
Assessing Entomological and Epidemiological Efficacy of Pyriproxyfen-Treated Ovitraps in the Reduction of Aedes Species: A Quasi-Experiment on Dengue Infection Using Saliva Samples

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
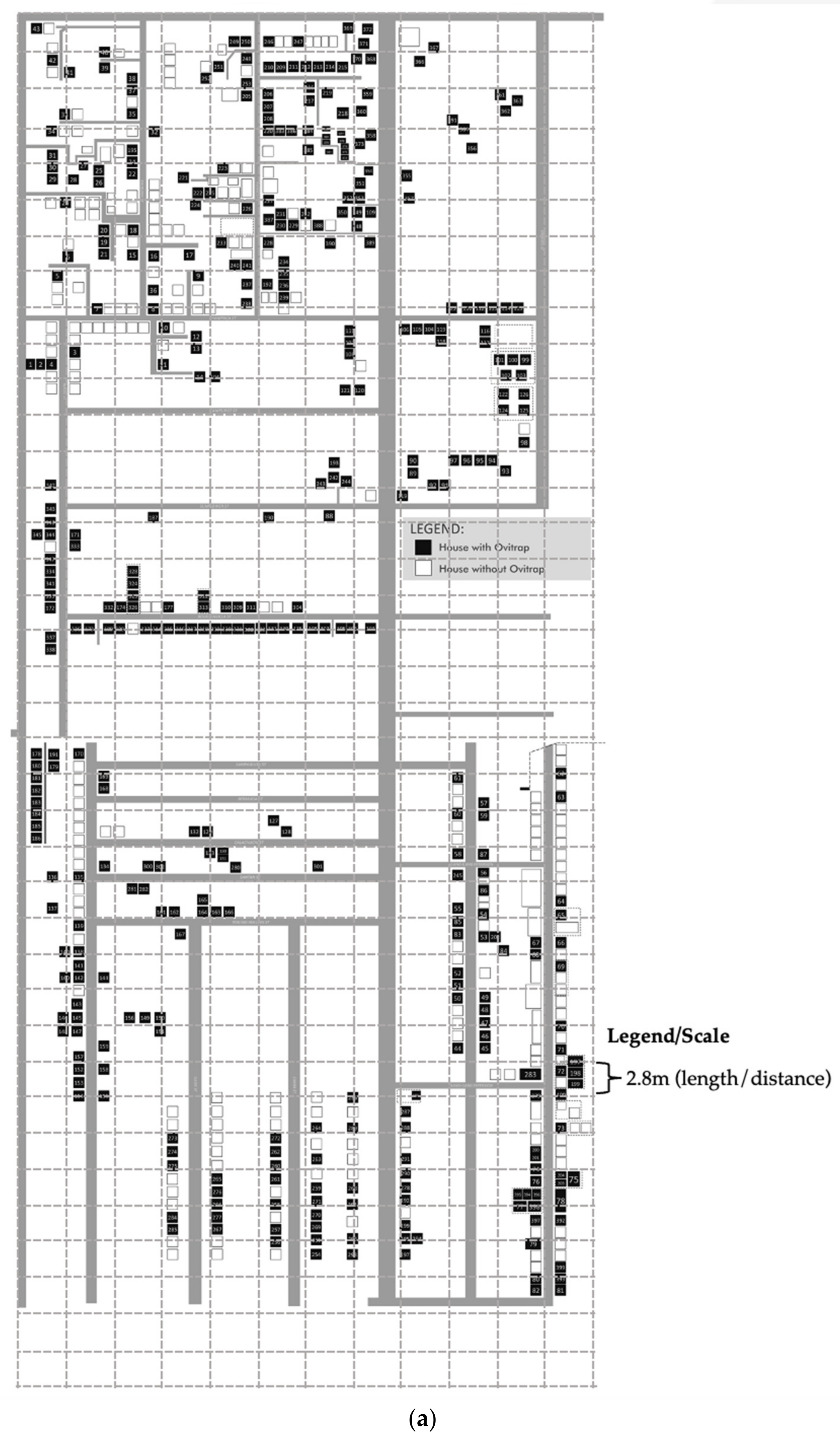
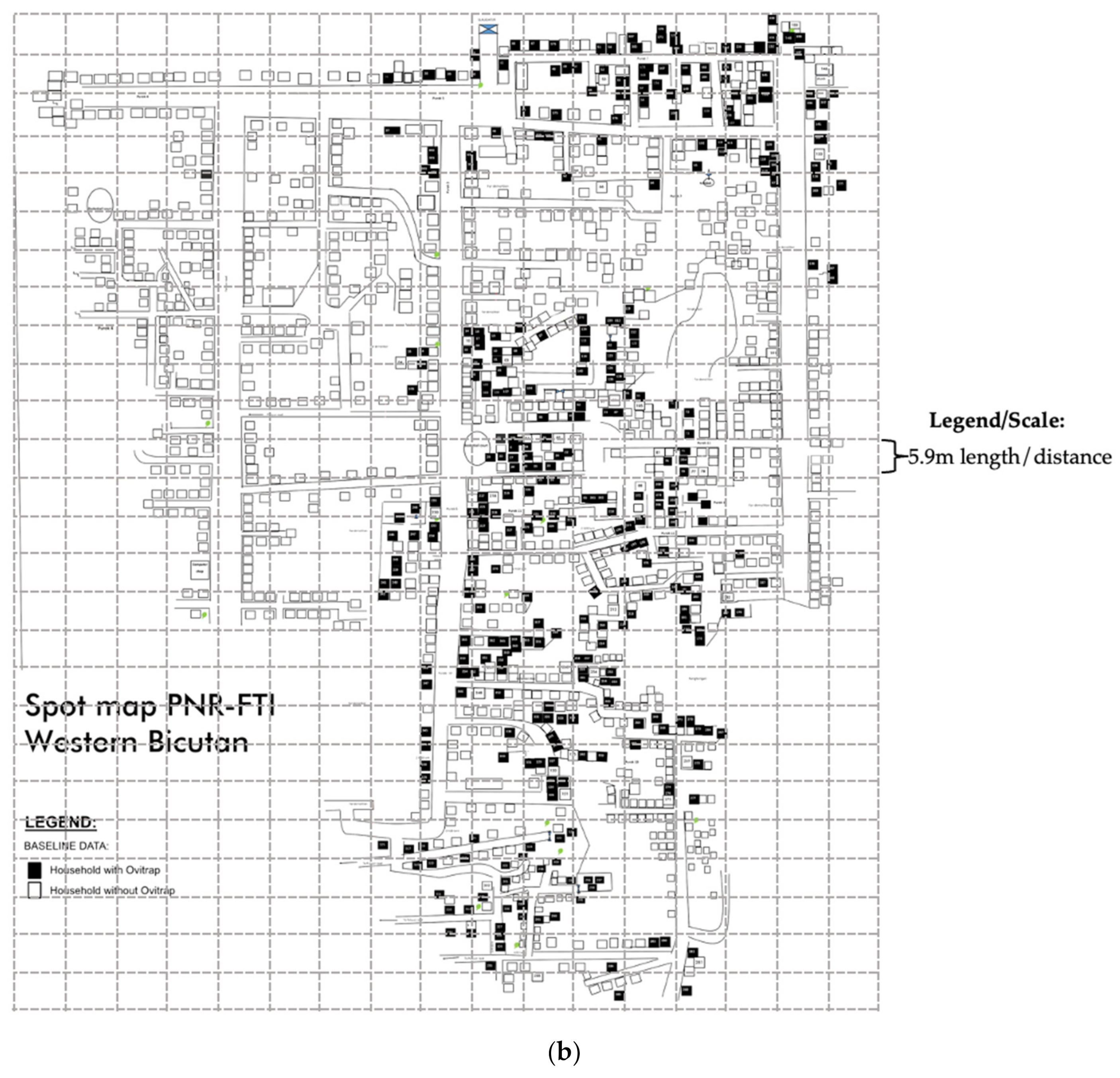
2.1. Study Design, Sites, and Population
2.2. Inclusion and Exclusion Criteria of Participants
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Data Collection
2.3.1. Entomological Indices, Intervention, and Control Ovitap Set-Up
2.3.2. Outcome Assessment: Antibody Measurements
2.4. Data Analysis
2.5. Ethical Considerations
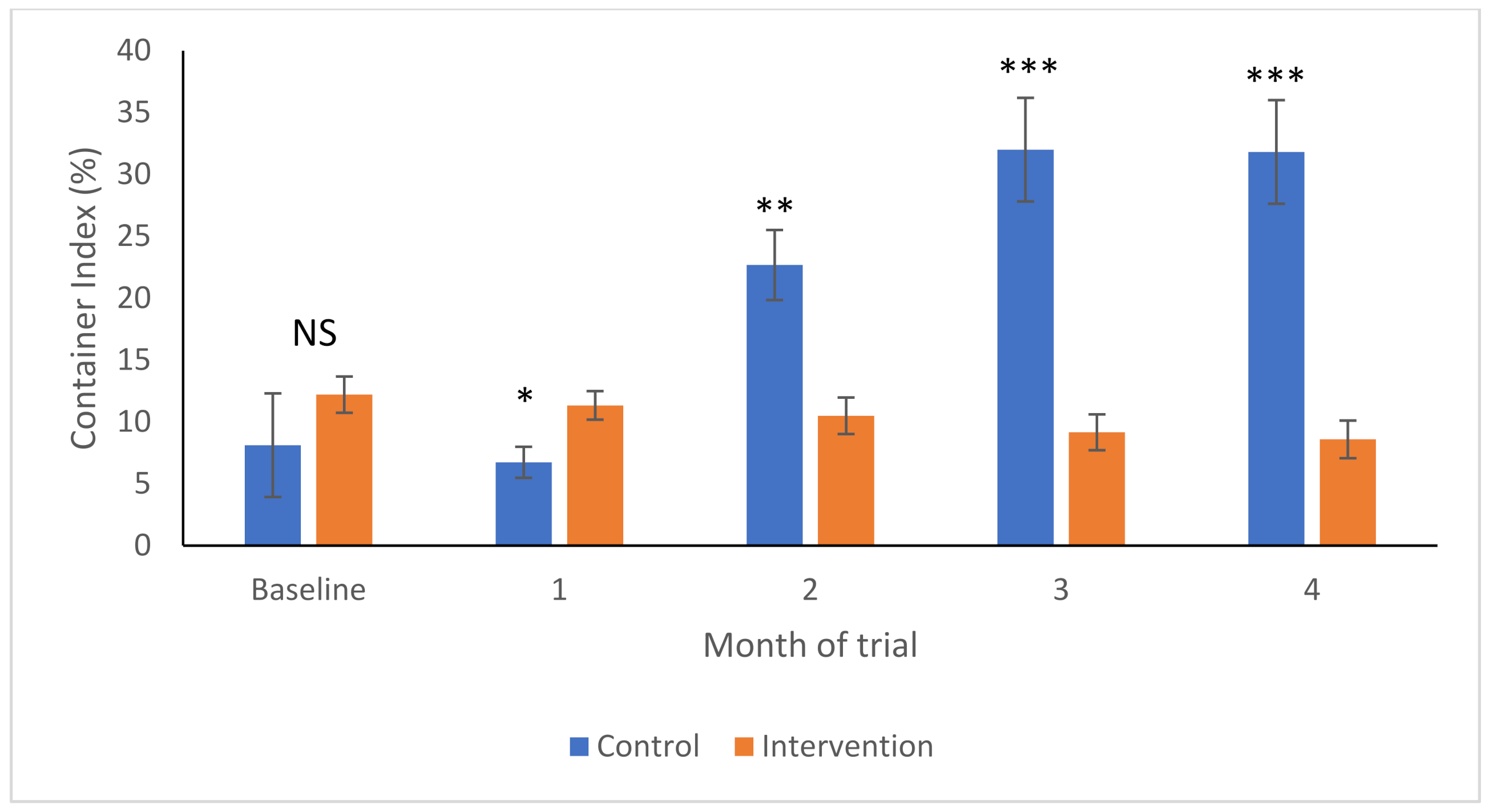
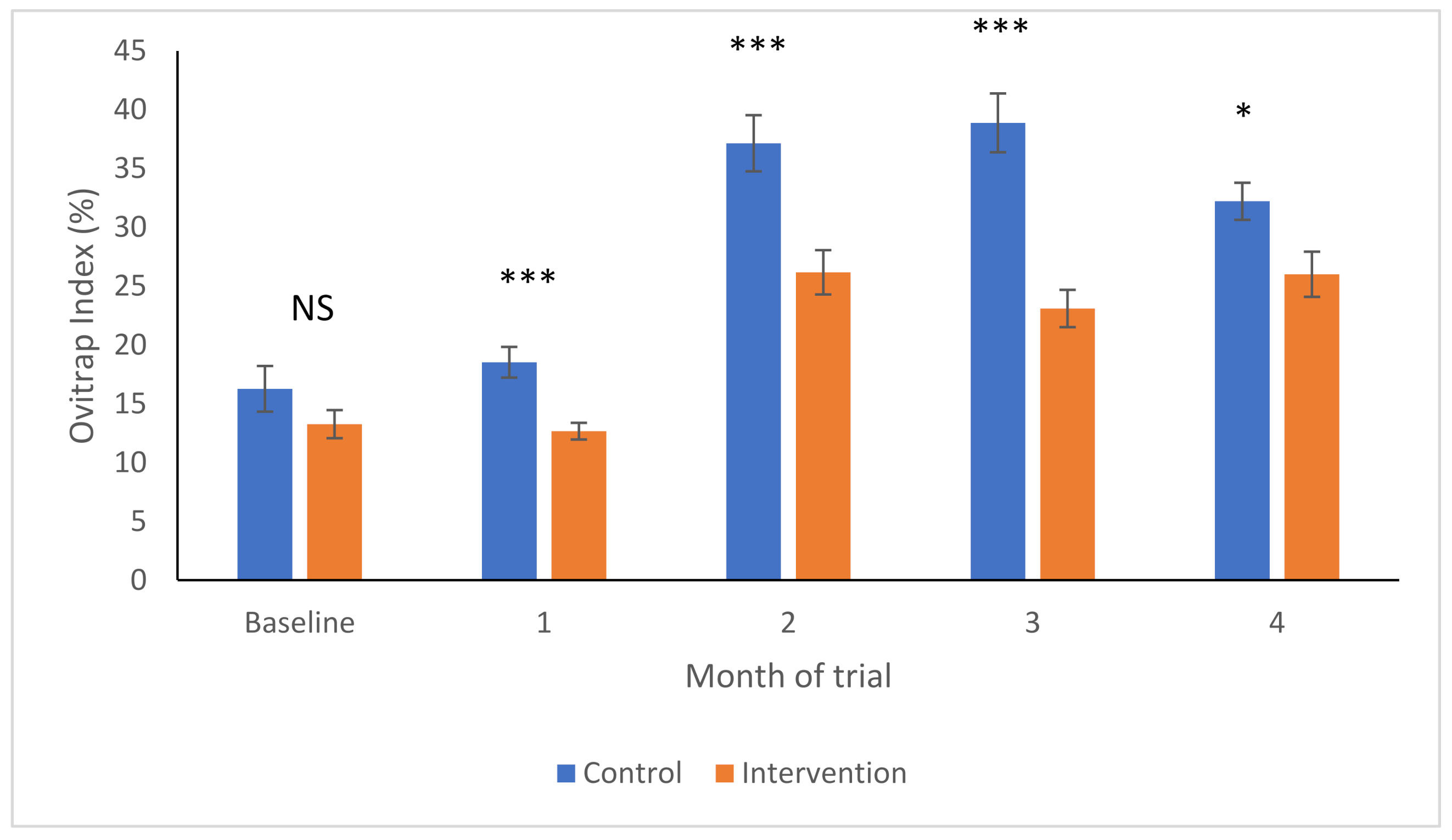
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stanaway, J.D.; Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Coffeng, L.E.; Brady, O.J.; Hay, S.I.; Bedi, N.; Bensenor, I.M.; Castañeda-Orjuela, C.A. The global burden of dengue: An analysis from the Global Burden of Disease Study 2013. Lancet Infect. Dis. 2016, 16, 712–723. [Google Scholar] [CrossRef]
- Chen, L.H.; Wilson, M.E. The role of the traveler in emerging infections and magnitude of travel. Med. Clin. N. Am. 2008, 92, 1409–1432. [Google Scholar] [CrossRef] [PubMed]
- Christophers, S.R. Aëdes aegypti (L.) the Yellow Fever Mosquito: Its Life History, Bionomics and Structure; Cambridge University Press: Cambridge, UK, 1960. [Google Scholar]
- Guzmán, M.G.; Kouri, G. Dengue: An update. Lancet Infect. Dis. 2002, 2, 33–42. [Google Scholar] [CrossRef]
- Gubler, D.J. Epidemic dengue/dengue hemorrhagic fever as a public health, social and economic problem in the 21st century. Trends Microbiol. 2002, 10, 100–103. [Google Scholar] [CrossRef]
- Rezza, G.; Nicoletti, L.; Angelini, R.; Romi, R.; Finarelli, A.; Panning, M.; Cordioli, P.; Fortuna, C.; Boros, S.; Magurano, F. Infection with chikungunya virus in Italy: An outbreak in a temperate region. Lancet 2007, 370, 1840–1846. [Google Scholar] [CrossRef]
