
Effects of Bullying Forms on Adolescent Mental Health and Protective Factors: A Global Cross-Regional Research Based on 65 Countries


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Sample
2.2. Ethics Statement
2.3. Measures
2.3.1. Dependent Variable: Mental Health
2.3.2. Independent Variables: Frequency and Forms of Being Bullied
2.3.3. Control Variables
2.3.4. Protective Factors: Parental Supports
2.4. Statistical Analysis
3. Results
3.1. Sample Description
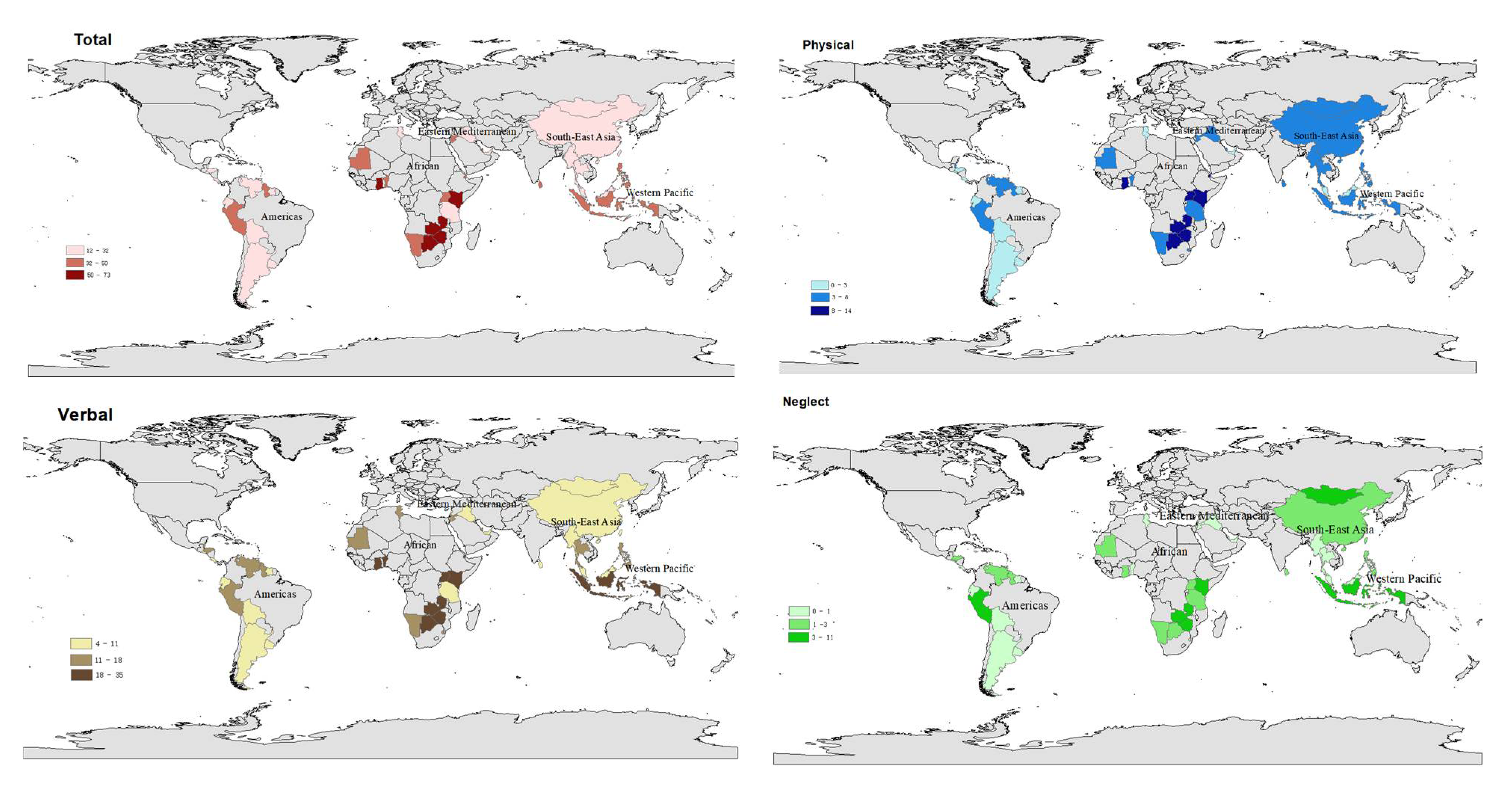
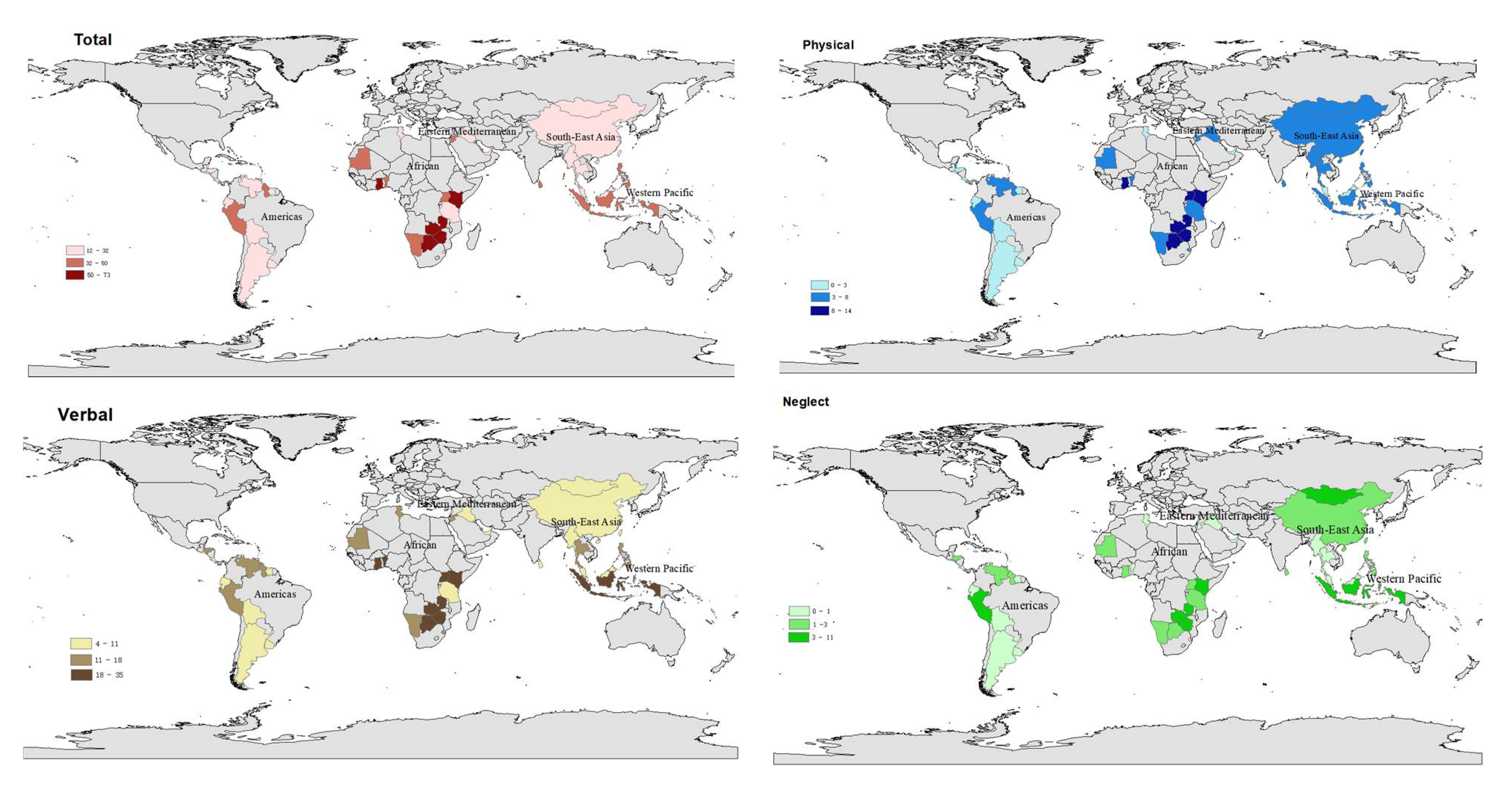
3.2. Prevalence and Forms of Bullying across the Regions
3.3. Effects of Bullying on Psychological Well-Being of Adolescents
3.4. Effects of Bullying on Psychological Well-Being in Adolescents of Different Gender
3.5. Effects of Bullying on Psychological Well-Being in Adolescents of Different Ages
3.6. The Protective Effect of Parental Support on the Psychological Well-Being
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klomek, A.B.; Sourander, A.; Elonheimo, H. Bullying by peers in childhood and effects on psychopathology, suicidality, and criminality in adulthood. Lancet Psychiatry 2015, 2, 930–941. [Google Scholar] [CrossRef]
