
Prevalence Estimates and Risk Factors of Anxiety among Healthcare Workers in Jordan over One Year of the COVID-19 Pandemic: A Cross-Sectional Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Population, and Ethical Approval
2.2. Survey Instruments
2.3. Statistical Analysis
3. Results
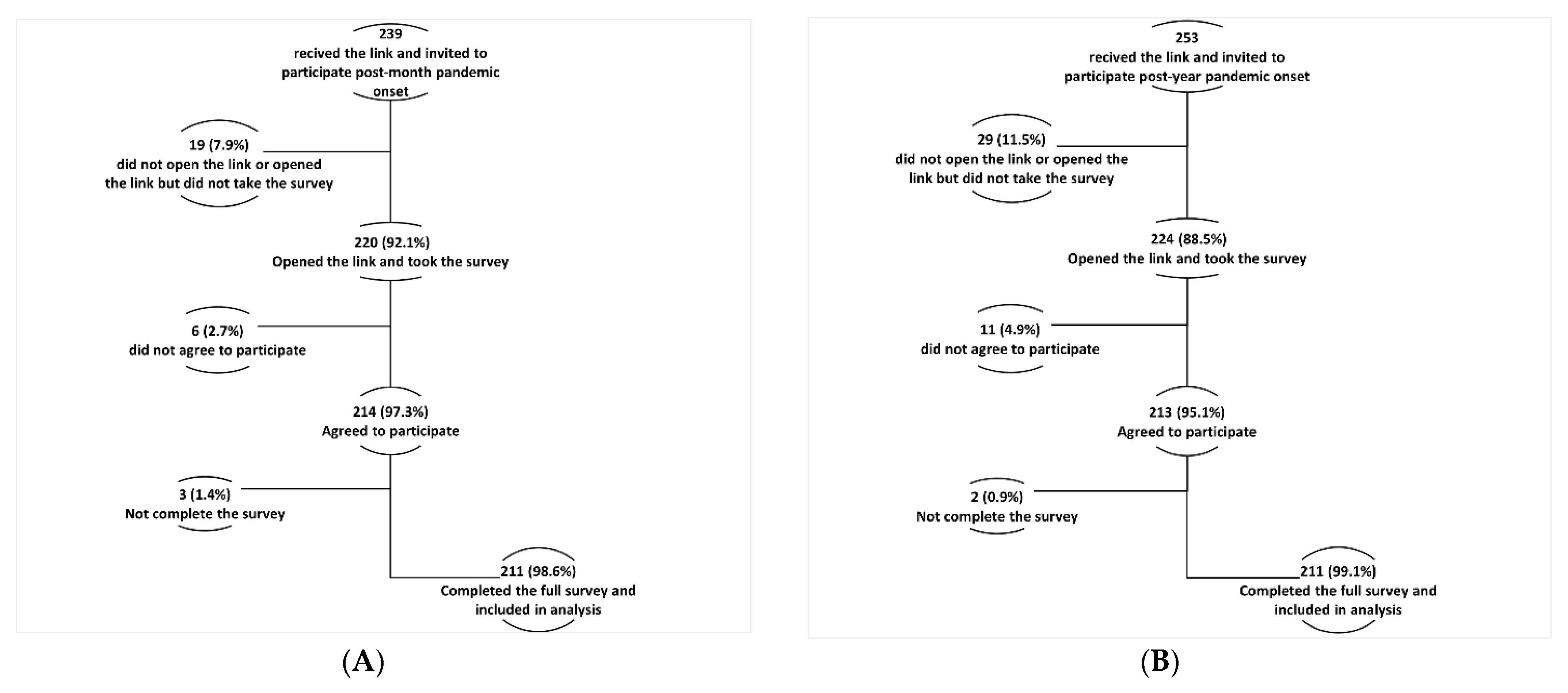
3.1. Participation Rate
3.2. Total Cohort’s Socio-Demographic Characteristics
3.3. The Onset and One-Year Samples’ Characteristics
3.4. Trends of Anxiety Symptoms among HCWs over a Year of COVID-19 Pandemic
3.5. Factors Associated with Anxiety Symptoms in the Onset Group
3.6. Factors Associated with Anxiety Symptoms in the One-Year Group
3.7. Risk Factors for Generalized Anxiety Disorder (GAD) among HCWs
4. Discussion
4.1. Anxiety among HCWs
4.2. Anxiety Risk Factors
4.2.1. Shared Risk Factors between the Onset and One-Year Groups
4.2.2. Risk Factors at Onset of the Pandemic
4.2.3. Risk Factors after One Year of the Pandemic
4.2.4. Strengths and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- JHU. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). 2021. Available online: https://github.com/CSSEGISandData/COVID-19 (accessed on 5 January 2022).
- Chriscaden, K. Impact of COVID-19 on People’s Livelihoods, Their Health and Our Food Systems; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/news/item/13-10-2020-impact-of-covid-19-on-people’s-livelihoods-their-health-and-our-food-systems (accessed on 5 December 2021).
- Allain-Dupré, D.; Chatry, I.; Kornprobst, A. The Territorial Impact of COVID-19: Managing the Crisis across Levels of Government. Available online: https://www.oecd.org/coronavirus/policy-responses/the-territorial-impact-of-covid-19-managing-the-crisis-across-levels-of-government-d3e314e1/ (accessed on 5 December 2021).
- Andersen, A.J.; Mary-Krause, M.; Bustamante, J.J.H.; Héron, M.; Aarbaoui, T.E.; Melchior, M. Symptoms of anxiety/depression during the COVID-19 pandemic and associated lockdown in the community: Longitudinal data from the TEMPO cohort in France. BMC Psychiatry 2021, 21, 1–9. [Google Scholar]
- Cohut, M. Global impact of the COVID-19 pandemic: 1 year on. Medicine News Today. 12 March 2021. Available online: https://www.medicalnewstoday.com/articles/global-impact-of-the-covid-19-pandemic-1-year-on (accessed on 5 December 2021).
