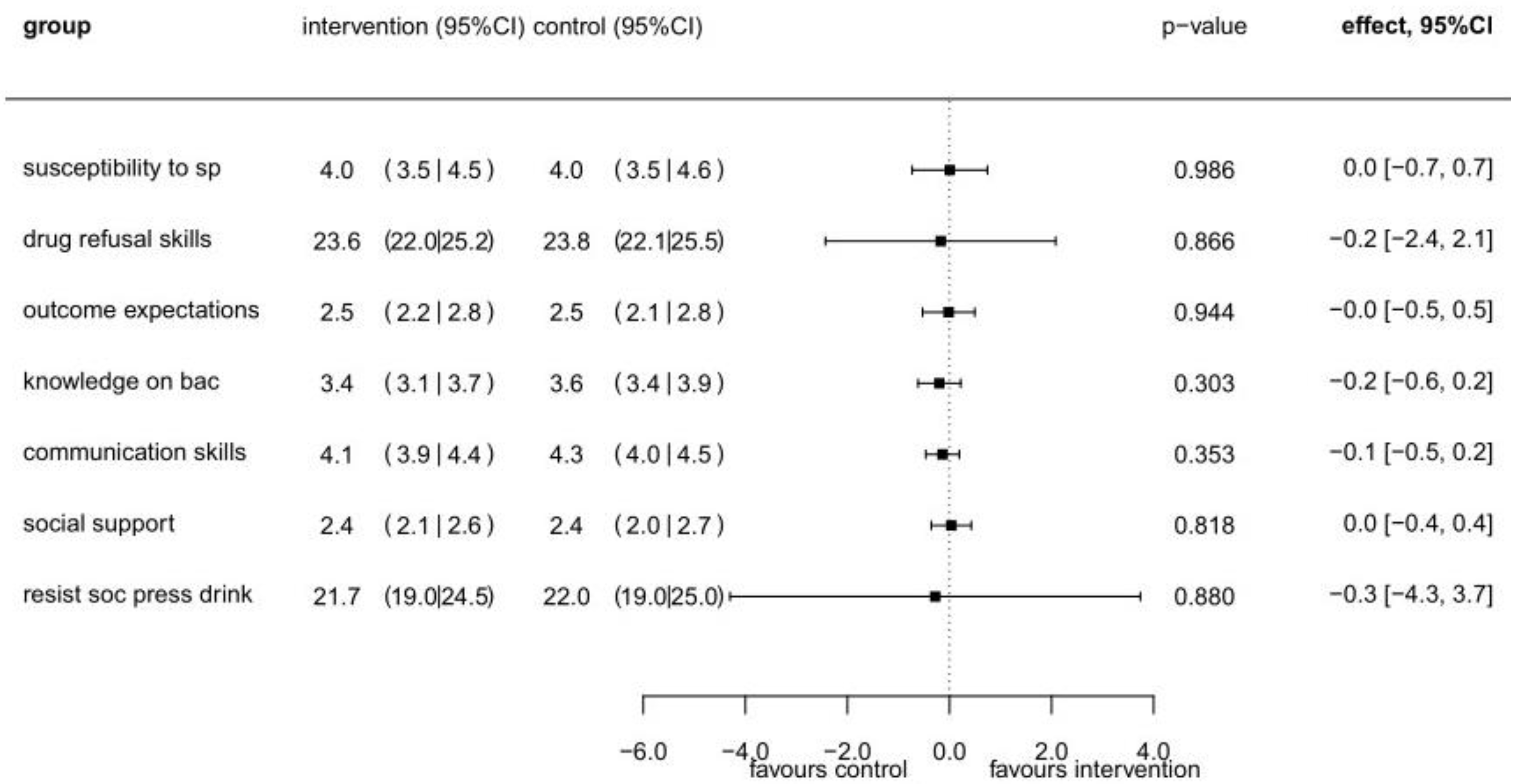
3.6. Multilevel Intervention Effects at Second Follow-Up
3.7. Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
Appendix A

References
- ESPAD Group. ESPAD report 2019: Results from the European School Survey Project on Alcohol and other Drugs; EMCDDA Joint Publications Publications Office of the European Union: Luxembourg, 2020. [Google Scholar]
- Meyer, M.; Lundgaard, P.; Zachariasen, E.; Christensen, A. Unges Alkoholvaner i Danmark 2019; Young People’s Alcohol Habits in Denmark 2019; Kræftens Bekæmpelse og TrygFonden smba (TryghedsGruppen smba): Copenhagen, Denmark, 2020. [Google Scholar]
- Babor, T.; Caetano, R.; Casswell, S.; Edwards, G.; Giesbrecht, N.; Graham, K. Alcohol: No ordinary commodity—A summary of the second edition. Addiction 2010, 105, 769–779. [Google Scholar] [CrossRef]
- Wechsler, H. Health and behavioral consequences of binge drinking in college: A national survey of students at 140 campuses. JAMA 1994, 7, 1672–1677. [Google Scholar] [CrossRef]
- Hingson, R.; White, A. New research findings since the 2007. Surgeon general’s call to action to prevent and reduce Underage drinking: A review. J. Stud. Alcohol. Drugs 2014, 75, 158–169. [Google Scholar] [CrossRef]
- Flory, K.; Lynam, D.; Milich, R.; Leukefeld, C.; Clayton, R. Early adolescent through young adult alcohol and marijuana use trajectories: Early predictors, young adult outcomes, and predictive utility. Dev. Psychopathol. 2004, 16, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Grant, B.F.; Stinson, F.S.; Harford, T.C. Age at onset of alcohol use and DSM-IV alcohol abuse and dependence: A 12-year follow-up. J. Subst. Abuse 2001, 13, 493–504. [Google Scholar] [CrossRef]