- Thomas, H.J.; Connor, J.P.; Scott, J.G. Integrating Traditional Bullying and Cyberbullying: Challenges of Definition and Measurement in Adolescents—A Review. Educ. Psychol. Rev. 2014, 27, 135–152. [Google Scholar] [CrossRef]
- Zhong, M.T.; Huang, X.C.; Huebner, E.S.; Tian, L.L. Association between bullying victimization and depressive symptoms in children: The mediating role of self-esteem. J. Affect. Disord. 2021, 294, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H.J.; Chan, G.C.; Scott, J.G.; Connor, J.P.; Kelly, A.B.; Williams, J. Association of different forms of bullying victimisation with adolescents’ psychological distress and reduced emotional wellbeing. Aust. N. Z. J. Psychiatry 2016, 50, 371–379. [Google Scholar] [CrossRef]
- Fund, U.N.I.C.E. Half of World’s Teens Experience Peer Violence in and around School. Available online: https://www.unicef.org/press-releases/half-worlds-teens-experience-peer-violence-and-around-school-unicef (accessed on 10 December 2021).
- World Health Organization. Children: New Threats to Health. Available online: https://www.who.int/news-room/fact-sheets/detail/children-new-threats-to-health (accessed on 10 December 2021).
- World Health Organization. Youth Violence. Available online: https://www.who.int/news-room/fact-sheets/detail/youth-violence (accessed on 10 December 2021).