- Yassin, A.; AlOmari, M.; Al-Azzam, S.; Karasneh, R.; Abu-Ismail, L.; Soudah, O. Impact of Social Media on Public Fear, Adoption of Precautionary Behaviors, and Compliance with Health Regulations during COVID-19 Pandemic. Int. J. Environ. Health Res. 2021, 31, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Yassin, A.; Nawaiseh, M.; Shaban, A.; Alsherbini, K.; El-Salem, K.; Soudah, O.; Abu-Rub, M. Neurological manifestations and complications of coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. BMC Neurol. 2021, 21, 1–17. [Google Scholar]
- Samrah, S.M.; Al-Mistarehi, A.-H.W.; Ibnian, A.M.; Raffee, L.A.; Momany, S.M.; Al-Ali, M.; Hayajneh, W.A.; Yusef, D.H.; Awad, S.M.; Khassawneh, B.Y. COVID-19 outbreak in Jordan: Epidemiological features, clinical characteristics, and laboratory findings. Ann. Med. Surg. 2020, 57, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Samrah, S.M.; Al-Mistarehi, A.-H.; Kewan, T.; Al-Khatib, S.M.; Ibnian, A.M.; Samrah, R.S.; Khassawneh, B.Y. Viral Clearance Course of COVID-19 Outbreaks. J. Multidiscip. Healthc. 2021, 14, 555–565. Available online: https://pubmed.ncbi.nlm.nih.gov/33707949/ (accessed on 5 December 2021). [CrossRef]
- Yassin, A.; Ghzawi, A.; Al-Mistarehi, A.-H.; El-Salem, K.; Benmelouka, A.Y.; Sherif, A.M.; BenhadjDahman, N.; AlAdamat, N.; Jemel, A.; Negida, A.; et al. Mortality rate and biomarker expression within COVID-19 patients who develop acute ischemic stroke: A systematic review and meta-analysis. Future Sci. OA 2021, 7, FSO713. Available online: https://pubmed.ncbi.nlm.nih.gov/34254031/ (accessed on 5 December 2021). [CrossRef]
- Hasabo, E.A.; Ayyad, F.A.; Alam Eldeen, S.A.M.; Noureldaim, M.K.; Abdallah, T.A.; Ahmed, Y.T.; Badi, S.; Khalid, W.K.; Mirghani, H.A.; Mohammed, Y.A.; et al. Clinical manifestations, complications, and outcomes of patients with COVID-19 in Sudan: A multicenter observational study. Trop. Med. Health 2021, 49, 1–13. Available online: https://tropmedhealth.biomedcentral.com/articles/10.1186/s41182-021-00382-4 (accessed on 5 December 2021). [CrossRef]
- Samrah, S.M.; Al-Mistarehi, A.-H.; Aleshawi, A.J.; Khasawneh, A.G.; Momany, S.M.; Momany, B.S.; Abu Za’Nouneh, F.J.; Keelani, T.; Alshorman, A.; Khassawneh, B.Y. Depression and coping among COVID-19-infected individuals after 10 days of mandatory in-hospital quarantine, irbid, jordan. Psychol. Res. Behav. Manag. 2020, 13, 823–830. [Google Scholar] [CrossRef]
- Rondung, E.; Leiler, A.; Meurling, J.; Bjärtå, A. Symptoms of Depression and Anxiety During the Early Phase of the COVID-19 Pandemic in Sweden. Front. Public Health 2021, 9, 562437. [Google Scholar] [CrossRef]
- Al-Shatanawi, T.N.; Sakka, S.A.; Kheirallah, K.A.; Al-Mistarehi, A.-H.; Al-Tamimi, S.; Alrabadi, N.; Alsulaiman, J.; Al Khader, A.; Abdallah, F.; Tawalbeh, L.I.; et al. Self-Reported Obsession Toward COVID-19 Preventive Measures Among Undergraduate Medical Students During the Early Phase of Pandemic in Jordan. Front. Public Health 2021, 9, 719668. Available online: https://pubmed.ncbi.nlm.nih.gov/34820347/ (accessed on 7 December 2021). [CrossRef]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Coping With COVID-19: Emergency Stress, Secondary Trauma and Self-Efficacy in Healthcare and Emergency Workers in Italy. Front. Psychol. 2020, 11. Available online: https://pubmed.ncbi.nlm.nih.gov/33013603/ (accessed on 7 December 2021). [CrossRef] [PubMed]
- Vagni, M.; Maiorano, T.; Giostra, V.; Pajardi, D. Protective Factors against Emergency Stress and Burnout in Healthcare and Emergency Workers during Second Wave of COVID-19. Soc. Sci. 2021, 10, 178. Available online: https://www.mdpi.com/2076-0760/10/5/178/htm (accessed on 7 December 2021). [CrossRef]
- Bohlken, J.; Schömig, F.; Lemke, M.R.; Pumberger, M.; Riedel-Heller, S.G. [COVID-19 Pandemic: Stress Experience of Healthcare Workers-A Short Current Review]. Psychiatr. Prax. 2020, 47, 190–197. Available online: https://pubmed.ncbi.nlm.nih.gov/32340048/ (accessed on 7 December 2021).