- Radke, E.G.; Gregory, C.J.; Kintziger, K.W.; Sauber-Schatz, E.K.; Hunsperger, E.A.; Gallagher, G.R.; Barber, J.M.; Biggerstaff, B.J.; Stanek, D.R.; Tomashek, K.M. Dengue outbreak in key west, Florida, USA, 2009. Emerg. Infect. Dis. 2012, 18, 135. [Google Scholar] [CrossRef]
- Sousa, C.; Clairouin, M.; Seixas, G.; Viveiros, B.; Novo, M.; Silva, A.; Escoval, M.; Economopoulou, A. Ongoing outbreak of dengue type 1 in the Autonomous Region of Madeira, Portugal: Preliminary report. Eurosurveillance 2012, 17, 20333. [Google Scholar] [CrossRef]
- Murray, K.O.; Rodriguez, L.F.; Herrington, E.; Kharat, V.; Vasilakis, N.; Walker, C.; Turner, C.; Khuwaja, S.; Arafat, R.; Weaver, S.C. Identification of dengue fever cases in Houston, Texas, with evidence of autochthonous transmission between 2003 and 2005. Vector-Borne Zoonotic Dis. 2013, 13, 835–845. [Google Scholar] [CrossRef]
- Paul, R.E. The when and the where of Zika epidemic potential in Europe–an evidence base for public health preparedness. EBioMedicine 2016, 9, 17–18. [Google Scholar] [CrossRef][Green Version]
- Giron, S.; Franke, F.; Decoppet, A.; Cadiou, B.; Travaglini, T.; Thirion, L.; Durand, G.; Jeannin, C.; L’ambert, G.; Grard, G. Vector-borne transmission of Zika virus in Europe, southern France, August 2019. Eurosurveillance 2019, 24, 1900655. [Google Scholar] [CrossRef]
- Faulde, M.K.; Rueda, L.M.; Khaireh, B.A. First record of the Asian malaria vector Anopheles stephensi and its possible role in the resurgence of malaria in Djibouti, Horn of Africa. Acta Trop. 2014, 139, 39–43. [Google Scholar] [CrossRef]
- Sinka, M.; Pironon, S.; Massey, N.; Longbottom, J.; Hemingway, J.; Moyes, C.; Willis, K. A new malaria vector in Africa: Predicting the expansion range of Anopheles stephensi and identifying the urban populations at risk. Proc. Natl. Acad. Sci. USA 2020, 117, 24900–24908. [Google Scholar] [CrossRef]