- Elgar, F.J.; McKinnon, B.; Walsh, S.D.; Freeman, J.; Donnelly, P.D.; de Matos, M.G.; Gariepy, G.; Aleman-Diaz, A.Y.; Pickett, W.; Molcho, M.; et al. Structural Determinants of Youth Bullying and Fighting in 79 Countries. J. Adolesc. Health 2015, 57, 643–650. [Google Scholar] [CrossRef]
- Yen, C.F.; Huang, M.F.; Kim, Y.S.; Wang, P.W.; Tang, T.C.; Yeh, Y.C.; Lin, H.C.; Liu, T.L.; Wu, Y.Y.; Yang, P. Association between types of involvement in school bullying and different dimensions of anxiety symptoms and the moderating effects of age and gender in Taiwanese adolescents. Child Abus. Negl. 2013, 37, 263–272. [Google Scholar] [CrossRef]
- Liu, T.L.; Hsiao, R.C.; Chou, W.J.; Yen, C.F. Self-Reported Depressive Symptoms and Suicidality in Adolescents with Attention-Deficit/Hyperactivity Disorder: Roles of Bullying Involvement, Frustration Intolerance, and Hostility. Int. J. Environ. Res. Public Health 2021, 18, 7829. [Google Scholar] [CrossRef]
- Li, L.; Chen, X.; Li, H. Bullying victimization, school belonging, academic engagement and achievement in adolescents in rural China: A serial mediation model. Child. Youth Serv. Rev. 2020, 113, 104946. [Google Scholar] [CrossRef]
- Gentry, R.H.; Pickel, K.L. Male and Female Observers’ Evaluations of a Bullying Case as a Function of Degree of Harm, Type of Bullying, and Academic Level. J. Aggress. Maltreatment Trauma 2014, 23, 1038–1056. [Google Scholar] [CrossRef]
- Smith, A.U.; Reidy, D. Bullying and suicide risk among sexual minority youth in the United States. Prev. Med. 2021, 153, 106728. [Google Scholar] [CrossRef]
- Tang, J.J.; Yu, Y.; Wilcox, H.C.; Kang, C.; Wang, K.; Wang, C.; Wu, Y.; Chen, R. Global risks of suicidal behaviours and being bullied and their association in adolescents: School-based health survey in 83 countries. EClinicalMedicine 2020, 19, 100253. [Google Scholar] [CrossRef] [Green Version]
- Zhu, X.X.; Griffiths, H.; Eisner, M.; Hepp, U.; Ribeaud, D.; Murray, A.L. Developmental associations between bullying victimization and suicidal ideation and direct self-injurious behavior in adolescence and emerging adulthood. J. Child Psychol. Psyc. 2021, 9, 1–9. [Google Scholar] [CrossRef]
- González-Cabrera, J.; Montiel, I.; Ortega-Barón, J.; Calvete, E.; Orue, I.; Machimbarrena, J.M. Epidemiology of Peer Victimization and its Impact on Health-Related Quality of Life in Adolescents: A Longitudinal Study. Sch. Ment. Health 2021, 13, 338–346. [Google Scholar] [CrossRef]
- Staubli, S.; Killias, M. Long-term outcomes of passive bullying during childhood: Suicide attempts, victimization and offending. Eur. J. Criminol. 2011, 8, 377–385. [Google Scholar] [CrossRef]
- Bettencourt, A.; Farrell, A.; Liu, W.; Sullivan, T. Stability and change in patterns of peer victimization and aggression during adolescence. J. Clin. Child Adolesc. Psychol. 2013, 42, 429–441. [Google Scholar] [CrossRef]
- Choi, B.; Park, S. Who Becomes a Bullying Perpetrator After the Experience of Bullying Victimization? The Moderating Role of Self-esteem. J. Youth Adolesc. 2018, 47, 2414–2423. [Google Scholar] [CrossRef]
- Yoon, D.; Shipe, S.L.; Park, J.; Yoon, M. Bullying patterns and their associations with child maltreatment and adolescent psychosocial problems. Child Youth Serv. Rev. 2021, 129, 106178. [Google Scholar] [CrossRef]
- Maunder, R.E.; Harrop, A.; Tattersall, A.J. Pupil and staff perceptions of bullying in secondary schools: Comparing behavioural definitions and their perceived seriousness. Educ. Res. 2010, 52, 263–282. [Google Scholar] [CrossRef]
- Chen, L.M.; Liu, K.S.; Cheng, Y.Y. Validation of the perceived school bullying severity scale. Educ. Psychol. 2012, 32, 169–182. [Google Scholar] [CrossRef]
- Baier, D.; Hong, J.S.; Kliem, S.; Bergmann, M.C. Consequences of Bullying on Adolescents’ Mental Health in Germany: Comparing Face-to-Face Bullying and Cyberbullying. J. Child Fam. Stud. 2018, 28, 2347–2357. [Google Scholar] [CrossRef]
- Turner, M.G.; Exum, M.L.; Brame, R.; Holt, T.J. Bullying victimization and adolescent mental health: General and typological effects across sex. J. Crim. Justice 2013, 41, 53–59. [Google Scholar] [CrossRef]