- Simione, L.; Gnagnarella, C. Differences Between Health Workers and General Population in Risk Perception, Behaviors, and Psychological Distress Related to COVID-19 Spread in Italy. Front. Psychol. 2020, 11, 2166. Available online: https://pubmed.ncbi.nlm.nih.gov/33013555/ (accessed on 7 December 2021). [CrossRef] [PubMed]
- Menzies, R.E.; Menzies, R.G. Death anxiety in the time of COVID-19: Theoretical explanations and clinical implications. Cogn. Behav. Ther. 2020, 13, e19. Available online: https://pubmed.ncbi.nlm.nih.gov/34191938/ (accessed on 12 December 2021). [CrossRef]
- Fernandez, R.; Sikhosana, N.; Green, H.; Halcomb, E.J.; Middleton, R.; Alananzeh, I.; Trakis, S.; Moxham, L. Anxiety and depression among healthcare workers during the COVID-19 pandemic: A systematic umbrella review of the global evidence. BMJ Open 2021, 11, e054528. Available online: https://bmjopen.bmj.com/content/11/9/e054528 (accessed on 12 December 2021). [CrossRef]
- Sahebi, A.; Nejati-Zarnaqi, B.; Moayedi, S.; Yousefi, K.; Torres, M.; Golitaleb, M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: An umbrella review of meta-analyses. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 107, 110247. Available online: https://pubmed.ncbi.nlm.nih.gov/33476692/ (accessed on 12 December 2021). [CrossRef]
- Khubchandani, J.; Sharma, S.; Webb, F.J.; Wiblishauser, M.J.; Bowman, S.L. Post-lockdown depression and anxiety in the USA during the COVID-19 pandemic. J. Public Health 2021, 43, 246–253. [Google Scholar] [CrossRef]
- Jin, Y.-H.; Huang, Q.; Wang, Y.-Y.; Zeng, X.-T.; Luo, L.-S.; Pan, Z.-Y.; Yuan, Y.-F.; Chen, Z.-M.; Cheng, Z.-S.; Huang, X.; et al. Perceived infection transmission routes, infection control practices, psychosocial changes, and management of COVID-19 infected healthcare workers in a tertiary acute care hospital in Wuhan: A cross-sectional survey. Mil. Med. Res. 2020, 7, 1–13. Available online: https://pubmed.ncbi.nlm.nih.gov/32393381/ (accessed on 12 December 2021). [CrossRef]
- Ramadan, M.; Hasan, Z.; Saleh, T.; Jaradat, M.; Al-Hazaimeh, M.; Hani, O.B.; Al-Tammemi, A.B.; Shorman, E.; Al-Mistarehi, A.; Kheirallah, K. Beyond knowledge: Evaluating the practices and precautionary measures towards COVID-19 amongst medical doctors in Jordan. Int. J. Clin. Pract. 2021, 75, e14122. Available online: https://pubmed.ncbi.nlm.nih.gov/33650228/ (accessed on 12 December 2021). [CrossRef]
- Terry, D.L.; Hui, P.; Buntoro, S. The Initial Positive and Negative Impacts of the COVID-19 Pandemic on Rural Healthcare Providers: Associations With Team Culture and Leadership. J. Healthc. Manag. 2021, 66, 396–406. Available online: https://pubmed.ncbi.nlm.nih.gov/34495004/ (accessed on 17 December 2021). [CrossRef] [PubMed]
- De Kock, J.H.; Latham, H.A.; Leslie, S.J.; Grindle, M.; Munoz, S.-A.; Ellis, L.; Polson, R.; O’Malley, C.M. A rapid review of the impact of COVID-19 on the mental health of healthcare workers: Implications for supporting psychological well-being. BMC Public Health 2021, 21, 1–18. Available online: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-10070-3 (accessed on 17 December 2021). [CrossRef] [PubMed]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. Available online: https://pubmed.ncbi.nlm.nih.gov/32276196/ (accessed on 17 December 2021). [CrossRef] [PubMed]
- Liu, C.-Y.; Yang, Y.-Z.; Zhang, X.-M.; Xu, X.; Dou, Q.-L.; Zhang, W.-W.; Cheng, A.S.K. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: A cross-sectional survey. Epidemiol. Infect. 2020, 148, 1–17. Available online: https://pubmed.ncbi.nlm.nih.gov/32430088/ (accessed on 17 December 2021). [CrossRef] [PubMed]
- Liang, Y.; Wu, K.; Zhou, Y.; Huang, X.; Zhou, Y.; Liu, Z. Mental health in frontline medical workers during the 2019 novel coronavirus disease epidemic in China: A comparison with the general population. Int. J. Environ. Res. Public Health 2020, 17, 6550. [Google Scholar] [CrossRef]
- Shreffler, J.; Petrey, J.; Huecker, M. The Impact of COVID-19 on Healthcare Worker Wellness: A Scoping Review. West. J. Emerg. Med. 2020, 21, 1059. [Google Scholar] [CrossRef]
- Kheirallah, K.; Bloukh, S.; Khasawneh, W.; Alsulaiman, J.; Khassawneh, A.; Al-Mistarehi, A.-H.; Alqudah, M.; Elsalem, L.; Bashir, S.A.; Awad, H.H.; et al. Medical students’ relative immunity, or lack thereof, against COVID-19 emotional distress and psychological challenges; a descriptive study from Jordan. F1000Research 2021, 10, 297. Available online: https://pubmed.ncbi.nlm.nih.gov/34026047/ (accessed on 17 December 2021). [CrossRef]