- Jennison, K.M. The short-term effects and unintended long-term consequences of binge drinking in college: A 10-year follow-up study. Am. J. Drug Alcohol. Abuse 2004, 30, 659–684. [Google Scholar] [CrossRef] [PubMed]
- Inchley, J.; Currie, D.; Vieno, A.; Torsheim, T.; Ferreira-Borges, C.; Weber, M.; Barnekow, V.; Breda, J. Adolescent Alcohol-Related Behaviours: Trends and Inequalities in the WHO European Region, 2002–2014; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Griffin, K.W.; Botvin, G.J. Evidence-based interventions for preventing substance use disorders in adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 2010, 19, 505–526. [Google Scholar] [CrossRef]
- Hendricks, G.; Savahl, S.; Florence, M. Adolescent peer pressure, leisure boredom, and substance use in low-income Cape Town communities. Soc. Behav. Personal. Int. J. 2015, 43, 99–109. [Google Scholar] [CrossRef]
- Sankar, M.; Maha, M.; Padmapriya, M. Peer pressure in alcohol abuse of adolescence. Int. J. Multidiscip Educ. Res. 2020, 9, 126. [Google Scholar]
- Faggiano, F.; Minozzi, S.; Versino, E.; Buscemi, D. Universal School-Based Prevention for Illicit Drug Use. Cochrane Database Syst. Rev. Cochrane Drugs and Alcohol Group, Ed.; 2014. Available online: https://doi.wiley.com/10.1002/14651858.CD003020.pub3 (accessed on 10 December 2021).