- Shongwe, M.C.; Dlamini, L.P.; Simelane, M.S.; Masuku, S.K.S.; Shabalala, F.S. Are there Gender Differences in the Prevalence and Correlates of Bullying Victimization Among in-School Youth in Eswatini? Sch. Ment. Health 2021, 13, 299–311. [Google Scholar] [CrossRef]
- Kim, Y.K.; Kim, Y.J.; Maleku, A.; Moon, S.S. Typologies of Peer Victimization, Depression, and Alcohol Use among High School Youth in the United States: Measuring Gender Differences. Soc. Work Public Health 2019, 34, 293–306. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Iannotti, R.J.; Nansel, T.R. School bullying among adolescents in the United States: Physical, verbal, relational, and cyber. J. Adolesc. Health 2009, 45, 368–375. [Google Scholar] [CrossRef] [Green Version]
- Yen, C.F.; Yang, P.; Wang, P.W.; Lin, H.C.; Liu, T.L.; Wu, Y.Y.; Tang, T.C. Association between school bullying levels/types and mental health problems among Taiwanese adolescents. Compr. Psychiatry 2014, 55, 405–413. [Google Scholar] [CrossRef]
- Wilkins, N.; Myers, L.; Kuehl, T.; Bauman, A.; Hertz, M. Connecting the Dots: State Health Department Approaches to Addressing Shared Risk and Protective Factors Across Multiple Forms of Violence. J. Public Health Manag. Pract. 2018, 24 (Suppl. 1), S32–S41. [Google Scholar] [CrossRef]
- Yule, K.; Houston, J.; Grych, J. Resilience in Children Exposed to Violence: A Meta-analysis of Protective Factors Across Ecological Contexts. Clin. Child Fam. Psychol. Rev. 2019, 22, 406–431. [Google Scholar] [CrossRef]
- Zych, I.; Farrington, D.P.; Ttofi, M.M. Protective factors against bullying and cyberbullying: A systematic review of meta-analyses. Aggress. Violent Behav. 2019, 45, 4–19. [Google Scholar] [CrossRef]
- Biswas, T.; Scott, J.G.; Munir, K.; Thomas, H.J.; Huda, M.M.; Hasan, M.M.; David de Vries, T.; Baxter, J.; Mamun, A.A. Global variation in the prevalence of bullying victimisation amongst adolescents: Role of peer and parental supports. EClinicalMedicine 2020, 20, 100276. [Google Scholar] [CrossRef]
- Sonja, P.; Julian, D.; Therese, S.; Donna, C. Bullying in school and cyberspace: Associations with depressive symptoms in Swiss and Australian adolescents. Child Adolesc. Psychiatry Ment. Health 2010, 4, 28. [Google Scholar]
- Srabstein, J.C. The Global Implications of Bullying and Other Forms of Maltreatment, in the Context of Migratory Trends and Psychiatric Resources. Child Adolesc. Psychiatry. Clin. N. Am. 2015, 24, 799–810. [Google Scholar] [CrossRef]
- Baldry, A.C.; Farrington, D.P. Protective Factors as Moderators of Risk Factors in Adolescence Bullying. Soc. Psychol. Educ. 2005, 8, 263–284. [Google Scholar] [CrossRef]
- Meinck, F.; Cluver, L.D.; Boyes, M.E.; Ndhlovu, L.D. Risk and Protective Factors for Physical and Emotional Abuse Victimisation amongst Vulnerable Children in South Africa. Child Abus. Rev. 2015, 24, 182–197. [Google Scholar] [CrossRef] [Green Version]
- Dendup, T.; Putra, I.G.N.E.; Dorji, T.; Tobgay, T.; Dorji, G.; Phuntsho, S.; Tshering, P. Correlates of sedentary behaviour among Bhutanese adolescents: Findings from the 2016 Global School-based health survey. Child. Youth Serv. Rev. 2020, 119, 105520. [Google Scholar] [CrossRef]
- Li, W.; Zhao, Y.; Wang, Q.; Zhou, J. Twenty Years of Entropy Research: A Bibliometric Overview. Entropy 2019, 21, 694. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.G.; Li, J. Influence of land acquisition for rural tourism on the well- being of landless farmers based on the empirical analysis of PSM model. Resour. Sci. 2021, 43, 171–184. [Google Scholar] [CrossRef]
- Smith, P.K.; López-Castro, L.; Robinson, S.; Görzig, A. Consistency of gender differences in bullying in cross-cultural surveys. Aggress. Violent Behav. 2019, 45, 33–40. [Google Scholar] [CrossRef]
- Chen, L.; Lu, R.R.; Duan, J.L.; Ma, J.; Zhu, G.R.; Song, Y.; Lau, P.W.C.; Prochaska, J.J. Combined Associations of Smoking and Bullying Victimization With Binge Drinking Among Adolescents in Beijing, China. Front. Psychiatry 2021, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Hammar, E.; Bladh, M.; Agnafors, S. Mental health and experience of being bullied in 12-year-old children with overweight and obesity. Acta Paediatr. 2020, 109, 1450–1457. [Google Scholar] [CrossRef]