- Ligsay, A.; Telle, O.; Paul, R. Challenges to Mitigating the Urban Health Burden of Mosquito-Borne Diseases in the Face of Climate Change. Int. J. Environ. Res. Public Health 2021, 18, 5035. [Google Scholar] [CrossRef]
- Nash, D.; Mostashari, F.; Fine, A.; Miller, J.; O’leary, D.; Murray, K.; Huang, A.; Rosenberg, A.; Greenberg, A.; Sherman, M. The outbreak of West Nile virus infection in the New York City area in 1999. N. Engl. J. Med. 2001, 344, 1807–1814. [Google Scholar] [CrossRef]
- Huhn, G.D.; Austin, C.; Langkop, C.; Kelly, K.; Lucht, R.; Lampman, R.; Novak, R.; Haramis, L.; Boker, R.; Smith, S. The emergence of West Nile virus during a large outbreak in Illinois in 2002. Am. J. Trop. Med. Hyg. 2005, 72, 768–776. [Google Scholar] [CrossRef]
- Ruiz, M.O.; Walker, E.D.; Foster, E.S.; Haramis, L.D.; Kitron, U.D. Association of West Nile virus illness and urban landscapes in Chicago and Detroit. Int. J. Health Geogr. 2007, 6, 10. [Google Scholar] [CrossRef]
- Murray, N.E.A.; Quam, M.B.; Wilder-Smith, A. Epidemiology of dengue: Past, present and future prospects. Clin. Epidemiol. 2013, 5, 299. [Google Scholar]
- Ebi, K.L.; Nealon, J. Dengue in a changing climate. Environ. Res. 2016, 151, 115–123. [Google Scholar] [CrossRef]
- Bowman, L.R.; Donegan, S.; McCall, P.J. Is dengue vector control deficient in effectiveness or evidence?: Systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2016, 10, e0004551. [Google Scholar] [CrossRef]
- Bartlett-Healy, K.; Hamilton, G.; Healy, S.; Crepeau, T.; Unlu, I.; Farajollahi, A.; Fonseca, D.; Gaugler, R.; Clark, G.G.; Strickman, D. Source reduction behavior as an independent measurement of the impact of a public health education campaign in an integrated vector management program for the Asian tiger mosquito. Int. J. Environ. Res. Public Health 2011, 8, 1358–1367. [Google Scholar] [CrossRef]