- Young, R.M.; Oei, T.P.S. The predictive utility of drinking refusal self-efficacy and alcohol expectancy. Addict. Behav. 2000, 25, 415–421. [Google Scholar] [CrossRef]
- Oei, T.P.S.; Morawska, A. A cognitive model of binge drinking: The influence of alcohol expectancies and drinking refusal self-efficacy. Addict. Behav. 2004, 29, 159–179. [Google Scholar] [CrossRef]
- Scheier, L.M.; Botvin, G.J.; Diaz, T.; Griffin, K.W. Social skills, competence, and drug refusal efficacy as predictors of adolescent alcohol use. J. Drug Educ. 1999, 29, 251–278. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, S.I.; Graham, J.W.; Piccinin, A.M.; Hansen, W.B. Resistance-skills training and onset of alcohol use: Evidence for beneficial and potentially harmful effects in public schools. In Addictive Behaviors: Readings on Etiology, Prevention, and Treatment; Marlatt, G.A., VandenBos, G.R., Eds.; American Psychological Association: Washington, DC, USA, 1997; pp. 215–238. [Google Scholar]
- Compton, J.; Jackson, B.; Dimmock, J.A. Persuading others to avoid persuasion: Inoculation theory and resistant health attitudes. Front. Psychol. 2016, 7, 122. [Google Scholar] [CrossRef] [PubMed]
- Onrust, S.A.; Otten, R.; Lammers, J.; Smit, F. School-based programmes to reduce and prevent substance use in different age groups: What works for whom? Systematic review and meta-regression analysis. Clin. Psychol. Rev. 2016, 44, 45–59. [Google Scholar] [CrossRef]
- Steinberg, L.; Monahan, K.C. Age differences in resistance to peer influence. Dev. Psychol. 2007, 43, 1531–1543. [Google Scholar] [CrossRef]
- Durl, J.; Dietrich, T.; Pang, B.; Potter, L.E.; Carter, L. Utilising virtual reality in alcohol studies: A systematic review. Health Educ. J. 2018, 77, 212–225. [Google Scholar] [CrossRef]
- Au, E.H.; Lee, J.J. Virtual reality in education: A tool for learning in the experience age. Int. J. Innov. Educ. 2017, 4, 215. [Google Scholar] [CrossRef]
- Barko, T.; Sadler, T.D. Practicality in virtuality: Finding student meaning in video game education. J. Sci. Educ. Technol. 2013, 22, 124–132. [Google Scholar] [CrossRef]
- McGrath, D.; Wegener, M.; McIntyre, T.J.; Savage, C.; Williamson, M. Student experiences of virtual reality: A case study in learning special relativity. Am. J. Phys. 2010, 78, 862–868. [Google Scholar] [CrossRef]
- Dietrich, T.; Rundle-Thiele, S.; Kubacki, K.; Durl, J.; Gullo, M.J.; Arli, D.; Connor, J.P. Virtual reality in social marketing: A process evaluation. Mark. Intell. Plan. 2019, 37, 806–820. [Google Scholar] [CrossRef]
- Weser, V.U.; Duncan, L.R.; Sands, B.E.; Schartmann, A.; Jacobo, S.; François, B.; Hieftje, K.D. Evaluation of a virtual reality E-cigarette prevention game for adolescents. Addict. Behav. 2021, 122, 107027. [Google Scholar] [CrossRef] [PubMed]
- Weser, V.U.; Duncan, L.R.; Pendergrass, T.M.; Fernandes, C.S.; Fiellin, L.E.; Hieftje, K.D. A quasi-experimental test of a virtual reality game prototype for adolescent E-Cigarette prevention. Addict. Behav. 2021, 112, 106639. [Google Scholar] [CrossRef]
- Norris, A.E.; Hughes, C.; Hecht, M.; Peragallo, N.; Nickerson, D. Randomized trial of a peer resistance skill-building game for hispanic early adolescent girls. Nurs. Res. 2013, 62, 25–35. [Google Scholar] [CrossRef]
- Prediger, C.; Helmer, S.M.; Hrynyschyn, R.; Stock, C. Virtual reality-based alcohol prevention in adolescents: A systematic review. Adolescents 2021, 1, 138–150. [Google Scholar] [CrossRef]
- Hadley, W.; Houck, C.D.; Barker, D.H.; Garcia, A.M.; Spitalnick, J.S.; Curtis, V.; Roye, S.; Brown, L.K. Eliciting affect via immersive virtual reality: A tool for adolescent risk reduction. J. Pediatr. Psychol. 2014, 39, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Rundle-Thiele, S.; Schuster, L.; Dietrich, T.; Russell-Bennett, R.; Drennan, J.; Leo, C.; Connor, J.P. Maintaining or changing a drinking behavior? GOKA’s short-term outcomes. J. Bus. Res. 2015, 68, 2155–2163. [Google Scholar] [CrossRef]