- Malecki, C.K.; Demaray, M.K.; Smith, T.J.; Emmons, J. Disability, poverty, and other risk factors associated with involvement in bullying behaviors. J. Sch. Psychol. 2020, 78, 115–132. [Google Scholar] [CrossRef]
- Petrella, E.; Grandi, G.; Di Cerbo, L.; Bertarini, V.; Neri, I.; Facchinetti, F. 813: Changes of body composition in women with BMI ≥ 25 included in a lifestyle program. Correlation with birthweight’s centile. Am. J. Obstet. Gynecol. 2018, 218, S484–S485. [Google Scholar] [CrossRef]
- Burns, R.D.; Bai, Y.; Pfledderer, C.D.; Brusseau, T.A.; Byun, W. Movement Behaviors and Perceived Loneliness and Sadness within Alaskan Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 6866. [Google Scholar] [CrossRef] [PubMed]
- Juan, A.; Zuze, L.; Hannan, S.; Govender, A.; Reddy, V. Bullies, victims and bully-victims in South African schools: Examining the risk factors. S. Afr. J. Educ. 2018, 38, S1–S10. [Google Scholar] [CrossRef]
- Scheithauer, H.; Hayer, T.; Petermann, F.; Jugert, G. Physical, verbal, and relational forms of bullying among German students: Age trends, gender differences, and correlates. Aggress. Behav. 2006, 32, 261–275. [Google Scholar] [CrossRef]
- Vieno, A.; Gini, G.; Santinello, M. Different forms of bullying and their association to smoking and drinking behavior in Italian adolescents. J. Sch. Health 2011, 81, 393–399. [Google Scholar] [CrossRef]
- Ybrandt, H. The relation between self-concept and social functioning in adolescence. J. Adolesc. 2008, 31, 1–16. [Google Scholar] [CrossRef]
- Smith, P.K.; Sharp, S. The Problem of School Bullying; Routledge: London, UK, 1994. [Google Scholar]
- Peltzer, K.; Pengpid, S. Prevalence of bullying victimisation and associated factors among in-school adolescents in Mozambique. J. Psychol. Afr. 2020, 30, 64–68. [Google Scholar] [CrossRef]
- Giumetti, G.W.; Kowalski, R.M.; Feinn, R.S. Predictors and outcomes of cyberbullying among college students: A two wave study. Aggress. Behav. 2021, 48, 40–54. [Google Scholar] [CrossRef]
- Gloppen, K.; McMorris, B.; Gower, A.; Eisenberg, M. Associations between bullying involvement, protective factors, and mental health among American Indian youth. Am. J. Orthopsychiatry 2018, 88, 413–421. [Google Scholar] [CrossRef]
- Gómez-Ortiz, O.; Del Rey, R.; Casas, J.-A.; Ortega-Ruiz, R. Parenting styles and bullying involvement/Estilos parentales e implicación en bullying. Cult. Y Educ. 2014, 26, 132–158. [Google Scholar] [CrossRef]
- Gomez-Ortiz, O.; Romera, E.M.; Ortega-Ruiz, R. Parenting styles and bullying. The mediating role of parental psychological aggression and physical punishment. Child Abus. Negl. 2016, 51, 132–143. [Google Scholar] [CrossRef]
- Espelage, D.L.; Bosworth, K.; Simon, T.R. Examining the social context of bullying behaviors in early adolescence. J. Couns. Dev. 2000, 73, 326–333. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Percentage/Mean (SD) | |||||
|---|---|---|---|---|---|---|
| Total | African | Americas | Eastern Mediterranean | South East Asia | Western Pacific | |
| Independent variable | ||||||
| Being bullied | 32.03% | 47.36% | 26.23% | 41.53% | 33.19% | 27.58% |
| Frequency of being bullied | ||||||
| 1–5 days | 24.68% | 35.68% | 20.46% | 31.31% | 26.73% | 21.34% |
| 6–19 days | 4.06% | 6.60% | 3.10% | 5.52% | 3.97% | 3.44% |
| >20 days | 3.28% | 5.08% | 2.67% | 4.70% | 2.50% | 2.79% |
| Form of being bullied | ||||||
| Physical | 24.02% | 28.98% | 18.84% | 24.71% | 25.66% | 24.26% |
| Verbal | 66.36% | 61.75% | 71.09% | 68.19% | 63.24% | 65.12% |
| Neglect | 9.62% | 9.26% | 10.07% | 7.11% | 11.10% | 10.61% |
| Dependent variable | ||||||
| Psychological well-being | 5.79 (1.82) | 5.47 (1.92) | 5.89 (1.81) | 5.69 (2.00) | 5.97 (1.78) | 5.81 (1.70) |
| Control variable | ||||||
| Age | 14.14 (1.20) | 14.45 (1.29) | 13.89 (0.99) | 13.85 (0.95) | 14.05 (1.18) | 14.45 (1.37) |
| Gender | ||||||
| Male | 46.74% | 45.81% | 46.77% | 47.10% | 45.20% | 47.34% |
| Female | 53.26% | 54.19% | 53.23% | 52.90% | 54.80% | 52.66% |
| Weight status | ||||||