- Khassawneh, A.H.; Alrabadi, N.; Al-Mistarehi, A.-H.; Obeidat, N.; Kheirallah, K.A. The role of non-state actors in combating COVID-19 spread in Northern Jordan. Ann. Med. Surg. 2020, 60, 484–486. Available online: https://pubmed.ncbi.nlm.nih.gov/33194175/ (accessed on 20 December 2021). [CrossRef]
- World Health Organization (WHO). Overview of Coronavirus Disease (COVID-19) by Date; World Health Organization: Amman, Jordan, 2021; Available online: https://www.who.int/countries/jor/ (accessed on 20 December 2021).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. Available online: http://www.thelancet.com/article/S1473309920301201/fulltext (accessed on 2 January 2022). [CrossRef]
- Al-Mistarehi, A.-H.; Kheirallah, K.A.; Yassin, A.; Alomari, S.; Aledrisi, M.K.; Ata, E.M.B.; Hammad, N.H.; Khanfar, A.N.; Ibnian, A.M.; Khassawneh, B.Y. Determinants of the willingness of the general population to get vaccinated against COVID-19 in a developing country. Clin. Exp. Vaccine Res. 2021, 10, 171–182. Available online: https://pubmed.ncbi.nlm.nih.gov/34222130/ (accessed on 20 December 2021). [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. Available online: https://pubmed.ncbi.nlm.nih.gov/16717171/ (accessed on 23 December 2021). [CrossRef] [Green Version]
- Swinson, R.P. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evid. Based Med. 2006, 11, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kertz, S.; Bigda-Peyton, J.; Bjorgvinsson, T. Validity of the generalized anxiety disorder-7 scale in an acute psychiatric sample. Clin. Psychol. Psychother. 2013, 20, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Beard, C.; Björgvinsson, T. Beyond generalized anxiety disorder: Psychometric properties of the GAD-7 in a heterogeneous psychiatric sample. J. Anxiety Disord. 2014, 28, 547–552. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.U.; Ulvenes, P.G.; Øktedalen, T.; Hoffart, A. Psychometric Properties of the General Anxiety Disorder 7-Item (GAD-7) Scale in a Heterogeneous Psychiatric Sample. Front. Psychol. 2019, 10, 1713. Available online: https://pubmed.ncbi.nlm.nih.gov/31447721/ (accessed on 23 December 2021). [CrossRef] [Green Version]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Lasalvia, A.; Bonetto, C.; Porru, S.; Carta, A.; Tardivo, S.; Bovo, C.; Ruggeri, M.; Amaddeo, F. Psychological impact of COVID-19 pandemic on healthcare workers in a highly burdened area of north-east Italy. Epidemiol. Psychiatr. Sci. 2020, 30, 1–28. [Google Scholar] [CrossRef]
- Ofori, A.A.; Osarfo, J.; Agbeno, E.K.; Manu, D.O.; Amoah, E. Psychological impact of COVID-19 on health workers in Ghana: A multicentre, cross-sectional study. SAGE Open Med. 2021, 9, 205031212110009. [Google Scholar] [CrossRef]
- Liu, C.H.; Zhang, E.; Wong, G.T.F.; Hyun, S.; Hahm, H.C. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Res. 2020, 290, 113172. [Google Scholar] [CrossRef]
- Benke, C.; Autenrieth, L.K.; Asselmann, E.; Pané-Farré, C.A. Lockdown, quarantine measures, and social distancing: Associations with depression, anxiety and distress at the beginning of the COVID-19 pandemic among adults from Germany. Psychiatry Res. 2020, 293, 113462. [Google Scholar] [CrossRef]
- Asnakew, S.; Amha, H.; Kassew, T. Mental Health Adverse Effects of COVID-19 Pandemic on Health Care Workers in North West Ethiopia: A Multicenter Cross-Sectional Study. Neuropsychiatr. Dis. Treat. 2021, 17, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Tu, B.; Ma, J.; Chen, L.; Fu, L.; Jiang, Y.; Zhuang, Q. Psychological Impact and Coping Strategies of Frontline Medical Staff in Hunan Between January and March 2020 During the Outbreak of Coronavirus Disease 2019 (COVID-19) in Hubei, China. Med. Sci. Monit. 2020, 26, e924171. Available online: https://pubmed.ncbi.nlm.nih.gov/32291383/ (accessed on 25 December 2021). [PubMed] [Green Version]
- Özdin, S.; Özdin, Ş.B. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: The importance of gender. Int. J. Soc. Psychiatry 2020, 66, 504–511. Available online: https://pubmed.ncbi.nlm.nih.gov/32380879/ (accessed on 25 December 2021). [CrossRef] [PubMed]
- Altemus, M.; Sarvaiya, N.; Epperson, C.N. Sex differences in anxiety and depression clinical perspectives. Front. Neuroendocrinol. 2014, 35, 320–330. Available online: https://pubmed.ncbi.nlm.nih.gov/24887405/ (accessed on 25 December 2021). [CrossRef] [Green Version]
