
HIIE Protocols Promote Better Acute Effects on Blood Glucose and Pressure Control in People with Type 2 Diabetes than Continuous Exercise

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Data Collection
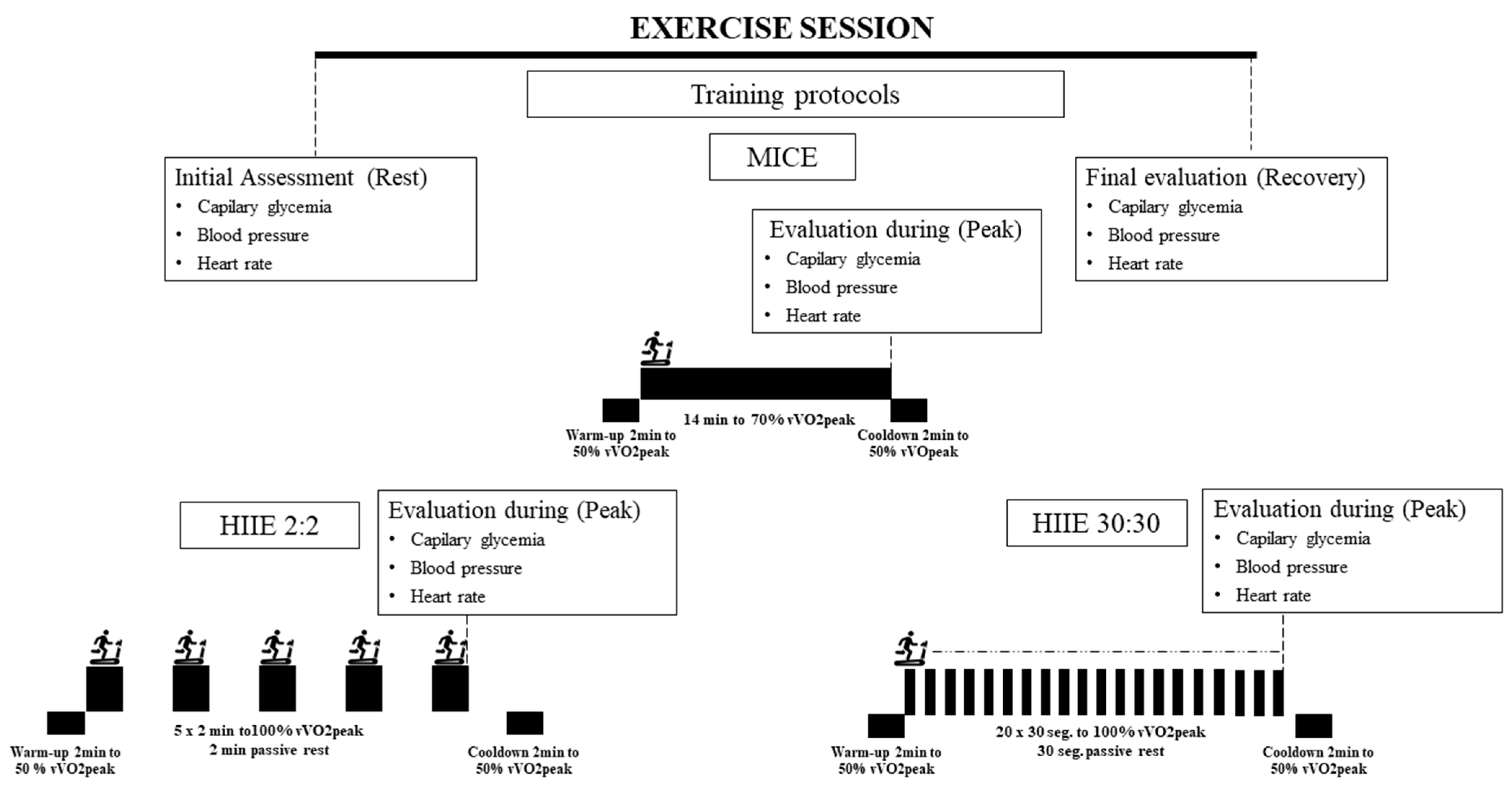
2.3. Exercise Sessions
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: A systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turnbull, F.; Neal, B.; Algert, C.; Chalmers, J.; Chapman, N.; Cutler, J.; Woodward, M.; MacMahon, S. Effects of different blood pressure-lowering regimens on major cardiovascular events in individuals with and without diabetes mellitus: Results of prospectively designed overviews of randomized trials. Arch. Intern. Med. 2005, 165, 1410–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metcalfe, R.S.; Fitzpatrick, B.; Fitzpatrick, S.; McDermott, G.; Brick, N.; McClean, C.; Davison, G.W. Extremely short duration interval exercise improves 24-h glycaemia in men with type 2 diabetes. Eur. J. Appl. Physiol. 2018, 118, 2551. [Google Scholar] [CrossRef] [PubMed]
- Terada, T.; Wilson, B.J.; Myette-Cóté, E.; Kuzik, N.; Bell, G.J.; McCargar, L.J.; Boulé, N.G. Targeting specific interstitial glycemic parameters with high-intensity interval exercise and fasted-state exercise in type 2 diabetes. Metabolism 2016, 65, 599–608. [Google Scholar] [CrossRef]
- Santiago, É.; Delevatti, R.S.; Bracht, C.G.; Netto, N.; Lisboa, S.C.; Vieira, A.F.; Costa, R.R.; Hübner, A.; Fossati, M.A.; Kruel, L.F.M. Acute glycemic and pressure responses of continuous and interval aerobic exercise in patients with type 2 diabetes. Clin. Exp. Hypertens. 2018, 40, 179–185. [Google Scholar] [CrossRef]
- Bird, S.R.; Hawley, J.A. Update on the effects of physical activity on insulin sensitivity in humans. BMJ Open Sport Exerc. Med. 2017, 2, e000143. [Google Scholar] [CrossRef] [Green Version]
- De Nardi, A.T.; Tolves, T.; Lenzi, T.L.; Signori, L.U.; da Silva, A.M.V. High-intensity interval training versus continuous training on physiological and metabolic variables in prediabetes and type 2 diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2018, 137, 149–159. [Google Scholar] [CrossRef]
- DiMenna, F.J.; Arad, A.D. Exercise as “precision medicine” for insulin resistance and its progression to type 2 diabetes: A research review. BMC Sports Sci. Med. Rehabil. 2018, 10, 21. [Google Scholar] [CrossRef]
- Francois, M.E.; Durrer, C.; Pistawka, K.J.; Halperin, F.A.; Little, J.P. Resistance-based interval exercise acutely improves endothelial function in type 2 diabetes. Am. J. Physiol. Heart Circ. Physiol. 2016, 311, H1258–H1267. [Google Scholar] [CrossRef]