- Ocampo, C.B.; Mina, N.J.; Carabalí, M.; Alexander, N.; Osorio, L. Reduction in dengue cases observed during mass control of Aedes (Stegomyia) in street catch basins in an endemic urban area in Colombia. Acta Trop. 2014, 132, 15–22. [Google Scholar] [CrossRef]
- Fouque, F.; Gross, K.; Leung, Z.; Boutsika, K. Introduction to a Landscape Analysis of Multisectoral Approaches for Prevention and Control of Infectious and Vector-Borne Diseases. J. Infect. Dis. 2020, 222, S695–S700. [Google Scholar] [CrossRef]
- Andries, A.-C.; Duong, V.; Ong, S.; Ros, S.; Sakuntabhai, A.; Horwood, P.; Dussart, P.; Buchy, P. Evaluation of the performances of six commercial kits designed for dengue NS1 and anti-dengue IgM, IgG and IgA detection in urine and saliva clinical specimens. BMC Infect. Dis. 2016, 16, 201. [Google Scholar] [CrossRef]
- WHO. Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Andries, A.-C.; Duong, V.; Ly, S.; Cappelle, J.; Kim, K.S.; Lorn Try, P.; Ros, S.; Ong, S.; Huy, R.; Horwood, P. Value of routine dengue diagnostic tests in urine and saliva specimens. PLoS Negl. Trop. Dis. 2015, 9, e0004100. [Google Scholar] [CrossRef]
- Loomis, D.; Richardson, D.B.; Elliott, L. Poisson regression analysis of ungrouped data. Occup. Environ. Med. 2005, 62, 325–329. [Google Scholar] [CrossRef]
- Itoh, T.; Kawada, H.; Abe, A.; Eshita, Y.; Rongsriyam, Y.; Igarashi, A. Utilization of bloodfed females of Aedes aegypti as a vehicle for the transfer of the insect growth regulator pyriproxyfen to larval habitats. J. Am. Mosq. Control. Assoc. Mosq. News 1994, 10, 344–347. [Google Scholar]
- Devine, G.J.; Overgaard, H.J.; Paul, R.E. Global vector control guidelines—The need for co-creation. Trends Parasitol. 2019, 35, 267–270. [Google Scholar] [CrossRef]