- Bartels, M.; Cacioppo, J.T.; Van Beijsterveldt, T.C.E.M.; Boomsma, D.I. Exploring the association between well-being and psychopathology in adolescents. Behav. Genet. 2013, 43, 177–190. Available online: https://pubmed.ncbi.nlm.nih.gov/23471543/ (accessed on 29 December 2021). [CrossRef] [Green Version]
- Ramos, G. OECD Policy Responses to Coronavirus (COVID-19). In Women at the Core of the Fight Against COVID-19 Crisis; OECD: Paris, France, 2020; Available online: https://www.oecd.org/coronavirus/policy-responses/women-at-the-core-of-the-fight-against-covid-19-crisis-553a8269/ (accessed on 29 December 2021).
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Szcześniak, D.; Gładka, A.; Misiak, B.; Cyran, A.; Rymaszewska, J. The SARS-CoV-2 and mental health: From biological mechanisms to social consequences. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 104, 110046. [Google Scholar] [CrossRef]
- Correa-Palacio, A.F.; Hernandez-Huerta, D.; Gómez-Arnau, J.; Loeck, C.; Caballero, I. Affective psychosis after COVID-19 infection in a previously healthy patient: A case report. Psychiatry Res. 2020, 290, 113115. Available online: https://pubmed.ncbi.nlm.nih.gov/32512352/ (accessed on 12 December 2021). [CrossRef]
- Heneka, M.T.; Golenbock, D.; Latz, E.; Morgan, D.; Brown, R. Immediate and long-term consequences of COVID-19 infections for the development of neurological disease. Alzheimers Res. Ther. 2020, 12, 1–3. Available online: https://pubmed.ncbi.nlm.nih.gov/32498691/ (accessed on 27 December 2021). [CrossRef]
- Clark, I.A.; Vissel, B. The meteorology of cytokine storms, and the clinical usefulness of this knowledge. Semin. Immunopathol. 2017, 39, 505–516. Available online: https://pubmed.ncbi.nlm.nih.gov/28451786/ (accessed on 23 December 2021). [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. Available online: https://pubmed.ncbi.nlm.nih.gov/31986264/ (accessed on 2 January 2022). [CrossRef] [Green Version]
- Conti, P.; Ronconi, G.; Caraffa, A.; Gallenga, C.; Ross, R.; Frydas, I.; Kritas, S. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by Coronavirus-19 (COVI-19 or SARS-CoV-2): Anti-inflammatory strategies. J. Biol. Regul. Homeost. Agents 2020, 34, 327–331. Available online: https://pubmed.ncbi.nlm.nih.gov/32171193/ (accessed on 2 January 2022). [PubMed]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. Available online: https://pubmed.ncbi.nlm.nih.gov/32125452/ (accessed on 2 January 2022). [CrossRef] [PubMed] [Green Version]
- Perez-Arce, F.; Angrisani, M.; Bennett, D.; Darling, J.; Kapteyn, A.; Thomas, K. COVID-19 vaccines and mental distress. PLoS ONE 2021, 16, e0256406. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0256406 (accessed on 2 January 2022). [CrossRef]
- DoS. Jordan In Figure 2018–Department of Statistics; Department Statistics: Amman, Jordan, 2018. Available online: http://dosweb.dos.gov.jo/products/jordan-in-figure2018/ (accessed on 2 January 2022).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total Cohort, n = 422 n (%) | Onset Group, n = 211 n (%) | One-Year Group, n = 211 n (%) | p-Value |
|---|---|---|---|---|
| Age, y ® | ||||
| 23–27 | 90 (21.3) | 47 (22.3) | 43 (20.4) | 0.761 |
| 28–31 | 107 (25.4) | 56 (26.5) | 51 (24.2) | |
| 32–39 | 118 (28.0) | 59 (28.0) | 59 (28.0) | |
| ≥40 | 107 (25.4) | 49 (23.2) | 58 (27.5) | |
| Gender | ||||
| Male | 301 (71.3) | 154 (73.0) | 147 (69.7) | 0.451 |
| Female | 121 (28.7) | 57 (27.0) | 64 (30.3) | |
| Marital status | ||||
| Unmarried * | 168 (39.8) | 79 (37.4) | 89 (42.2) | 0.320 |
| Married | 254 (60.2) | 132 (62.6) | 122 (57.8) | |
| Living with elderly of 65 years old or older | ||||
| No | 217 (51.4) | 125 (59.2) | 92 (43.6) | 0.001 |
| Yes | 205 (48.6) | 86 (40.8) | 119 (56.4) | |
| Occupation | ||||
| Physician | 344 (81.5) | 164 (77.7) | 180 (85.3) | 0.060 |
| Others † | 78 (18.5) | 47 (22.3) | 31 (14.7) | |
| Monthly income, Jordanian Dinar (JD) | ||||
| <500 | 56 (13.3) | 25 (11.8) | 31 (14.7) | 0.066 |
| 500–1000 | 189 (44.8) | 107 (50.7) | 82 (38.9) | |
| 1000–2000 | 66 (15.6) | 33 (15.6) | 33 (15.6) | |
| >2000 | 111 (26.3) | 46 (21.8) | 65 (30.8) | |
| COVID-19 characteristics | ||||
| Vaccinated against COVID-19 ¥ | - | - | 151 (71.6) | - |
| Tested for COVID-19 | 233 (55.2) | 49 (23.2) | 184 (87.2) | <0.001 |
| Hx of COVID-19 infection | 98 (23.2) | 1 (0.5) | 97 (46.0) | <0.001 |
| Hx of hospital admission due to COVID-19 infection (% out of infected persons) | 5 (5.1) | 0 (0.0) | 5 (5.2) | - |
| Direct contact with confirmed or suspected COVID-19 individuals or samples | 197 (46.7) | 52 (24.6) | 145 (68.7) | <0.001 |