- Gillen, J.B.; Little, J.P.; Punthakee, Z.; Tarnopolsky, M.A.; Riddell, M.C.; Gibala, M.J. Acute high-intensity interval exercise reduces the postprandial glucose response and prevalence of hyperglycaemia in patients with type 2 diabetes. Diabetes Obes. Metab. 2012, 14, 575–577. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.; Raphael, L.; Silva, B.; Gentil, P.; Seguro, C.S.; Campos Martins De Oliveira, J.; Silva, M.S.; Alves Marques, V.; Beltrame, T.; Cristina, A.; et al. High-Intensity Interval Training Improves Cardiac Autonomic Function in Patients with Type 2 Diabetes: A Randomized Controlled Trial. Biology 2022, 11, 66. [Google Scholar] [CrossRef]
- Viana, A.A.; Fernandes, B.; Alvarez, C.; Guimarães, G.V.; Ciolac, E.G. Prescribing high-intensity interval exercise by RPE in individuals with type 2 diabetes: Metabolic and hemodynamic responses. Appl. Physiol. Nutr. Metab. 2019, 44, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.; Sousa, N.; Themudo-Barata, J.L.; Reis, V.M. High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in Middle-Aged and Older Patients with Type 2 Diabetes: A Randomized Controlled Crossover Trial of the Acute Effects of Treadmill Walking on Glycemic Control. Int. J. Environ. Res. Public Health 2019, 16, 4163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viana, R.B.; de Lira, C.A.B.; Naves, J.P.A.; Coswig, V.S.; Del Vecchio, F.B.; Ramirez-Campillo, R.; Vieira, C.A.; Gentil, P. Can We Draw General Conclusions from Interval Training Studies? Sports Med. 2018, 48, 2001–2009. [Google Scholar] [CrossRef]
- Kilpatrick, M.W.; Martinez, N.; Little, J.P.; Jung, M.E.; Jones, A.M.; Price, N.W.; Lende, D.H. Impact of High-Intensity Interval Duration on Perceived Exertion. Med. Sci. Sports Exerc. 2015, 47, 1038–1045. [Google Scholar] [CrossRef]
- Kilpatrick, M.W.; Greeley, S.J. Exertional responses to sprint interval training: A comparison of 30-sec. and 60-sec. conditions. Psychol. Rep. 2014, 114, 854–865. [Google Scholar] [CrossRef]
- Naves, J.P.A.; Rebelo, A.C.S.; Silva, L.R.B.E.; Silva, M.S.; Ramirez-Campillo, R.; Ramírez-Vélez, R.; Gentil, P. Cardiorespiratory and perceptual responses of two interval training and a continuous training protocol in healthy young men. Eur. J. Sports Sci. 2019, 19, 653–660. [Google Scholar] [CrossRef]
- Silva, L.R.B.; Gentil, P.R.V.; Beltrame, T.; Basso Filho, M.A.; Alves, F.M.; Silva, M.S.; Pedrino, G.R.; Ramirez-Campillo, R.; Coswig, V.; Rebelo, A.C.S. Exponential model for analysis of heart rate responses and autonomic cardiac modulation during different intensities of physical exercise. R. Soc. Open Sci. 2019, 6, 190639. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Standards of Medical Care in Diabetes—2019 Abridged for Primary Care Providers. Clin. Diabetes 2019, 37, 11–34. [Google Scholar] [CrossRef] [Green Version]