- Abad-Franch, F.; Zamora-Perea, E.; Luz, S.L. Mosquito-disseminated insecticide for citywide vector control and its potential to block arbovirus epidemics: Entomological observations and modeling results from Amazonian Brazil. PLoS Med. 2017, 14, e1002213. [Google Scholar] [CrossRef]
- Ohba, S.-y.; Ohashi, K.; Pujiyati, E.; Higa, Y.; Kawada, H.; Mito, N.; Takagi, M. The effect of pyriproxyfen as a “population growth regulator” against Aedes albopictus under semi-field conditions. PLoS ONE 2013, 8, e67045. [Google Scholar] [CrossRef]
- Unlu, I.; Suman, D.S.; Wang, Y.; Klingler, K.; Faraji, A.; Gaugler, R. Effectiveness of autodissemination stations containing pyriproxyfen in reducing immature populations Aedes albopictus. Parasites Vectors 2017, 10, 139. [Google Scholar] [CrossRef]
- Seixas, G.; Paul, R.E.; Pires, B.; Alves, G.; de Jesus, A.; Silva, A.-C.; Devine, G.J.; Sousa, C.A. An evaluation of efficacy of the auto-dissemination technique as a tool for Aedes aegypti control in Madeira, Portugal. Parasites Vectors 2019, 12, 202. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, S.A.; Paton, C.; Buhagiar, T.; Webb, G.A.; Jovic, V. Residual treatment of Aedes aegypti (Diptera: Culicidae) in containers using pyriproxyfen slow-release granules (Sumilarv 0.5 G). J. Med. Entomol. 2013, 50, 1169–1172. [Google Scholar] [CrossRef] [PubMed]
- Sihuincha, M.; Zamora-Perea, E.; Orellana-Rios, W.; Stancil, J.D.; López-Sifuentes, V.; Vidal-Ore, C.; Devine, G.J. Potential use of pyriproxyfen for control of Aedes aegypti (Diptera: Culicidae) in Iquitos, Peru. J. Med. Entomol. 2005, 42, 620–630. [Google Scholar] [CrossRef] [PubMed]
- WHO. Efficacy-Testing of Traps for Control of Aedes spp. Mosquito Vectors; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Wang, W.-H.; Urbina, A.N.; Chang, M.R.; Assavalapsakul, W.; Lu, P.-L.; Chen, Y.-H.; Wang, S.-F. Dengue hemorrhagic fever—A systemic literature review of current perspectives on pathogenesis, prevention and control. J. Microbiol. Immunol. Infect. 2020, 53, 963–978. [Google Scholar] [CrossRef]