| Underweight | 26.63% | 20.66% | 17.29% | 27.45% | 48.43% | 34.12% |
| Normal weight | 63.69% | 75.31% | 73.17% | 62.76% | 47.86% | 52.09% |
| Overweight | 9.67% | 4.03% | 9.55% | 9.80% | 3.71% | 13.79% |
| Cigarettes smoking | ||||||
| <5 days | 96.11% | 97.72% | 95.98% | 95.96% | 97.58% | 95.24% |
| 6–19 days | 1.92% | 1.13% | 2.22% | 2.01% | 1.17% | 2.05% |
| >20 days | 1.98% | 1.14% | 1.80% | 2.03% | 1.26% | 2.71% |
| Alcohol use | ||||||
| <5 days | 95.97% | 96.73% | 91.84% | 99.58% | 98.65% | 98.17% |
| 6–19 days | 2.91% | 2.08% | 6.11% | 0.31% | 0.90% | 1.19% |
| >20 days | 1.12% | 1.19% | 2.05% | 0.12% | 0.44% | 0.63% |
| Socioeconomic status | 4.20 (1.01) | 3.89 (1.09) | 4.39 (0.93) | 4.36 (1.03) | 4.18 (1.05) | 4.04 (1.01) |
| Close friendship | 2.41 (0.92) | 1.91 (1.04) | 2.45 (0.91) | 2.39 (0.91) | 2.53 (0.83) | 2.56 (0.84) |
| Frequency of missing school | ||||||
| <2 days | 91.58% | 90.04% | 90.93% | 90.64% | 94.77% | 92.52% |
| 3–9 days | 6.62% | 7.82% | 6.89% | 7.48% | 4.04% | 6.13% |
| >10 days | 1.80% | 2.14% | 2.18% | 1.87% | 1.20% | 1.35% |
| Parental supervision | 2.94 (1.49) | 3.14 (1.51) | 2.97 (1.51) | 3.37 (1.56) | 3.15 (1.42) | 2.57 (1.36) |
| Parental connectedness | 3.00 (1.46) | 3.11 (1.44) | 3.16 (1.48) | 3.16 (1.48) | 2.98 (1.44) | 2.81 (1.37) |
| Parental bonding | 3.19 (1.44) | 3.06 (1.43) | 3.34 (1.46) | 3.34 (1.50) | 3.35 (1.39) | 3.17 (1.36) |
| Region | Being Bullied (%) | Physical (%) | Verbal (%) | Neglect (%) | Total Sample (n) |
|---|---|---|---|---|---|
| Total | 32.03 | 4.50 | 12.43 | 1.80 | 167,286 |
| African | 47.36 | 9.65 | 20.56 | 3.08 | 21501 |
| Benin | 42.46 | 6.28 | 19.96 | 0.75 | 1067 |
| Botswana | 52.20 | 11.64 | 23.90 | 3.53 | 1134 |
| Ghana | 56.72 | 12.79 | 20.15 | 2.31 | 2119 |
| Kenya | 54.35 | 13.56 | 26.94 | 5.47 | 2138 |
| Mauritania | 47.46 | 6.30 | 15.50 | 2.10 | 1142 |
| Namibia | 45.59 | 8.27 | 17.19 | 1.80 | 2937 |
| Seychelles | 47.26 | 3.56 | 17.46 | 1.37 | 1094 |
| Swaziland | 31.28 | 5.91 | 11.66 | 0.92 | 2487 |
| Uganda | 43.09 | 11.66 | 20.52 | 2.54 | 1613 |
| Tanzania | 25.74 | 6.78 | 9.48 | 2.13 | 1593 |
| Zambia | 61.58 | 13.07 | 34.52 | 4.93 | 872 |
| Zimbabwe | 59.15 | 12.22 | 29.89 | 6.54 | 3305 |
| Americas | 26.23 | 2.77 | 10.44 | 1.48 | 59326 |
| Antigua and Barbuda | 26.87 | 3.55 | 12.75 | 0.55 | 1098 |
| Argentina | 25.07 | 1.79 | 9.97 | 1.32 | 19559 |
| Bahamas | 21.74 | 2.42 | 10.03 | 1.09 | 1196 |
| Barbados | 12.50 | 2.11 | 4.94 | 0.36 | 1376 |
| Belize | 30.29 | 4.05 | 12.07 | 1.40 | 1433 |
| Bolivia | 30.51 | 3.07 | 10.08 | 1.63 | 2511 |
| British Virgin Is. | 18.06 | 1.80 | 7.91 | 0.63 | 1113 |
| Cayman Is. | 26.51 | 5.26 | 11.50 | 1.36 | 1026 |
| Costa Rica | 19.34 | 1.34 | 8.68 | 1.39 | 2166 |
| Curacao | 26.59 | 0.73 | 12.90 | 1.17 | 2046 |
| El Salvador | 25.30 | 3.43 | 8.85 | 1.99 | 3965 |
| Ecuador | 22.50 | 1.39 | 8.76 | 1.46 | 1507 |
| Grenada | 27.77 | 3.76 | 12.65 | 1.28 | 1091 |
| Guyana | 38.32 | 4.78 | 13.56 | 2.19 | 1777 |
| Honduras | 31.00 | 1.89 | 12.15 | 2.69 | 1374 |
| Jamaica | 36.91 | 5.37 | 14.36 | 1.46 | 1024 |
| Montserrat | 28.77 | 5.48 | 12.33 | 10.96 | 146 |
| Peru | 47.14 | 4.24 | 17.83 | 4.51 | 2238 |
| St. Kitts and Nevis | 22.07 | 4.16 | 8.77 | 0.89 | 1346 |
| St. Lucia | 25.20 | 2.87 | 10.76 | 1.43 | 976 |
| St. Vincent and the Grenadines | 28.48 | 5.43 | 11.07 | 1.43 | 976 |
| Suriname | 26.26 | 0.91 | 7.55 | 0.30 | 994 |
| Trinidad and Tobago | 15.77 | 2.90 | 6.30 | 0.50 | 2207 |
| Uruguay | 18.98 | 0.74 | 9.60 | 1.26 | 2689 |
| Venezuela | 32.36 | 6.98 | 12.40 | 1.81 | 3483 |
| Eastern Mediterranean | 41.53 | 5.42 | 14.95 | 1.56 | 23222 |
| Bahrain | 40.06 | 10.92 | 20.17 | 1.26 | 714 |
| Djibouti | 40.06 | 10.92 | 20.17 | 1.26 | 714 |
| Iraq | 27.45 | 6.10 | 7.12 | 0.58 | 1377 |
| Jordan | 41.57 | 5.35 | 14.96 | 1.47 | 1364 |
| Lebanon | 23.79 | 5.08 | 8.44 | 0.33 | 1812 |
| Occupied Palestinian territory | 52.27 | 5.67 | 18.22 | 1.96 | 11614 |
| Qatar | 37.40 | 4.28 | 13.58 | 1.67 | 1377 |
| Tunisia | 30.28 | 3.79 | 11.69 | 1.58 | 2087 |
| United Arab Emirates | 22.10 | 2.64 | 8.41 | 1.20 | 2163 |
| South East Asia | 33.19 | 4.68 | 11.53 | 2.02 | 13301 |