- Malachias, M.V.; Gomes, M.A.; Nobre, F.; Alessi, A.; Feitosa, A.D.; Coelho, E.B. 7th Brazilian Guideline of Arterial Hypertension: Chapter 2—Diagnosis and classification. Arq. Bras. Cardiol. 2016, 107, 7–13. [Google Scholar] [PubMed]
- WHO. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 2000; p. 252. Available online: http://apps.who.int/iris/bitstream/10665/42330/1/WHO_TRS_894.pdf?ua¼1&ua¼1 (accessed on 12 January 2022).
- Thompson, P.D.; Arena, R.; Riebe, D.; Pescatello, L.S. ACSM’s new preparticipation health screening recommendations from ACSM’s guidelines for exercise testing and prescription, ninth edition. Curr. Sports Med. Rep. 2013, 12, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billat, V.L. Interval training for performance: A scientific and empirical practice: Special recommendations for middle- and long-distance running. Part II: Anaerobic interval training. Sports Med. 2001, 31, 75–90. [Google Scholar] [CrossRef]
- Silva, L.R.B.; Gentil, P.; Seguro, C.S.; de Oliveira, G.T.; Silva, M.S.; Zamunér, A.R.; Beltrame, T.; Rebelo, A.C.S. High Fasting Glycemia Predicts Impairment of Cardiac Autonomic Control in Adults with Type 2 Diabetes: A Case-Control Study. Front. Endocrinol. 2021, 12, 760292. [Google Scholar] [CrossRef]
- Silva, L.R.B.E.; Zamunér, A.R.; Gentil, P.; Alves, F.M.; Leal, A.G.F.; Soares, V.; Silva, M.S.; Vieira, M.F.; Simões, K.; Pedrino, G.R.; et al. Cardiac autonomic modulation and the kinetics of heart rate responses in the on- and off-transient during exercise in women with metabolic syndrome. Front. Physiol. 2017, 8, 542. [Google Scholar] [CrossRef]
- Cassidy, S.; Vaidya, V.; Houghton, D.; Zalewski, P.; Seferovic, J.P.; Hallsworth, K.; MacGowan, G.A.; Trenell, M.I.; Jakovljevic, D.G. Unsupervised high-intensity interval training improves glycaemic control but not cardiovascular autonomic function in type 2 diabetes patients: A randomised controlled trial. Diabetes Vasc. Dis. Res. 2019, 16, 69–76. [Google Scholar] [CrossRef]
- Yardley, J.E.; Sigal, R.J.; Perkins, B.A.; Riddell, M.C.; Kenny, G.P. Resistance exercise in type 1 diabetes. Can. J. Diabetes 2013, 37, 420–426. [Google Scholar] [CrossRef]
- De Brito, L.C.; Fecchio, R.Y.; Peçanha, T.; Lima, A.; Halliwill, J.; Forjaz, C.L.D.M. Recommendations in Post-exercise Hypotension: Concerns, Best Practices and Interpretation. Int. J. Sports Med. 2019, 40, 487–497. [Google Scholar] [CrossRef] [Green Version]