- Lyk, P.B.; Majgaard, G.; Vallentin-Holbech, L.; Guldager, J.D.; Dietrich, T.; Rundle-Thiele, S.; Stock, C. Co-designing and learning in virtual reality: Development of tool for alcohol resistance training. Electron. J. E-Learn 2020, 18, 219–223. [Google Scholar] [CrossRef]
- Vallentin-Holbech, L.; Guldager, J.D.; Dietrich, T.; Rundle-Thiele, S.; Majgaard, G.; Lyk, P.; Stock, C. Co-creating a virtual alcohol prevention simulation with young people. Int. J. Environ. Res. Public Health 2020, 17, 1097. [Google Scholar] [CrossRef]
- Michie, S.; Van Stralen, M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 1–12. [Google Scholar] [CrossRef]
- Stock, C.; Guldager, J.D.; Grittner, U. Statistical Analysis Plan: “Efficacy Testing of the VR-Game ‘VR FestLab’—Does a VR Based Game Improve Alcohol Resistance Skills Among Adolescents?”, Figshare. 2021. Available online: https://figshare.com/articles/online_resource/Statistical_Analysis_Plan/14141114 (accessed on 10 November 2021).
- Davis, S.; Nesbitt, K.; Nalivaiko, E. A Systematic Review of Cybersickness. In Proceedings of the 2014 Conference on Interactive Entertainment, Newcastle, NSW, Australia, 2–3 December 2014; pp. 1–9. Available online: https://dl.acm.org/doi/10.1145/2677758.2677780 (accessed on 1 September 2021).
- Rebenitsch, L.; Owen, C. Review on cybersickness in applications and visual displays. Virtual Real. 2016, 20, 101–125. [Google Scholar] [CrossRef]
- McCauley, M.E.; Sharkey, T.J. Cybersickness: Perception of self-motion in virtual environments. Presence. Teleoperators Virtual Environ. 1992, 1, 311–318. [Google Scholar] [CrossRef]
- Young, R.M.; Hasking, P.A.; Oei, T.P.S.; Loveday, W. Validation of the drinking refusal self-efficacy questionnaire—Revised in an adolescent sample (DRSEQ-RA). Addict. Behav. 2007, 32, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Macaulay, A.P.; Griffin, K.W.; Botvin, G.J. Initial internal reliability and descriptive statistics for a brief assessment tool for the life skills training drug-abuse prevention program. Psychol. Rep. 2002, 91, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Shope, J.T.; Copeland, L.A.; Maharg, R.; Dielman, T.E.; Butchart, A.T. Assessment of adolescent refusal skills in an alcohol misuse prevention study. Health Educ. Q. 1993, 20, 373–390. [Google Scholar] [CrossRef] [PubMed]
- Dielman, T.E.; Campanelli, P.C.; Shope, J.T.; Butchart, A.T. Susceptibility to peer pressure, self-esteem, and health locus of control as correlates of adolescent substance abuse. Health Educ. Q. 1987, 14, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Bendtsen, P.; Mikkelsen, S.; Tolstrup, J. Ungdomsprofilen 2014: Sundhedsadfærd, Helbred og Trivsel Blandt Elever på Ungdomsuddannelser; Youth Profile 2014: Health Behaviour, Health and Well-Being among Pupils in Secondary Education; University of Southern Denmark, National Institute of Public Health: Copenhagen, Denmark, 2015. [Google Scholar]
- Currie, C.; Inchley, J.; Molcho, M.; Lenzi, M.; Veselska, Z.; Wild, F. Health Behaviour in School-Aged Children (HBSC) Study Protocol: Background, Methodology and Mandatory Items for the 2013/14 Survey; Child and Adolescent Health Research Unit (CAHRU): St Andrews, UK, 2014. [Google Scholar]
- Kraus, L.; Nociar, A. ESPAD Report 2015—Results from the European School Survey Project on Alcohol and other Drugs; European Monitoring Centre for Drugs and Drug Addiction, Publications office of the European Union: Luxembourg, 2016.