- Devine, G. Auto-Dissemination of Pyriproxyfen for the Control of Container-inhabiting Mosquitoes—A Progress Review. Outlooks Pest Manag. 2016, 27, 164–167. [Google Scholar] [CrossRef]
- Cuzzubbo, A.J.; Vaughn, D.W.; Nisalak, A.; Suntayakorn, S.; Aaskov, J.; Devine, P.L. Detection of specific antibodies in saliva during dengue infection. J. Clin. Microbiol. 1998, 36, 3737–3739. [Google Scholar] [CrossRef]
- De Las Llagas, L.A.; Bersales, L.G.S.; Bertuso, A.G.; Mistica, M.S.; Ocampo, V.R.; Samaniego, J.B.; Magsino, E.A.; Alzona, F.D. Mosquito Larvicidal Trap (MLT) as surveillance and control tool for Aedes mosquitoes. Southeast Asian J. Trop. Med. Public Health 2016, 47, 701. [Google Scholar]
- Rockstroh, A.; Moges, B.; Barzon, L.; Sinigaglia, A.; Palù, G.; Kumbukgolla, W.; Schmidt-Chanasit, J.; Sarno, M.; Brites, C.; Moreira-Soto, A. Specific detection of dengue and Zika virus antibodies using envelope proteins with mutations in the conserved fusion loop. Emerg. Microbes Microbes Microbes Infect. 2017, 6, e99. [Google Scholar] [CrossRef]
- Da Silva, M.V.; Camargo, E.D.; Vaz, A.J.; Batista, L. Immunodiagnosis of human leptospirosis using saliva. Trans. R. Soc. Trop. Med. Hyg. 1992, 86, 560–561. [Google Scholar] [CrossRef]
- Frerichs, R. Saliva assays for HIV antibody diagnosis. Labmed. Int. 1994, 5, 16–19. [Google Scholar]
- Friedman, M.G.; Phillip, M.; Dagan, R. Virus-specific IgA in serum, saliva, and tears of children with measles. Clin. Exp. Immunol. 1989, 75, 58. [Google Scholar]
- WHO. Guidelines for diagnosis, Treatment. In Prevention and Control; WHO: Geneva, Switzerland, 2009; Volume 1. [Google Scholar]