| Perceived level of contact with COVID-19 patients and samples, Mean (SD) (score range; 1–5) | 3.09 (1.30) | 2.59 (1.19) | 3.59 (1.20) | <0.001 |
| Estimated number ofconfirmed or suspected COVID-19 cases and samples that participants dealt with | ||||
| Zero | 227 (53.8) | 160 (75.8) | 67 (31.8) | <0.001 |
| 1–49 | 91 (21.6) | 31 (14.7) | 60 (28.4) | |
| 50–100 | 40 (9.5) | 9 (4.3) | 31 (14.7) | |
| >100 | 64 (15.2) | 11 (5.2) | 53 (25.1) | |
| Receiving an exceptional education to deal with COVID-19 patients | ||||
| No | 293 (69.4) | 152 (72.0) | 141 (66.8) | 0.245 |
| Yes | 129 (30.6) | 59 (28.0) | 70 (33.2) | |
| Participants’ evaluations of their institution preparedness to deal with COVID-19 patients | ||||
| Very bad | 26 (6.2) | 9 (4.3) | 17 (8.1) | 0.002 |
| Bad | 63 (14.9) | 25 (11.8) | 38 (18.0) | |
| Fair | 98 (23.2) | 38 (18.0) | 60 (28.4) | |
| Good | 116 (27.5) | 65 (30.8) | 51 (24.2) | |
| Very good | 92 (21.8) | 57 (27.0) | 35 (16.6) | |
| Excellent | 27 (6.4) | 17 (8.1) | 10 (4.7) | |
| Perceived changes in work schedule and intensity due to COVID-19 pandemic | ||||
| No perceived changes | 27 (6.4) | 10 (4.7) | 17 (8.1) | 0.474 |
| A little | 31 (7.3) | 19 (9.0) | 12 (5.7) | |
| Some | 78 (18.5) | 39 (18.5) | 39 (18.5) | |
| Much | 165 (39.1) | 81 (38.4) | 84 (39.8) | |
| Very much | 121 (28.7) | 62 (29.4) | 59 (28.0) | |
| Characteristic | Total Cohort, n = 422 | Onset Group, n = 211 | One-Year Group, n = 211 | p-Value |
|---|---|---|---|---|
| GAD-7, anxiety | ||||
| Total score, Mean (SD) | 7.05 (4.83) | 6.15 (4.15) | 7.94 (5.29) | <0.001 |
| Anxiety severity categories, n (%) | ||||
| Normal | 132 (31.3) | 74 (35.1) | 58 (27.5) | 0.003 |
| Mild | 190 (45.0) | 102 (48.3) | 88 (41.7) | |
| Moderate | 58 (13.7) | 24 (11.4) | 34 (16.1) | |
| Severe | 42 (10.0) | 11 (5.2) | 31 (14.7) | |
| Characteristic | GAD-7, Anxiety | ||||||
|---|---|---|---|---|---|---|---|
| Total Score, Mean (SD) | p-Value | Anxiety Severity Categories, n (%) | |||||
| Normal | Mild | Moderate | Severe | p-Value | |||
| Age, y | |||||||
| 23–27 | 7.49 (4.51) | 0.015 | 13 (27.7) | 20 (42.6) | 9 (19.1) | 5 (10.6) | 0.005 |
| 28–31 | 6.09 (4.06) | 18 (32.1) | 30 (53.6) | 5 (8.9) | 3 (5.4) | ||
| 32–39 | 6.29 (4.25) | 22 (37.3) | 28 (47.5) | 6 (10.2) | 3 (5.1) | ||
| ≥40 | 4.78 (3.38) | 21 (42.9) | 24 (49.0) | 4 (8.2) | 0 (0.0) | ||
| Gender | |||||||
| Male | 5.44 (4.04) | <0.001 | 65 (42.2) | 72 (46.8) | 11 (7.1) | 6 (3.9) | <0.001 |
| Female | 8.07 (3.85) | 9 (15.8) | 30 (52.6) | 13 (22.8) | 5 (8.8) | ||
| Marriage status | |||||||
| Unmarried * | 7.19 (4.63) | 0.005 | 22 (27.8) | 38 (48.1) | 10 (12.7) | 9 (11.4) | 0.010 |
| Married | 5.53 (3.72) | 52 (39.4) | 64 (48.5) | 14 (10.6) | 2 (1.5) | ||
| Living with elderly of 65 years old or older | |||||||
| No | 5.91 (4.18) | 0.313 | 46 (36.8) | 59 (47.2) | 13 (10.4) | 7 (5.6) | 0.876 |
| Yes | 6.50 (4.09) | 28 (32.6) | 43 (50.0) | 11 (12.8) | 4 (4.7) | ||
| Occupation | |||||||
| Physician | 6.36 (4.20) | 0.174 | 51 (31.1) | 85 (51.8) | 18 (11.0) | 10 (6.1) | 0.095 |
| Others † | 5.43 (3.91) | 23 (48.9) | 17 (36.2) | 6 (12.8) | 1 (2.1) | ||
| Monthly income, Jordanian Dinar (JD) | |||||||
| <500 | 8.60 (4.74) | <0.001 | 4 (16.0) | 13 (52.0) | 4 (16.0) | 4 (16.0) | 0.003 |
| 500–1000 | 6.78 (4.16) | 32 (29.9) | 53 (49.5) | 15 (14.0) | 7 (6.5) | ||
| 1000–2000 | 4.21 (3.17) | 20 (60.6) | 11 (33.3) | 2 (6.1) | 0 (0.0) | ||
| >2000 | 4.76 (3.37) | 18 (39.1) | 25 (54.3) | 3 (6.5) | 0 (0.0) | ||
| COVID-19 characteristics | |||||||
| COVID-19 tested | 7.63 (4.59) | 0.004 | 12 (24.5) | 22 (44.9) | 9 (18.4) | 6 (12.2) | 0.012 |
| Direct contact with COVID-19 patients and samples | 7.75 (4.89) | 0.001 | 11 (21.2) | 24 (46.2) | 10 (19.2) | 7 (13.5) | 0.001 |
| Perceived contact with COVID-19 patients and samples, Mean (SD) | 2.35 (1.22) | 2.60 (1.17) | 3.04 (1.08) | 3.09 (1.04) | 0.037 | ||
| Estimated number of confirmed or suspected COVID-19 cases and samples that participants dealt with | |||||||
| Zero | 5.42 (3.61) | <0.001 | 63 (39.4) | 80 (50.0) | 15 (9.4) | 2 (1.3) | <0.001 |
| 1–49 | 7.61 (4.57) | 6 (19.4) | 16 (51.6) | 6 (19.4) | 3 (9.7) | ||
| 50–100 | 9.44 (3.81) | 1 (11.1) | 4 (44.4) | 3 (33.3) | 1 (11.1) | ||
| >100 | 10.00 (6.26) | 2 (18.2) | 1 (9.1) | 3 (27.3) | 5 (45.5) | ||
| Receiving an exceptional education to deal with COVID-19 patients | |||||||
| No | 6.74 (4.18) | 0.001 | 44 (28.9) | 78 (51.3) | 20 (13.2) | 10 (6.6) | 0.016 |
| Yes | 4.63 (3.69) | 30 (50.8) | 24 (40.7) | 4 (6.8) | 1 (1.7) | ||
| Participants’ evaluations of their institution preparedness to deal with COVID-19 patients | |||||||