- Hoyle, R.H.; Stephenson, M.T.; Palmgreen, P.; Lorch, E.P.; Donohew, R.L. Reliability and validity of a brief measure of sensation seeking. Personal. Individ. Differ. 2002, 32, 401–414. [Google Scholar] [CrossRef]
- LaViola, J.J. A discussion of cybersickness in virtual environments. ACM SIGCHI Bull. 2000, 32, 47–56. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 5; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 4 December 2021).
- Ehret, P.J.; Ghaidarov, T.M.; LaBrie, J.W. Can you say no? Examining the relationship between drinking refusal self-efficacy and protective behavioral strategy use on alcohol outcomes. Addict. Behav. 2013, 38, 1898–1904. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; The R Foundation: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 4 July 2021).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. arXiv Prepr. 2014, arXiv:1406.5823. [Google Scholar]
- Lenth, R.V. Emmeans: Estimated Marginal Means, aka Least-Squares Means. R Package Version 1.7.0. 2021, 3. Available online: https://CRAN.R-project.org/package=emmeans (accessed on 11 June 2021).
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Guldager, J.D.; Kjær, S.L.; Lyk, P.; Dietrich, T.; Rundle-Thiele, S.; Majgaard, G.; Stock, C. User experiences with a virtual alcohol prevention simulation for danish adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6945. [Google Scholar] [CrossRef]
- Veltri, N.; Krasnova, H.; Baumann, A.; Kalayamthanam, N. Gender differences in online gaming: A literature review. In Proceedings of the Twentieth Americas Conference on Information Systems, Savannah, GA, USA, 7–9 August 2014. [Google Scholar]
- Wood, S.; Bellis, M. Socio-Economic Inequalities in Alcohol Consumption and Harm: Evidence for Effective Interventions and Policy Across EU Countries; European Commission: Brussels, Belgium, 2017.
- Limone, P.; Toto, G.A. Psychological and emotional effects of digital technology on children in COVID-19 pandemic. Brain. Sci. 2021, 11, 1126. [Google Scholar] [CrossRef]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors associated with virtual reality sickness in head-mounted displays: A systematic review and meta-analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef]
- Toto, G.A. From educational contexts to addictions: The role of technology in teaching methodologies and in prevention as an educational function. J. E-Learn Knowl. Soc. 2018, 14, 203–212. [Google Scholar] [CrossRef]
- Danish Health Authority. COVID-19 i Danmark, Status Ved Indgang Til 5. Epidemiuge; Danish health authority: COVID-19 in Denmark, Status in the 5th week of epidemy; Sundhedsstyrelsen: Copenhagen, Denmark, 2020.




| Intervention | Control | Total Cohort | ||||
|---|---|---|---|---|---|---|
| (n = 183) | (n = 195) | (n = 378) | ||||
| n | % | n | % | n | % | |
| Sex | ||||||
| Male | 92 | 50.3 | 94 | 48.2 | 186 | 49.2 |
| Female | 91 | 49.7 | 101 | 51.8 | 192 | 50.8 |
| Age | ||||||
| 14 | 8 | 4.4 | 4 | 2.1 | 12 | 3.2 |
| 15 | 63 | 34.4 | 90 | 46.2 | 153 | 40.5 |
| 16 | 96 | 52.5 | 68 | 34.9 | 164 | 43.4 |
| 17 | 15 | 8.2 | 31 | 15.9 | 46 | 12.2 |