- Sigal, R.J.; Kenny, G.P.; Wasserman, D.H.; Castaneda-Sceppa, C. Physical activity/exercise and type 2 diabetes. Diabetes Care 2004, 27, 2518–2539. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, J.R. Potential causes, mechanisms, and implications of post exercise hypotension. J. Hum. Hypertens. 2002, 16, 225–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamer, M. The anti-hypertensive effects of exercise: Integrating acute and chronic mechanisms. Sports Med. 2006, 36, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Anunciação, P.G.; Polito, M.D. A review on post-exercise hypotension in hypertensive individuals. Arq. Bras. Cardiol. 2011, 96, e100–e109. [Google Scholar]
- Kirwan, J.P.; Sacks, J.; Nieuwoudt, S. The essential role of exercise in the management of type 2 diabetes. Cleve. Clin. J. Med. 2017, 84, S15. [Google Scholar] [CrossRef]
- Angadi, S.S.; Mookadam, F.; Lee, C.D.; Tucker, W.J.; Haykowsky, M.J.; Gaesser, G.A. High-intensity interval training vs. moderate-intensity continuous exercise training in heart failure with preserved ejection fraction: A pilot study. J. Appl. Physiol. 2015, 119, 753–758. [Google Scholar] [CrossRef]
- Kemi, O.J.; Wisløff, U. Mechanisms of exercise-induced improvements in the contractile apparatus of the mammalian myocardium. Acta Physiol. 2010, 199, 425–439. [Google Scholar] [CrossRef]
- Freyssin, C.; Verkindt, C.; Prieur, F.; Benaich, P.; Maunier, S.; Blanc, P. Cardiac rehabilitation in chronic heart failure: Effect of an 8-week, high-intensity interval training versus continuous training. Arch. Phys. Med. Rehabil. 2012, 93, 1359–1364. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| HIIE Long (n = 14) | HIIE Short (n = 15) | MICE (n = 15) | TOTAL (n = 44) | |
|---|---|---|---|---|
| Age (years) | 54.64 ± 8.91 | 55.67 ± 7.44 | 57.33 ± 8.93 | 55.91 ± 1.25 |
| Weight (kg) | 80.65 ± 14.52 | 79.45 ± 10.95 | 76.27 ± 16.91 | 78.75 ± 21.30 |
| BMI (kg/m2) | 29.44 ± 4.94 | 28.94 ± 3.64 | 28.49 ± 4.94 | 28.95 ± 0.67 |
| Blood glucose (mg/dL) | 142.43 ± 59.06 | 126.47 ± 38.23 | 133.80 ± 54.84 | 134.05 ± 7.62 |
| Hb1ac (% mmol/mol) | 9.6 ± 2.9; 81 | 8.9 ± 1.6; 74 | 9.0 ± 2.4; 75 | 9.1 ± 2.3; 76 |
| HR (bpm) | 75.0 ± 7.38 | 66.0 ± 9.35 | 70.75 ± 9.39 | 71.11 ± 9.07 |
| SBP (mmHg) | 143.57 ± 23.65 | 131.07 ± 14.24 | 131.0 ± 15.12 | 135.12 ± 18.62 |
| DBP (mmHg) | 90.14 ± 12.24 | 83.47 ± 9.19 | 87.50 ± 8.69 | 86.95 ± 10.28 |
| HIIE Long (n = 14) | HIIE Short (n = 15) | MICE (n = 15) | TOTAL (n = 44) | |
|---|---|---|---|---|
| Velocity (km/h) | 8.22 ± 0.56 | 7.32 ± 0.38 | 5.19 ± 0.43 | 6.88 ± 2.14 |
| Central SPE | 7.5 ± 1.02 * | 5.47 ± 2.0 | 5.33 ± 2.29 | 6.07 ± 2.07 |