- Wang, Y.; Suman, D.S.; Bertrand, J.; Dong, L.; Gaugler, R. Dual-treatment autodissemination station with enhanced transfer of an insect growth regulator to mosquito oviposition sites. Pest Manag. Sci. 2014, 70, 1299–1304. [Google Scholar] [CrossRef]
- Iwanaga, K.; Kanda, T. The effects of a juvenile hormone active oxime ether compound on the metamorphosis and reproduction of an anopheline vector, Anopheles balabacensis (Diptera: Culicidae). Appl. Entomol. Zool. 1988, 23, 186–193. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Intervention Group | Control Group | Total | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Age, years old | ||||||
| Child, 1–12 | 99 | 45 | 73 | 32.8 | 172 | 38.83 |
| Adolescent, 13–18 | 60 | 27.3 | 38 | 17 | 98 | 22.12 |
| Young adult, 19–30 | 61 | 27.7 | 112 | 50.2 | 173 | 39.05 |
| Sex | ||||||
| Male | 103 | 46.8 | 103 | 46.2 | 206 | 46.50 |
| Female | 117 | 53.2 | 120 | 53.8 | 237 | 53.50 |
| Income, PhP | ||||||
| No income | 3 | 1.4 | 19 | 8.5 | 22 | 4.97 |
| 1 to <10,000 | 41 | 18.6 | 48 | 21.5 | 89 | 20.09 |
| 10,001 to <20,000 | 161 | 73.2 | 123 | 55.2 | 284 | 64.11 |
| 20,001 to <30,000 | 14 | 6.4 | 24 | 10.8 | 38 | 8.58 |
| 30,001 and above | 1 | 0.4 | 9 | 4 | 10 | 2.26 |
| Mother’s Education | ||||||
| At least High School | 199 | 90.5 | 168 | 75.3 | 367 | 82.84 |
| College/Postgraduate | 20 | 9.1 | 51 | 22.9 | 71 | 16.03 |
| Deceased/No Data | 1 | 0.4 | 4 | 1.8 | 5 | 1.13 |
| Father’s Education | ||||||
| At Least High School | 183 | 83.2 | 164 | 73.5 | 347 | 78.33 |
| College/Postgraduate | 26 | 11.8 | 57 | 25.6 | 83 | 18.74 |
| Deceased/No Data | 11 | 5 | 2 | 0.9 | 13 | 2.93 |
| Average IgG, g/L | 220 | 0.046 ± 0.036 | 223 | 0.044 ± 0.033 | ||
| Groups | Number of Dengue Seropositive Individuals | |||
|---|---|---|---|---|
| Baseline | Month 2 | Month 3 | Month 4 | |
| Intervention (n = 220) | Intervention (n = 203) | Intervention (n = 181) | Intervention (n = 173) | |