| Very bad | 9.78 (3.07) | <0.001 | 0 (0.0) | 3 (33.3) | 5 (55.6) | 1 (11.1) | <0.001 |
| Bad | 8.68 (5.51) | 7 (28.0) | 9 (36.0) | 4 (16.0) | 5 (20.0) | ||
| Fair | 6.82 (3.84) | 10 (26.3) | 22 (57.9) | 4 (10.5) | 2 (5.3) | ||
| Good | 5.69 (3.41) | 22 (33.8) | 37 (56.9) | 5 (7.7) | 1 (1.5) | ||
| Very good | 5.39 (3.64) | 24 (42.1) | 26 (45.6) | 6 (10.5) | 1 (1.8) | ||
| Excellent | 3.35 (4.34) | 11 (64.7) | 5 (29.4) | 0 (0.0) | 1 (5.9) | ||
| Perceived changes in work schedule and intensity due to COVID-19 pandemic | |||||||
| No changes | 5.80 (3.88) | 0.151 | 3 (30.0) | 6 (60.0) | 1 (10.0) | 0 (0.0) | 0.276 |
| A little | 5.89 (5.43) | 9 (47.4) | 8 (42.1) | 0 (0.0) | 2 (10.5) | ||
| Some | 4.85 (3.54) | 19 (48.7) | 17 (43.6) | 2 (5.1) | 1 (2.6) | ||
| Much | 6.22 (3.81) | 25 (30.9) | 43 (53.1) | 9 (11.1) | 4 (4.9) | ||
| Very much | 7.02 (4.42) | 18 (29.0) | 28 (45.2) | 12 (19.4) | 4 (6.5) | ||
| Characteristic | GAD-7, Anxiety | ||||||
|---|---|---|---|---|---|---|---|
| Total Score, Mean (SD) | p-Value | Anxiety Severity Categories, n (%) | |||||
| Normal | Mild | Moderate | Severe | p-Value | |||
| Age, y | |||||||
| 23–27 | 9.65 (5.23) | <0.001 | 8 (18.6) | 15 (34.9) | 8 (18.6) | 12 (27.9) | 0.016 |
| 28–31 | 8.96 (5.38) | 10 (19.6) | 22 (43.1) | 10 (19.6) | 9 (17.6) | ||
| 32–39 | 8.17 (5.09) | 15 (25.4) | 26 (44.1) | 11 (18.6) | 7 (11.9) | ||
| ≥40 | 5.53 (4.71) | 25 (43.1) | 25 (43.1) | 5 (8.6) | 3 (5.2) | ||
| Gender | |||||||
| Male | 7.02 (5.12) | <0.001 | 52 (35.4) | 60 (40.8) | 20 (13.6) | 15 (10.2) | <0.001 |
| Female | 10.05 (5.11) | 6 (9.4) | 28 (43.8) | 14 (21.9) | 16 (25.0) | ||
| Marriage status | |||||||
| Unmarried * | 9.24 (5.07) | 0.002 | 15 (16.9) | 36 (40.4) | 21 (23.6) | 17 (19.1) | 0.003 |
| Married | 6.99 (5.27) | 43 (35.2) | 52 (42.6) | 13 (10.7) | 14 (11.5) | ||
| Living with elderly of 65 years old or older | |||||||
| No | 8.23 (5.31) | 0.486 | 25 (27.2) | 37 (40.2) | 14 (15.2) | 16 (17.4) | 0.805 |
| Yes | 7.71 (5.29) | 33 (27.7) | 51 (42.9) | 20 (16.8) | 15 (12.6) | ||
| Occupation | |||||||
| Physician | 8.37 (5.43) | 0.004 | 44 (24.4) | 75 (41.7) | 31 (17.2) | 30 (16.7) | 0.004 |
| Others † | 5.45 (3.54) | 14 (45.2) | 13 (41.9) | 3 (9.7) | 1 (3.2) | ||
| Monthly income, Jordanian Dinar (JD) | |||||||
| <500 | 12.77 (5.08) | <0.001 | 2 (6.5) | 5 (16.1) | 12 (38.7) | 12 (38.7) | <0.001 |
| 500–1000 | 8.54 (5.03) | 16 (19.5) | 39 (47.6) | 13 (15.9) | 14 (17.1) | ||
| 1000–2000 | 7.18 (5.13) | 10 (30.3) | 16 (48.5) | 4 (12.1) | 3 (9.1) | ||
| >2000 | 5.26 (3.91) | 30 (46.2) | 28 (43.1) | 5 (7.7) | 2 (3.1) | ||
| COVID-19 characteristics | |||||||
| Vaccinated | 7.75 (5.32) | 0.745 | 36 (23.8) | 69 (45.7) | 24 (15.9) | 22 (14.6) | 0.202 |
| COVID-19 tested | 8.31 (5.24) | 0.007 | 42 (22.8) | 81 (44.0) | 32 (17.4) | 29 (15.8) | 0.001 |
| COVID-19 infected | 8.82 (5.65) | 0.024 | 24 (24.7) | 33 (34.0) | 21 (21.6) | 19 (19.6) | 0.025 |
| Direct contact with COVID-19 patients and samples | 8.83 (5.47) | <0.001 | 32 (22.1) | 59 (40.7) | 25 (17.2) | 29 (20.0) | 0.002 |
| Perceived contact with COVID-19 patients and samples, Mean (SD) | 3.07 (1.29) | 3.53 (1.16) | 4.06 (1.01) | 4.19 (0.87) | <0.001 | ||
| Estimated number of confirmed or suspected COVID-19 cases and samples that participants were dealt with | |||||||
| Zero | 6.21 (4.57) | <0.001 | 26 (38.8) | 27 (40.3) | 12 (17.9) | 2 (3.0) | <0.001 |
| 1–49 | 7.32 (4.72) | 13 (21.7) | 36 (60.0) | 4 (6.7) | 7 (11.7) | ||
| 50–100 | 9.16 (5.48) | 8 (25.8) | 9 (29.0) | 9 (29.0) | 5 (16.1) | ||
| >100 | 10.11 (5.83) | 11 (20.8) | 16 (30.2) | 9 (17.0) | 17 (32.1) | ||
| Receiving an exceptional education to deal with COVID-19 patients | |||||||
| No | 9.10 (5.49) | <0.001 | 29 (20.6) | 55 (39.0) | 31 (22.0) | 26 (18.4) | <0.001 |
| Yes | 5.60 (3.97) | 29 (41.4) | 33 (47.1) | 3 (4.3) | 5 (7.1) | ||
| Participants’ evaluations of their institution preparedness to deal with COVID-19 patients | |||||||
| Very bad | 14.29 (4.78) | <0.001 | 0 (0.0) | 4 (23.5) | 3 (17.6) | 10 (58.8) | <0.001 |
| Bad | 9.39 (5.68) | 8 (21.1) | 13 (34.2) | 9 (23.7) | 8 (21.1) | ||
| Fair | 7.58 (4.20) | 13 (21.7) | 31 (51.7) | 12 (20.0) | 4 (6.7) | ||
| Good | 6.78 (4.80) | 17 (33.3) | 23 (45.1) | 8 (15.7) | 3 (5.9) | ||
| Very good | 6.14 (5.25) | 14 (40.0) | 15 (42.9) | 1 (2.9) | 5 (14.3) | ||
| Excellent | 5.90 (4.68) | 6 (60.0) | 2 (20.0) | 1 (10.0) | 1 (10.0) | ||
| Perceived changes in work schedule and intensity due to COVID-19 pandemic | |||||||