| 18 | 1 | 0.5 | 2 | 1.0 | 3 | 0.8 |
| Perceived family affluence | ||||||
| Low to medium a | 160 | 87.4 | 159 | 81.5 | 319 | 84.4 |
| High b | 23 | 12.6 | 36 | 18.5 | 59 | 15.6 |
| Lifetime binge drinking | ||||||
| No | 47 | 25.7 | 54 | 27.7 | 101 | 26.7 |
| Yes | 136 | 74.3 | 141 | 72.3 | 277 | 73.3 |
| Intervention | Control | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |||||||
| (n = 183) | (n = 181) | (n = 102) | (n = 195) | (n = 191) | (n = 112) | |||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Drinking refusal self-efficacy (Range: 5–30) | 20.2 | 6.7 | 21.2 | 6.9 | 22.3 | 6.8 | 20.0 | 7.0 | 20.4 | 7.4 | 21.5 | 6.3 |
| Drug refusal skills (Range: 7–28) | 22.9 | 5.4 | 22.7 | 5.2 | 24.0 | 5.1 | 22.9 | 5.3 | 22.9 | 5.2 | 23.3 | 4.6 |
| Knowledge/awareness of blood alcohol concentration (Range: 2–10) | 3.6 | 0.9 | 3.6 | 0.9 | 3.5 | 1.0 | 3.4 | 1.1 | 3.5 | 1.1 | 3.6 | 1.0 |
| Communication skills (Range: 2–10) | 4.3 | 0.9 | 4.2 | 0.9 | 4.2 | 0.9 | 4.3 | 0.8 | 4.2 | 0.9 | 4.3 | 0.7 |
| Social support willingness (Range: 0–4) | 2.5 | 0.9 | 2.6 | 0.9 | 2.5 | 0.9 | 2.5 | 0.8 | 2.5 | 0.8 | 2.4 | 0.9 |
| Susceptibility to peer pressure (Range: 1–5) | 2.7 | 1.3 | 2.8 | 1.3 | 3.0 | 1.3 | 3.2 | 1.4 | 3.2 | 1.4 | 3.2 | 1.2 |
| Outcome expectations (Range: 1–5) | 2.2 | 0.9 | 2.3 | 0.9 | 2.4 | 0.9 | 2.3 | 1.0 | 2.3 | 0.9 | 2.4 | 1.0 |
| Intervention | Control | Total Cohort | |||||||
|---|---|---|---|---|---|---|---|---|---|
| (n = 181) | (n = 191) | (n = 372) | |||||||
| n | % | (95% CI) | n | % | (95% CI) | n | % | (95% CI) | |
| None | 141 | 77.9 | 71.2–83.7 | 152 | 79.6 | 73.2–85.1 | 293 | 78.8 | 74.3–82.8 |
| Yes, symptoms of cybersickness | 33 | 18.2 | 12.9–24.6 | 32 | 16.8 | 11.8–22.8 | 65 | 17.5 | 13.8–21.7 |
| Yes, other symptoms/not specified | 4 | 2.2 | 0.6–5.6 | 3 | 1.6 | 0.3–4. | 7 | 1.9 | 0.8–3.8 |
| Yes, physical distress on face from wearing the VR equipment | 4 | 2.2 | 0.6–5.6 | 6 | 3.1 | 1.2–6.7 | 10 | 2.7 | 1.3–4.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guldager, J.D.; Kjær, S.L.; Grittner, U.; Stock, C. Efficacy of the Virtual Reality Intervention VR FestLab on Alcohol Refusal Self-Efficacy: A Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 3293. https://doi.org/10.3390/ijerph19063293
Guldager JD, Kjær SL, Grittner U, Stock C. Efficacy of the Virtual Reality Intervention VR FestLab on Alcohol Refusal Self-Efficacy: A Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(6):3293. https://doi.org/10.3390/ijerph19063293
Chicago/Turabian StyleGuldager, Julie Dalgaard, Satayesh Lavasani Kjær, Ulrike Grittner, and Christiane Stock. 2022. "Efficacy of the Virtual Reality Intervention VR FestLab on Alcohol Refusal Self-Efficacy: A Cluster-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 6: 3293. https://doi.org/10.3390/ijerph19063293
APA StyleGuldager, J. D., Kjær, S. L., Grittner, U., & Stock, C. (2022). Efficacy of the Virtual Reality Intervention VR FestLab on Alcohol Refusal Self-Efficacy: A Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(6), 3293. https://doi.org/10.3390/ijerph19063293