| Peripheral SPE | 7.79 ± 1.37 * | 5.80 ± 2.37 | 5.80 ± 1.74 | 6.43 ± 2.06 |
| Resting | Peak | Recovery | ∆ | η2 | ||
|---|---|---|---|---|---|---|
| HIIE long | 134.21 ± 19.95 | 159.93 ± 6.72 | 121.79 ± 14.68 | −12.43 * | 0.11 | |
| HIIE short | SBP | 123.60 ± 12.72 | 154.0 ± 4.96 | 114.87 ± 9.08 | −8.73 * | 0.13 |
| MICE | 125.33 ± 15.56 | 155.0 ± 7.22 | 124.87 ± 17.30 | −0.47 | 0.00 | |
| HIIE long | 134.21 ± 19.95 | 159.93 ± 6.72 | 121.79 ± 14.68 | −12.43 * | 0.11 | |
| HIIE short | DBP | 123.60 ± 12.72 | 154.0 ± 4.96 | 114.87 ± 9.08 | −8.73 * | 0.13 |
| MICE | 125.33 ± 15.56 | 155.0 ± 7.22 | 124.87 ± 17.30 | −0.47 | 0.00 | |
| HIIE long | 77.57 ± 9.33 | 133.93 ± 11.70 | 89.93 ± 12.04 | 12.35 * | 0.24 | |
| HIIE short | HR | 79.60 ± 10.70 | 124.53 ± 6.55 | 92.07 ± 23.41 | 12.47 * | 0.10 |
| MICE | 76.6 ± 12.25 | 105.0 ± 9.30 | 84.73 ± 13.32 | 8.13 | 0.09 | |
| HIIE long | 172.86 ± 77.33 | 161.29 ± 77.05 | 140.71 ± 72.61 | −32.14 * | 0.04 | |
| HIIE short | Glucose | 168.67 ± 73.88 | 152.33 ± 68.12 | 137.27 ± 69.31 | −31.40 * | 0.04 |
| MICE | 148.13 ± 43.99 | 126.80 ± 44.0 | 143.07 ± 56.80 | −5.07 | 0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teles, G.d.O.; Gentil, P.; Silva, L.R.B.e.; Sousa, W.d.M.; Seguro, C.S.; Rebelo, A.C.S. HIIE Protocols Promote Better Acute Effects on Blood Glucose and Pressure Control in People with Type 2 Diabetes than Continuous Exercise. Int. J. Environ. Res. Public Health 2022, 19, 2601. https://doi.org/10.3390/ijerph19052601
Teles GdO, Gentil P, Silva LRBe, Sousa WdM, Seguro CS, Rebelo ACS. HIIE Protocols Promote Better Acute Effects on Blood Glucose and Pressure Control in People with Type 2 Diabetes than Continuous Exercise. International Journal of Environmental Research and Public Health. 2022; 19(5):2601. https://doi.org/10.3390/ijerph19052601
Chicago/Turabian StyleTeles, Gabriela de Oliveira, Paulo Gentil, Lucas Raphael Bento e Silva, Wátila de Moura Sousa, Camila Simões Seguro, and Ana Cristina Silva Rebelo. 2022. "HIIE Protocols Promote Better Acute Effects on Blood Glucose and Pressure Control in People with Type 2 Diabetes than Continuous Exercise" International Journal of Environmental Research and Public Health 19, no. 5: 2601. https://doi.org/10.3390/ijerph19052601
APA StyleTeles, G. d. O., Gentil, P., Silva, L. R. B. e., Sousa, W. d. M., Seguro, C. S., & Rebelo, A. C. S. (2022). HIIE Protocols Promote Better Acute Effects on Blood Glucose and Pressure Control in People with Type 2 Diabetes than Continuous Exercise. International Journal of Environmental Research and Public Health, 19(5), 2601. https://doi.org/10.3390/ijerph19052601