| No changes | 5.65 (3.45) | <0.001 | 9 (52.9) | 5 (29.4) | 3 (17.6) | 0 (0.0) | <0.001 |
| A little | 6.33 (4.89) | 3 (25.0) | 8 (66.7) | 0 (0.0) | 1 (8.3) | ||
| Some | 6.23 (4.77) | 15 (38.5) | 19 (48.7) | 1 (2.6) | 4 (10.3) | ||
| Much | 7.71 (4.75) | 20 (23.8) | 37 (44.0) | 20 (23.8) | 7 (8.3) | ||
| Very much | 10.37 (6.02) | 11 (18.6) | 19 (32.2) | 10 (16.9) | 19 (32.2) | ||
| Variable | No. of Disease Cases/ No. of Total Cases (%) | Adjusted OR | 95% CI (Lower–Upper) | p-Value |
|---|---|---|---|---|
| Onset sample (n = 211) | ||||
| Gender | ||||
| Male | 17/154 (11.0) | REF | REF | REF |
| Female | 18/57 (31.6) | 3.224 | 1.440–7.218 | 0.004 |
| Monthly income, Jordanian Dinar (JD) | – | 0.690 | −0.094–−1.335 | 0.028 |
| COVID-19 test | ||||
| Yes | 15/49 (30.6) | 2.196 | 0.855–5.637 | 0.102 |
| No | 20/162 (12.3) | REF | REF | REF |
| Direct contact with COVID-19 patients and samples | ||||
| Yes | 17/52 (32.7) | 2.292 | 0.909–5.777 | 0.079 |
| No | 18/159 (11.3) | REF | REF | REF |
| Receiving an exceptional education to deal with COVID-19 patients | ||||
| Yes | 5/59 (8.5) | REF | REF | REF |
| No | 30/152 (19.7) | 3.245 | 1.123–9.378 | 0.030 |
| Participants’ evaluations of institution preparedness to deal with COVID-19 patients | ||||
| Very bad | 6/9 (66.7) | 7.075 | 0.477–104.834 | 0.155 |
| Bad | 9/25 (36.0) | 2.861 | 0.266–30.800 | 0.386 |
| Fair | 6/38 (15.8) | 1.247 | 0.121–12.828 | 0.853 |
| Good | 6/65 (9.2) | 0.660 | 0.064–6.829 | 0.728 |
| Very good | 7/57 (12.3) | 1.477 | 0.160–13.661 | 0.731 |
| Excellent | 1/17 (5.9) | REF | REF | REF |
| One-year sample (n = 211) † | ||||
| Gender | ||||
| Male | 35/147 (23.8) | REF | REF | REF |
| Female | 30/64 (46.9) | 1.888 | 0.847–4.206 | 0.120 |
| Occupation | ||||
| Physician | 61/180 (33.9) | 3.214 | 0.868–11.899 | 0.080 |
| Others | 4/31 (12.9) | REF | REF | REF |
| Monthly income, Jordanian Dinar (JD) | ||||
| <500 | 24/31 (77.4) | 12.945 | 3.537–47.380 | <0.001 |
| 500–1000 | 27/82 (32.9) | 3.273 | 1.197–8.949 | 0.021 |
| 1000–2000 | 7/33 (21.2) | 1.611 | 0.452–5.738 | 0.462 |
| >2000 | 7/65 (10.8) | REF | REF | REF |
| Hx of COVID-19 infection | ||||
| Yes | 40/97 (41.2) | 1.707 | 0.790–3.688 | 0.174 |
| No | 25/114 (21.9) | REF | REF | REF |
| Direct contact with COVID-19 patients and samples | ||||
| Yes | 54/145 (37.2) | 2.238 | 0.944–5.302 | 0.067 |
| No | 11/66 (16.7) | REF | REF | REF |
| Receiving an exceptional education to deal with COVID-19 patients | ||||
| Yes | 8/70 (11.4) | REF | REF | REF |
| No | 57/141 (40.4) | 6.052 | 2.394–15.296 | <0.001 |
| Participants’ evaluations of institution preparedness to deal with COVID-19 patients | ||||
| Very bad | 13/17 (76.5) | 8.716 | 1.215–62.523 | 0.031 |
| Bad | 17/38 (44.7) | 2.694 | 0.483–15.024 | 0.258 |
| Fair | 16/60 (26.7) | 1.204 | 0.221–6.563 | 0.830 |
| Good | 11/51 (21.6) | 0.912 | 0.161–5.169 | 0.917 |
| Very good | 6/35 (17.1) | 1.028 | 0.166–6.379 | 0.977 |
| Excellent | 2/10 (20.0) | REF | REF | REF |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yassin, A.; Al-Mistarehi, A.-H.; El-Salem, K.; Karasneh, R.A.; Al-Azzam, S.; Qarqash, A.A.; Khasawneh, A.G.; Zein Alaabdin, A.M.; Soudah, O. Prevalence Estimates and Risk Factors of Anxiety among Healthcare Workers in Jordan over One Year of the COVID-19 Pandemic: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 2615. https://doi.org/10.3390/ijerph19052615
Yassin A, Al-Mistarehi A-H, El-Salem K, Karasneh RA, Al-Azzam S, Qarqash AA, Khasawneh AG, Zein Alaabdin AM, Soudah O. Prevalence Estimates and Risk Factors of Anxiety among Healthcare Workers in Jordan over One Year of the COVID-19 Pandemic: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(5):2615. https://doi.org/10.3390/ijerph19052615
Chicago/Turabian StyleYassin, Ahmed, Abdel-Hameed Al-Mistarehi, Khalid El-Salem, Reema A. Karasneh, Sayer Al-Azzam, Aref A. Qarqash, Aws G. Khasawneh, Anas M. Zein Alaabdin, and Ola Soudah. 2022. "Prevalence Estimates and Risk Factors of Anxiety among Healthcare Workers in Jordan over One Year of the COVID-19 Pandemic: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 5: 2615. https://doi.org/10.3390/ijerph19052615
APA StyleYassin, A., Al-Mistarehi, A.-H., El-Salem, K., Karasneh, R. A., Al-Azzam, S., Qarqash, A. A., Khasawneh, A. G., Zein Alaabdin, A. M., & Soudah, O. (2022). Prevalence Estimates and Risk Factors of Anxiety among Healthcare Workers in Jordan over One Year of the COVID-19 Pandemic: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(5), 2615. https://doi.org/10.3390/ijerph19052615