| Control (n = 223) | Control (n = 210) | Control (n = 208) | Control (n = 202) | |
| Intervention | 17 | 22 | 8 | 3 |
| Control | 13 | 2 | 6 | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ligsay, A.D.; Tambio, K.J.M.; Aytona, M.J.M.; Alejandro, G.J.D.; Regencia, Z.J.G.; Baja, E.S.; Paul, R.E.L. Assessing Entomological and Epidemiological Efficacy of Pyriproxyfen-Treated Ovitraps in the Reduction of Aedes Species: A Quasi-Experiment on Dengue Infection Using Saliva Samples. Int. J. Environ. Res. Public Health 2022, 19, 3026. https://doi.org/10.3390/ijerph19053026
Ligsay AD, Tambio KJM, Aytona MJM, Alejandro GJD, Regencia ZJG, Baja ES, Paul REL. Assessing Entomological and Epidemiological Efficacy of Pyriproxyfen-Treated Ovitraps in the Reduction of Aedes Species: A Quasi-Experiment on Dengue Infection Using Saliva Samples. International Journal of Environmental Research and Public Health. 2022; 19(5):3026. https://doi.org/10.3390/ijerph19053026
Chicago/Turabian StyleLigsay, Antonio D., Kristan Jela M. Tambio, Michelle Joyce M. Aytona, Grecebio Jonathan D. Alejandro, Zypher Jude G. Regencia, Emmanuel S. Baja, and Richard Edward L. Paul. 2022. "Assessing Entomological and Epidemiological Efficacy of Pyriproxyfen-Treated Ovitraps in the Reduction of Aedes Species: A Quasi-Experiment on Dengue Infection Using Saliva Samples" International Journal of Environmental Research and Public Health 19, no. 5: 3026. https://doi.org/10.3390/ijerph19053026
APA StyleLigsay, A. D., Tambio, K. J. M., Aytona, M. J. M., Alejandro, G. J. D., Regencia, Z. J. G., Baja, E. S., & Paul, R. E. L. (2022). Assessing Entomological and Epidemiological Efficacy of Pyriproxyfen-Treated Ovitraps in the Reduction of Aedes Species: A Quasi-Experiment on Dengue Infection Using Saliva Samples. International Journal of Environmental Research and Public Health, 19(5), 3026. https://doi.org/10.3390/ijerph19053026