| Indonesia | 50.14 | 4.49 | 20.20 | 4.53 | 2559 |
| Maldives | 32.73 | 3.17 | 9.84 | 1.58 | 1830 |
| Myanmar | 19.51 | 4.77 | 7.84 | 1.66 | 1927 |
| Sri Lanka | 36.00 | 4.26 | 6.96 | 2.47 | 2228 |
| Thailand | 28.23 | 6.42 | 12.94 | 0.74 | 2288 |
| Timor Leste | 28.72 | 4.66 | 9.48 | 0.81 | 2469 |
| Western Pacific | 27.58 | 3.86 | 10.37 | 1.69 | 49936 |
| Brunei | 20.40 | 1.45 | 7.41 | 1.32 | 2417 |
| China | 28.29 | 5.30 | 8.71 | 1.83 | 7780 |
| Cook Is. | 27.14 | 3.95 | 9.54 | 1.32 | 608 |
| Kiribati | 34.96 | 8.24 | 18.27 | 0.64 | 1396 |
| Malaysia | 16.99 | 1.51 | 7.88 | 0.63 | 23476 |
| Mongolia | 27.62 | 4.18 | 4.71 | 4.95 | 4885 |
| Nauru | 38.72 | 10.44 | 15.15 | 0.67 | 297 |
| Philippines | 48.22 | 4.29 | 15.46 | 3.70 | 3544 |
| Samoa | 72.40 | 13.06 | 34.66 | 2.91 | 1685 |
| Solomon Is. | 63.55 | 10.61 | 24.68 | 3.58 | 782 |
| Tonga | 51.00 | 8.54 | 20.67 | 2.00 | 1698 |
| Tuvalu | 29.62 | 6.87 | 7.04 | 0.65 | 611 |
| Vanuatu | 65.92 | 14.93 | 21.80 | 2.11 | 757 |
| Model 1 (95% CI) | Model 2 (95% CI) | |
|---|---|---|
| Frequency of being bullied | ||
| 1–5 days | −1.22 *** (−1.27, −1.18) | |
| 6–19 days | −1.43 *** (−1.47, −1.38) | |
| >20 days | −7.53 *** (−7.72, −7.33) | |
| Form of being bullied | ||
| Physical | −7.49 *** (−7.89, −7.10) | |
| Verbal | −9.64 *** (−9.89, −1.01) | |
| Neglect | −1.21 *** (−1.27, −1.15) | |
| Age | −1.29 *** (−1.36, −1.23) | −1.27 *** (−1.33, −1.20) |
| Gender (Female) | −5.97 *** (−6.13, −5.81) | −5.80 *** (−5.96, −5.63) |
| Weight Status | ||
| Normal weight | −1.28 *** (−1.46, −1.09) | −1.25 *** (−1.43, −1.06) |
| Overweight | −7.60 *** (−9.41, −3.42) | −4.47 *** (−7.48, −1.05) |
| Cigarettes smoking | ||
| 6–19 days | −3.43 *** (−4.02, −2.84) | −3.84 *** (−4.43, −3.25) |
| >20 days | −3.64 *** (−4.22, −3.05) | −4.16 *** (−4.75, −3.57) |
| Alcohol use | ||
| 6–19 days | −3.13 *** (−3.61, −2.65) | −3.23 *** (−3.71, −2.75) |
| >20 days | −3.84 *** (−4.61, −3.07) | −4.46 *** (−5.23, −3.69) |
| Socioeconomic status | ||
| Middle-low | −2.64 *** (−3.32, −1.97) | −2.47 *** (−3.15, −1.80) |
| Middle | −2.64 (−8.25, 2.96) | 2.07 (−3.55, 7.68) |
| Middle-high | 2.66 *** (2.10, 3.22) | 3.29 *** (2.73, 3.85) |
| High | 6.15 *** (5.60, 6.69) | 6.74 *** (6.20, 7.28) |
| Close friendship | ||
| 1 friend | 1.27 *** (0.04, 1.71) | 1.45 *** (1.05, 1.84) |
| 2 friends | 1.65 *** (1.27, 2.02) | 1.89 *** (1.52, 2.27) |
| 3 or more friends | 3.58 *** (3.24, 3.91) | 3.82 *** (3.48, 4.15) |
| Frequency of missing school | ||
| 3–9 days | −2.63 *** (−2.95, −2.30) | −2.85 *** (−3.17, −2.52) |
| >10 days | −4.08 *** (−4.69, −3.48) | −4.68 *** (−5.28, −4.07) |
| Parental supervision | ||
| Rarely | 5.98 *** (3.44, 8.53) | 5.86 *** (3.31, 8.41) |
| Sometimes | 1.25 (−2.37, 2.62) | 5.66 (−1.93, 3.06) |
| Most of the time | 6.48 *** (3.69, 9.27) | 6.84 *** (4.04, 9.63) |
| Always | 7.33 (4.79, 9.86) | 6.97 *** (4.43, 9.51) |
| Parental connectedness | ||
| Rarely | 5.98 *** (3.44, 8.53) | 6.34 *** (3.65, 9.03) |
| Sometimes | 1.25 (−2.37, 2.62) | 5.96 (3.44, 8.49) |
| Most of the time | 6.48 *** (3.69, 9.27) | 1.92 *** (1.63, 2.20) |
| Always | 7.33 *** (4.79, 9.86) | 3.559 *** (3.32, 3.86) |
| Parental bonding | ||
| Rarely | −9.73 *** (−1.26, −6.88) | −8.33 *** (−1.12, −5.47) |
| Sometimes | −7.61 *** (−1.03, −4.96) | −6.24 *** (−8.89, −3.59) |
| Most of the time | −1.99 (−4.85, 8.68) | 1.45 (−2.72, 3.01) |
| Always | 1.30 *** (1.03, 1.57) | 1.48 *** (1.21, 1.75) |
| Constant | 8.15 *** | 7.96 *** |
| R2 | 0.17 | 0.17 |
| N | 167,286 | 167,286 |
| Total | African | Americas | Eastern Mediterranean | South East Asia | Western Pacific | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |
| Frequency of being bullied (X2) | 293.43 *** | 4.80 | 26.69 *** | 284.47 *** | 168.79 *** | 67.34 *** | ||||||
| 1–5 days | −1.21 *** | −1.23 *** | −1.21 *** | −9.93 *** | −1.29 *** | −1.23 *** | −1.15 *** | −1.55 *** | −1.08 *** | −1.22 *** | −1.03 *** | −1.16 *** |
| 6–19 days | −1.40 *** | −1.45 *** | −1.16 *** | −1.29 *** | −1.51 *** | −1.48 *** | −1.50 *** | −1.83 *** | −1.02 *** | −1.69 *** | −1.25 *** | −1.16 *** |
| >20 days | −7.01 *** | −7.94 *** | −6.74 *** | −7.10 *** | −7.54 *** | −8.25 *** | −6.15 *** | −8.46 *** | −6.44 *** | −8.50 *** | −5.95 *** | −7.36 *** |
| Form of being bullied (X2) | 1.0 *** | 73.69 *** | 424.39 *** | 547.14 *** | 211.67 *** | 224.02 *** | ||||||
| Physical | −7.86 *** | −6.62 *** | −7.21 *** | −7.02 *** | −8.64 *** | −5.63 *** | −8.10 *** | −9.72 *** | −6.93 *** | −8.36 *** | −5.94 *** | −6.48 *** |
| Verbal | −9.55 *** | −1.01 *** | −9.37 *** | −9.17 *** | −1.07 *** | −1.07 *** | −1.20 *** | −8.13 *** | −1.11 *** | −8.62 *** | −8.39 *** | −8.05 *** |
| Neglect | −1.24 *** | −1.18 *** | −6.80 *** | −1.11 *** | −1.28 *** | −1.33 *** | −1.70 *** | −1.40 *** | −1.30 *** | −1.14 *** | −1.25 *** | −9.89 *** |
| Total | African | Americas | Eastern Mediterranean | South East Asia | Western Pacific | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≥15 | <15 | ≥15 | <15 | ≥15 | <15 | ≥15 | <15 | ≥15 | <15 | ≥15 | <15 | |
| Frequency of being bullied (X2) | 218.44 *** | 10.73 * | 8.11 * | 35.85 *** | 19.10 *** | 815.58 *** | ||||||
| 1–5 days | −1.07 *** | −1.25 *** | −9.92 *** | −1.20 *** | −1.16 *** | −1.31 *** | −1.23 *** | −1.40 *** | −7.83 *** | −1.32 *** | −1.01 *** | −1.13 *** |
| 6–19 days | −1.30 *** | −1.46 *** | −1.09 *** | −1.36 *** | −1.46 *** | −1.50 *** | −1.68 *** | −1.64 *** | −1.08 *** | −1.41 *** | −1.00 *** | −1.31 *** |
| >20 days | −6.80 *** | −7.61 *** | −6.29 *** | −7.64 *** | −7.24 *** | −8.27 *** | −6.78 *** | −7.71 *** | −6.68 *** | −7.97 *** | −6.56 *** | −6.70 *** |
| Form of being bullied (X2) | 211.83 *** | 23.29 *** | 25.00 *** | 56.24 *** | 70.41 *** | 703.00 *** | ||||||
| Physical | −5.97 *** | −6.72 *** | −7.14 *** | −7.20 *** | −6.21 *** | −7.82 *** | −8.80 *** | −8.86 *** | −5.56 *** | −7.60 *** | −5.65 *** | −6.23 *** |
| Verbal | −9.10 *** | −1.02 *** | −8.18 *** | −9.32 *** | −1.02 *** | −1.08 *** | −9.49 *** | −9.98 *** | −9.71 *** | −9.97 *** | −7.71 *** | −8.26 *** |
| Neglect | −1.09 *** | −1.32 *** | −8.04 *** | −8.65 *** | −1.19 *** | −1.31 *** | −1.40 *** | −1.56 *** | −1.18 *** | −1.25 *** | −9.75 *** | −1.15 *** |
| B | R2 | 95% CI | |
|---|---|---|---|
| Model 1 | 0.15 | ||
| Being bullied | −9.98 *** | (−9.60, −1.03) | |
| Parental supervision * Being bullied | 3.22 *** | (2.13, 4.31) | |
| Constant | 8.41 *** | (8.29, 8.54) | |
| Model 2 | 0.16 | ||
| Being bullied | −1.14 *** | (−1.18, −1.10) | |
| Parental connectedness * Being bullied | 8.19 *** | (7.05, 9.34) | |
| Constant | 8.43 *** | (8.30, 8.55) | |
| Model 3 | 0.15 | ||
| Being bullied | −1.05 *** | (−1.09, −1.01) | |
| Parental bonding * Being bullied | 4.93 *** | (3.78, 6.07) | |
| Constant | 8.43 *** | (8.30, 8.55) |
| Physical | Verbal | Neglect | |
|---|---|---|---|
| Parental supervision | −1.53 | 8.21 | 3.14 |
| Parental connectedness | 2.36 | 8.71 *** | 1.05 *** |
| Parental bonding | 2.23 | 2.47 * | 8.98 |
| Constant | 0.00 *** | 0.00 *** | 0.00 ** |
| N | 7554 | 20,875 | 3031 |
| R2 | 0.08 | 0.10 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Man, X.; Liu, J.; Xue, Z. Effects of Bullying Forms on Adolescent Mental Health and Protective Factors: A Global Cross-Regional Research Based on 65 Countries. Int. J. Environ. Res. Public Health 2022, 19, 2374. https://doi.org/10.3390/ijerph19042374
Man X, Liu J, Xue Z. Effects of Bullying Forms on Adolescent Mental Health and Protective Factors: A Global Cross-Regional Research Based on 65 Countries. International Journal of Environmental Research and Public Health. 2022; 19(4):2374. https://doi.org/10.3390/ijerph19042374
Chicago/Turabian StyleMan, Xiaoou, Jiatong Liu, and Zengxin Xue. 2022. "Effects of Bullying Forms on Adolescent Mental Health and Protective Factors: A Global Cross-Regional Research Based on 65 Countries" International Journal of Environmental Research and Public Health 19, no. 4: 2374. https://doi.org/10.3390/ijerph19042374
APA StyleMan, X., Liu, J., & Xue, Z. (2022). Effects of Bullying Forms on Adolescent Mental Health and Protective Factors: A Global Cross-Regional Research Based on 65 Countries. International Journal of Environmental Research and Public Health, 19(4), 2374. https://doi.org/10.3390/ijerph19042374